

Short Communication | DOI: https://doi.org/10.31579/2835-8295/062
Primary Sclerosing Cholangitis Post Liver Transplantation
- Miah Lingelbach
- James Keane
- Leonard B. Goldstein *
Assistant Vice President for Clinical Education Development, A.T. Still University
*Corresponding Author: Leonard B. Goldstein, Assistant Vice President for Clinical Education Development, A.T. Still University.
Citation: Miah Lingelbach, James Keane, Leonard B. Goldstein (2024), Primary Sclerosing Cholangitis Post Liver Transplantation, International Journal of Clinical Reports and Studies, 3(3); DOI:10.31579/2835-8295/062
Copyright: © 2024, Leonard B. Goldstein. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 March 2024 | Accepted: 24 April 2024 | Published: 07 May 2024
Keywords: autism; evidence-based treatment; expert opinion
Abstract
Background: For decades, autism disorders have been considered life-long disorders without curative therapies despite a variety of medications have been tried including pyridoxine, magnesium, thiamine, biotin, folic acid, and omega-3. However, we have recently described a new therapeutic approach aiming primarily at improving and curing the two major diagnostic features of autism which are poor responsiveness to their name and poor eye contact. The first book which described the cure of the autistic features was included in Book authority’s lists best books of all time. Therefore, we have been consulted about the treatment of autism from many countries in the world including the United Kingdom, Canada, United Arab of Emirate, Tunisia, Palestine, India, and Pakistan, and many of the international cases have been reported.
Patients and methods: During November, 2023, we received a consultation about the possible treatment of a three and half year’s girl from Cuba who was diagnosed with autism at about the age of three years. She has been treated mostly with supplements including thiamine (Vitamin B1), Biotin, and vitamin B6 daily. She was also receiving other treatments without any known scientific basis including homeopathic carcinosin, topical lugol iodine solution 1% (One drop daily), and Tibetan precious pill (Rinchen Ratna Jamphel) which was prescribed by the Tibetan Medical Institute.
Results: At the age of three and half years (November, 2023), she was still having the two major diagnostic features of autism which are the lack of appropriate responsiveness to own name, and the lack of eye contact. She was able to go to the toilet and possibly know about 100-150 words. However, she was saying mostly words like mama, juice (to ask for a juice), and bye-bye. She was also talking with herself most of the time, saying unintelligible words and meaningless sounds. She was capable of holding a pen and drawing circular figures and other things. She was also capable of identifying letters. She was able to eat with a spoon, but she needed help with hand washing. She was also able to announce her need to go toilet and she could go to toilet, but she was needing help with clothes after she has been in the toilet. Therefore, she had acceptable fine motor skills and adaptive behaviors and her disorder was considered to be associated with normal intelligence. Therefore, the patient received a provisional diagnosis of classic autism and the initial recommended evidence-based treatment included courses of intramuscular cerebrospinal and oral risperidone. After one month of treatment the parents reported great improvements that made risperidone no longer necessary, her behavior was better and she started talking more. The major diagnostic features of autism have disappeared. She began talking with sentences and using more verbs.
Expert opinion: The current evidence-based expert opinion suggests that the individualized use of courses of intramuscular cerebrospinal can be in this case of autism with the aim curing the major diagnostic features of autism. Citicoline treatment can be considered in this patient to improve speech after the occurrence of improvement in autistic features and hyperactivity.
Introduction
Patients with primary Sclerosing Cholangitis (PSC) suffer from autoimmune destruction of the hepatobiliary tracts, which culminates in:
- Ductal Damage;
- Ductopenia;
- Lymphocytic Infiltration of Hepatobiliary Tracts;
- Parenchymal Inflammation; and,
- Fibrosis (1).
There is currently no effective intervention in controlling the natural history of this condition, and it often results in cirrhosis and end-stage liver disease (2). Liver transplant (LT) stands as the therapeutic intervention of choice to halt liver failure (3). However, LT is well known to have operative risk as a major, life-threatening surgery. Various donor and recipient risk factors alter post-transplant prognosis and life expectancy. (4, 5, 6). Patients with PSC suffer from systemic autoimmune destruction of the native hepatobiliary tracts and liver, which puts them at risk of destruction of transplanted liver. The sub-acute to long term prognosis of post-liver transplantation course with respect to PSC recurrence, graft viability, and survival, rejection, and system specific causes of death have seldomly been evaluated. Hence, a comprehensive examination of the prognostic relationships that exist between PSC-IBD subtypes and post-LT outcomes is needed to characterize the impact of PSC recurrence on post-LT outcomes of PSC patients. This article aims to explore the issue of primary sclerosing cholangitis, the likelihood and effects of recurrence post-liver transplantation
Discussion:
Diagnosis of Recurrent PSC
Recurrent PSC progresses similarly to the native liver PSC with increased ductal proliferation and inflammation within the portal tract resulting in periportal edema8. As PSC continues to progress, there are fibro-obliterative lesions seen with destruction of medium and small bile ducts8. These findings are unfortunately similar to bile duct injuries that are seen with chronic allograft rejection, ischemia from preservation injury, or hepatic artery thrombosis. All of these can result in a very similar clinical picture with elevated liver enzymes, jaundice, right upper quadrant pain and other signs of liver failure. Thus, diagnosing recurrent PSC post-liver transplantation is clinically difficult and must be done supplemented with imaging. The current suggested imaging used for diagnosis today with magnetic resonance cholangiography (MRC)8. This is needed to reveal biliary strictures that are not associated with transplantation anastomosis of the biliary tree as strictures can commonly occur at anastomosis sites due to the scarring process.
With these other disease processes that result in a very similar clinical picture, the only way to diagnose recurrent PSC status post liver transplantation with characteristic cholangiographic findings after exclusion of other causes of biliary strictures that may result from suboptimal immunosuppression or other pathological processes8. Many have adopted the Mayo criteria for the diagnosis of recurrent PSC. These inclusion and exclusion criteria are outlined in Table 110.
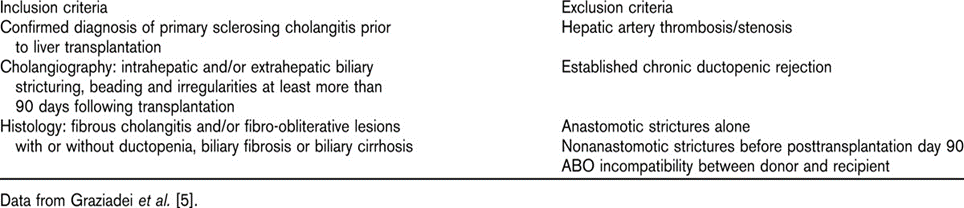
Table 110
Risk Factors for Recurrent PSC
There are many peritransplantation variables that have been studied in various analyses that may predict the recurrence of PSC8. Many suggested risk factors include age, male gender, donor-recipient gender mismatch, and coexistent IBD8. There are many reasons we have not yet been able to pin-point specific risk factors leading to the recurrence of PSC after liver transplant but the main reason being that the pathogenesis of PSC in the native liver remains unclear as PSC results from an autoimmune process stemming from many genetic and environmental factors8. As PSC has a significantly higher occurrence rate in patients with irritable bowel disease like ulcerative colitis, there have been many hypotheses as to IBD being the root cause of the pathogenesis of PSC. In the setting of concurrent IBD, many studies have aimed to test the leaky theory of IBD in the setting of PSC stating that bacterial toxins from the inflamed colon may have a genetic predisposition to rendering patients susceptible to PSC8. This was studied in patient populations without concurrent IBD or underwent a total colectomy prior to transplantation. These populations were found to have a significant reduction in PSC recurrence post transplantation8.
Recurrence of PSC and Graft/Patient Survival
Comparing the 3309 patients with PSC in United Network for Organ Sharing (UNOS) and the 3254 patients with primary biliary cirrhosis (PBC) who had liver transplantation from 1987-2001, the rate of repeat liver transplantation was significantly higher in patients with PSC (12.4% vs 8.5%)8. In continuing this comparison, patients with PSC had lower graft and patient survival during 10-year follow-up than patients with PBC8. Campsen et al. reported that once a patient was diagnosed with recurrent disease, the median survival time without receiving a second transplant was 39.1 months8. In a study of 15 patients from a single center that received single liver transplantation grafts due to PSC and received either cyclosporine or tacrolimus for immunosuppression. In this study the 7-year graft survival rate was 65% and 7-year patient survival rate was 60%9. In this study, 2 patients (12%) resulted in recurrent PSC as assessed by liver histology and MRC9. This study was limited by lack of gold standard diagnostic criteria of recurrent PSC vs. other posttransplant conditions that resemble similar ductal injuries, making it hard to distinguish the true cause of graft failure. In an additional study based on the Mayo criteria (Table 1) for diagnosing recurrent PSC, the incidence lies in the range of 10% - 37% appearing anywhere from 7-60 months post liver transplant10. Analyzing a retrospective study from a single center, they divided 58 patients into living donor liver transplant and deceased donor liver transplant10. Recurrent PSC was seen in 4 of the 14 living donor liver transplants (28.6%) in which patients receive a portion of resected liver from a living donor and 7 of 44 deceased donor liver transplants (15.9%)10.
Conclusion:
In conclusion, the analysis of the few studies completed to date analyzing the recurrence of PSC in a donor liver post-transplantation shows that PSC has a recurrence rate of 10-30% and results in increased risk of re-transplantation compared to another autoimmune hepatobiliary diseases requiring liver transplant, primary biliary cholangitis. Recurrence of PSC has been shown to lead to graft dysfunction and need may result in the need for re-transplantation. Although many centers have adopted the use of the Mayo criteria for inclusion and exclusion criteria regarding the diagnosis of recurrent PSC, there is a need for solidifying a gold standard diagnostic to further analyze the true recurrence of PSC versus other causes of biliary tree dysfunction post-liver transplantation. With true diagnostic studies, there would be more clarification as to the risks of recurrent PSC and treatment options targeted to the cause of graft failure.
References
- Fosby B, Karlsen TH, Melum E.: (2012). “Recurrence and Rejection in Liver Transplantation for Primary Sclerosing Cholangitis”; World J Gastroenterol; 18: 1-15
View at Publisher | View at Google Scholar - Karlsen TH, Folseraas T, Thorburn D, Vesterhus M: (2017). “Primary Sclerosing Cholangitis-A Comprehensive Review; J Hepatol; 67: 1298-1323
View at Publisher | View at Google Scholar - Lazaridis KN, LaRusso NF: (2016). “Primary Sclerosing Cholangitis”; NEJM; 375: 1161-1170
View at Publisher | View at Google Scholar - Durand F, Levitsky J, Cauchy F, et.al.: (2019). “Age and Liver Transplantation”; J Hepatol; 70: 745-758
View at Publisher | View at Google Scholar - Barman PM, VanWagner LB: (2021). “Cardiac Risk Assessment in Liver Transplant Candidates: Current Controversies and Future Directions”; Hepatology; 73: 2564-2576
View at Publisher | View at Google Scholar - Feng S, Goodrich NP, Bradd-Gresham JL, et.al. (2006). “Characteristics Associated with Liver Graft Failure: The Concept of Donor Risk Index”; Am J Transplant; 6: 783-790
View at Publisher | View at Google Scholar - Ricciuto A, Kamath BM, Griffiths AM: (2018). “The IBD and PSC Phenotypes of PSC-IBD”; Curr Gastroentreol Rep; 20: 16
View at Publisher | View at Google Scholar - Charatcharoenwitthaya, P., Lindor, K.D.: “Recurrence of Primary Sclerosing Cholangitis After Liver Transplantation”; Disease Recurrence After Liver Transplantation; 2016; 121-134
View at Publisher | View at Google Scholar - U. Ołdakowska-Jedynak, M. Nowak, K. Mucha, B. (2006). Foroncewicz: “Recurrence of Primary Sclerosing Cholangitis in Patients After Liver Transplantation”; Transplantation Proceedings vol 38: 240-243
View at Publisher | View at Google Scholar - Graziadei, Ivo W. (2011). “Live donor liver transplantation for primary sclerosing cholangitis: is disease recurrence increased?” Current opinion in gastroenterology vol. 27,3: 301-305.
View at Publisher | View at Google Scholar
