

Research Article | DOI: https://doi.org/10.31579/2835-2882/022
Prevalence of Respiratory Failure and Associated Factors in Adult Intensive Care Unit of Saint Paul’s and Addis Ababa Burn, Emergency and Trauma Hospital, Ethiopia 2020
Kindalem Gebeyehu Abebe, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia.
*Corresponding Author: Kindalem Gebeyehu Abebe, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia.
Citation: Kindalem G. Abebe, Yohannes Koster, Melke Bimrew, (2023), Prevalence Of Respiratory Failure and Associated Factors in Adult Intensive Care Unit of Saint Paul’s and Addis Ababa Burn, Emergency and Trauma Hospital, Ethiopia 2020, Clinical Research and Studies, 2(3); DOI:10.31579/2835-2882/022
Copyright: 2023, Kindalem Gebeyehu Abebe. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 June 2023 | Accepted: 19 June 2023 | Published: 27 June 2023
Keywords: prevalence; respiratory failure and associated factors; ethiopia
Abstract
Background: Severe respiratory failure is a common reason for admission to the intensive care unit that occurs for several reasons, including pulmonary disease, neuromuscular disease, shock and the necessity for airway protection or temporary breathing support after major surgery. For patients with ARF, mechanical aeration is the cornerstone of management.
Objective: to assess the prevalence of respiratory failure and associated factors among patients admitted the adult intensive care unit of Saint Paul’s Millennium Medical College and Addis Ababa Burn, Emergency and Trauma hospitals Addis Ababa, Ethiopia, 2020.
The prevalence of respiratory failure was high. Multiple factors influence the development of respiratory failure. Older age, cardiac disease, Human Immune Deficiency Virus and trauma were at risk of developed respiratory failure Therefore, Health care professionals, policy makers and other concerned bodies should give emphasis to the factors that contribute to the development of respiratory failure. They should give priority especially for older, HIV, cardiac, and trauma patients to provide easily accessible and quality care.
Introduction
Respiratory failure is a disorder, characterized by inability of the respiratory system to support effective and continuous gas exchange. The most common causes of acute respiratory failure are pneumonia, acute respiratory distress syndrome (ARDS), sepsis, asthma, drug ingestion, and trauma. In the aging, pneumonia, heart failure, chronic obstructive pulmonary disease (COPD), ARDS, and sepsis predominate [1].
Severe respiratory failure is a common reason for admission to the intensive care unit that occurs for several reasons, including pulmonary disease, neuromuscular disease, shock and the necessity for airway protection or temporary breathing support after major surgery. For patients with ARF, mechanical aeration is the cornerstone of management. [2, 3]
The magnitude of acute respiratory failure has become one of the most epidemiological tasks facing today's health systems in all intensive care units around the world.[4] Though, it is difficult to enumerate because the cause of death is more likely to be registered as pneumonia, COPD, or another underlying condition, rather than respiratory failure [5]. Respiratory failure endure a major cause of morbidity and mortality in the intensive care location, RF may be responsible for as many as 10–15% for admissions to medical ICU and for as many as 50–75% of those patients who require ICU stays longer than 7 days [6].
It also grounds numerous complications such as pulmonary embolism, reduced cardiac output, arrhythmias, acute kidney injury, incidence of acute respiratory failure admitted to ICU department is ranged 500 patients in the year 2016 affording to the statistical record of Assiut University Hospital [7].
Despite significant technological advances in mechanical ventilator support, the mortality is considerably high, exceeding 40% in many series [8, 9]. other studies also show, despite advances in the management of ARF with mechanical ventilator, death has not decreased significantly and costs continue high [10, 11].
A prospective cohort study conducted in Brazil showed that, among 1732 enrolled patients, 843 (49%) were admitted to an ICU with ARF and the remaining 889 (51%) patients who were admitted without ARF, 141(8%) developed ARF during their stay in the ICU and among total of ARF case (984),475 (48%) died during the ICU stay [12].
A retrospective study showed by the American Journal of Surgery, patients who developed respiratory failure (21%) had a 42% mortality compared with a 6% mortality in patients who did not develop respiratory failure [13]. A prospective cohort study conducted at the Intensive care department, Saint-Louis Hospital University Paris, among 99 patients were admitted for acute respiratory failure, the 30-day mortality rate was 26.2% [14]
In a descriptive study conducted at Assiut University Hospital, the age of patients, admission category to ICU, and cardiac disease were significantly associated with respiratory failure development [7]. A prospective cohort study conducted at Brazilian showed, patients age, type of ICU admission and length of stay in ICU are significantly associated with respiratory failure [12].
A retrospective descriptive chart review was conducted in Addis Ababa, Ethiopia. The finding revealed that respiratory failure was the leading complication or immediate cause of death accounts (32.8%) followed by cardiovascular failure (16.1%) [15].
The objective of this research was to assess the prevalence of respiratory failure and associated factors in adult ICU of St. Paul’s Hospitals Millennium Medical College, and AaBET, Addis Ababa, Ethiopia.
Methods And Materials
Method: An institution based retrospective cross-sectional study was conducted from August 26 to September 25, 2020. Among a total of 2198 population, 384 samples were selected using systematic random sampling. A multivariable logistic regression analysis was used to identify predictors of respiratory failure using odds ratio, 95% confidence interval, and p-value < 0>
Study area and period
This study was conducted in Addis Ababa Ethiopia. Addis Ababa is the capital city of Ethiopia. Addis Ababa is administratively divided into ten sub-cities and 116 districts. Data was collected from two hospitals, namely Saint Paul’s Hospital Millennium Medical College and Addis Ababa Burn, Emergency and Trauma Hospital from August 26 to September 25, 2020.Saint Paul’s Hospital Millennium Medical College is a specialty hospital providing care to the underserved population in the outskirts of Addis Ababa. It currently has 580 beds, with an annual average of 200,000 patients and a catchment population of more than 5 million.
Addis Ababa Burn, Emergency and Trauma Hospital is a newly established 250 bed and 14 ICU bed, teaching and public referral hospital in Addis Ababa, Ethiopia, affiliated with St. Paul’s Hospital Millennium Medical College. Addis Ababa Burn, Emergency and Trauma Hospital provides 24/7 specialty services in emergency medicine, critical care, trauma and acute care surgery, orthopedics, neuro-surgery, and forensic medicine; patients presenting with complaints requiring additional specialty services (example cardiology, gastroenterology) are stabilized and transferred to nearby SPHMMC. There are 40 nurses and 11 mechanical ventilators in ICU.
Sample Size determination
The sample size was estimated using single population proportion formula by assuming the prevalence of respiratory failure is assumed as 50% since there is no previous related study; and desired precision level of 5%, 95% confidence level. For single proportion population,
no=

Where, no=sample size, p=prevalence respiratory failure is 50% and d=margin of error (0.05)
Hence, the sample size was calculated as [no= (Zα/2) ²p (1-p) /d2] = (1.96) ²× (0.5x0.5)/ (0.05) ² = 384. Therefore, the final calculated sample size is 384.
Data Collection Procedures and tools
The checklist for this study was adapted with some modification from a research conducted at Assiut University Hospital [7]. It was first translated from English to Amharic and then retranslated back to English by a linguistic graduate to assure its consistency. The checklist was pretested before the actual data collection. The data collectors were two BSc critical care nurses. The principal investigator and the supervisors were checked for missed values and completeness on daily basis.
Data Management and analysis
This data was entered into Epi data 3.1 and export to SPSS version 24 statistical software packages for cleaning and analysis. Binary logistic regression model was fitted to identify the association between independent versus out-come variable. All independent variables with a p-value of 0.25 and less in the bivariable analysis was entered into multivariable logistic regression models in order to identify independent predictors of respiratory failure. Crude and adjusted odd ratios were computed with their corresponding 95% confidence interval. P-value with < 0.05 was used to declare statistical significance of the results.
Socio demographic Information
Among a total, more than half of respondents 193(50.3%) were male. More than half of the respondent’s’ age distribution, 202(52.6%) were between 18–40 years, 37(9.6%) were in the age group of 41–50 years and the remaining 145(37.8%) were above 50 years of age with a mean age of 43.55 ± 19.49 of standard deviation (Table 1).
Variables (n = 384) | Frequency | Percent (%) |
|---|---|---|
Age group |
|
|
18–40 years | 202 | 52.6 |
41–50 years | 37 | 9.6 |
>50 years | 145 | 37.8 |
Sex |
|
|
Male | 193 | 50.3 |
Female | 191 | 49.7 |
Table 1: Socio-demographic characteristics of respondents who had admitted ICU from September 2014 to August 2020, at Saint Paul’s Hospital Millennium Medical College and Addis Ababa Burn Emergency and Trauma (AaBET) Hospital Addis Ababa, Ethiopia, 2020
Medical, surgical and trauma related characteristics of respondent’s response
This research tried to assess respondent’s admission type, medical, surgical and trauma related characteristics, and their history of diseases condition. In this study the prevalence of respiratory failure was 139(36.2%). Among the total admitted patients, 259(67.4%) were admitted by medical case. Majority of them 319(83.1%) were admitted for the first time. Most of the respondents had history of 291(75.8%) pneumonia, 243(63.3%) sepsis, 209(54.4%) renal and 162(42.2%) cardiac disease respectively (Table 2).
Table 2: Medical, surgical and trauma related characteristics of respondents (n = 384) in adult ICU from September 2014 to August 2020 at SPHMMC and AaBET Hospital Addis Ababa, Ethiopia, 2020
Variables (n = 384) | Frequency | Percent (%) |
|---|---|---|
History of respiratory failure |
|
|
Yes | 139 | 36.2 |
No | 245 | 63.8 |
Admission type to ICU |
|
|
First time admission | 319 | 83.1 |
Recurrent admission | 65 | 16.9 |
History of hypertension |
|
|
Yes | 139 | 36.2 |
No | 245 | 63.8 |
History of diabetes mellitus |
|
|
Yes | 65 | 16.9 |
No | 319 | 83.1 |
History of COPD |
|
|
Yes | 128 | 33.3 |
No | 256 | 66.7 |
History of pneumonia |
|
|
Yes | 291 | 75.8 |
No | 93 | 24.2 |
History of asthma |
|
|
Yes | 60 | 15.6 |
No | 324 | 84.4 |
History of tuberculosis (TB) |
|
|
Yes | 100 | 26 |
No | 284 | 74 |
History of cardiac disease |
|
|
Yes | 162 | 42.2 |
No | 222 | 57.8 |
History of renal disease |
|
|
Yes | 209 | 54.4 |
No | 175 | 45.6 |
Case of ICU admission |
|
|
Medical | 259 | 67.4 |
Surgical | 73 | 19 |
Gynecology | 52 | 13.5 |
History of sepsis |
|
|
Yes | 243 | 63.3 |
No | 141 | 36.7 |
Acute Respiratory Distress Syndrome |
|
|
Yes | 193 | 50.3 |
No | 191 | 49.7 |
History of malignancy/lung cancer |
|
|
Yes | 22 | 5.7 |
No | 362 | 94.3 |
Status of HIV/AIDS |
|
|
Reactive | 39 | 10.2 |
Nonreactive | 345 | 89.8 |
History of trauma/injury |
|
|
Yes | 159 | 41.4 |
No | 225 | 58.6 |
History of anemia |
|
|
Yes | 199 | 51.8 |
No | 185 | 48.2 |
History of pulmonary edema |
|
|
Yes | 73 | 19 |
No | 311 | 81 |
Hx of pulmonary thrombo embolism (PTE) |
|
|
Yes | 44 | 11.5 |
No | 340 | 88.5 |
Regarding duration of ICU stay, more than half of respondents 203 (52.9%) were stay in ICU greater than 15 days, 55(14.3%) of them were stay between 11–15 days, whereas 63(16.4%) of them between 5–10 days and the remaining 63(16.4%) were stay less than five (5) days; with a mean duration of 3.04 ± 1.162 of standard deviation (Figure 1).
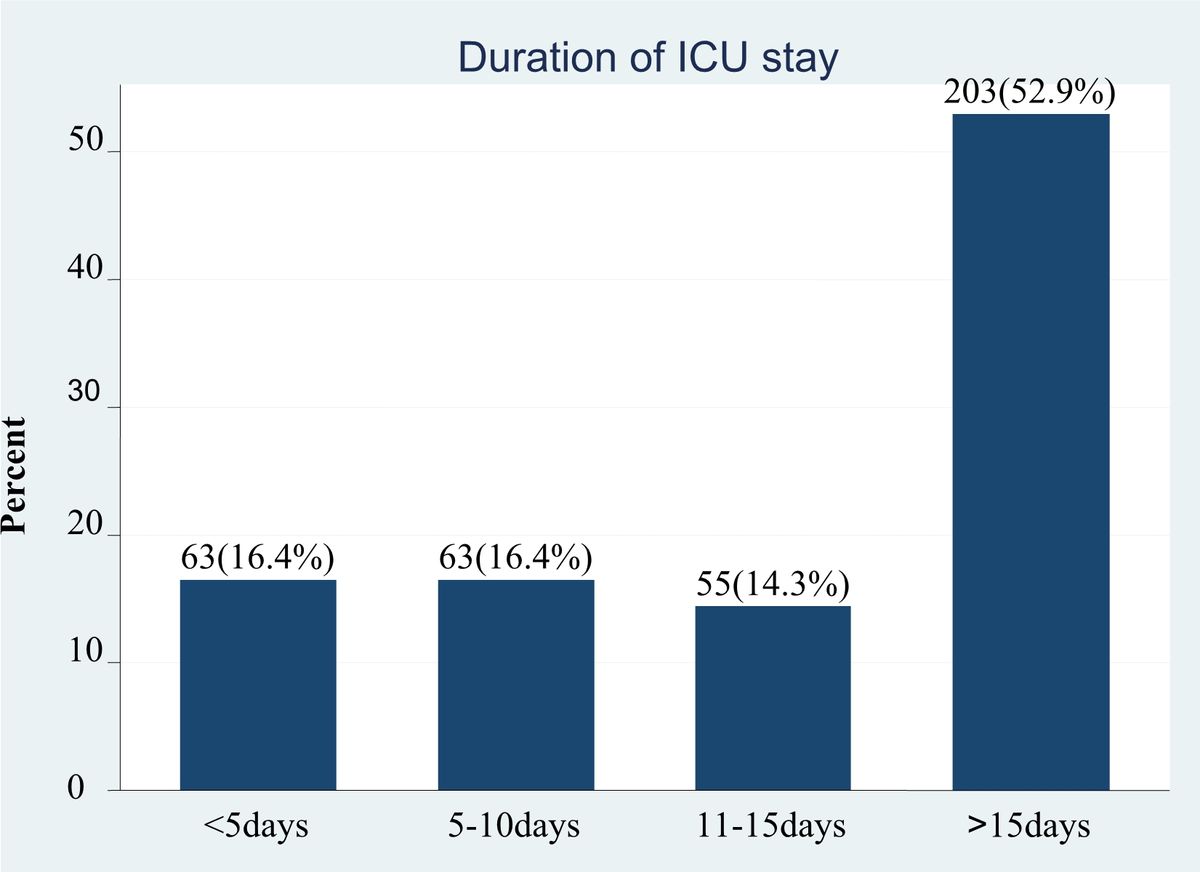
Figure 1: Duration of stay in adult intensive care unit at Saint Paul’s Hospital Millennium Medical College and Addis Ababa Burn, Emergency and Trauma Hospital from September.2014 to August 2020.
Factors associated with respiratory failure
In simple binary logistic regression age, duration of ICU stays, COPD, TB, Cardiac disease, Renal disease, Asthma, case of ICU admission, sepsis, ARDS, HIV, pulmonary edema and trauma were significantly associated with respiratory failure at p-value less than 0.25. In multivariable logistic regression age > 50 years, duration of stay > 15 days, COPD, CHD, Asthma, sepsis, HIV and trauma were significant at p-value less than 0.05 and 95% confidence interval.
Age of the respondent was significantly associated with respiratory failure of intensive care unit patient. Patients whose age greater than > 50 years were 5 times more likely to develop respiratory failure than patients whose age between 18–40 years (AOR = 4.88(95%CI: 2.1, 11.4). Patients who stayed more than 15 days of duration in intensive care unit were 76% (AOR = 0.24(95%CI: 0.086,0.65) less likely to develop respiratory failure as compared to the patients who’s stayed less than 5 days duration.
Patients who had history of chronic obstructive pulmonary disease were 2 times more likely develop respiratory failure as compared to patients who had not history of chronic obstructive pulmonary disease (AOR = 2.3(95%CI: 1.98, 4.79) (Table 3). Patients who had history of asthma were 77% (AOR = 0.23(95%CI: 0.087, 0.6) less likely to develop respiratory failure compared to patients who had no history of asthma. Patients who got cardiac disease were 3 times more likely to develop respiratory failure as compared to patients who did not have cardiac disease (AOR = 3.01(95%CI: 1.36, 6.66) (Table 3).
Regarding to history of sepsis, patients who had sepsis were 57% (AOR = 0.43(95%CI: 0.2, 0.94) less likely to develop respiratory failure than patients who had no history of sepsis. Patients who were HIV reactive were 4 times more likely to develop respiratory failure as compared to patients who were HIV non-reactive patients (AOR = 4.3(95%CI: 1.34, 13.92). Patients who had history of trauma were 3 times more likely to develop respiratory failure as compared to patients who were had not history of trauma (AOR = 2.93(95%CI: 1.36, 6.35) (Table 3).
| Variable | Respiratory failure | COR(95%CI) | AOR(95% CI) | P-value | |
| Yes | No | ||||
| Age group | |||||
| 18–40 years | 34(8.9) | 168(43.8) | 1 | 1 | |
| 41–50 years | 7(1.8) | 30(7.8) | 1.15(0.47,2.84) | 0.96(0.27,3.37) | 0.95 |
| > 50 years | 98(25.5) | 47(12.2) | 10.3(6.2,17.1) | 4.88(2.1,11.4) | 0.0001** |
| Duration of stay | |||||
| < 5 days | 20(5.2) | 43(11.2) | 1 | 1 | |
| 5–10 days | 15(3.9) | 48(12.5) | 0.67(0.31,1.47) | 0.5(0.16,1.51) | 0.22 |
| 11–15 days | 19(5) | 36(9.4) | 1.14(0.53,2.45) | 1.77(0.63,4.96) | 0.28 |
| > 15 days | 85(22.1) | 118(30.7) | 1.55(0.85,2.82) | 0.24(0.086,0.65) | 0.005** |
| History of COPD | |||||
| Yes | 74(19.3) | 54(14.1) | 4.02(1.5,8.4) | 2.3(1.98,4.79) | 0.0001** |
| No | 65(17) | 191(49.6) | 1 | 1 | |
| History of asthma | |||||
| Yes | 13(3.4) | 47(12.2) | 0.44(0.23,0.84) | 0.23(0.087,0.6) | 0.001** |
| No | 126(32.8) | 198(51.6) | 1 | ||
| TB | |||||
| Yes | 45(11.7) | 55(14.3) | 1.65(1.04,2.63) | 2.03(0.87,4.75) | 0.1 |
| No | 94(24.5) | 190(49.5) | 1 | 1 | |
| Cardiac disease | |||||
| Yes | 98(25.5) | 64(16.7) | 6.76(4.26,10.74) | 3.01(1.36,6.66) | 0.006** |
| No | 41(10.7) | 181(47.1) | 1 | 1 | |
| Renal failure | |||||
| Yes | 103 (26.9) | 106 (27.7 ) | 3.86(2.44, 6.11) | 0.77(0.36,1.64) | 0.5 |
| No | 35(9.1) | 139 (36.3) | 1 | 1 | |
| Cases of admission | |||||
| Medical | 102(26.6) | 157(40.9) | 2.16(1.08,4.32) | 0.84(0.28,2.49) | 0.75 |
| Surgical | 25(6.5) | 48(12.5) | 1.73(0.78, 3.89) | 0.97(0.28,3.37) | 0.95 |
| Gynecology | 12(3.13) | 40(10.4) | 1 | 1 | |
| Sepsis | |||||
| Yes | 101(26.3) | 142(37) | 1.92(1.23,3.03) | 0.43(0.2,0.94) | 0.034** |
| No | 38(9.9) | 103(26.8) | 1 | 1 | |
| ARDS | |||||
| Yes | 94(24.5) | 99(25.8) | 3.1(2, 4.77) | 0.52(0.23,1.15) | 0.11 |
| No | 45(11.7) | 146(38) | 1 | 1 | |
| HIV status | |||||
| Reactive | 20(5.2) | 19(5) | 2(1.03,3.9) | 4.3(1.34,13.92) | 0.014** |
| Non-reactive | 119(31) | 226(58.8) | 1 | 1 | |
| Trauma | |||||
| Yes | 99(25.8) | 60(15.6) | 7.6(4.78,12.2) | 2.93(1.36,6.35) | 0.006** |
| No | 40(10.4) | 185(48.2) | 1 | 1 | |
| Pulmonary edema | |||||
| Yes | 32(8.3) | 41(10.7) | 1.49(0.89,2.5) | 1.7(0.74,3.93) | 0.21 |
| No | 107(27.9) | 204(53.1) | 1 | 1 | |
| Where: 1 = reference, ** Significant at p-value of ≤ 0.05 | |||||
Table 3: Multivariable logistic regression analysis of factors associated with respiratory failure in adult ICU at SPHMMC and AaBET Hospital Addis Ababa, Ethiopia, 2020
Discussion
Our study aimed to assess the prevalence of respiratory failure and its associated factors using 384 samples among a total of 2198 population admitted in adult intensive care unit from September 2014 to August 2020 at SPHMMC and AaBET Hospital Addis Ababa, Ethiopia.
The study reveals that, the prevalence of respiratory failure was 139(36.2%). The finding of this study is lower than the previous studies which was 57% (12) and (58%). (8) However, this study was slightly higher compared than the previous study which was (35%). (16) The difference might be due to methodological variations and differences in sociocultural, economical, health and health provision consumption characteristics between respondents of the referenced areas and the study place.
The finding of our study shows that, respondent’s age category 50 and above were more likely to develop respiratory failure than respondents age category between 18 and 40 years. This study was consistent with the previous three studies. (12, 17, 18)
Regarding to duration in ICU stay, this finding revealed that patients stay fifteen (15) and above were 76% less likely to develop respiratory failure as compared to the patients whose stayed less than 5 days duration. This was in line with a previous study that reported patients stay longer time in ICU increase respiratory failure development. (12, 19) However in contrast with this finding, patients stay in ICU between five and teen were more likely develop respiratory failure. (20) The difference could be due to methodological variation (study design, exclusion and inclusion criteria), sociocultural difference, health service quality and study area.
The present finding revealed that, past history of chronic pulmonary disease, cardiac disorder and trauma was indicated the risk factors associated with respiratory failure. This is agreement with the previous finding. (21) Other studies also compatible with the present study, founded that COPD is the main risk factor of ARF. (20, 22)
Regarding to profile of sepsis, the present study indicated that patients who have sepsis were 57% less likely to develop respiratory failure than patients who had no history of sepsis. This was similar with the previous study which was reported that common risk factors for ARF include sepsis. (23)
This study showed that, patients who have history of asthma were 77% less likely to develop respiratory failure compared to patients who had no history of asthma. This was inconsistent with the previous study. (20) The difference might be due to sociocultural (life style) difference of the population, variation in study area and methodology.
Result
The prevalence of respiratory failure in this study was 139(36.2%).The variables which were significantly associated with respiratory failure were, patients age >50 (AOR =4.88(95%CI: 2.1, 11.4),Duration of stay at intensive care unit >15 days (AOR=0.24(95%CI: 0.086, 0.65), prolonged obstructive pulmonary disease (AOR=2.3 (95%CI: 1.98, 4.79),Asthma (AOR=0.23(95%CI: 0.087, 0.6) , sepsis (AOR= 0.43 (95% CI:0.2,0.94) , cardiac disease (AOR= 3.01(95%CI: 1.36, 6.66)), Human Immune Deficiency Virus (AOR=4.3(95%CI: 1.34, 13.92) and trauma (AOR= 2.93(95%CI: 1.36, 6.35).
Conclusion
This study conducted that, patients with older age, prolonged length of ICU stay and previous history of chronic obstructed pulmonary disease, cardiac disease, asthma, sepsis, status of HIV and trauma have an increased risk of respiratory failure. More attention should be paid to prevent those leading factors in order to minimize the magnitude and the burden of respiratory failure.
Declarations
Ethical consideration
Ethical clearance was obtained from Saint Paul’s Hospital Millennium Medical College Institute of Health Ethical Review Board. Information about the study was given to the selected participants in order to obtain their written consent before administering the questionnaires. Participants were informed that they have the right to discontinue or refuse to participate in the study. Answers to any question were completely confidential and the privacy of the respondents was maintained. All methods were performed in accordance with the relevant guidelines and regulations.
Availability of data and materials
Data will be available upon request from the corresponding author
Competing interests
The authors declare that they have no competing interests
Funding
All funding of this original research process covers by all authors
Funding for Publication
Not applicable
Consent for Publication
Not applicable
Authors’ contributions
GB, YK and MB were involved in conception, designing methods, analysis, interpretation and drafting of the manuscript. KG and YK were participated in write-up of the manuscript. All authors have reviewed and approved the submission of the manuscript.
Authors’ detail
Yohannes Koster: MPH, Public Health expert, Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Melke Bimrew: MSc in oncology, Lecturer, Department of nursing, Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Kindalem Gbeyehu: Department of emergency and critical care, faculty of health science, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Acknowledgment We would like to thank Saint Paul’s Hospital Millennium Medical College for the support for the realization of this finding. Special thanks and appreciation to all those who agreed to participate in this study, mainly respondents, data collectors and supervisors.
References
- Wallbridge P, Steinfort D, Tay TR, Irving L, Hew M. (2018), Diagnostic chest ultrasound for acute respiratory failure. Respir Med. 141:26–36.
View at Publisher | View at Google Scholar - Rittayamai N, Katsios CM, Beloncle F, Friedrich JO, Mancebo J, et al. (2015), Pressure-controlled vs volume-controlled ventilation in acute respiratory failure: a physiology-based narrative and systematic review. Chest. 148(2):340–55.
View at Publisher | View at Google Scholar - Slutsky AS. (2015), History of mechanical ventilation. From Vesalius to ventilator-induced lung injury. Am J Respir Crit Care Med. 191(10):1106–1115.
View at Publisher | View at Google Scholar - Scala R. (2012), Respiratory high-dependency care units for the burden of acute respiratory failure. Eur J Intern Med. 23(4):302–8.
View at Publisher | View at Google Scholar - Keenan SP, Mehta S. (2009), Noninvasive ventilation for patients presenting with acute respiratory failure: the randomized controlled trials. Respir Care. 54(1):116–26.
View at Publisher | View at Google Scholar - Guidet B, Flaatten H, Boumendil A, Morandi A, Andersen FH, et al. (2018), Withholding or withdrawing of life-sustaining therapy in older adults (≥ 80 years) admitted to the intensive care unit. Intensive Care Med. 44(7):1027–1038.
View at Publisher | View at Google Scholar - Azza Farhan Amer1 AOMMAAEA. (2019), Prevalence and Risk Factors Leading to Acute Respiratory Failure among Critically Ill Patients at Assiut University Hospital. Assiut Scientific Nursing Journal. 7(17).
View at Publisher | View at Google Scholar - Lobo SM, Lobo FR, Lopes-Ferreira F, Bota DP, Melot C, et al. (2006), Initial and delayed onset of acute respiratory failure: factors associated with development and outcome. Anesth Analgesia. 103(5):1219–1223.
View at Publisher | View at Google Scholar - Wind J, Versteegt J, Twisk J, van der Werf TS, Bindels AJ, et al. (2007), Epidemiology of acute lung injury and acute respiratory distress syndrome in The Netherlands: a survey. Respir Med. 101(10):2091–2098.
View at Publisher | View at Google Scholar - Carson SS, Cox CE, Holmes GM, Howard A, Carey TS. (2006), The changing epidemiology of mechanical ventilation: a population-based study. J Intensive Care Med. 21(3):173–182.
View at Publisher | View at Google Scholar - Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, et al. (2010), The epidemiology of mechanical ventilation uses in the United States. Crit Care Med. 38(10):1947–1953.
View at Publisher | View at Google Scholar - Franca SA, Junior CT, Hovnanian ALD, Albuquerque ALP, Borges ER, et al. (2011), The epidemiology of acute respiratory failure in hospitalized patients: a Brazilian prospective cohort study. J Crit Care. 26(3):330. e1-. e8.
View at Publisher | View at Google Scholar - Money SR, Rice K, Crockett D, Becker M, Abdoh A, et al. (1994), Risk of respiratory failure after repair of thoracoabdominal aortic aneurysms. Am J Surg. 168(2):152–155.
View at Publisher | View at Google Scholar - Azoulay E, Alberti C, Bornstain C, Leleu G, Moreau D, et al. (2001), Improved survival in cancer patients requiring mechanical ventilatory support: impact of noninvasive mechanical ventilatory support. Crit Care Med. 29(3):519–525.
View at Publisher | View at Google Scholar - Getnet M. (2015), Assessment of Mortality Pattern Among Patients Admitted to Medical Icu in Tash During the Last Five Years (sEP2009-aUG2014). Addis Ababa, Ethiopia: Addis Ababa University.
View at Publisher | View at Google Scholar - Vincent J-L, De AS A, Haji-Michael P, Sprung C, Moreno R, et al. (2002), The epidemiology of acute respiratory failure in critically ill patients. Chest. 121(5):1602–1609.
View at Publisher | View at Google Scholar - Burgos J, Luján M, Larrosa MN, Fontanals D, Bermudo G, et al. (2014), Risk factors for respiratory failure in pneumococcal pneumonia: the importance of pneumococcal serotypes. Eur Respir J. 43(2):545–553.
View at Publisher | View at Google Scholar - Herridge MS, Chu LM, Matte A, Tomlinson G, Chan L, et al. (2016), The RECOVER program: disability risk groups and 1-year outcome after 7 or more days of mechanical ventilation. Am J Respir Crit Care Med. 194(7):831–844.
View at Publisher | View at Google Scholar - Vincent J-L, Akça S, De Mendonça A, Haji-Michael P, Sprung C, et al. (2002), The epidemiology of acute respiratory failure in critically ill patients. Chest. 121(5):1602–1609.
View at Publisher | View at Google Scholar - Amer AF, Mohamed AO, El–Aziz A, Anwar M. (2019), Prevalence and Risk Factors Leading to Acute Respiratory Failure among Critically Ill Patients at Assiut University Hospital. Assiut Sci Nurs J. 7(17):81–93.
View at Publisher | View at Google Scholar - Sarkar M, Niranjan N, Banyal P. (2017), Mechanisms of hypoxemia. Lung India: official organ of Indian Chest Society. 34(1):47.
View at Publisher | View at Google Scholar - Avolio AW, Gaspari R, Teofili L, Bianco G, Spinazzola G, et al. (2019), Postoperative respiratory failure in liver transplantation: risk factors and effect on prognosis. PLoS ONE. 14(2): e0211678.
View at Publisher | View at Google Scholar - de Prost N, Pham T, Carteaux G, Dessap AM, Brun-Buisson C, et al. (2017), Etiologies, diagnostic work-up and outcomes of acute respiratory distress syndrome with no common risk factor: a prospective multicenter study. Ann Intensiv Care. 7(1):69.
View at Publisher | View at Google Scholar
