

Research Article | DOI: https://doi.org/10.31579/2834-8486/004
Prevalence Of Anemia and Associated Risk Factors Among Type 2 Diabetic Mellitus Patients Attending Ambo Town Government Hospitals in West Shewa, Ethiopia
- Jafero oljira
- Fekadu Urgessa *
- Mintewab Hussein
Department of Medical Laboratory Sciences, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia.
*Corresponding Author: Fekadu Urgessa, Department of Medical Laboratory Sciences, College of Health Science, Addis Ababa University, Ethiopia.
Citation: Oljira J., Urgessa F. and Hussein M. (2022). Prevalence Of Anemia and Associated Risk Factors Among Type 2 Diabetic Mellitus Patients Attending Ambo Town Government Hospitals in West Shewa, Ethiopia. Biomedical and Clinical Research. 1(1); DOI:10.31579/2834-8486/004
Copyright: © 2022 Fekadu Urgessa, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 September 2022 | Accepted: 21 September 2022 | Published: 04 October 2022
Keywords: anemia; diabetes; renal disease
Abstract
Background: Anemia is the most common blood disorder and common complications of Diabetes mellitus. It is also a global public health problem affecting both developing and developed countries with major consequences for human health, social and economic development. In Ethiopia, chronic illnesses are tremendously rising with their complications, but very little research has been conducted, particularly on anemia among type two diabetic mellitus patients.
Objective: To assess the prevalence of anemia and associated risk factors among type 2 diabetic patients attending Ambo town government Hospitals in West Shewa, Ethiopia from September – October 2020 G.C.
Method: A Hospital-based cross-sectional study was conducted on T2DM patients from September - October 2020. A simple random sampling technique was used to select 356 patients. Data were collected by face-to-face interviews, Administered Questionnaires, and Other Biological Samples such as, blood and urine from 356 patients. Data was entered to EPI-info and exported to SPSS software package for further analysis, Bivariate and multivariate logistic regression models were fitted; Crude Odds Ratio and Adjusted Odds Ratio with 95 Percentage Confidence Interval (CI) were computed. In all cases, P-value less than 0.05 is taken as statistically significant.
Results: The study showed that 27.5 Percentage of participants were anemic. Out of anemic T2DM patients, 92 (92.9 Percentage) and 7 (7.1 Percentage) had mild and moderate anemia, respectively. Having nephropathy (AOR = 6.2, CI: 1.82, 21.16), being male (AOR = 4.32, CI: 1.09, 517.03), duration of diabetes for 5 years and greater (AOR = 4.42, CI: 1.27, 15.45) and having high serum creatinine (AOR=10.07, CI: 2.89, 35.2) were all significantly associated with anemia.
Conclusion: The magnitude of anemia was 27.5 Percentage among T2DM patients in the study area. Therefore, routine screening of anemia for all T2DM patients assisting in early identification and improved management of diabetes will lead to improved quality of life in this patient population.
Abbreviations and Acronyms
ACE: Angiotension Converting Enzyme
AOR; Adjusted Odds Ratio
BMI: Body Mass Index
BP: Blood Pressure
CKD: Chronic Kidney Disease
EDTA: Ethylenediamine tetra acetic acid
DM: Diabetes Mellitus
eGFR: Estimated Glomerular Filtration Rate
Hgb: Hemoglobin
IL: Interleukin
K/DOQI: Kidney disease outcomes quality initiatives
MDRD: Modification of diet in renal disease
SOP: Standard Operating Procedure
SST: Serum Separation Tube
T2DM: Type two Diabetes Mellitus
WHO: World health organization
Introduction
Anemia is the most common blood disorder and a common finding in patients with diabetes. It is also considered a key indicator of chronic kidney disease and an important cardiovascular risk factor [1]. Patients with diabetes mellitus are also twice as likely to have anemia as those with renal impairment from other causes. Furthermore, declining hemoglobin levels may be observed before changes in renal function [2]. It results from diminished erythropoietin production and to a lesser degree due to the increased excretion of erythropoietin in urine [3]. Growing evidence indicates that anemia in T2DM patients is a strong and independent indicator of increased risk for diabetes-related macro-vascular and micro-vascular complications. It causes early occurrence and rapid progression of complications like diabetic nephropathy, diabetic retinopathy, diabetic neuropathy, end-stage renal diseases, ischemic heart disease, and non-healing diabetic foot ulcer [4]. Evidence indicates that the incidence and prevalence of anemia in patients with diabetes is typically associated with erythropoietin deficiency due to concomitant renal disease [5, 6].
Furthermore anemia is a common complication of diabetes mellitus, and the risk of anemia in diabetic patients is estimated to be two to three times higher than that of patients without diabetes [7]. The risk of developing anemia in patients with diabetes and renal disease is significantly greater, and is often more severe, and occurs earlier than in non-diabetic patients with renal diseases [8, 9]. Recent studies have demonstrated the unfavorable influence of anemia on the progression of renal disease, cost of managing the disease, quality of life and cardiovascular disease, and all-cause mortality in diabetic patients who also have renal disease and the combination of anemia and kidney disease in diabetics identifies a group with adverse outcomes [10–12]. There are, however, other factors that could contribute to the development of anemia in diabetes, including chronic inflammation, oxidative stress, autonomic neuropathy, nutritional deficiencies (iron, folate, and vitamin B12), autoimmune diseases, drugs, and advanced glycation [5,13].
Anemia is a global public health problem affecting both developing and developed countries with major consequences for human health as well as social and economic development. It occurs at all stages of the life cycle [4] and affects nearly two billion (27 Percentage) people worldwide [14]. Globally, the prevalence of concurrent anemia and diabetes mellitus (both type1 and type2) ranges from 14 Percentage to 45 Percentage in various ethnic populations worldwide [9]. The magnitude of anemia among T2DM patients varies among studies and regions, ranging from 7.7 Percentage in the United States of America (USA) to 67 Percentage in India [15- 20].
The cause of anemia in diabetes is multi-factorial and includes nutritional deficiencies, inflammation, concomitant autoimmune diseases, advanced age; lower Body Mass Index (BMI), longer duration of diabetes, peripheral vascular disease, specific medications, and hormonal changes in addition to kidney disease [21–24]. Various studies revealed the development of anemia in T2DM patients is significantly associated with sex [25- 27], age [26-28], marital status [21], educational status [28], BMI, hypertension, hematological diseases [40], glycemic control, gastrointestinal disorders, and chronic kidney diseases [3]. The duration of diabetes [26] and microvascular complications of diabetes such as diabetic nephropathy, neuropathy, and retinopathy [26, 28-33] have all found to be significantly associated with anemia in T2DM patients.
In spite of many types of research were done on the prevalence of anemia among T2DM, anemia in T2DM remains unrecognized and untreated in 25 Percentage of the diabetic patients [21, 34] because both share similar symptoms such as lethargy, pale skin, chest pain, irritability, numbness/coldness in the hands and feet, tachycardia, shortness of breath and headache [23]. Our country, Ethiopia is one of the developing countries where both anemia and diabetes mellitus are major public health issues [35, 36] with an increased incidence of DM, [2] it becomes mandatory to be aware of such co-morbidities at the earliest. Therefore, this study will aim to incorporate anemia screening in the Guideline on the management of diabetes and to determine the prevalence of anemia and its associated risk factors among patients with type 2 diabetic mellitus patients attending Ambo town government Hospitals, West Shewa, Ethiopia.
Methods
Study area, period and Design
The study was conducted at Ambo town in government hospitals, west shewa, Oromia, Ethiopia. Ambo town is located 115km from the capital city of Ethiopia, Addis Ababa. A hospital-based cross-sectional study was conducted at Ambo town in government hospitals from September - October 2020 G.C. The source population includes all type two diabetic patients seeking healthcare services at Ambo town government hospitals. The study population includes all type two diabetic patients seeking healthcare services at Ambo Town Government Hospitals for follow-up from September through October 2020 G.C.
Inclusion and Exclusion Criteria
Inclusion Criteria
Patients with diagnosed type 2 diabetes, irrespective of gender and aged 18 years or above were included.
Exclusion Criteria
Participants, who are seriously ill, and unable to stand and sit without assistance or support, were excluded from the study because it is difficult to get an appropriate and accurate measurement from these patients.
Study Variable
Dependent Variables
Prevalence of anemia
Independent Variables
Socio-demographic characteristics: Age, Sex, Marital status, Occupational status, Educational status, and Residence
Lifestyle characteristics: Cigarette smoking, alcohol consumption, physical activity, Nutritional status (Body Mass Index or BMI)
Clinical conditions: Duration of diabetes(in years), medications taken for diabetes, medications taken for diseases other than diabetes, types of diseases for which other medications taken, Neuropathy, Retinopathy, Nephropathy, history of hypertension, HIV status, history of blood loss, Glycemic control, Systolic blood pressure(mmHg), Diastolic blood pressure(mmHg), Serum creatinine and Urine albumin.
Sample size Calculation
By Using Single proportion sample size determination, the sample size was estimated assuming a prevalence of anemia of 34.8 Percentage based on a previous study in people with diabetes in Harari Region Eastern Ethiopia [39], a precision of 5 Percentage and a z value of 1.96. By adding 10 Percentage for non-respondent a total of 383 participants were required. A simple random sampling procedure was used to select the study subjects. Patients with missing the clinical data were excluded, leaving 356 patients for the final analysis.
Data Collection and Laboratory Measurement
Data were collected by using a semi-structured questionnaire. Four data collectors (two nurses and two laboratory professionals) were collect the data. The collected information includes Socio-demographic characteristics, clinical characteristics, anthropometric measurements, and laboratory analysis. Socio-demographic data and clinical characteristics like duration of DM were collected using an interview guide; whereas the presence of diabetes-related complications like; retinopathy, neuropathy, nephropathy, and other complication; history of hypertension and current diabetic medications were collected from reviewing of patient’s medical records. The Duration of Diabetes is categorized as less than five years and greater than or equal to five years [39]. Four consecutive fasting blood glucose measurements, including measurement at the time of the data collection period, were also recorded from the patient’s medical records for calculating the mean blood glucose level. Anthropometric measurements such as weight (kg) and height (m) were measured according to WHO recommendations. The body mass index (BMI) was computed as weight in kilograms divided by the square of the height in meters (kg/m2). The BMI of the participants were classified as: underweight less than 18.5 kg/m2, normal (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), and obese (greater 30 kg/m2) [4]. Blood pressure (BP) was measured by using a manual sphygmomanometer after 10 mins of rest in a sitting position Hypertension was defined as Systolic Blood Pressure (SBP) ≥140 mmHg and/or Diastolic Blood Pressure (DBP) ≥90 mmHg [40]. For laboratory data, from each participant, five mL of venous blood was collected under aseptic conditions by venous puncture from the vein using a disposable syringe for hemoglobin determination, and serum creatinine analysis. Hemoglobin (Hgb) values were calculated by using a hematology analyzer, mission hemoglobin meter. Serum creatinine was analyzed by BS-200 Analyzer chemistry analyzer computed and as mg/dl. Serum creatinine values were considered abnormal if values of serum creatinine analysis were greater than 1.2 mg/dl [4]. Good glycemic control: an average of four consecutive fasting blood glucose measurements was less than or equal to 130 mg/dl and Poor glycemic control: an average of four consecutive fasting blood glucose measurements was greater than130 mg/d [40]. Urine samples were collected from the participating patients to detect the presence of albumin which indicates abnormal and the absence of albumin indicates that normal by using dipsticks [2].
Data Quality Assurance
The principal investigator supervised the data collection process. The training was given to the data collectors. The completeness of data collected was checked every day by the principal investigator. The reliability of the study findings is guaranteed by implementing Quality control (QC) measures throughout the whole process of the laboratory works. All materials, equipment, and procedures were adequately controlled.
Pre-analytical:- in this phase, the principal investigator checked the sample quality and its accuracy by checking the patient request with full information and proper labeling, handling, and transportation of the sample. Based on sample acceptance and rejection criteria the sample was evaluated for clot, hemolysis, and lipemic. Any sample with that problem was rejected and also patient request that is not properly filled with necessary patient information and miss-match of sample in identification was rejected.
Analytical phase: - in this phase, the patient specimen was prepared for testing and ends when the test result is interpreted and verified. Doing this the specimen was rechecked for its correct labeling and identifications again by the personnel who analyze the sample. After checking the sample accuracy the personnel checked the machine and by doing daily, weekly, or as-needed maintenance. After doing the maintenance the personnel processed the daily QC.
Post-analytical phase: - Post-analytical quality assurance was insured by using appropriate result formats and registrations.
Data Analysis and Interpretation
The data was entered into “Epi info version 7” and was exported to SPSS version 23 statistical software for analysis and the results were explained by percentages, tables, and frequencies. Chi-squared (x square) test was used for comparison of categorical variables. Multivariate logistic regression analysis was conducted. The crudes odds ratio was computed (COR) and the corresponding adjusted odds ratios (AOR) and 95 Percentage confidence intervals (CI) were used to identify factors independently associated with anemia. In all cases, P-value less than 0.05 is taken as statistically significant.
Operational Definition
Anemia is defined according to the WHO criteria: Hgb concentration less than13 g/dl for males and less than 12 g/dl for females [41]. It was further classified into mild anemia (female: 11–11.9 g/dl; male: 11–12.9 g/dl), moderate anemia (8–10.9 g/dl) and severe anemia ( less than 8 g/ dl) [4].
Results
Socio-demographic characteristics of the participants
A total of 356 Type 2 diabetic patients took part in the study, with a response rate of 92.9 Percentage. The main reasons for the non-response were a failure to follow through, COVID 19, and a refusal to participate. Males made up 195(54.8 Percentage) out of the participants. The average age of the participants was 48.25 years (SD = 11.401), with the dominant 128(36 Percentage) age group was 40-49 years. Out of the total participants 281(78.9 Percentage) were married and 129(36.2 Percentage) government employers. There are 144(40.4 Percentage) participants from the total sample having an educational level college and above and 293(82.3 Percentage) were living in the urban area (Table 1).
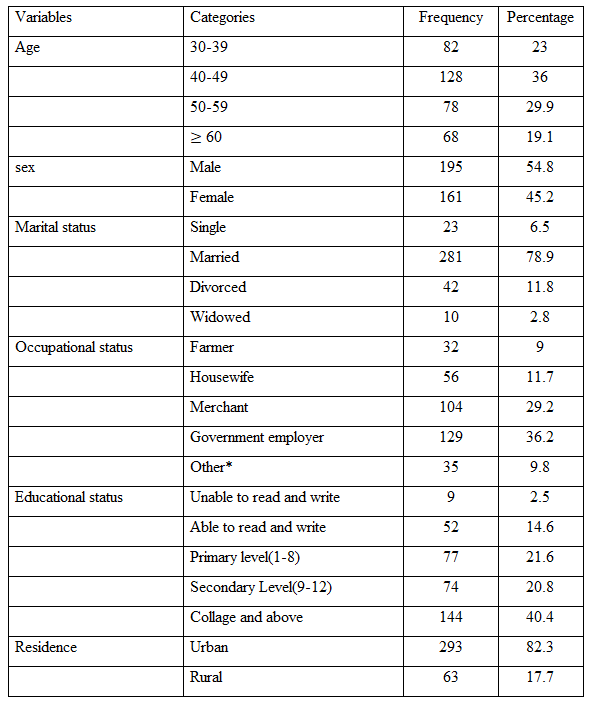
*daily laborers, Non- governmental organization, Driver
Lifestyle of the participants
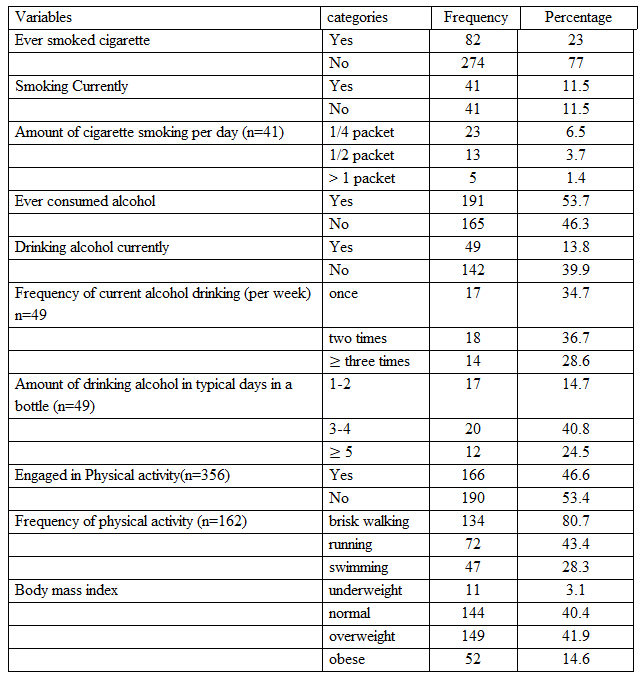
In this study, 82 (23 Percentage) of the participants had smoked cigarettes at least once in their lives, and 41 (11.5 Percentage) of the participants were active smokers. Similarly, 191 (53.7 Percentage) of the study subjects had used alcohol at least once in their lives, and 49 (13.8 Percentage) of the participants were drinking alcohol currently. Most of the participants 18(36.7 Percentage) were drinking two times per week. Of the total study participants, 166(46.6 Percentage) were engaged in physical activity, and walking 134(80.7 Percentage) is the major physical activity used by the participants. The majority of the study subjects were overweight 149 (41.9 Percentage) (Table 2).
Clinical conditions, complications, and co-morbidities of the participants
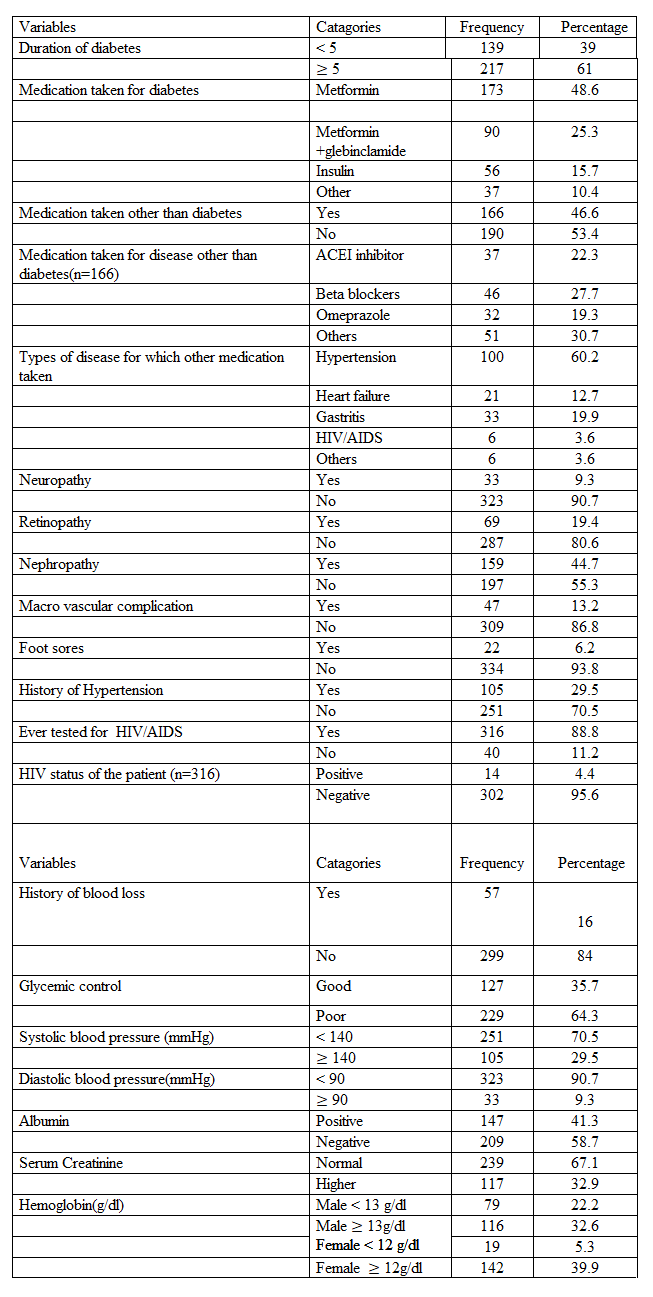
The study showed that the duration of diabetes in most 217 (61 Percentage) of the participants was greater than or equal to5 years. All the patients were taking drugs for the treatment of their diabetes. Metformin was the most commonly used drug. Among the patients, 173(48.6 Percentage) taking it. Besides this, 166(46.6 Percentage) of the patients were taking medication for the management of diseases other than diabetes, and 100(60.2 Percentage) of the patients were taking antihypertensive drugs. Regarding the diabetes-related complications, 33(9.3 Percentage), 69(19.4 Percentage), 159(44.7 Percentage), 47(13.2 Percentage), 22(6.2 Percentage), 105(29.5 Percentage), and 14(4.4 Percentage) of the patients had neuropathy, retinopathy, nephropathy, macro-vascular complication, foot sores, history of hypertension and a history of HIV/AIDS respectively. In addition, 57(16 Percentage) of the patients have a history of blood loss. Of the study participants, 229(64.3 Percentage) of the patients had poor glycemic control. Similarly, 105 (29.5 Percentage) had a systolic blood pressure of greater than or equal to140mmHg, and 33(9.3 Percentage) had a diastolic blood pressure of greater than or equal to 90mmHg. On the other hand, 147 (41.3 Percentage) of the participants had positive urine albumin, and 117 (32.9 Percentage) of the participants had higher or abnormal serum creatinine (Table 3).
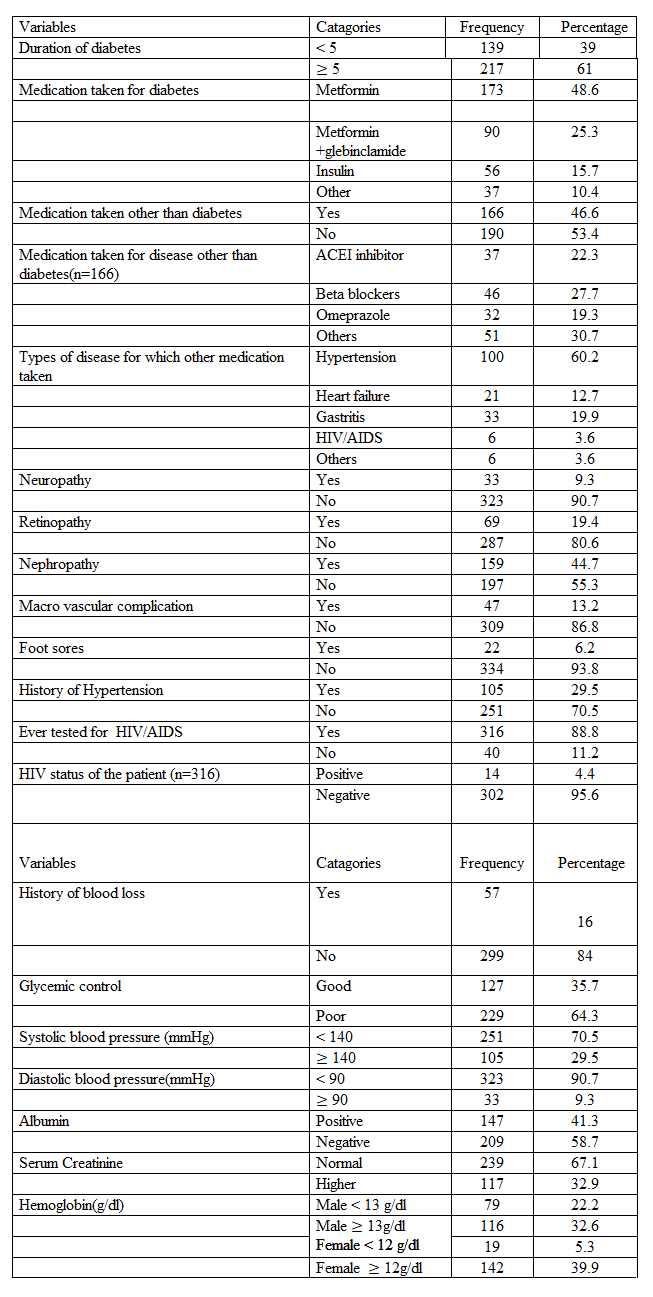
*Glimepiride, Galvusmet,
** Amoxicillin, Ciprofloxacin, nifidipine, lamuvudine, Efaverenz and Tenofovir
*** Pneumonia, Urinary tract infection, Typhoid fever
Magnitude of anemia and associated factors
The results of the hemoglobin test showed that 98 (27.5 Percentage) of the participants were anemic (Table 3). Males (78.6 Percentage) had a higher proportion of anemia than females (22.4 Percentage). Furthermore, it was greatest in patients aged 50 years and above (64.3 Percentage) and lowest in those aged less than 50 years (35.7 Percentage). Out of anemic T2DM patients, 91 (92.9 Percentage) and 7 (7.1 Percentage) had mild and moderate anemia, respectively. To classify variables linked to anemia, bivariate and multivariate analyses were used in binary logistic regression. As a result, having nephropathy, being male, having diabetes for five years or longer, and having a high serum creatinine level were identified as associated factors for anemia in T2DM patients. Male patients were 4.32 times more likely to have anemia than females (AOR = 4.32, CI: 1.09, 517.03). The occurrence of anemia was 6.2 times higher among patients who had nephropathy (AOR = 6.2, CI: 1.82, 21.16). Patients with high serum creatinine (AOR=10.07, CI: 2.89, 35.2) and patients having diabetes for five years and above (AOR = 4.42, CI: 1.27, 15.45) were significantly associated with anemia (Table 4).
Discussion
In this Hospital-based cross-sectional study, the prevalence of anemia and its associated factors among T2DM patients at Ambo Town government hospital, West Shewa Ethiopia, has been assessed. A result of the hemoglobin test showed 27.5 percent of the participants in the study were anemic. Out of anemic T2DM patients, 54 (87 Percentage) and 8 (13 Percentage) had mild and moderate anemia, respectively. Being male, diabetic nephropathy, High serum creatinine, and duration of diabetes greater than or equal to five years were identified as associated factors of anemia among T2DM patients.
Anemia is a common finding in patients with diabetes and harms the patient’s sense of wellbeing; it also impairs the ability to work and reduces the quality of life. Out of the total participants in this study, 27.5 Percentage of the diabetes patients had anemia. This finding is similar to a previous study done in Iran, which showed a 30.4 Percentage prevalence of anemia among diabetes patients [30]. This is also consistent with a study conducted in China and Kuwait which is 22.8 Percentage [29], 29.7 Percentage [42] respectively showed the prevalence of anemia among diabetes patients.
However, it was higher than other study conducted from various regions of the world, in Iran (19.6 Percentage) [33], India (12.3 Percentage) [26], Nigeria (15.3 Percentage) [1], Debre-Berhan (20.1 Percentage) [4], Kuwait (13 Percentage) [43] and Gondar (8.6 Percentage) [40]. These differences might be due to socio-demography, Feeding Habits, duration of DM, and age of the study participant.
On the other hand, the magnitude of anemia in this study was lower compared to the findings of other studies conducted in Brazil (34.2 Percentage) [44], Sub-Saharan Africa (Cameroon) (41.1 Percentage) [28], Pakistan (63 Percentage) [3], Harari Region (34.8 Percentage) [39], Ghana (84.8 Percentage) [45], Egypt (63 Percentage) [46], And United Kingdom (59 Percentage) [47]. These differences might be due to socio-demographic, feeding habits, lifestyle, measurements, duration of DM, age of the study participants, and altitude could all contribute to the variations.
Gender was shown to be significantly associated with anemia in the current study. Male patients were 4.32 times more likely to have anemia than females. Similar findings have been reported in Harari [39], Gonder [40], and the USA [9]. However, another analysis conducted in Pakistan [25] and India contradicted this finding [26]. The possible explanation could relate to the number of anemic type two diabetic female participants in this study is small and many anemic type diabetic females are in the age of menopause.
Even though there is no significant association between anemia and age among type two diabetes, this study showed the prevalence of anemia is greater in older age. This is consistent with other related studies done at the diabetes clinic of Dessie Referral hospital in Northeast Ethiopia [2], Amri Hospital and polyclinics, Kuwait [42], Debre Berhan Referral Hospital (DBRH), North-East, Ethiopia [4], and Australia [48]. This result was anticipated since aging is related to decreased hemoglobin levels and an increase of anemia irrespective of health status [49 and 50]. It also may be related to deficiencies of vitamins such as folate, bone marrow abnormality, and a higher number of co-morbidities, which are common in the elder [48].
In this study, anemia is more prevalent in hypertensive patients, while no significant association between anemia and hypertension by multivariate logistic regression. The main cause could be diabetic patients, the risk of renal impairment, thus increasing the subsequent development of anemia. In addition, nutritional deficiencies especially iron deficiency and chronic inflammation can be the cause [2]. This finding is consistent with a cross-sectional study performed in Ethiopia [2 and 40].
Although drug therapy which is taken for a disease other than diabetes such as, ACE inhibitors and Beta are associated with anemia [2] there is no significant association between anemias and thus drugs in this study. A Descriptive and analytical study done in Brazil [44] showed that there is a significant association between body mass index and anemia this is inconsistent with this study reveals there is no significant association between anemia and body mass index. Another study was done in China [51] and Ethiopia [2] showed that there is a significant association between anemia and high serum creatinine level which contradicts this study.
Anemia was 6.2 times more common in patients with nephropathy, which is consistent with research from Malaysia [31], Iran [30], and Harari [39]. Erythropoietin is a hormone made by the kidney and if the kidney is not working properly, there may not be sufficient hormone produced [39]. Anemia is a well-known complication of diabetes-related chronic kidney disease (CKD) and related to the degree of renal impairment, mainly due to impaired production of erythropoietin by peritubular fibroblast of the kidney [32]. The finding in this study further supports this principle, as the results showed a gradual increase in the prevalence of anemia with a progressive reduction in renal function. There are many potential mechanisms, by which anemia can exist in patients with reduced renal function tests. Damage to erythropoietin-producing cells through either fibrosis or chronic inflammatory activities; tubulointerstitial changes; and autonomic neuropathy, which prevents anemia detection by peritubular fibroblasts of the kidney is the possible mechanism [40, 52, and 53].
The duration of DM is one of the factors linked to the prevalence of anemia in this study. It was observed that a positive relationship between the duration of DM and anemia with a higher chance in patients with greater than or equal to 5 years. Compared with patients with less than 5 years duration of DM, the odds ratio of developing anemia in individuals with greater than or equal to5 years was 4.42 times. This finding is in agreement with the previous studies in Harari Region [39] and Iran [30]. The reason for this increased chance of anemia development with increasing duration of DM may be due to the chronic effects of hyperglycemia. Diabetes-related chronic hyperglycemia can cause a chronic hypoxic milieu in the renal interstitium and disturbance of the interstitial organization of vascular architecture, atypical cell growth, and collagen proliferation in tubular cells and peritubular fibroblasts, which cause the impaired synthesis of erythropoietin by the peritubular fibroblasts [45 and 54].In addition, in patients with prolonged hyperglycemic conditions, the erythrocyte precursors cells in the bone marrow might be exposed to prolonged direct glucose toxicity leading to disturbances in the erythrocyte production [42].
The multivariate analysis of this study showed that having high serum creatinine is independently associated with greater odds for the presence of anemia. A patient with high serum creatinine was 10.07 times more likely to develop anemia and this is consistent with other related studies done in northeast Ethiopia and Ghana [40, 45]. Elevated creatinine level signifies impaired kidney function or kidney disease. As the kidneys become impaired for any reason, the creatinine level in the blood will rise due to poor clearance of creatinine by the kidneys. Abnormally high levels of creatinine thus warn of possible malfunction or failure of the kidneys. Anemia due to renal insufficiency is primarily a result of reduced secretion of EPO by the failing kidneys, and anemia subsequently occurs when creatinine clearance is less than 50 mL/minute. This is observed earlier in patients with diabetes with renal insufficiency or disease [45, 55]. The high incidence of anemia may also be due to other risk factors related to DM. Several studies have reported factors that increase the risk of anemia, which include; damage to renal interstitium due to chronic hyperglycemia and consequent formation of advanced glycation end products by increased reactive oxygen species, and systemic inflammation as well as reduced androgen levels induced by diabetes [45, 55, and 56].
Limitations
The study lacks control groups and did not assess the causes of anemia in diabetic patients; due to the nature of the study design, cross-sectional studies. The other limitation in this study is, morphological classification of anemia was not done due to budget problems.
Conclusions
The study showed that 27.5 Percentage of participants were anemic. In this study anemia is more common in diabetes mellitus particularly in diabetic male’s patients and is a frequent complication of diabetic nephropathy. Out of anemic T2DM patients, 92.9 Percentage and 7.1 Percentage had mild and moderate anemia, respectively. Having nephropathy, being male, duration of diabetes for 5 years and greater, having high serum creatinine were all significantly associated with anemia.
Recommendation
The results suggest all Health institutions or diabetic clinics must incorporate routine screening for anemia in all T2DM patients mainly for patients with these identified risk factors to facilitate early detection and management of anemia among T2DM and consequently improve the overall care of these patients. Keeping diabetes under control and proper investigations to identify anemia in diabetic patients at an early stage can reduce the severity of the complications caused due to anemia in a diabetic population. Diabetic males and patients with nephropathy are the most vulnerable group to anemia, thus care should be taken in terms of their nutrition and supplements. Further studies are needed because of the cross-sectional nature of this study since relationship between anemia and different potential factors affecting it progressively cannot be well established. Thus, a longitudinal study is needed to assess the relationship over time, and to elaborate the mechanisms of anemia in patients with diabetes.
Ethical Considerations
Ethical clearance was obtained from the Addis Ababa University, College of Health Sciences, Department of Medical Laboratory Sciences, Department Research and Ethical Review Committee (DRERC). Permission was obtained from administrators of hospitals involved. The study aim, benefit, risk, and right for withdrawal any time from the study was explained to the study participants, and informed verbal, as well as written consent was obtained from each study participant. Physicians were informed about anemic and renal disease patients for proper management. Samples were coded and confidentiality of patient data was maintained throughout the study. Type two diabetic patients who are with mild anemic 7.1 Percentage were got treatment.
Acknowledgement
First we acknowledge the Department of Medical Laboratory Sciences, College of Health Sciences Addis Ababa University, for giving us the opportunity.
We are thankful to the Ambo University Referral Hospital and Ambo General Hospital staffs specially, lab staffs, Physicians as well as Ambo town health office who contributed much for this thesis writing.
Our heartfelt gratitude also goes to study participants for giving me important information. Last, but not least my thanks also go to data collectors for their fruitful works.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due [we do not have consent from all patients and ethical approval committees to publish this data] but are available from the corresponding author on reasonable request.
Funding
Not applicable
Authors’ contributions
JO, FU, and MH conducted the literature search, collected and analyzed the data, and wrote the manuscript. JO and FU contributed to the conception and design of the study, the interpretation of data, and critically reviewed the manuscript. JO participated in the writing, analysis and data interpretation, in addition to providing critical input to the research. FU conceptualized and designed the study, supervised the survey team and data analysis, participated in data analysis, contributed to the discussion, reviewed and edited the manuscript, and provided critical data interpretation. All authors read and accepted the final manuscript.
References
- Adejumo B., Dimkpa U., Ewenighi C., Onifade A., Mokogwu A., et al.; (2012). Incidence and risk of anemia in type-2 diabetic patients in the absence of renal impairment. Health.2012; 4: 304–308.
View at Publisher | View at Google Scholar - FisehaT., Adamu A., Tesfaye M., Gebreweld A. (2019). Prevalence of anemia in diabetic adult outpatients in Northeast Ethiopia. PLoSONE.; 14(9): e0222111.
View at Publisher | View at Google Scholar - Shams N. and Osmani M.H.; (2015). newly diagnosed anemia in admitted diabetics, frequency, and etiology and associated factors. J Coll Physicians Surg Pak.; 25(4): 242–246.
View at Publisher | View at Google Scholar - M. M. Taderegew, T. Gebremariam, A. A. Tareke, and G. G.Woldeamanuel. (2020). Anemia and its associated factors among type 2 diabetes mellitus patients attending Debre Berhan referral hospital, north-east Ethiopia: a cross-sectional study. Journal of Blood Medicine, vol. 11, p. 47.
View at Publisher | View at Google Scholar - Thomas MC. (2007). Anemia in diabetes: marker or mediator of microvascular disease? Nat Clin Pr Nephrology. 3(1):20–30.
View at Publisher | View at Google Scholar - Thomas MC. (2006). The High Prevalence of Anemia in Diabetes Is Linked to Functional Erythropoietin Deficiency. SeminNephrol. 26:275-282.
View at Publisher | View at Google Scholar - Sahay M., Kalra S., Badani R., Bantwal G., Bhoraskar A., et al. (2017). Diabetes and Anemia: International Diabetes Federation (IDF) Southeast Asian Region (SEAR) position statement. Diabetes Metab Syndr. 11: S685–S695.
View at Publisher | View at Google Scholar - Al-Khoury S., Afzali B., Shah N., Covic A., Thomas S., et al. (2006). Anemia in diabetic patients with chronic kidney disease prevalence and predictors. Diabetologia. 49:1183–1189.
View at Publisher | View at Google Scholar - El-Achkar TM., Ohmit SE., Mccullough PA., Crook ED., Brown WW., et al. (2005). Higher prevalence of anemia with diabetes mellitus in moderate kidney insufficiency: The Kidney Early Evaluation Program. Kidney Inte. 67: 1483–1488.
View at Publisher | View at Google Scholar - Ueda H., Ishimura E., Shoji T., Emoto M., Morioka T., et al. (2003). Factors affecting the progression of renal failure in patients with type2 diabetes. Diabetes Care. 26: 1530–1534.
View at Publisher | View at Google Scholar - Vlagopoulos PT., Tighiouart H., Weiner DE., Griffith J., Pettitt D., et al. (2005). Anemia as a risk factor for cardiovascular disease and all-cause mortality in diabetes: the impact of chronic kidney disease. J Am SocNephrolJASN. 16(11):3403–3410.
View at Publisher | View at Google Scholar - Azmi S., Goh A., Muhammad NA., Tohid H., Rashid MRA. (2017). The Cost and Quality of Life of Malaysian Type 2 Diabetes Mellitus Patients with Chronic Kidney Disease and Anemia. Value Health Reg Issues. 15:42-49.
View at Publisher | View at Google Scholar - Deray G., Heurtier A., Grimaldi A., LaunayVacher V., Isnard Bagnis C. (2004). Anemia and diabetes. Am J Nephrol. 24: 522–526.
View at Publisher | View at Google Scholar - Kassebaum N.J., Global Burden of Disease (GBD) 2013 Anemia Collaborators: (2016). The global burden of anemia. Hematol Oncol Clin North Am. 30: 247–308.
View at Publisher | View at Google Scholar - Thomas M.C., Tsalamandris C., MacIsaac R.J., and Jerums G. (2006). the epidemiology of hemoglobin levels in patients with type2 diabetes. Am J Kidney Dis. 48(4): 537–545.
View at Publisher | View at Google Scholar - Abdulrahman H. and Haridas N. (2017). Anemia in type 2 diabetes patients with and without nephropathy in Anand-Gujarat, India. International Journal of Advanced Research. 5(6): 367–374.
View at Publisher | View at Google Scholar - Gulati M. and Agrawal N.; (2016). Study of prevalence of anemia in patients with type2 diabetes mellitus. Scholars Journal of Applied Medical Sciences. 4(5F): 1826–1829.
View at Publisher | View at Google Scholar - Idris I., Tohid H., Muhammad N.A., Rashid M.R.A., Ahad A.M., et al. (2018). Anaemia among primary care patients with type2 diabetes mellitus (T2DM) and chronic kidney disease:amulti-centered cross-sectional study. BMJOpen. 8.
View at Publisher | View at Google Scholar - Rathod G.B., Parmar P., Rathod S., and Parikh A. (2016). Prevalence of anemia in patients with Type 2 Diabetes Mellitus at Gandhinagar, Gujarat, India. IAIM. 3(3):1 2–16.
View at Publisher | View at Google Scholar - Panda A.K. and Ambade R.A. (2018). Prevalence of anemia and its correlation with HBA1c of patients in type-II diabetes mellitus: a pilot study. Natl J Physiol Pharm Pharmacol. 8 (10):409–1413.
View at Publisher | View at Google Scholar - Abate A., Birhan W., and Alemu A. (2013). Association of anemia and renal function test among diabetes mellitus patients attending Fenote Selam Hospital, West Gojam, and North West Ethiopia: a cross-sectional study. BMC Hematology. 13(1): 6.
View at Publisher | View at Google Scholar - Thomas M.C., Cooper M.E., Rossing K., and Parving H.H. (2006). Anaemia in diabetes: Is there a rationale to TREAT? Diabetologia. 49(6): 1151–1157.
View at Publisher | View at Google Scholar - Bev B. (2009). recognizing anemia in people with diabetes. Association Manager Anemia.
View at Publisher | View at Google Scholar - Bolen S., Wilson L., Vassy J., Feldman L., Yeh J., et al. (2007). Comparative effectiveness and safety of oral diabetes medications for adults with type 2 diabetes. Comparative effectiveness review No.8. (Prepared by Johns Hopkins Evidence-based Practice Center under contract No. 290-02-0018). Rockville, MD: Agency for Health care Research and Quality.
View at Publisher | View at Google Scholar - Sharif A., Younus S., Baig K., Ali NH. (2014). Prevalence and risk of anemia in type-2 diabetic patients. Health. 2014; 6(12):1415.
View at Publisher | View at Google Scholar - Ranil P.K., Raman R., Rachepalli S.R., Pal S.S., Kulothungan V., et al. (2010). Anemia and diabetic retinopathy in type 2 diabetes mellitus. J Assoc Physicians India. 58:91–94.
View at Publisher | View at Google Scholar - Salman M.A. (2015). Anemia in patients with diabetes mellitus: prevalence and progression. General Medicine. 3(1):162.
View at Publisher | View at Google Scholar - Feteh V.F., Choukem S.P., Kengne A.P., Nebongo D.N., and Ngowe-Ngowe M. (2016). Anemia in type 2 diabetic patients and correlation with kidney function in a tertiary care sub-Saharan African hospital: a cross-sectional study. BMC Nephrology. 17: 29.
View at Publisher | View at Google Scholar - He B.B., Xu M., Wei L., Gu Y.J., Han J.F., et al. (2015). Relationship between Anemia and Chronic Complications in Chinese Patients with Type 2 Diabetes Mellitus. Arch Iran Med. 18(5): 277–283.
View at Publisher | View at Google Scholar - Hosseini M.S., Rostami Z., Saadat A., Saadatmand S.M., and Naeimi E. (2014). Anemia and Microvascular Complications in Patients WithType2 Diabetes Mellitus. Nephro Urol Mon. 6(4).
View at Publisher | View at Google Scholar - Thambiah SC., Samsudin IN., George E., et al. (2015). Anaemia in type 2 diabetes mellitus (T2DM) patients in Hospital Putrajaya. Malaysian J Med Health Sci. 11(1):49–62.
View at Publisher | View at Google Scholar - Jones S.C., Smith D., Nag S., Bilous M.T., and Winship S. (2010). Prevalence and nature of anemia in a prospective, population-based sample of people with diabetes: Teesside Anaemia in Diabetes (TAD) study. Diabet Med. 2010; 27(6): 655–659.
View at Publisher | View at Google Scholar - Bonakdaran S., Gharebaghi M., and Vahedian M. (2011). Prevalence of anemia in type two diabetic patients and role of renal involvement. Saudi J Kidney Dis Transp. 22: 286–290.
View at Publisher | View at Google Scholar - Baisakhiya S., Garg P., and Singh S.; (2017). Anemia in patients with type II diabetes mellitus with and without diabetic retinopathy. International Journal of Medical Science and Public Health. 6(2):303-306.
View at Publisher | View at Google Scholar - (2016). Central Statistical Agency (CSA) [Ethiopia] and ICF Ethiopia demographic and health Survey.; Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF.
View at Publisher | View at Google Scholar - Shaw J.E., Sicree R.A., and Zimmet P.Z. (2009). Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Research and Clinical Practice. 2010; 87:4–14.
View at Publisher | View at Google Scholar - (2012). Ambo General Hospital planning and Budget of Ethiopian fiscal year.
View at Publisher | View at Google Scholar - (2012). AmboUniversity Referral Hospital planning and Budget of Ethiopian fiscal year.
View at Publisher | View at Google Scholar - Bekele A., Teji Roba K., Egata G., and Gebremichael B. (2019). Anemia and associated factors among type-2 diabetes mellitus patients attending public hospitals in Harari Region, Eastern Ethiopia. PLoS One. 14(12): e0225725.
View at Publisher | View at Google Scholar - Kebede SA., Tusa BS. and Weldesenbet AB. (2021). Prevalence of Anaemia and Its Associated Factors among Type 2 Diabetes Mellitus Patients in University of Gondar Comprehensive Specialized Hospital. Anemia. 6627979.
View at Publisher | View at Google Scholar - Mehdi U., Toto RD. (2009). Anemia, diabetes, and chronic kidney disease. Diabetes Care. 32(7):13206.
View at Publisher | View at Google Scholar - Samuel TR., Tejaswi N., Kumar P., et al. (2018). Clinical significance of screening for anemia in diabetic patients. Artic Int J Pharm Sci Rev Res. 48(2):20–24.
View at Publisher | View at Google Scholar - Mojiminiyi OA., Abdella NA., Zaki MY., El Gebely SA., Mohamedi HM., et al. (2006). Prevalence and associations of low plasma erythropoietin in patients with Type 2 diabetes mellitus. Diabet Med. 23(8):839–844.
View at Publisher | View at Google Scholar - Barbieri J., Fontela P.C., Winkelmann E.R., Zimmermann C.E.P., Sandri Y.P., et al. (2015). Anemia in Patients with Type 2 Diabetes Mellitus. Anemia.7
View at Publisher | View at Google Scholar - Antwi-Bafour S., Hammond S., Adjei J.K, Kyeremeh R., Martin-Odoom A., et al. (2016). A case-control study of the prevalence of anemia among patients with type 2 diabetes. Journal of Medical Case Reports. 10(110): 2-8.
View at Publisher | View at Google Scholar - Fayed HM., Elsaied AR., Alsenbesy MA., and Moubark IA. (2013). The proportion of anemia in type 2 diabetic patients in qena governorate Case-Control Study: clinical correlates and prognostic significance. Int J of Diabet Res. 2(4):64–75.
View at Publisher | View at Google Scholar - Trevest K., Treadway H., Hawkins-van der Cingel G., Bailey C., Abdelhafiz AH., et al. (2014). Prevalence and determinants of anemia in older people with diabetes attending an outpatient clinic: a cross-sectional audit. Clin Diabetes. 32(4):158.
View at Publisher | View at Google Scholar - Thomas M., Tsalamandris C., MacIsaac R. and Jerums G. (2005). Anaemia in diabetes: an emerging complication of microvascular disease. Curr Diabetes Rev. 1(1):107–126.
View at Publisher | View at Google Scholar - Salive ME., Cornoni-Huntley J., Guralnik JM, et al. (1992). Anemia and hemoglobin levels in older persons: relationship with age, gender, and health status. J Am Geriatr Soc. 40(5):489–496.
View at Publisher | View at Google Scholar - Gaskell H., Derry S., Moore RA. and Mc Quay HJ. (2008). Prevalence of anemia in older persons: a systematic review. BMC Geriatr. 8(1):1.
View at Publisher | View at Google Scholar - Chen CXR., Li YC., Chan SL.,and Chan KH. (2013). Anemia and type 2 diabetes: implications from a retrospectively studied primary care case series. Hong Kong Med J. 19: 214-221.
View at Publisher | View at Google Scholar - McGill JB., Bell DS. (2005). Anemia and the role of erythropoietin in diabetes. J Diabetes Complications. 20(4):262–272.
View at Publisher | View at Google Scholar - Loutradis C., Skodra A., Georgianos P., et al. (2016). Diabetes mellitus increases the prevalence of anemia in patients with chronic kidney disease: a nested case-control study. World J Nephrol. 5(4):358.
View at Publisher | View at Google Scholar - M. Andrews and M. Arredondo. (2012). Ferritin levels and hepcidin mRNA expression in peripheral mononuclear cells from anemic type 2 diabetic patients. Biological Trace Element Research, vol. 149, no. 1, pp. 1–4.
View at Publisher | View at Google Scholar - Thomas MC., MacIsaac RJ., Tsalamandris C., Molyneaux L., Goubina I., et al. (2004). The burden of anemia in type 2 diabetes and the role of nephropathy. A cross-sectional audit. Nephrol Dial Transplant.; 19:1792–1797.
View at Publisher | View at Google Scholar - Bosman DR., Winkler AS., Marsden JT., Macdougall IC., Watkins PJ. (2001). Anemia with erythropoietin deficiency occurs early in diabetic nephropathy. Diabetes Care. 24(3):495–499.
View at Publisher | View at Google Scholar
