

Research Article | DOI: https://doi.org/10.31579/2835-785X/011
Preparation and Evaluation of Topical Formulation of Diphenylcyclopropenone for the Treatment of Alopecia Areata
- Atefeh Naeimifar 1
- Behnaz Daneshmand 3
- Negar Namini 2
- Fatemeh Amiri 3
- Alireza Firooz 3
- Saman Ahmad Nasrollahi 3*
1 Department of Pharmaceutics, Faculty of Pharmacy, Tehran University of Medical Sciences, Tehran, Iran.
2 Drug and Food Control Department, Faculty of Pharmacy, Tehran University of Medical Sciences, Tehran, Iran.
3 Pharmaceutical, Cosmeceutical and Hygienic Formulation Lab, Center for Research & Training in Skin Diseases & Leprosy, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Saman Ahmad Nasrollahi PharmD, PhD, Center for Research & Training in Skin Diseases & Leprosy (CRTSDL), Tehran University of Medical Sciences (TUMS), # 415 Taleqani Ave, Tehran, Iran.
Citation: Atefeh Naeimifar, Behnaz Daneshmand, Negar Namini, Fatemeh Amiri, Saman Ahmad Nasrollahi, et al., (2023), Preparation and Evaluation of Topical Formulation of Diphenylcyclopropenone for the Treatment of Alopecia Areata, J. International Journal of Clinical Research and Reports 2(3); DOI:10.31579/2835-785X/011
Copyright: © 2023, Saman Ahmad Nasrollahi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 June 2023 | Accepted: 19 June 2023 | Published: 26 June 2023
Keywords: alopecia areate; diphenylcyclopropenone; stability study; topical formulation; ICH standards; hair loss
Abstract
Background: Greatly variable results of topical diphenylcyclopropenone (DPCP) in the treatment of alopecia areata have been reported until now.
Objective: The purposes of the present study were to evaluate the stability of DPC in different solutions with two preparation methods and investigate the physicochemical parameters during the stability period.
Methods: Two methods for the preparation of DPCP topical solution were studied. Method A was made by acetone, and the method B method was made by propylene glycol diluted with acetone at the application time. The manufactured solutions were evaluated according to the ICH standards by long-term stability tests of 6 months at 5ºC±3ºC.
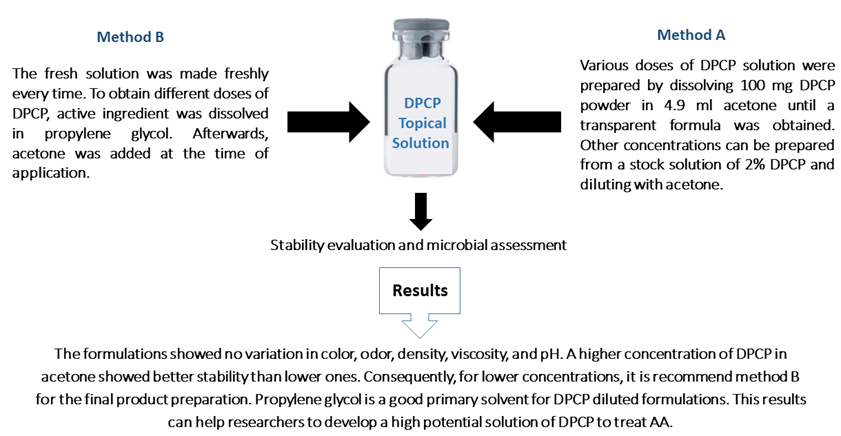
Results: During the period of storage, the formulations showed no variation in color, odor, density, viscosity, and pH. The DPCP solutions in high concentrations, such as 2%, 1%, and 0.5% were entirely stable and appropriate. However, in lower concentrations, including 0.05%, 0.1%, and 0.01%, the assays dropped during 3 months. A higher concentration of DPCP in acetone showed better stability than lower ones. Consequently, for lower concentrations, it recommends method B for the final product preparation. Propylene glycol is a good primary solvent for DPCP diluted formulations.
Conclusion: This result can help researchers to develop a high potential solution of DPCP to treat AA.
1. Introduction
Alopecia areata (AA) is a skin condition of uncertain etiology. However, environmental, immunologic, and genetic factors may play roles in the development of temporary or permanent hair loss. Aa occurs in about 2% of the population and is characterized by limited alopecic patches on the scalp. In cases of AA totalis, patients present total loss of hair on the scalp, and AA universalis is the loss of hair over the body and entire scalp, including the groin, armpits, eyelashes, and eyebrows [1].
Clinically, the skin within the affected areas remains normal. In some patients, changes in nails, such as regular ridging and onycholysis, have been witnessed. Although hair regrowth may happen naturally or after treatment, regrowth is unlikely in the treatment-resistant type of disease. Risk factors that may deteriorate the course of the disease include widespread hair loss, nail involvement, the presence of band-like hair loss, concomitant auto-immune, and atopic diseases, as well as family history of the disease [2, 3].
Dermatosis of the scalp in AA is a problem for many patients and is often resistant even to extensive therapy [4-7]. There is no gold standard for the treatment of AA. Topical and intra-lesional corticosteroid therapy is regularly administered, but the advantage of such treatment is often temporary. Systemic corticosteroid treatment may be effective in some circumstances, but the required maintenance dose is often high [8]. Immunomodulators, such as tacrolimus, pimecrolimus, minoxidil solution, irritant or immunogenic ingredients, and ultraviolet A could also be beneficial [9, 10]. Some achievements have been described with anthralin, but the outcomes seem variable [11, 12].
Other treatments which have been assessed with variable success rates entail cyclosporine a [13-15], alpha-interferon [16], and acupuncture [17]. Moreover, psychotherapy plays a role in the treatment of AA, particularly in patients who have experienced stressful events, have low self-esteem, or whose course of illness is related to stress [18]. Topical immunotherapy is described as the induction of allergic contact dermatitis by applying a potent contact allergen. In 1965, the alkylating agent triethyleneimino benzoquinone was the initial topical sensitizer used to treat cutaneous disease, but it was abandoned due to mutagenicity. Topical immunotherapy, such as squaric acid dibutyl ester, dinitrochlorobenzene, and diphenylcyclopropenone (DPCP), has been used for more than 10 years for severe AA and numerous contact allergens and led to hair regrowth in patients with AA [19-21].
Dpcp, also known as diphencyprone (DPC), is an experimental sensitizing agent commonly used for the treatment of AA with various doses from 2% to 0.0001% [22]. The DPCP is often selected for treating patients with more than 50% of hair loss and demonstrates high efficacy. It is a potent contact allergen in humans and animals with 98%-99% of the cases of AA sensitized to the scalp skin. Rare studies have defined the efficacy of DPCP maintenance treatment with different relapse rates [23-25].
Topical immunotherapy agents have diverse mechanisms of action. Primarily, a decrease in CD4:CD8 lymphocyte count from 4:1 to 1:1 occurs. A theory has suggested a probable interference of contact allergens with the preexisting proinflammatory cytokines and their constant production by follicular keratinocytes [26]. Other investigations noted a decline in elevated IFN-γ levels, a rise in mRNA expression of IL-2, IL-8, and IL-10, as well as TNF-α in the lesional skin. It has also been reported that IL-10 is responsible for the effectiveness of DPCP by inhibiting T lymphocytes. In successfully treated patients, augmented levels of tumor growth factor β were detected [26]. The DCP works by inducing contact dermatitis. The immune system is stimulated causing inflammation on the skin. By diverting the white blood cells away from the hair bulb, the hair can regrow.
The scalp is the normal sensitization site. A cotton-tipped applicator saturated with 2% DPCP in acetone were applied to an area of at least 10 cm2 and left on for 24 h. After that, the patch should be removed by wiping the chemical with a tissue before washing the area in the shower. An itchy area or even blisters will develop in 3-5 days where the DPCP solution was applied and will fade in 2-3 weeks. Patients are guided to avoid the washing area and protect it from sunlight for 48 h. If a patient demonstrates a strong reaction to DPCP, this means that the patient has been successfully sensitized to DPCP.
DPCP has diverse concentrations, including 0.001%, 0.01%, 0.1%, 0.05%, 0.5%, and 1%. The physician chooses the best dose for initiating the treatment after sensitization by different concentrations from lower to higher concentrations. In the treatment course, DPCP will be applied to all bald areas of the scalp once a week. The DPCP will be continued until the bald area has completely regrown, which will usually take several months. The doctor will monitor the patient one month after starting the treatment. The concentration of DPCP will be adjusted according to the response to previous concentrations. When the treatment is deemed successful, the physician will either reduce the frequency and put on a maintenance regime or stop the treatment completely [26].
The formulation and stability data are not available for many specialists and usually, DPCP solutions are prepared in clinics or pharmacies as requested. There are no commercial preparations and no one is concerned about industrialization. Furthermore, there is not enough stability evaluation for DPCP.
The present study aimed to formulate six different concentrations of DPCP solutions by two preparation methods and evaluate the physicochemical parameters during the stability period
.
2. Materials and Methods
The DPCP powder was purchased from ALADDIN Biochemical Technology Co. Ltd (Shanghai, China). Propylene glycol, acetonitrile, and acetone were obtained from Merck (Darmstadt, Germany). For microbial analysis, Sabouraud dextrose agar was purchased from Merck (Germany), and tryptic soy agar, tryptic soy broth, and cetrimide agar were all obtained from Liofilchem (Italy). Borosilicate glass Type 1 Crimp Cap Vial in amber color, bromobuthyl rubber 20 mm, and aluminum seal cap were purchased from Pars Ampoule Company, Parsam Rubber Pharmed, and Ako-Sanat Tejarat Aria Company (Iran), respectively.
2.1. Preparation of DPCP Topical Solutions
We investigated two methods for the preparation of DPCP topical solution. The solutions were filled in borosilicate amber vials as 5 ml in each vial. In the method A, various doses of 0.001%, 0.01%, 0.05%, 0.1%, 0.5%, 1%, and 2% were prepared by dissolving 100 mg DPCP powder in 4.9 ml acetone until a transparent formula was obtained. Further dilution can be prepared by making a stock solution of 2% and diluting it with acetone (Table 1). For example, to prepare a 0.1% solution, 0.25 ml stock solution was mixed with 4.75 ml acetone.
Preparation | Stock solution 2% (ml) | Propylene glycol (ml) | Acetone (ml) | Final requested DPCP solution (%V/V) |
Method A | 2.5 | - | 2.5 | 1 |
1.25 | - | 3.75 | 0.5 | |
0.25 | - | 4.75 | 0.1 | |
0.125 | - | 4.875 | 0.05 | |
0.025 | - | 4.975 | 0.01 | |
0.0025 | - | 4.997 | 0.001 | |
Method B | 0.1 | 0.9 | 4 | 0.1 |
0.05 | 0.95 | 4 | 0.05 | |
0.01 | 0.99 | 4 | 0.01 | |
0.001 | 0.999 | 4 | 0.001 |
Table 1: Dilution from the stock solution DPCP 2% W/W to prepare 5ml various solutions by methods A and B
In method B, the fresh solution was made freshly every time. Therefore, to obtain different doses of 0.001%, 0.01%, 0.05%, and 0.1%, DPCP was dissolved in propylene glycol. Afterwards, acetone was added at the time of application. At first, for preparing 2% DPCP solution as a stock solution, 500 mg DPCP powder was dissolved in 1 ml acetone. Next, 0.2 ml stock solution was taken to the vial and 0.8 ml propylene glycol was added to the vial and was sealed with an aluminum cap until acetone was added to the vial at the usage time. Other concentrations were made by diluting the stock solution. For preparing low concentrations of DPCP solution, such as 0.001%, a laboratory sampler was utilized to provide the exact volume (µl) for each sample.
2.2. Stability Studies
The manufactured solutions were evaluated by long-term stability tests of 6 months at 5ºC±3ºC. Physicochemical analysis of color, odor, density, and pH was performed on months 0, 1, 3, and 6 as mentioned in the ICH stability guideline. Moreover, microbial assessments were also completed.
2.2.1. Density
The density of a material is defined as mass per unit volume. The precise volume of the pycnometer was measured by filling it with water and the sides were filled with DPCP solution. The container was weighted full of a solution and simply the density was measured by the following equation:
p=mV
Where “p” is the density of the DPCP solution, "m" denotes the mass of the DPCP solution, and “V" refers to the volume of pycnometer filled by the DPCP solution.
2.2.2. Determination of pH
The pH of 5 ml of solution without dilution was determined in 25ºC±2ºC by pH meter (Metrohm 827, Swiss) (15).
2.2.3. Viscosity
The viscosity of the solution was measured by Polyvisc Viscometer (Brookfield, USA) using a spindle R1 at 100 RPM with a run time of 1 min. Viscosity was measured at room temperature (25ºC±2ºC).
Viscosity in centipoises (cps) = Dial reading×factor
2.2.4. Assay of Active Ingredients
High-performance liquid chromatography was performed by Acme 9000 Youngling (Tracer Excel 120 ODS-A TR-016340, South Korea) with Zorbax Bonus-RP C18, 150 mm × 4.6 mm column (Agilent, United States) as the stationary phase. The mobile phase for DPCP was acetonitrile and water (70:30). Injection volume and mobile phase flow rates were 5 µl and 1 ml/min, respectively. The wavelength of the ultraviolet detector for DPCP was 205 nm. Sample solutions of 100 ppm were prepared and injected in equivalent volumes. This experiment was performed in duplicate.
2.2.5. Microbial Assessments
A volume of 10 ml of solution was added to a 90 ml TSB medium to diagnose bacteria (Mixture A).
The colonies of plates were counted as 25-250 and the average number of CFU/g was calculated. Two dilutions (10-1, 10-2) of the TSB culture medium were prepared and 1-2 ml of premed dilution was added to 2 sterile plates containing 10-20 ml of TSA culture medium. Incubation was completed for 24-48 h at 30ºC-35°C (Pure plate). For fungal counting, the agar was left to solidify at room temperature, 1 ml of 0.1 dilution was added and incubated for 5-7 days at 20ºC-25°C.
Colonies were counted after incubation and all operations were carried out in duplicates. All microbial counts were transformed into logarithms of the number of colony forming units (log 10 CFU/g). Counting was passed in plates that contained less than 100 colonies for microbial count (TAMC) and contained less than 10 colonies for fungal count (TYMC) [27, 28].
2.2.5.1. Pseudomonas aeruginosa Count
Colonies were counted after 24-48 h of incubation at 30ºC-35ºC.
2.2.5.2. Staphylococcus aureus Count
Colonies of Staphylococcus were nominated, gram-stained, and tested for oxidase and catalase reactions to confirm presence [29].
2.2.5.3. Yeast and Mold Counts
After the incubation period, the white colonies were confirmed as Candida albicans with differential tests, such as tuberculosis.
3. Results
In both production methods, transparent and clear DPCP solutions were prepared, followed by filling and sealing in amber vials. The stability of topical solutions was studied as per ICH guidelines for 6 months. It was investigated at 5ºC±3ºC with no light exposure. During the period of storage, the formulations showed no variation in color, odor, density, viscosity, and pH. As shown in Table 2, the average initial pH of samples made by the method A and then at months 1, 3, and 6 were in the range of 7.5-8.05. The viscosity at the whole 6 months period was 0.321-0.324 cps. The density of the formulations had a range of 0.77-0.79 g/m³. According to Table 2, the assay of an active pharmaceutical ingredient in the formulations was in the range of 85%-115%.
Test | Period of storage | Standard | ||||
Initial | 1st M | 3rd M | 6th M | |||
Description | Complies | Complies | Complies | Complies | Transparent solution | |
Odor | Complies | Complies | Complies | Complies | Characteristic odor | |
Density (g/m³) | All prepared formulation has a density near each other and within the range. | aNLT 0.75 bNMT 0.80 | ||||
Viscosity (cps) | All prepared formulation has a viscosity near each other and within the range. | NLT 0.30 NMT 0.34 | ||||
pH
| All prepared formulation has a pH near each other and within the range. By reduction in DPCP concentration, the pH also decreased from 8 to 7.5. | NLT 6 NMT 9 | ||||
Assay (%) mean±SD | 2% 1% 0.5% 0.1% 0.05% 0.01% 0.001% | 114±0.19 100±0.62 96±1.97 106±6.34 102±1.08 101±0.56 98±1.09 | 95±3.06 96±0.42 97±0.19 90±0.31 94±0.63 85±2.78 78±1.39 | 94±2.95 96±0.22 97±5.39 88±0.59 90±4.36 70±2.95 8±1.40 | 94±0.49 98±0.84 97±3.13 80±2.70 82±1.53 11±0.53 No peak | 85-115
|
Remark / Conclusion | Approved | Approved | Approved | Approved | - | |
aNLT: Not Less Than
bNMT: Not More Than
Table 2. Stability evaluation and antimicrobial test result in method A
The DPCP solutions in high concentrations, such as 2%, 1%, and 0.5% were completely stable and suitable. In lower concentrations, including 0.05%, 0.1%, and 0.01%, the assays declined during 3 months. Chromatograms from the analysis of all solutions of DPCP made by methods A and B on the first day, as well as the 1st, 3rd, and 6th month are depicted in the attached file. Moreover, microbial assessments did not detect any bacterial or fungal colonies.
4. Discussion
DPCP is used as an immune-modulating therapeutic agent topically administered for AA treatment. The DPCP is applied at a high concentration of 2%, usually once for sensitization and then at lower concentrations of 0.001%-0.5% once weekly. Systemic immunological effects of DPCP were observed in mice treated with 0.01% or 0.1% DPCP [30]. Topical immunotherapy can cause few side effects, such as persistent dermatitis, painful cervical lymphadenopathy, generalized eczema, blistering, contact leukoderma, and urticarial reaction. Treatment with DPCP is usually safe and side effects are usually due to hypersensitivity to the chemical. The possible side effects include redness, blisters, itch, and white patches. These have been noted with DPCP suggesting possible absorption through the skin and distribution throughout the body. However, it has not been detected in the serum or urine after topical application [26]. The DPCP is non-mutagenic in the Ames assay at the concentrations of 50 and 100 µg/ml [26].
According to our findings, the good chemical stability of all DPCP solutions has been revealed at 5ºC±3ºC without light. Higher concentrations of DPCP showed much better stability than lower ones. By increasing the acetone portion in the lower concentrations of DPCP, the decomposition of DPCP was augmented. For example, a DPCP solution of 0.001
Conclusion
In the present study, two production methods were performed. One method was by acetone, and the second method was by propylene glycol diluted with acetone at the application time. All Formulas were assessed according to the ICH standards and were stable during long-term conditions. A higher concentration of DPCP in acetone showed better stability than lower ones. Therefore, for lower concentrations, we recommend method B for the final product. Propylene glycol is a good primary solvent for DPCP diluted products. The preferable storage condition for DPCP in a solution with both preparation methods is 5ºC±3ºC without light exposure. To increase the stability of the formulations and to inhibit solvent evaporation during storage, amber vials with rubber and aluminum cap are suggested. Our data can help scientists to develop a high potential solution to treat AA.
Ethics Approval and Consent to Participate
Not applicable.
Human and Animal Rights
No animals/humans were used for studies that are basis of this research.
Consent for Publication
Not applicable.
Funding
This study was supported by the Center for Research and Training in Skin Diseases and Leprosy, Tehran University of Medical Sciences with the Grant Number 97-03-34-39420. The authors would like to thank the pharmaceutical company, Jarf Andishan Navid Salamat (Janus), located in Tehran, Iran, for supplying materials for preparation and analyzing of diphencyprone solution.
Conflicts of Interest
The author declares no conflict of interest, financial or otherwise.
References
- Pratt CH, King LE Jr, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nat Rev Dis Primers 2017; 3:1-17
View at Publisher | View at Google Scholar - Tosti A, Bellavista S, Iorizzo M. Alopecia areata: a long-term follow-up study of 191 patients. J Am Acad Dermatol 2006; 55:438–441
View at Publisher | View at Google Scholar - Tan E, Tay YK, Goh CL, Chin GY. The pattern and profile of alopecia areata in Singapore: a study of 219 Asians. Int J Dermatol 2002; 41:748–753
View at Publisher | View at Google Scholar - Fiedler VC, Alaiti S. Treatment of alopecia areata. Dermatol Clin 1996; 14:733–738
View at Publisher | View at Google Scholar - Fiedler VC. Alopecia areata: a review of therapy, efficacy, safety and mechanism. Arch Dermatol 1992; 128:1519–1529
View at Publisher | View at Google Scholar - Schwartz RA, Jonninger CK. Alopecia areata. Cutis 1997; 59:238–241
View at Publisher | View at Google Scholar - Hapiro J. Alopecia areata: Update on therapy. Dermatol Clin 1993; 11:35–46
View at Publisher | View at Google Scholar - Olsen EA, Carson SC, Turney EA. Systemic steroids with or without 2% topical minoxidil in the treatment of alopecia areata. Arch Dermatol 1992; 128: 1467–73
View at Publisher | View at Google Scholar - Fiedler VC, Wendrow A, Szpunar GJ, Metzier C, De Villez RL. Treatment-resistant alopecia areata. Response to combination therapy with minoxidil plus anthralin. Arch Dermatol 1990; 126:756–9
View at Publisher | View at Google Scholar - Fiedler-Weiss VC. Topical minoxidil solution (1% and 5%) in the treatment of alopecia areata. J Am Acad Dermatol 1987; 16:745–8
View at Publisher | View at Google Scholar - Schmoeckel C, Weissman I, Pelwig G, Braun-Falco O. Treatment of alopecia areata by anthralin-induced dermatitis. Arch Dermatol 1979; 115:1254–5
View at Publisher | View at Google Scholar - Fiedler-Weiss VC, Buys CM. Evaluation of anthralin in the treatment of alopecia areata. Arch Dermatol 1987; 123:1491–3
View at Publisher | View at Google Scholar - Gupta AK, Ellis CN, Cooper KD, et al. Oral cyclosporine for treatment of alopecia areata. A clinical and immunohistochemical analysis. J Am Acad Dermatol 1990; 22:242–250
View at Publisher | View at Google Scholar - Gilhar A, Pillar T, Etzioni A. Topical cyclosporine A in alopecia areata. Acta Derm Venereol 1989; 69:252–253
View at Publisher | View at Google Scholar - de Prost Y, Teillac D, Paquez F, et al. Placebo-controlled trials of topical cyclosporine in severe alopecia areata. Lancet 1986; ii: 803–804
View at Publisher | View at Google Scholar - Magee KL, Hsu SM, Tucker SB. Trial of intralesional interferon-alpha in the treatment of alopecia areata. Arch Dermatol 1990; 126: 760–2
View at Publisher | View at Google Scholar - Ge S. Treatment of alopecia areata with acupuncture. J Trad Chinese Med. 1990; 10: 199–200.
View at Publisher | View at Google Scholar - Brzezińska-Wcisło LA, Wcisło-Dziadecka D. Hair diseases: a big problem on a small surface. Postep Dermatol Alergol 2016; 33: 317–322
View at Publisher | View at Google Scholar - Daman L, Rosenberg W, Drake L. Treatment of alopecia areata with DNCB. Arch Dermatol 1978; 114: 1036–1038
View at Publisher | View at Google Scholar - Happle R, Kalveran KJ, Buchner U, et al. Contact allergy as a therapeutic tool for alopecia areata: application of squaric acid dibutylester. Dermatologica 1980; 161:289–297
View at Publisher | View at Google Scholar - Happle R, Hansen BM, Wiesner-Menzel L. Diphenylcyclopropenone in the treatment of alopecia areata. Acta Derm Venereol (Stockh) 1983; 63: 49–52
View at Publisher | View at Google Scholar - Alkhalifah A, Alsantali A, Wang E, et al. Alopecia areata update: part II. Treatment. J Am Acad Dermatol 2010; 62: 191-202
View at Publisher | View at Google Scholar - Durdu M, Ozcan D, Baba M, et al. Efficacy and safety of diphenylcyclopropenone alone or in combination with anthralin in the treatment of chronic extensive alopecia areata: a retrospective case series. J Am Acad Dermatol 2015; 72: 640-650
View at Publisher | View at Google Scholar - Wiseman MC, Shapiro J, MacDonald N, et al. Predictive model for immunotherapy of alopecia areata with diphencyprone. Arch Dermatol 2001; 137: 1063-1068
View at Publisher | View at Google Scholar - El-Zawahry BM, Bassiouny DA, Khella A, et al. Five-year experience in the treatment of alopecia areata with DPC. J Eur Acad Dermatol Venereol 2010; 24: 264-269
View at Publisher | View at Google Scholar - Buckley DA, Du Vivier AW. The therapeutic use of topical contact sensitizers in benign dermatoses. Br J Dermatol 2001; 145: 385–405
View at Publisher | View at Google Scholar - United States pharmacopeia (USP39) and National Formulary (NF34), Twin brook Rockville MD 20852, Antimicrobial effectiveness testing 2016; 51: 111
View at Publisher | View at Google Scholar - United States pharmacopeia (USP39) and National Formulary (NF34), Twin brook Rockville MD 20852, Antimicrobial preservative effectiveness testing 2016; 61:117
View at Publisher | View at Google Scholar - Gupta AK, Jain HC, Lynde CW, et al. Prevalence and epidemiology of onychomycosis in patients visiting physicians’ of!ces: a multicenter Canadian survey of 15,000 patients. J Am Acad Dermatol 2000; 43(2 Pt 1):244-248
View at Publisher | View at Google Scholar - Buchanan R., Huynh G., Tanner J. Hosp. Pharm 2014; 49-59.
View at Publisher | View at Google Scholar - Ohlmeier MC, Traupe H, Luger TA, et al. (2012). Topical immunotherapy with diphenylcyclopropenone of patients with alopecia areata–a large retrospective study on 142 patients with a self‐controlled design; J Eur Acad Dermatol Venereol 2012; 26: 503
View at Publisher | View at Google Scholar - Svalgaard JD, S_rmark C, Dall M, et al. Immunol Res 2015; 58: 40
View at Publisher | View at Google Scholar - Singh G, Lavanya M. Topical immunotherapy in alopecia areata. Int J Trichology 2010; 2: 36–9
View at Publisher | View at Google Scholar - Katarzyna B, Tomasz, W. Stability of solutions of 2, 3 diphenylcyclopropenone in various solvents. A novel formula diphencyclopropenone in isopropanol may be useful in topical therapy of patients with alopecia areata. Acta Pol Pharm 2017; 74(2): 459-464.
View at Publisher | View at Google Scholar
