

Case Report | DOI: https://doi.org/10.31579/2834-5126/086
Post-Traumatic Carotid-Cavernous Fistula on Magnetic Resonance Imaging (Mri): A Case Report and Review of Imaging
- Gele IH *
- Sule MB
- Shamaki AMB
- Hafsat AR
- Kabir FU
Ibrahim Haruna Gele., Department of Radiology, Usmanu Danfodiyo University Teaching Hospital, Sokoto. Nigeria.
*Corresponding Author: Ibrahim Haruna Gele., Department of Radiology, Usmanu Danfodiyo University Teaching Hospital, Sokoto. Nigeria.
Citation: Gele IH., Sule MB., Shamaki AMB., Hafsat AR., Kabir FU., (2025), Post-Traumatic Carotid-Cavernous Fistula on Magnetic Resonance Imaging (Mri): A Case Report and Review of Imaging, Clinical Trials and Clinical Research,4(1); DOI:10.31579/2834-5126/086
Copyright: © 2025, Ibrahim Haruna Gele. This is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 November 2024 | Accepted: 20 December 2024 | Published: 15 January 2025
Keywords: carotid-cavernous fistula; trauma; magnetic resonance imaging
Abstract
Carotid-cavernous fistula (CCF) is an abnormal vascular connection between the carotid arteries or their branches and the cavernous sinus. It can be direct or indirect depending on the site of the fistula. It is a rare abnormality. CCF results in shunting of blood from the artery to the venous system leading to retrograde flow in the draining veins and possible brain ischaemia. Imaging is fundamental in the diagnosis and evaluation of complications. We report a rare case of CCF on MRI with review of imaging. An 18-year-old male presented with a week history of painful swollen left eye following road traffic accident. There was associated watery discharge, proptosis and poor vision. There was also history of headache which was generalized. On examination, the vital signs were normal. There was proptosis, peri-orbital oedema, redness and reduce vision in the left eye. A bruit was felt in the left eye. The right eye examination was unremarkable. The multisequence MRI of the orbit and brain show proptosis of the left eye with thickened extra-ocular muscle and orbital oedema. The superior orbital vein was grossly dilated and shows early contrast filling after intravenous gadolinium administration. In addition, there was cerebrospinal fluid collection (CSF hygroma) in the left retro-orbital region. The right orbit was normal. No intracranial aneurysm or haemorrhage was demonstrated. A diagnosis of left carotid-cavernous fistula was made.
Introduction
Carotid – Cavernous fistula (CCF) is an abnormal vascular connection between the carotid arteries (internal and or external carotid) or their branches and the cavernous sinus1. It is a rare abnormality (direct fistulas complicate 0.3% of cranio-facial trauma) 2,3. Two types exist, the direct and indirect CCF depending on the site of the fistula. In direct CCF, there is communication between the internal carotid artery and the cavernous sinus. It occurs usually in males as a rare complication of cranio-facial trauma. Other causes include intracranial aneurysm and weakened vascular wall. In indirect CCF, the communication is via the branches of the internal carotid artery (ICA) and or external carotid artery (ECA). It usually occurs in post menopausal women 4
CCF results in shunting of blood from the artery to the venous system leading to retrograde flow in the draining veins and possible brain ischemia. Imaging is fundamental in the diagnosis and evaluation of complications1,3.
We report a post traumatic carotid-cavernous fistula on MRI in an 18 year old male with review of imaging.
Case Report:
An 18 year old male undergraduate student presented with a week history of painful swollen left eye following road traffic accident. There was associated watery discharge, proptosis and poor vision. There was also history of headache which is generalized. No loss of consciousness, nausea or vomiting. No history of bleeding from the orifices. He had fever which subsided after taken antibiotics.
Not a known hypertensive, diabetic or sickle cell anaemic patient. No history of chronic cough or surgical intervention. No family history of similar problems in the past.
On examination, the patient was conscious but appears depressed, not in obvious painful or respiratory distress. He was not pale or icteric. The vital signs were normal. No feature of cranial nerve palsy or lateralizing sign was detected on neurological examination. The was proptosis, peri-orbital oedema, redness and reduce vision in the left eye. A bruit was felt in the left eye. The right eye examination was unremarkable. Other systemic examinations were also unremarkable. A provisional diagnosis of carotid-cavernous fistula was made and was referred to radiology department for magnetic resonance imaging (MRI).
The multisequence MRI of the orbit and brain shows proptosis of the left eye with thickened extraocular muscle and marked orbital oedema (fig. 3). The superior orbital vein was grossly dilated, tortuous and show early contrast filling after intravenous gadolinium administration (fig. 1 and 2). In addition, there was cerebrospinal fluid collection (CSF hygroma) in the left retro-orbital region (fig. 1). The right orbit was normal. No intracranial aneurysm or haemorrhage was demonstrated. A diagnosis of left carotid-cavernous fistula was made.
The patient was initially managed conservatively with antibiotics and carotid compression. There was no significant clinical improvement and he was later referred to a center with vascular intervention facility for definitive treatment.
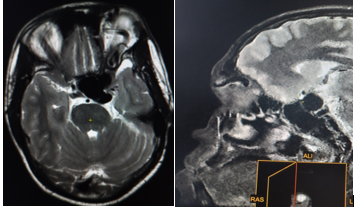
Figure 1: Axial T2 and sagital T1 magnetic resonance images of the brain and orbit shows dilated tortuous left superior ophthalmic vein (arrows). Note also the enlarged left cavernous sinus (star) and left retro-orbital T2 hyperintense collection.
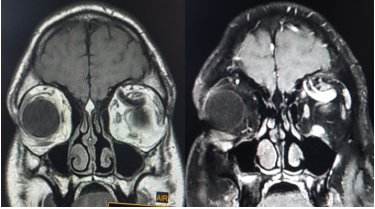
Figure 2: Coronal T1 and T1 + contrast magnetic resonance images of the orbit shows dilated left superior ophthalmic vein. Note the early contrast filling of the vein (arrow).
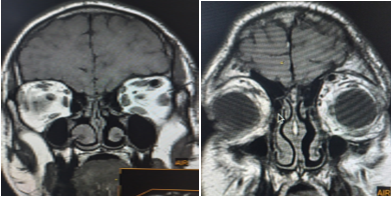
Coronal T1 magnetic resonance images show thickening of the left extra-ocular muscles (horizontal arrow) and oedema of the orbital soft tissues (vertical arrow) compared to the normal right side. Note also dilated left superior ophthalmic vein.
Discussion:
Carotid-cavernous fistula is an abnormal vascular communication between the carotid artery and cavernous sinus. They can be direct or indirect. The direct fistula is a high flow fistula between the intracavernous part of the internal carotid artery and the cavernous sinus1. The indirect carotid-cavernous fistulas are low flow fistula between the branches of the internal or external carotid artery and the cavernous sinus. Barrow et al classified CCF into 4 types A-D. Type A is when the fistula is with the intracavernous ICA, type B is with the meningeal branches of ICA, type is with meningeal branches of ECA and the type D is when the fistula is with meningeal branches of both ICA and ECA1,3.
Clinical presentation of CCF is commonly with proptosis, chemosis of the conjunctiva, diplopia, orbital bruit, visual disturbances ocular pain and headache5,6. These features were present in the index patient. The clinical course and complication of CCF vary from cranial nerve palsy to intracranial haemorrhage, bleeding from the nose and ear. Severe and persistent proptosis may lead to exposure keratopathy, ophthalmoplegia and glaucoma7.
Imaging modalities for evaluation of suspected CCF are Doppler ultrasonography, computed tomography and angiography (CT and CTA), magnetic resonance imaging and angiography (MRI and MRA) and digital subtraction angiography (DSA)2,5. The imaging findings are similar in both direct and indirect fistula. Doppler ultrasonography is readily available and does not use ionising radiation. However, it is operator dependent. Ocular Doppler findings that suggest CCF includes presence of flow reversal or thrombosis in the superior ophthalmic vein (SOV) and arterialization with low resistance of the vein, demonstrated in colour and spectral Doppler respectively 2. CT and MRI are the initial imaging technique employed in the evaluation of CCF especially in post traumatic cases. Their findings are usually similar and highly suggest the diagnosis. These includes proptosis, enlarged superior ophthalmic vein, extra-ocular muscle thickening as well as orbital and peri-orbital oedema as demonstrated in this case (fig.2,3). Other findings are distension or bulging of the cavernous sinusj. However, MRI with its multisequence protocol is superior to CT in the detection of radiological signs, minimal SOV dilatation, subtle proptosis and small extra-ocular muscle thickening. Also abnormal signal void within the cavernous sinus due to increase flow may additionally be demonstrated in MRI. CT has the advantage of demonstrating basal skull fracture in post traumatic CCF2,5.
CTA and MRA both show early opacification of the cavernous sinus, SOV and venous drainage of the fistula. Digital subtraction angiography (DSA) is the gold standard for confirmation of diagnosis, classification and treatment planning. However, it is not routinely employed in all patients due to its invasiveness. It also has limitation in evaluating orbital soft tissues and brain parenchyma. Imaging findings in DSA are rapid shunting of flow from internal carotid artery to cavernous sinus, enlarged draining veins and retrograde flow from the cavernous sinus to the ophthalmic veins2,4.
Differential diagnosis of CCF is cavernous sinus thrombosis. This usually present with bilateral ocular symptoms and imaging findings. Other differentials are orbital cellulitis, conjunctivitis and thyroid ophthalmopathy. These can be differentiated by the imaging features of CCF earlier described.
Treatment options for CCF include conservative management by manual compression of the carotid artery at the neck. Other options are open surgery, radiosurgery and endovascular embolization3. In few cases spontaneous closure of the fistula may occur2.
Conclusion:
Post traumatic carotid-cavernous fistula is a rare abnormality with sight threatening and intracranial complications. Positive findings on initial radiological imaging such as CT and MRI are highly sensitive for the diagnosis. DSA is reserve for confirmation, classification and treatment planning.
References
- Htun L, Kyaw K, Htwe HY, Deepak K, Sammy SMA, et al. (2018). A case of right-sided direct carotid cavernous fistula: A diagnostic challenge. Am J Case Rep; 19: 47-51.
View at Publisher | View at Google Scholar - Daniela dos S, Lucas MM, Guilherme SN, Antonio AVC, Benedicto OC, et al. (2014). Imaging diagnosis of dural and direct cavernous carotid fistulae. Radiol Bras; 47(4): 251-255.
View at Publisher | View at Google Scholar - Muhammad SS, Sai SY, Sidra J, Favour CM, Muhammad S, et al. (2023). Traumatic carotid cavernous fistula resulting in symptoms in the ipsilateral eye: A case report.
View at Publisher | View at Google Scholar - Daniel P. (2023). Caroticocavernous fistula.
View at Publisher | View at Google Scholar - Kim D, Choi YJ, Song Y, Chung SR, Baek JH, et al. (2020). imaging for carotid cavernous sinus fistula. Am J Neuro Radiol.; 41(9): 1599-1605.
View at Publisher | View at Google Scholar - Hooman H, Daniel HP, William B, Nicholas DA. (2022). Traumatic carotid-cavernous fistula: A case report. Radiol Case Rep.; 17 (6): 1955-1958.
View at Publisher | View at Google Scholar - Nirupama K, Pooja K, Gayatri N, Nagarajan K. (2019). Post-traumatic carotid-cavernous fistula with bilateral proptosis simulating cavernous sinus thrombosis. BMJ Case Rep.; 12(3): e227757.
View at Publisher | View at Google Scholar
