

Case Report | DOI: https://doi.org/10.31579/2835-8295/042
Pleomorphic Liposarcoma Resection at Right Lower Extremity and Anterolateral Thigh Flap Reconstruction
1 Cirujano General. Residente de Cirugía Plastica y Reconstructiva del Hospital Universitario de
Caracas. Caracas. Venezuela
2 Cirujano Oncólogo, Oncoplástico y Mastólogo. Jefe del Servicio de Cirugía Oncológica del Hospital Universitario de Los Andes. Mérida. Venezuela
3 Cirujano Oncólogo, Oncoplástico y Mastólogo. Adjunto al Servicio de Cirugía Oncológica del Hospital Universitario de Los Andes. Mérida. Venezuela
4 Cirujano Oncólogo, Oncoplástico y Mastólogo. Adjunto al Servicio de Cirugía Oncológica del Hospital Universitario de Los Andes. Mérida. Venezuela
5 Interno de Pregrado del Hospital Universitario de Los Andes.
*Corresponding Author: Juan A Ricciardi V, Cirujano General. Residente de Cirugía Plastica y Reconstructiva del Hospital Universitario de
Citation: Juan A Ricciardi V, José L Valderrama, Demian Spinetti, Eliana Sanabria, Arianny E Santiago., (2023), Pleomorphic Liposarcoma Resection at Right Lower Extremity and Anterolateral Thigh Flap Reconstruction, International Journal of Clinical Reports and Studies, 2(6); DOI:10.31579/2835-8295/042
Copyright: © 2023, Juan A Ricciardi V. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 November 2023 | Accepted: 09 December 2023 | Published: 12 December 2023
Keywords: soft tissue sarcoma; pleomorphic liposarcoma; reconstruction; flap; graft
Abstract
Sarcomas are a heterogeneous group of malignant neoplasms and can occur in almost every anatomic site and side. The vast majority of diagnosed sarcomas are soft tissue sarcomas and the treatment of these tumors is very complex and depends on their specific subtypes. Case Report: 45 years old female patient who reports the onset of the current disease 2 years prior to admission, characterized by progressive growth of a local mass at the proximal third and medial aspect of the right leg and knee which is why goes to her local doctor from where they refer to the IAHULA oncological surgery service. Trucut needle biopsy and immunohistochemistry report a well-differentiated pleomorphic liposarcoma. Resonance magnetic image of the extremity and CT-Scan was performed finding suspicious lymph nodes at the right inguinal station and no pulmonary or other metastases. Preoperative oncological evaluation EC III G1 T2b N1 M0, was taken to the operation room where was performed a wide local resection + anterolateral thigh flap reconstruction + full thickness free graft for donor area and inguinofemoral lymphadenectomy. After a satisfactory postoperative recovery, monitoring output through aspiration and without signs of infection or dehiscence, she was discharged for adjuvant treatment with radiotherapy. Discussion: According the Sarcoma NCCN Guidelines 2023 possible treatment pathways for stage 3 and non-metastasic stage 4 sarcomas include surgery and radiation therapy or chemoradiation. Conclusion: Sarcoma soft tissue are aggressive lesions that require a quick diagnosis and correct orientation in order to give a correct oncological approach to the patient and reduce morbidity and mortality
Introduction
Sarcomas are a heterogeneous group of malignant neoplasms. These tumors arise from mesenchymal cells, which include dozens of histological types, and can occur in almost every anatomic site and side. The vast majority of diagnosed sarcomas are soft tissue sarcomas [1] and the treatment of these tumors is very complex and depends on their specific subtypes [2]. The World Health Organization defines pleomorphic liposarcoma (PLPS) as a pleomorphic, high-grade sarcoma containing a variable number of pleomorphic lipoblasts; is the rarest subtype of liposarcoma, accounting for approximately 5% of all liposarcomas [3]. It commonly occurs in adults later in life, with a peak incidence in the seventh decade of life; its incidence is slightly higher in men than in women. PLPS is an aggressive sarcoma with local recurrence and metastatic rate of 30–50% and an overall survival (OS) rate of 60% [3].
Despite being rare as compared to other tumors, their incidence continues to steadily increase, and they are associated with relevant morbidity and mortality, in particular in young adults where certain sarcoma subtypes are among the leading causes of death. The prediction of survival for patients diagnosed is challenging, as the currently available tools such as tumor-node-metastasis staging systems are limited in their accuracy [4]. Surgery represents the main therapeutic option, and the tumors of the thigh requires a carefully resection of the neoplastic mass [5]. Here, we report a case of a relatively young woman, with a big lower limb liposarcoma who requires a huge surgical resection with a complex reconstructivealternative.
Case Report
A 45 years old female patient from El Vigia , Merida state, without comorbidities, who reports the onset of the current disease 2 years prior to admission, characterized by progressive growth of a local mass at the proximal third and medial aspect of the right leg and knee, it started as a small lesion but due to the patient's shame and fear of consulting in a timely manner, it grew progressively which is why she goes to her local doctor from where they refer to the emergency of adults of the University Hospital of Los Andes where it is valued by the oncological surgery service.
No personal or family history of cancer. On physical examination, the patient was in well general condition.
At the lower extremity at the proximal third and medial aspect of the right leg and knee an exophytic tumor lesion, partially ulcerated, with irregular edges, non-mobile adhered to deep planes, with necrotic edges and perilesional phlogosis of approximately 15 x 12 cm. (Figure 2).
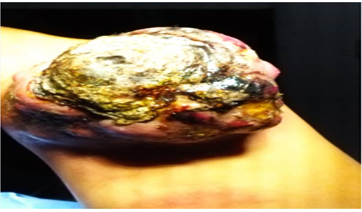
Figure 2: Exophytic tumor lesion, partially ulcerated, with irregular edges, non-mobile adhered to deep planes, with necrotic edges at the right lower extremity
Trucut needle biopsy and immunohistochemistry report a well-differentiated Pleomorphic Liposarcoma. Resonance magnetic image of the extremity and CT-Scan was performed in order to find lymph lessions and stadificate the disease, finding suspicious lymph nodes at the right inguinal station and no pulmonary or other metastases. Reason why, with the correct preoperative oncological evaluation EC III G1 T2b N1 M0, she was taken to the operation room by the IAHULA Oncological Surgery Service where under general anesthesia was performed a wide local resection + anterolateral thigh flap reconstruction + full thickness free graft for donor area and inguinofemoral lymphadenectomy (Figures 3 to 5).

Figure 3: IAHULA Oncological Surgery Service and PGY4 General Surgery Resident performed the wide local resection + anterolateral thigh flap reconstruction + full thickness free graft for donor area and inguinofemoral lymphadenectomy

Figure 4 : Right lower extremity after the oncological resection.
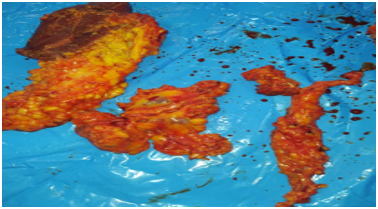
Figure 5 : Inguinofemoral lymphadenectomy piece.
Results of the surgical piece's reports negative margins of the huge resection but lymph node piece with positive metastases. After a satisfactory postoperative recovery, monitoring output through aspiration and without signs of infection or dehiscence, she was discharged for adjuvant treatment with radiotherapy. However, unfortunately the patient and her family were unable to acquire the resources for adjuvant therapy and 8 months after the surgery she returned with a lesion suggestive of recurrence in the reconstructed limb.
</>< style="text-align:center;">Figure 1: Adults Emergency Department at the IAHULA, Merida, Venezuela
Discussion
There are different therapeutic approaches for treatment of sarcoma patients. The primary treatment in early-stage sarcoma patients consists of a wide surgical resection to obtain tumor-free resection margins. Data from prospective studies support the use of radiotherapy in addition to surgery among appropriately selected patients in terms of an improvement in disease-free survival with the exception of overall survival [1]. However, despite the surgical resection is currently the main treatment for this disease, those patients have a higher relapse propensity even after complete resection, wich is why the resection margin and histological subtype remain the most important prognostic predictors for local recurrence and overall survival [6].
In this case, the patient was a woman of 45 years old, so according the epidemiology of the disease, has no relation with the publication of Müller J, Delink K, et al. [1] that show that the prevalence sex was male patient but it coincides with the same authors because they describe that the majority of patients with sarcoma of soft tissues are older than 40 years.
According Nakamura T, Sakai T, et al. [7] generally the margins comprise soft tissue, such as the fascia and muscle, although sarcoma soft tissues may directly about the bone, a fact that has relation with our case because when the patient was diagnosed, a huge mass tumor at the right lower extremity comprise the fascia and the muscles of part of the leg wich was later confirmed by the pathological state after the pathologist report of the surgical piece. Also, the MRI at the preoperative stratification reports that the bone was intact as the majority of soft tissue sarcomas, even in advances stages, having relation with the publication of Ferguson P, Griffin A, et al. [8] in their review of 874 patients with soft tissue sarcomas of the extremities. Identified only 48 patients (5.5%) with evidence of bone invasion.
The diagnosis of the patient was confirmed by the histopathological report of the previous trucut needle biopsy, a fact that has relation by the publication of Islam N, Das R, et al. [9] who said that the trucut biopsy is a simple, safe, and reliable adjunct to the fine-needle aspiration cytology. Instead, immunohistochemistry enhances the diagnostic accuracy.
Our patient debuts with a pleomorphic liposarcoma of the lower limb, the most common type of all the soft tissue sarcomas in relation with the research of Katal S, Gholamrezanezhad A, et al. (10) who describe that liposarcoma is among the most common sarcoma soft tissues and they arise most often from the deep soft tissues of the extremities and retroperitoneum, and can demonstrate multiple histologic subtypes, including myxoid, pleomorphic, and dedifferentiated tumor cells. But, according the anatomical site, have no relation with the publication of Zafar R, Wheeler Y [11] because they said that dedifferentiated liposarcoma is much more common in retroperitoneal locations, while myxoid liposarcoma occurs in the lower extremities.
Talking about the surgical margin’s excision, according the research of Shafiq M, Rafi I, et al. [12] the most common site of occurrence was lower extremity 102 (70.3%) and all the patients had residual disease after unplanned excisions; and 107 underwent R0 resection, while 38 underwent R1 resection. Our patient had a R0 resection, but her oncological evolution was not as expected taking in count the fact of not being able to receive radiotherapy due to lack of financial resources. In fact, the conclusion research of Smoller M, Andreou D, et al. [13] neoadjuvant and adjuvant radiotherapy are associated with lower reduce local recurrence risk, but do not seem to affect distant metastasis or overall survival.
In addition to the resection of the tumor piece, in our patient was performed a inguinofemoral lymphadenectomy according to the findings of the clinical and image preoperative stratification, a fact that has a strong evidence according to the article of Sawamura C, Matsumoto S, et al. [14] when said that several authors concluded that patients who underwent lymphadenectomy had better overall survival than that for patients treated by chemotherapy and radiotherapy only.
According the Sarcoma NCCN Guidelines 2023 [15] possible treatment pathways for stage 3 and non-metastasis stage 4 sarcomas include surgery and radiation therapy or chemoradiation as our patient who unfortunately, after the correct surgery don’t receive the radiation therapy as we explained.
The soft tissue coverage after the oncological resection was made with an anterolateral thigh flap reconstruction + full thickness free graft for donor area, an important decision that was described by Otieno D, Oduor N, Hania J, et al. [16] they said the importance and practical applicability of the technique in different clinical settings like lower limb reconstruction, and also the fact that the anterolateral thigh flap is versatile due to its good pedicle length and caliber and its large, pliable skin paddle capable of achieving functional and aesthetic reconstruction. However, on the research of Onuma H, Fuse Y, et al. [17] said that an anterolateral thigh flap would have necessitated skin grafting at the donor site, which could have prolonged the healing process and delayed postoperative treatments of sarcoma which heroically can represent a advantage.
Conclusion
Sarcoma soft tissue are aggressive lesions that require a quick diagnosis and correct orientation in order to give a correct oncological approach to the patient and reduce morbidity and mortality.
Implications
The implications of share the importance of the multidisciplinary approach of these patients that include Oncological Surgeons, Plastic and Reconstructive Surgeons, Radio oncologist, Pathology
Department, Radio diagnosis Department.
Funding
This research received no specific funding from any sector or agency.
Author Contributions
The autor contributed to the creation and desing of this manuscript. All the tutors approved the final version.
Conflict Of Interest Statement
None declared.
References
- Müller J, Delank K, Laudner K, (2023). Clinical characteristics of sarcoma patients: a population‑based data analysis from a German clinical cancer registry. Journal of Cancer Research and Clinical Oncology 149:17051–17069.
View at Publisher | View at Google Scholar - Zajac A, Czarnecka A, Rutkowski P. (2023). The Role of Macrophages in Sarcoma Tumor Microenvironment and Treatment. Cancers 15, 5294.
View at Publisher | View at Google Scholar - Shimomura S, Shirai T,Terauchi R, (2023). Pleomorphic liposarcoma of the extremity with solitary huge liver metastasis at initial diagnosis treated with conversion surgery combined with adjuvant chemotherapy: a case report. Journal of Medical Case Reports. 17:484
View at Publisher | View at Google Scholar - Vignoli A, Miolo G, Tenori L, et al . (2023). Novel metabolomics-biohumoral biomarkers model for predicting survival of metastatic soft tissue sarcomas. iScience 26, 107678 October 20,
View at Publisher | View at Google Scholar - Ipponi E, Di Lonardo M, Bechini E, et al .(2023). Giant atypical lipomatous tumors of the thigh: a case series. Acta Biomed; Vol. 94, N. 5 e2023202
View at Publisher | View at Google Scholar - Deng H, Gao J, Xu X, (2023). Predictors and outcomes of recurrent retroperitoneal liposarcoma: new insights into its recurrence patterns. BMC Cancer 23:1076
View at Publisher | View at Google Scholar - Nakamura T, Sakai T, Tsukushi S, (2023). Clinical Outcome in Patients With High-grade Soft-tissue Sarcoma Receiving Prosthetic Replacement After Tumor Resection of the Lower Extremities: Tokai Musculoskeletal Oncology Consortium Study. in vivo 37: 2642-2647.
View at Publisher | View at Google Scholar - erguson P, Griffin A, O’Sullivan B, (2006). Bone invasion in extremity soft tissue sarcoma. Cancer 106(12): 2692-2700,
View at Publisher | View at Google Scholar - slam N, Das R, Chatterjee U, (2022 ). Utility of trucut biopsy in diagnosis of palpable pediatric soft tissue neoplasms. Indian J Pathol Microbiol.65(2):374-380.
View at Publisher | View at Google Scholar - Katal S, Gholamrezanezhad A, Kessler M, (2018). PET in the Diagnostic Management of Soft Tissue Sarcomas of Musculoskeletal Origin. PET Clin. 13(4): 609–621.
View at Publisher | View at Google Scholar - afar R, Wheeler Y. Liposarcoma.(2023). StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Jan.2023
View at Publisher | View at Google Scholar - Shafiq M, Rafi I, Shoaib A, et al. (2022) The Outcome of Extremity Soft Tissue Sarcomas in Terms of Resection Margins: A Study from a Cancer Dedicated Center. Cureus 14(6): e26086.
View at Publisher | View at Google Scholar - Smolle M, Andreou D, Wolfel J, (2023). Effect of radiotherapy on local recurrence, distant metastasis and overall survival in 1200 extremity soft tissue sarcoma patients. Retrospective analysis using IPTW-adjusted models. Radiotherapy and Oncology 189 109944
View at Publisher | View at Google Scholar - Sawamura C, Matsumoto S, Shimoji T, (2013). Lymphadenectomy and Histologic Subtype Affect Overall Survival of Soft Tissue Sarcoma Patients With Nodal Metastases. Clin Orthop Relat Res 471:926–931
View at Publisher | View at Google Scholar - NCCN Guidelines for patients, Soft Tissue Sarcoma 2023
View at Publisher | View at Google Scholar - Otieno D, Oduor N, Hania J, (2023). A staged approach for complex scalp defects using titanium mesh and anterolateral thigh flaps: Two case reports. International Journal of Surgery Case Reports 110 108766
View at Publisher | View at Google Scholar - Onuma H, Fuse Y, Karakawa R, (2023). The Pedicled Anterolateral Thigh Flap for Donor Site Closure after a Large Superficial Circumflex Iliac Artery Perforator Flap Harvest. Plast Reconstr Surg Glob Open; 11: e5115;
View at Publisher | View at Google Scholar
