

Research Article | DOI: https://doi.org/10.31579/2835-8147/091
Personalized Transcranial Electrical Stimulation Improves Sleep – Early Findings
*Corresponding Author: R. Gurumoorthy, StimScience Inc.
Citation: V. Ayanampudi, A. Krishnan1, R. Gurumoorthy, (2025), Personalized Transcranial Electrical Stimulation Improves Sleep – Early Findings, Clinics in Nursing, 4(5); DOI:10.31579/2835-8147/091
Copyright: © 2025, R. Gurumoorthy. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 August 2025 | Accepted: 27 August 2025 | Published: 11 September 2025
Keywords: radiation safety; contrast-enhanced radiology; quality assurance; north-western Nigeria
Abstract
Sleep is fundamental to both physical and mental health, regulating major physiological systems (e.g., cardiovascular, immune, endocrine, metabolic) and supporting cognitive and emotional functioning here we report results of a non-invasive electrical brain stimulation approach using personalized transcranial alternating current stimulation (tACS) in improving sleep. A total of 31 participants were recruited for null-stimulation and personalized stimulation within subjects randomized crossed design. The study was conducted with a full PSG measurement in a controlled sleep lab setting. The personalized stimulation modulated neural activity in the theta/alpha bands using a pre-sleep 15 ½ minutes stimulation. The personalization involved using each individual’s peak EEG frequencies in their theta and alpha bands. Personalized stimulation improved sleep efficiency by 13.4%, and reduced onset latency to 6.7 minutes (a reduction of 54%), and increased the sleep duration by 26.3 minutes. These results suggest that personalized stimulation improves sleep quality and motivates its potential for being a sleep therapeutic for people suffering from insomnia.
Introduction
Sleep is fundamental to both physical and mental health, regulating major physiological systems (e.g., cardiovascular, immune, endocrine, metabolic) and supporting cognitive and emotional functioning [1]. Despite this, one in three adults sleeps less than the CDC’s recommended seven hours per night [4], and more than 30% of the general population will experience insomnia during their lifetime [25][4]. Pharmacological interventions, such as sedative hypnotics, are widely prescribed for sleep difficulties. However, these drugs have significant side effects, limited long-term efficacy, and may fail to restore normal sleep architecture [2]. Due to these safety and efficacy concerns, they are no longer recommended as a first-line treatment for insomnia [2]. These limitations have driven interest in non-pharmacological approaches to improving sleep. One such method is non-invasive brain stimulation (NIBS), which uses external stimuli to modulate neural activity. Techniques include acoustic, magnetic, and electrical stimulation, each targeting outcomes such as sleep onset, quality, or duration [3]. Two primary electrical stimulation methods are transcranial direct current stimulation (tDCS) and transcranial alternating current stimulation (tACS). Both apply low-intensity electrical currents (1–2 mA) to the scalp. While tDCS delivers a constant current, tACS alternates, enabling more flexible waveforms tailored to modulate specific neural frequency bands. Electrical brain stimulation has a strong safety profile, with no serious adverse effects reported [13]. Large datasets—over 33,000 tDCS sessions and 1,000 participants—show only mild, transient sensations such as tingling, itching, or warmth [14][15]. tACS shares this safety record [17] and often produces even less scalp sensation than tDCS [16]. Brain oscillations occur in frequency bands tied to distinct functions [9][18][19][20][41][42][43]. Regarding sleep, EEG studies indicate that frontal-lobe oscillations are reliable biomarkers of sleep onset and maintenance [5][24], likely reflecting top-down regulation of cortico-thalamic feedback loops [6]. Experimental evidence supports the sleep-modulating potential of frontal tACS. For example, 5 Hz stimulation over the frontal cortex increases subjective sleepiness and slow-frequency EEG power [7]. Bilateral 5 Hz tACS over fronto-temporal regions can shorten sleep onset latency [30] and enhance slow- wave activity early in NREM sleep [8]. Alpha-band activity (8–13 Hz) has also been linked to drowsiness and wake–sleep transitions [31]. Past tACS sleep studies have applied uniform protocols across participants, typically targeting 0.5–16 Hz [32]. However, individuals show substantial variability in peak alpha and theta frequencies [33][34], which may limit the effectiveness of fixed protocols. This has motivated exploration of personalized tACS, in which stimulation is tuned to an individual’s intrinsic EEG peaks [26]. Personalized alpha or theta stimulation during wakefulness has been shown to improve entrainment, neural plasticity, and functional outcomes [35][22][23][27][12][28]. Building on this evidence, the present study tested whether personalized pre-sleep tACS could improve sleep efficiency, duration and onset. We compared two protocols: (1) a sham stimulation (30seconds ramp-up, ramp-down, followed by 15 minutes of null stimulation) and (2) a 15 ½ minute personalized waveform based on each participant’s personalized EEG peaks. Both were administered for 15 ½ minutes before bedtime using frontal electrodes. We hypothesized that personalized stimulation would outperform null-stimulation control.
Study Aim
The primary aim of this study was to evaluate whether frequency-specific personalized transcranial alternating current stimulation (tACS) administered prior to sleep could enhance objective sleep outcomes compared to a null-stimulation control condition.
Specifically, the study sought to:
1. Assess overall sleep efficiency improvement by tACS over control:
Determine whether either active stimulation protocol (Personalized) increases total sleep efficiency and reduces the tossing/turning or wake-after-sleep-onset (WASO).
2. Compare onset latency changes with personalized vs. control protocol:
Test whether aligning stimulation frequencies to each participant’s individual EEG peaks produces superior improvements in sleep onset compared to sham control.
3. Explore overall sleep duration changes:
Investigate whether overall sleep duration improved with the personalized stimulation.
By addressing these objectives, the study aimed to generate preliminary evidence supporting the development of individualized, non-pharmacological neuromodulation strategies to improve sleep health.
Method
Overview
Participants (n = 31; a mix of male-female, and young-old) completed a within-subject, randomized, crossover trial with two conditions: Personalized tACS, and Control (null stimulation). Single channel of stimulation using bilateral frontal electrodes (Fp3 and Fp4) delivered 15 ½ minutes of pre-sleep stimulation. Personalized stimulation frequencies were derived from individual EEG. Sham (null) stimulation was a standard 30 second ramp-up, ramp-down stimulation which was null for the remaining 15 min duration. The order of null stimulation and personalized stimulation was randomized. Participants were outfitted with full PSG measurements including wet EEG (frontal, central, parietal, occipital electrodes), ECG, EOG and EMG (chin myography). Using a Neuroconn electrical stimulation device, we applied a single channel of stimulation using bilateral frontal electrode (Fp3 and Fp4) locations. The device used regular wet medical grade gel-based electrodes for stimulation. The stimulation waveforms of interest were programmed using their software API and uploaded into the device.
Participants and procedures
Participants were recruited from San Francisco Bay Area. All participants were screened for neurological or medical disorders or conditions that are known to affect EEG or cognitive functioning. A total of 31 participants were tested in a randomized, cross-over design (mean age: 56, with the age ranging between 30-70, 17 male and 14 female). Participants completed the Insomnia Severity Index questionnaire prior to their first session using an online form. Participants were primarily distributed on the first 3 ISI categories of no-insomnia, subclinical and clinical insomnia, with only 1 severe insomniac. For the Personalized tACS condition, a preliminary session was conducted to collect EEG data from the participants to identify, on an individual basis, the power peaks within their EEG. These data were obtained during 15-minute sessions, with the participant in a relaxed, eyes-closed state, before any of the pre-sleep stimulation sessions. The EEG signal was band pass filtered with cutoff frequencies at 0.3Hz and 45 Hz. The power spectral density (PSD) was calculated using the Welch method on the filtered data and the Fooof algorithm [18] was used to determine frequency peaks after removing the aperiodic component of the spectrum. A k- means algorithm was used to calculate power peaks within the alpha and theta bands. For the personalized tACS condition, a stimulation waveform composed of two sinusoids was created, based on their power peaks in the alpha and theta bands. The component waveforms were started in phase and summed. These two frequency bands were targeted given their association with sleep onset, with alpha band activity (8-13Hz) linked to stage I sleep and theta band activity (4-8 Hz) linked to the transition to stage II sleep [9]. The amplitude of both sinusoids was set at 0.6mA intensity (peak-to-peak).
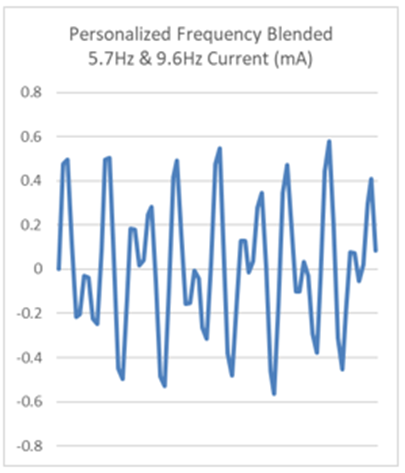
Figure 1: Sample personalized stimulation waveform blending 5.7Hz and 9.6Hz frequencies
Data Collection
Continuous PSG was recorded using the NATUS PSG system, from each subject through the night with EEG (midline and bilateral coverage in the frontal, central, midline parietal and occipital, and mastoids), vertical and horizontal eye movements (EOG) were recorded using external electrodes positioned directly above and to the side of the left eye, ECG signal were also measured, along with chin myography from two electrodes on the chin. Signals were digitized and processed offline.
Data Preprocessing and Analysis
Sleep Data Processing
The data collected was first divided into 30 second epochs. An experienced sleep scoring specialist visually inspected all the signals in each epoch and assigned a sleep stage based on predefined rules and criteria specified in the AASM manual. It was reviewed by another sleep tech separately and any differences in scoring were resolved by both scorers discussing and coming to a consensus.
Data Analysis
Sleep tracking data was obtained using the overnight sleep tracking scores from the Natus PSG data. Sleep stage data from the device were not analyzed for this study – as the aim of the study was to explore the overview metrics of Sleep Efficiency, Onset, and Duration. Sleep onset was defined as the interval between the end of stimulation and the first epoch scored as light, deep or REM sleep. The change in sleep onset between the two conditions was calculated as the difference in the onset of personalized stimulation compared to the null stimulation condition for each participant. Sleep Efficiency was measured as the time slept (light sleep, deep sleep, REM) as a percentage of the time they spent in bed (including wakes in between). The change in sleep efficiency between the two conditions was calculated as the difference in the efficiency of personalized stimulation compared to the null stimulation condition as a percentage of the null stimulation measurement for each participant. Sleep Duration was measured as the total time slept including light sleep, deep sleep, and REM sleep. The change in sleep duration between the two conditions was calculated as the difference in the sleep duration of personalized stimulation compared to the null stimulation condition.
Results
Using the PSG data, the results of the sleep measures across the personalized stimulation and sham (null-stim condition) are presented in Table 1. To get a context on the improvements seen with personalized stimulation, we reviewed other published results for sleep pill Zolpidem (Ambien) [36], and the hormonal supplement Melatonin [37],[38].
| Stim | Sham | P value |
SleepEfficiency | 85.7% | 78.4% | 0.007 |
Onset Latency (minutes) | 6.7 | 14.7 | 0.009 |
Sleep Duration (minutes) | 308.5 | 282.2 | 0.008 |
Table 1: Sleep Performance Results
| Sleep Efficiency (% improvement) | OnsetLatency (mins) |
Personalized tACS | 13.4% | 6.7 |
Ambien | 8.7% | 14.2 |
Melatonin | 3.1% | 10.8 |
Table 2: Results from this study, and reported data for Ambien, Melatonin
Sleep Efficiency:
As seen in Table 1, personalized tACS stimulation improved sleep efficiency significantly to 85.7% from 78.4% for sham (p-value 0.007). This shows an improvement of 13.4% on average across the group. In comparison the sleeping pill Zolpidem (Ambien) reports 8.7% improvement [36], and the hormonal supplement Melatonin is the least with 3.1% improvement [37]. As we can see Personalized tACS is more efficient, almost 4x more efficient than Melatonin (Table 2).
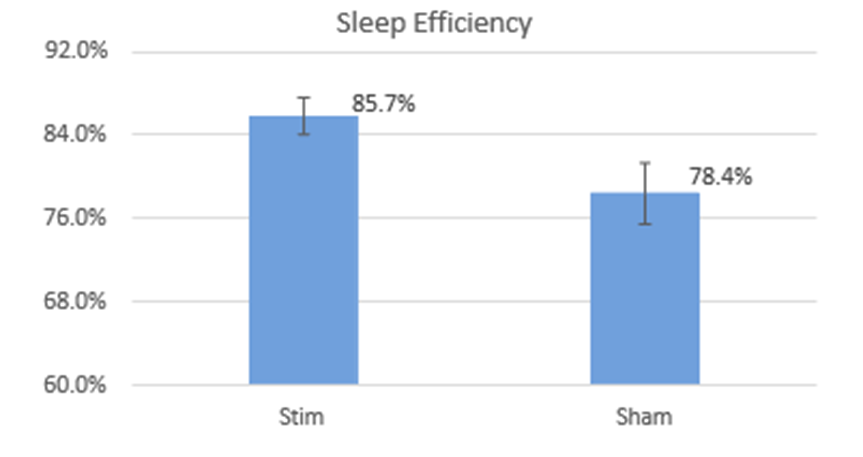
Figure 2: Sleep Efficiency Comparison
Looking at the sleep efficiency improvement from a perspective of the interruptions in sleep (the period spent awake in bed, also called tossing/turning) – we calculated the interruptions (WASO) as a percentage of bedtime (1 – efficiency). On the aggregate interruptions reduced from 21% to 14% (p- value 0.007) - a reduction of about a third.
Onset Latency:
Personalized tACS stimulation reduced the time taken to fall asleep to 6.7 min compared to 14.7 min for sham, a significant 8 min improvement over sham condition (p-value 0.009) (Table 1). It has cut the time taken to fall asleep by over half, across the group. In contrast, Melatonin reduces onset latency by 4 minutes [37].
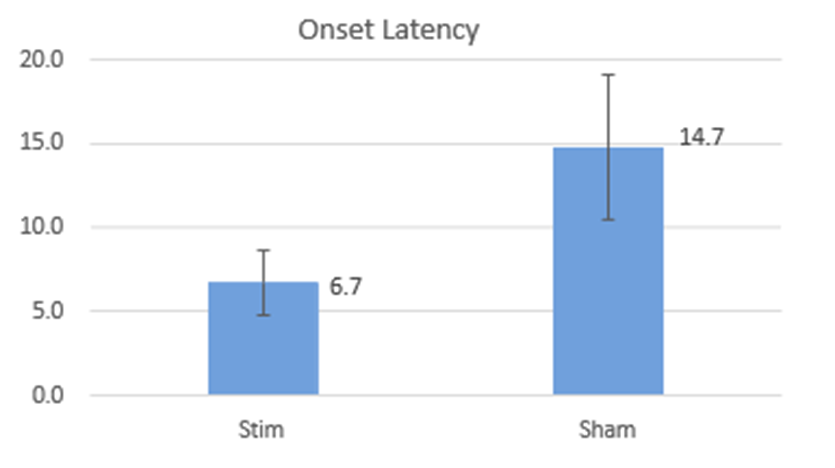
Figure 3: Onset Latency Comparison
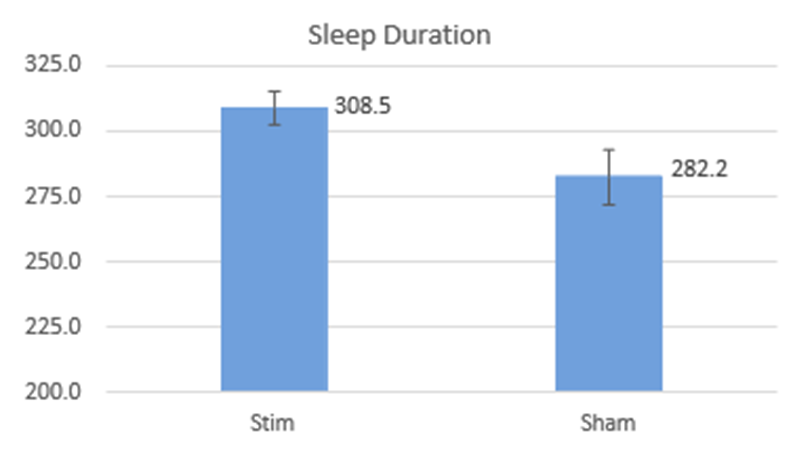
Sleep Duration:
Personalized tACS stimulation added 26.3 minutes of sleep on average across the group (308.5 minutes in Stim vs. 282.2 minutes in sham, p-value 0.008). For context, Melatonin adds 12.8 minutes of sleep [37].
Discussion
To date, research has shown that non-invasive stimulations of varied forms can improve sleep quality [5] [6] [7] [8]. These methods include tDCS, tACS, and rTMS that modulate the electrical brain activity during sleep in an open loop i.e., fixed-stimulation manner. Studies with tACS and rTMS protocols targeting oscillatory patterns in different frequency bands (0.5Hz to 16Hz) using fixed stimulation waveforms across all subjects have shown improvements in different sleep metrics [21][39]. Additionally, invasive pharmaceutical interventions such as sleeping pills (Ambien) and Melatonin have also demonstrated varying levels of effectiveness in enhancing sleep [36][37][38]. The current study took a different approach. Specifically, the study tested whether a novel personalized tACS stimulation with multiple frequencies blended, would improve sleep. In addition, this study did stimulation before (rather than during) sleep. With participants aware of stimulation sensations, this approach has been selected based on multiple studies showing that the benefits of stimulation last well beyond the stimulation period [10][11][29]. This study has shown the efficacy of personalized tACS stimulation in improving sleep onset, duration and sleep efficiency. A study [40], done in a user’s home setting, has explored the comparison of personalized stimulation vs fixed stimulation (using fixed 5Hz, 10Hz representation for theta and alpha bands rather than individual specific peaks). It shows that personalized tACS is indeed more efficacious in improving sleep outcomes. In addition, it showed that participants with severe insomnia benefited more from this personalized stimulation approach.
Conclusions
Personalized electrical brain stimulation that targets specific brainwave frequencies shows promise as a way to improve sleep quality. This method could become a valuable therapeutic option in the future.
Funding
This study was internally funded by StimScience Inc. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscripts.
Conflicts Of Interest
V. Ayanampudi, A.Krishnan, and R.Gurumoorthy were employed by StimScience Inc., and have equity positions in StimScience. All authors declare no other competing interests.
References
- Matthew P Walker, Sleep essentialism, Brain, Volume 144, Issue 3, March 2021, Pages 697-699, DOI: https://doi.org/10.1093/brain/awab026
View at Publisher | View at Google Scholar - Amir Qaseem, MD, PhD, MHA, Devan Kansagara, MD, MCR, Mary Ann Forciea, MD, Molly Cooke, MD, and Thomas D. Denberg, MD, PhD, Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians, Annals of Internal Medicine, 19 July 2016, DOI: https://doi.org/10.7326/M15-2175
View at Publisher | View at Google Scholar - Roneil G Malkani, Phyllis C Zee, Brain Stimulation for Improving Sleep and Memory, Sleep Medicine Clinics 2020 Mar 15(1), Pages 101-115, DOI: https://doi.org/ 10.1016/j.jsmc.2019.11.002
View at Publisher | View at Google Scholar - Sleep and Sleep Disorders: Data and Statistics. https://www.cdc.gov/sleep/data_statistics.html
View at Publisher | View at Google Scholar - Cristina Marzano, Fabio Moroni, Maurizio Gorgoni, Lino Nobili, Michele Ferrara, Luigi De Gennaro, How we fall asleep: regional and temporal differences in electroencephalographic synchronization at sleep onset, Sleep Medicine, Volume 14, Issue 11,2013, Pages 1112-1122, ISSN 1389-9457, DOI: https://doi.org/10.1016/j.sleep.2013.05.021.
View at Publisher | View at Google Scholar - Frase, L., Piosczyk, H., Zittel, S., Jahn, F., Selhausen, P., Krone, L., et al. Modulation of Total Sleep Time by Transcranial Direct Current Stimulation (tDCS). Neuropsychopharmacology 41, 2577–2586 (2016).
View at Publisher | View at Google Scholar - DOI: https://doi.org/10.1038/npp.2016.65
View at Publisher | View at Google Scholar - D’Atri, A., De Simoni, E., Gorgoni, M., Ferrara, M., Ferlazzo, F., Rossini, P.M., et al. Electrical Stimulation of the Frontal Cortex Enhances Slow-Frequency Eeg Activity and Sleepiness. Neuroscience, DOI: https://doi.org/10.1016/j.neuroscience.2016.03.007 (2016).
View at Publisher | View at Google Scholar - D’Atri, A., Scarpelli, S., Gorgoni, M., Alfonsi, V., Annarumma, L., Giannini, A.M., et al. “Bilateral Theta Transcranial Alternating Current Stimulation (tACS) Modulates EEG Activity: When tACS Works Awake It Also Works Asleep.” Nature and science of sleep vol. 11 343-356. 19 Nov. 2019, DOI: https://doi.org/10.2147/NSS.S229925
View at Publisher | View at Google Scholar - Basar, E. (1998). Brain Function and Oscillations: Principles and Approaches. Berlin, Heidelberg: Springer Berlin Heidelberg.
View at Publisher | View at Google Scholar - 10 .Thut, G., Schyns, P.G., and Gross, J. (2011). Entrainment of perceptually relevant brain oscillations by non-invasive rhythmic stimulation of the human brain. Front. Psychol. 2:170. DOI: https://doi.org/10.3389/fpsyg.2011.00170
View at Publisher | View at Google Scholar - HE W, Po-Yu Fong, Thomas Wai Hong leung, Ying-Zu Huang. Protocols of non-invasive brain stimulation for neuroplasticity induction. Neuroscience Letters (2018 vol 719), DOI: https://doi.org/10.1016/j.neulet.2018.02.045
View at Publisher | View at Google Scholar - Vosskuhl, J., Strüber, D. and Herrmann, C.S. (2018) Non-invasive Brain Stimulation: A Paradigm Shift in Understanding Brain Oscillations.Front. Hum. Neurosci. 12:211. DOI: https://doi.org/10.3389/fnhum.2018.00211
View at Publisher | View at Google Scholar - Bikson, M., Inoue, M., Akiyama, H., Deans, J.K., Fox, J.E., Miyakawa, H., Jefferys, J.G.R. Effects of uniform extracellular DC electric fields on excitability in rat hippocampal slices in vitro. J Physiol. 2004;557(Pt 1):175–190.
View at Publisher | View at Google Scholar - Chhatbar, P.Y., Chen, R., Deardorff, R., Dellenbach, B., Kautz, S.A., George, M.S., Feng, W. Safety and tolerability of transcranial direct current stimulation to stroke patients - A phase I current escalation study. Brain Stimul. 2017 May-Jun;10(3):553-559. doi: 10.1016/j.brs.2017.02.007. Epub 2017 Feb 27. PMID: 28279641; PMCID: PMC5411981. DOI: https://dx.doi.org/10.1016/j.brs.2017.02.007
View at Publisher | View at Google Scholar - Michael A. Nitsche and Marom Bikson. Extending the parameter range for tDCS: Safety and tolerability of 4 mA stimulation. DOI: https://doi.org/10.1016/j.brs.2017.03.002
View at Publisher | View at Google Scholar - Anna Fertonani, Clarissa Ferrari, Carlo Miniussi, What do you feel if I apply transcranial electric stimulation? Safety, sensations and secondary induced effects, Clinical Neurophysiology,Volume 126, Issue 11,2015,Pages 2181-2188,ISSN 1388-2457, DOI: https://doi.org/10.1016/j.clinph.2015.03.015.
View at Publisher | View at Google Scholar - Tadini, L., El-Nazer, R., Brunoni, A.R., Williams, J., Carvas, M., Boggio, P., et al. Cognitive, mood, and electroencephalographic effects of noninvasive cortical stimulation with weak electrical currents. J ECT. 2011;27:134–40.
View at Publisher | View at Google Scholar - Matar Haller, Thomas Donoghue, Erik Peterson, Paroma Varma, Priyadarshini Sebastian, Richard Gao, Torben Noto, Robert T. Knight, Avgusta Shestyuk, Bradley Voytek. Parametrizing neural power spectra. DOI: https://doi.org/10.1101/299859
View at Publisher | View at Google Scholar - Canolty, R. T., Edwards, E., Dalal, S. S., Soltani, M., Nagarajan, S. S., Kirsch, H. E., Berger, M. S., Barbaro, N. M., & Knight, R. T. (2006). High Gamma Power Is Phase-Locked to Theta Oscillations in Human Neocortex. Science, 313(5793), 1626–1628. DOI: https://doi.org/10.1126/science.1128115
View at Publisher | View at Google Scholar - Canolty, R. T., and Knight, R. T. (2010). The functional role of cross-frequency coupling. Trends Cogn. Sci. 14, 506–515. doi: 10.1016/j.tics.2010.09.001
View at Publisher | View at Google Scholar - Ngo, H.-V. V., Martinetz, T., Born, J., and Mölle, M. (2013b). Auditory closed-loop stimulation of the sleep slow oscillation enhances memory. Neuron 78, 545–553. DOI: https://doi.org/10.1016/j.neuron.2013.03.006
View at Publisher | View at Google Scholar - Grover, S., Nguyen, J., Reinhart, R. Synchronizing Brain Rhythms to Improve Cognition. Annual Review of Medicine, 2021, Vol 72, Pages 29-43. DOI: https://doi.org/10.1146/annurev-med-060619- 022857
View at Publisher | View at Google Scholar - van Bueren, N., Reed, T., Nguyen, V., et al. Personalized brain stimulation for effective neurointervention across participants. PLoS Computational Biology, 2021 Sep. DOI: https://doi.org/10.1371/journal.pcbi.1008886
View at Publisher | View at Google Scholar - Helfrich, R.F., Lendner, J.D., Mander, B.A., Guillen, H., Paff, M., Mnatsakanyan, L., Vadeera, S., Walker, M.P., Lin, J.J. and Knight, R.T. Bidirectional prefrontal-hippocampal dynamics organize information transfer during sleep in humans. Nature Communications, 10, Article number: 3572 (2019). DOI: https://doi.org/10.1038/s41467-019-11444-x, 10(1): 1-16, 2019. PMID: 31395890
View at Publisher | View at Google Scholar - Roth, Thomas, Insomnia: Definition, Prevalence, Etiology, and Consequences. J Clin Sleep Medicine 2007 Aug 15: 3(5 Suppl): S7-S10.
View at Publisher | View at Google Scholar - Okazaki, Yuka., Nakagawa, Yumi., Mizuno, Yuji., Hanakawa, Takashi., and Kitajo, Keiichi. Frequency- and Area-Specific Phase Entrainment of Intrinsic Cortical Oscillations by Repetitive Transcranial Magnetic Stimulation. Frontiers in Human Neuroscience, March 2021 DOI: https://doi.org/10.3389/fnhum.2021.608947
View at Publisher | View at Google Scholar - Vossen, Alexandra., Gross, Joachim., Thut, Gregor. Alpha Power Increase After Transcranial Alternating Current Stimulation at Alpha Frequency Reflects Plastic Changes Rather Than Entrainment. Brain Stimulation. Volume 8, Issue 3, P499-508, 2015. DOI: https://doi.org/10.1016/j.brs.2014.12.004
View at Publisher | View at Google Scholar - Huang, Wei., Stitt, Iain M., Negahbani, Ehsan., Passey, D.J., Ahn, Sangtae., Davey, Marshall., et al. Transcranial alternating current stimulation entrains alpha oscillations by preferential phase synchronization of fast-spiking cortical neurons to stimulation waveform. Nature Communications, 12, 2021 DOI: https://doi.org/10.1038/s41467-021-23021-2
View at Publisher | View at Google Scholar - Kasten, F.H., Dowsett, J., Herrmann, C.S. Sustained Aftereffect of α-tACS Lasts Up to 70 min after Stimulation. Frontiers in Human Neuroscience. 2016;10:245. Published 2016 May 25. DOI: https://10.3389/fnhum.2016.00245
View at Publisher | View at Google Scholar - Xie, Jiaxin , Wang, Lin., Xiao, Chao., Ying, Shaofei., Ren, Junru., Chen, Zhuo., et al. Low Frequency Transcranial Alternating Current Stimulation Accelerates Sleep Onset Process. IEEE Transactions on Neural Systems and Rehabilitation Engineering, Vol 29 2021. DOI: https://doi.org/ 10.1109/TNSRE.2021.3131728
View at Publisher | View at Google Scholar - Cantero, J., Atienza, M., Salas, R. Human alpha oscillations in wakefulness, drowsiness period, and REM sleep: different electroencephalographic phenomena within the alpha band. Clinical Neurophysiology Volume 32, Issue 1, Jan 2002 Pages 54-71. DOI: https://doi.org/10.1016/s0987-
View at Publisher | View at Google Scholar - 7053(01)00289-1
View at Publisher | View at Google Scholar - Donde, Clement., Brunelin, Jerome., Micoulaud-Franchi, Jean-Arthur., Maruani, Julia., Lejoyeux, Michel., Polosan, Mircea., Geoffroy, Pierre. The Effects of Transcranial Electrical Stimulation of the Brain on Sleep: A Systematic Review. Frontiers in Psychiatry June 2021. DOI: https://doi.org/10.3389/fpsyt.2021.646569
View at Publisher | View at Google Scholar - Yanhui Zhang, Yingzhi Lu, Dandan Wang, Chenglin Zhou, Chang Xu. Relationship between individual alpha peak frequency and attentional performance in a multiple object tracking task among ice-hockey players. PLOS ONE May 2021. DOI: https://doi.org/10.1371/journal.pone.0251443
View at Publisher | View at Google Scholar - Salinsky, M C., Osken, B S., Morehead L. Test-retest reliability in EEG frequency analysis. Electroencephalography and Clinical Neurophysiology. 1991 Nov. 382-392. DOI: https://10.1016/0013- 4694(91)90203-g
View at Publisher | View at Google Scholar - Zaehle, T., Rach, Stefan., Hermann, C. Transcranial Alternating Current Stimulation Enhances Individual Alpha Activity in Human EEG. PLoS One, 2010, Nov. DOI: https://doi.org/10.1371/journal.pone.0013766
View at Publisher | View at Google Scholar - Randall, S., Roehrs, T.A., Roth, T., Efficacy of Eight Months of Nightly Zolpidem: A prospective Placebo-Controlled Study. Sleep 2012 Nov 1: 35(11). DOI: https://doi.org/10.5665/sleep.2208
View at Publisher | View at Google Scholar - Brzezinski, A. et. al. Effects of exogenous melatonin on sleep: a meta-analysis. Sleep Medicine Reviews, Vol 9, Issue 1, 2009 Feb. DOI: https://doi.org/10.1016/j.smrv.2004.06.004
View at Publisher | View at Google Scholar - Wade, A.G., et. al. Efficacy of prolonged release melatonin in insomnia patients aged 55–80 years: quality of sleep and next-day alertness outcomes. Current Medical Research and Opinion, Vol 23, Issue 10, 2007 Sep. DOI: https://doi.org/10.1185/030079907X233098
View at Publisher | View at Google Scholar - Oroz, R. Kung S. Croarkin, P. Cheung, J. Transcranial magnetic stimulation therapeutic applications on sleep and insomnia: a review. Sleep Science and Practice. 5, Article 3, 2021. DOI: https://doi.org/10.1186/s41606-020-00057-9
View at Publisher | View at Google Scholar - Ayanampudi, V., Kumar, V., Krishnan, A., Walker, M.P., Ivry, R.B., Knight, R.T., Gurumoorthy, R. Personalized transcranial alternating current stimulation improves sleep quality: Initial findings. Frontiers in Human Neuroscience, 2023, Jan. DOI: https://doi.org/10.3389/fnhum.2022.1066453
View at Publisher | View at Google Scholar - Cohen, Michael., Where Does EEG Come From and What Does It Mean?. Trends in Neurosciences, April 2017, Vol. 40, No. 4. DOI: http://dx.doi.org/10.1016/j.tins.2017.02.004
View at Publisher | View at Google Scholar - Srinivasan, R., Winter, W., Nunez, Paul. Source analysis of EEG oscillations using high resolution EEG and MEG. Progress in Brain Research, Vol. 159. DOI: https://doi.org/10.1016/S0079-6123(06)59003-X
View at Publisher | View at Google Scholar - Thut, G., Miniussi, C. New insights into rhythmic brain activity from TMS–EEG studies. Trends in Cognitive Science, April 13, Pages 182-189. DOI: https://doi.org/10.1016/j.tics.2009.01.004
View at Publisher | View at Google Scholar
