

Research Article | DOI: https://doi.org/10.37579/2834-5142/022
Perforated Appendicitis: Can it be a Bedside Diagnosis?
- Maham Tariq 1
- Sara Malik 2
- Eesha Yaqoob 3*
- Mehwish Changez 4
- Saad Javed 5
- Ramlah Ghazanfor 6
- Ghulam Khadija 7
- Javaria Malik 8
- Bilal Ahmad 9
- Khawaja Rafay Ghazanfor 10
1MBBS, MRCS, FCPS, Rawalpindi, Pakistan.
2Postgraduate resident,Surgical Unit 1,Holy Family Hospital,Rawalpindi, Pakistan.
3PhD Sociology, Pir Mehr Ali Shah Arid Agriculture University, Rawalpindi, Pakistan 4-MBBS, MRCS, FCPS, Rawalpindi, Pakistan.
5Resident of neurosurgery, Department of Neurosurgery, Holy Family Hospital, Rawalpindi, Pakistan.
6MBBS, FCPS, Senior Registrar, Surgical unit 1, Holy Family hospital, Rawalpindi, Pakistan.
7MBBS, Postgraduate resident, surgical Unit 1, Holy Family hospital, Rawalpindi, Pakistan.
8MBBS, FCPS, Senior Registrar Medicine, District Headquarter Hospital, Rawalpindi, Pakistan.
9MBBS, Pakistan.
104th year medical student, CMH, Lahore, Pakistan.
*Corresponding Author: Eesha Yaqoob. PhD Sociology, Pir Mehr Ali Shah Arid Agriculture University, Rawalpindi, Pakistan 4-MBBS, MRCS, FCPS, Rawalpindi, Pakistan.
Citation: Maham Tariq, Sara Malik, Eesha Yaqoob, Mehwish Changez, Saad Javed, et al., (2024), Perforated Appendicitis: Can it be a Bedside Diagnosis? International Journal of Clinical Nephrology. 3(2); DOI:10.37579/2834-5142/022
Copyright: © 2024, Eesha Yaqoob. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 March 2024 | Accepted: 15 April 2024 | Published: 29 April 2024
Keywords: perforated appendicitis; acute appendicitis
Abstract
Appendicitis remains one of the most common causes of acute abdomen worldwide. It presents as a spectrum of disease ranging from an acutely inflamed appendix to a perforated one. where acutely inflamed can be managed conservatively, a perforated appendix always needs surgery to prevent complications like pelvic abscesses. Bedside diagnosis remains relevant in our setup.
Aims and objectives: To determine whether history, clinical examination, and basic laboratory investigations can help in confident bedside diagnosis of perforated appendicitis especially in the absence of sophisticated diagnostic modalities.
Materials And Methods: A retrospective case-control study was conducted. Hospital records of patients who underwent open appendectomy in the year 2016 were reviewed. Two groups of 100 patients each were made based on per operative findings. Appendices having macroscopic holes in the base or tip were labeled as perforated. Group A had acutely inflamed appendix and group b had perforated appendix. Patients’ demographic details were taken from hospital admission tickets. Findings of history and examination were retrieved from treating resident and operating surgeon's notes. Data were analyzed through SPSS.
Results: Out of 200 patients the total number of males was 102 (51%) and females were 98 (49%). Mean age was 24.13+9.73 in males and 18.7+ 6.4 in females of group A and 26.0+10.1 in males and 20.56+7.53 in females of Group B. Group B showed a significant delay in presentation to emergency after the onset of pain (P = 0.022). Upon history and clinical examination, the presence of anorexia, malaise, generalized abdominal pain, guarding, mass in right iliac fossa were significantly associated with perforation. Whereas gender, fever, vomiting, and dysuria showed no association with perforation.
Conclusion: Bedside conventional methods of history taking and examination remain a useful tool in anticipating perforated appendicitis. This helps surgeons in planning incisions and prioritizing patients on heavy operating lists. This remains especially relevant in resource- constrained setups where sophisticated modalities like CT scans are largely unavailable.
Introduction
Acute appendicitis remains one of the most frequent cases encountered on surgical emergency floors, worldwide. An open or laparoscopic appendectomy was once considered necessary in all cases. Recent guidelines suggest the use of antibiotics in uncomplicated episodes of appendicitis, which is supposed to be equally efficacious and less morbid [1,2]. However, the formidable state of perforated and gangrenous appendicitis remains an exception.
Differentiating between a perforated and simple appendicitis happens to be among the commonest parameters studied because of its contribution in guiding treatment and timing of surgery [3] and accuracy in predicting prospective intimidating complications like peritonitis, abscess formation, and postoperative intra-abdominal collection. [4]
Differentiate between a perforated and a non-perforated appendix has been a matter of great debate since both have overlapping presentations. Extremes of ages, increasing duration of symptoms, pyrexia, tenderness outside right lower quadrant, leukocyte count, C-Reactive Protein levels, Erythrocyte Sedimentation Rate levels neutrophil to lymphocyte ratio and high bilirubin count were good predictors of perforation according to several studies. Inturn these parameters will provide a useful guide between the conservative or surgical treatment of appendicitis, and early use of antibiotics. [5-9]
Despite this, a wide range of spectrums of presentation is displayed by both acute and perforated appendix and diagnosing them before surgery remains a dilemma to date. Hence, the importance of meticulous history taking and bedside examination of the patient by the consulting surgeon in clinching the diagnosis cannot be out shadowed. This coupled with lab findings is a useful aid in distinguishing both. Moreover, this can also help in planning incision i.e Gridiron vs Lanz incision, and surgical approach of open vs laparoscopic appendectomy.
Our study was aimed at analyzing the differences in signs, symptoms, and investigations to distinguish an acutely inflamed appendix from a perforated or gangrenous one preoperatively, in essence providing a reliable direction to proceed with.
Material And Methods
It was a case-control study conducted retrospectively. After permission from the hospital's ethical committee, medical records of all patients who underwent open appendectomy in surgical unit-1, Holy Family Hospital during the year 2016 were retrieved. Patients were separated into two groups: those with perforated and those with non-perforated appendicitis. There were 100 patients in each group. All patients were received in the emergency department by the on-call residents. History taking and clinical examination were performed by the registrars in charge. Per-operative findings documented in operation notes were also recorded. Those cases where a per-operatively macroscopic hole was noted in the appendix were labeled as perforated. Demographic information was collected from hospital admission forms. Data were analyzed by SPSS version 20. Chi-square and independent-sample t-test were used to analyze nominal and categorical data respectively. A p-value of <0>
Results
Two groups of 100 patients each were made. Group A had acutely inflamed appendix and group B had perforated appendix. The total number of males was 102 (51%) and females were 98 (49%). Demographic information of participants is given below in chart no 1.0
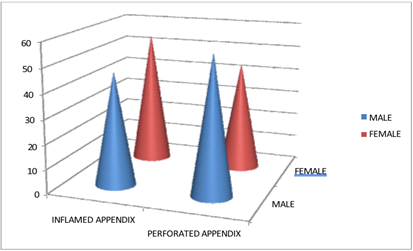
Chart no 1: Total number of respondents with respect to their sex
| Mean age | Inflamed appendix | Perforated appendix |
| Male | 24.13+9.73 | 26.0+10.1 |
| female | 18.7+ 6.4 | 20.56+7.53 |
Table no 1: Mean age of respondents according to their sex.
Table 1 showed that mean age was 24.13+9.73 in males and 18.7+ 6.4 in females of group A and 26.0+10.1 in males and 20.56+7.53 in females of Group B.
Group Statistics
Outcome prop | N | Mean (hours) | Std. Deviation | P value | |
| Pre-hospital onsetof | Inflamed | 100 | 60.3300 | 70.21483 | 0.022 |
| Pain | Perforated | 100 | 88.9100 | 101.93899 | 0.022 |
| Assessment time taken | Inflamed | 100 | 3.3100 | 4.77725 | 0.66 |
| By Emergency Surgeon | Perforated | 100 | 3.6700 | 6.63942 | 0.66 |
Mean duration of pain before presenting to hospital was found to be significantly longer in those with perforated appendix (p value <0>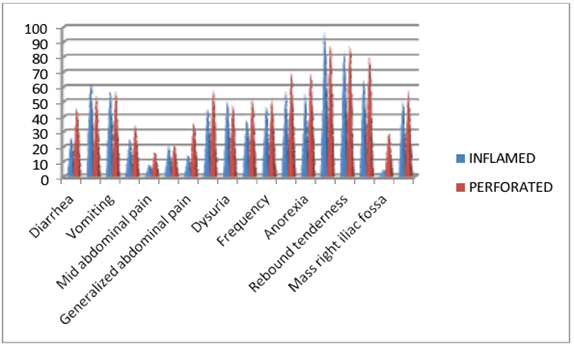
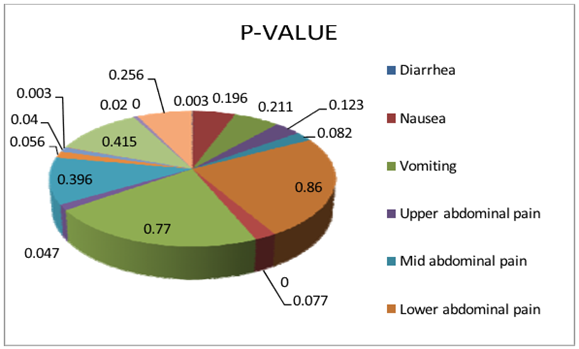
Nineteen factors in history and clinical examination were evaluated in both groups. Chi- square test showed that diarrhea, anorexia, malaise, right lumbar quadrant pain, generalized abdominal pain, tenderness and guarding in right iliac fossa on palpation, mass in right iliac fossa were significantly related to perforation. Whereas gender, nausea, fever, vomiting, pain in right iliac fossa, or dysuria were not found to be significant.
TLC was found to be significantly associated with perforation.
| outcome per- op | Mean | Std.Deviation | p-value |
totalleukocyte | inflamed | 9.8910 | 2.65654 | 0.00 |
count | perforated | 13.0411 | 4.06697 | 0.00 |
Discussion
Acute appendicitis is the most common cause of intra-abdominal surgery in the emergency setting, the world over. The lifetime risk of suffering from this condition is approximately 8%. [10] Historically it was believed that all cases of appendicitis if untreated will lead to perforation, gangrene and abscess formation. This concept changed at the turn of the century. Nowadays the term appendicitis is used as an umbrella term covering many situations from self-limiting episodes of inflammation to frank perforation and gangrenous appendix. No specific underlying mechanism has been explained for the fulminant course of disease in the latter cases.
The current body of literature shows promising results of conservative management in cases of mild acute appendicitis [2]. However, in cases where perforation has occurred, the evidence is unequivocally in favor of early surgical intervention. Therefore, the importance of the ability of an emergency resident in discriminating against these two situations cannot be overestimated [11].
Over the years several scoring systems have been devised to distinguish between these two entities. Various studies show CRP, neutrophil ratio, serum bilirubin CT scan to be very useful in the early and confident diagnosis of perforated appendicitis [12-14]. However, all these modalities are expensive and mostly unavailable in emergency setups of third world countries. Therefore, the age-old tools of history taking and bedside examination remain extremely useful in picking up cases of perforated appendicitis. In their 2010 guidelines, the American College of Emergency Physicians (ACEP) also recommends the use of clinical signs and symptoms in stratifying patients suspected of acute appendicitis [15]. This helps to hierarchize patients for surgery on crammed OR lists and forethinking incision for surgery.
In this study, 19 components of history and clinical examination were investigated. Among laboratory tests, only total leucocyte count was considered that is an affordable AND EASILY AVAILABLE test at even basic health facilities. Males have been reported present more often with perforated appendixes [16]. However, in our study, no significant dominance of either gender was observed (p-value). There was no significant difference in age was also found in both age groups. This is in contrast with existing studies found [17] On history taking anorexia, nausea, generalized abdominal pain, and right lumbar quadrant pain was more significant in the perforated appendix group. On clinical examination, tenderness, guarding and rigidity were more pronounced in group b. Palpation of a phlegmonous mass in right iliac fossa was also found in 24 cases of this group (p-value). Surprisingly rebound tenderness was not able to significantly differentiate between inflamed and perforated appendix. Raised TLC and tachycardia are two important components of the classical Alvarado s score. They were raised in all cases but significantly more so in group B (p-value < 0>
Conclusion
Despite diagnostic advancements, traditional bedside evaluation remains a relevant tool in the diagnosis of perforated appendicitis. Moreover, longer duration of pain and presence of atypical symptoms like right lumbar quadrant pain, anorexia and diarrhea should alert the treating surgeon as to the possibility of a perforated appendix.
References
- Salminen P, Paajanen H, Rautio T, Nordström P, Aarnio M, Rantanen T, et al. Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial. JAMA. 2015 Jun 16;313(23):2340–8.
View at Publisher | View at Google Scholar - Hansson J, Körner U, Khorram Manesh A, Solberg A, Lundholm K. Randomized clinical trial of antibiotic therapy versus appendicectomy as primary treatment of acute appendicitis in unselected patients. BJS. 2009;96(5):473–81.
View at Publisher | View at Google Scholar - Leeuwenburgh MM1, Wiezer MJ, Wiarda BM, Bouma WH, Phoa SS, Stockmann HB et al: Accuracy of MRI compared with ultrasound imaging and selective use of CT to discriminate simple from perforated appendicitis. Br J Surg. 2014 Jan;101(1): e147-55.
View at Publisher | View at Google Scholar - Rogers AP1, Zens TJ2, Leys CM2, Nichol PF2, Ostlie DJ2: A call for a standardized definition of perforated appendicitis. J Pediatr Surg. 2017 Jan;52(1):89-92.
View at Publisher | View at Google Scholar - Bröker ME1, van Lieshout EM, van der Elst M, Stassen LP, Schepers T: Discriminating between simple and perforated appendicitis. J Surg Res. 2012 Jul;176(1):79-83.
View at Publisher | View at Google Scholar - Sevinç MM1, Kınacı E2, Çakar E2, Bayrak S2, Özakay A2, Aren A2 et al: Diagnostic value of basic laboratory parameters for simple and perforated acute appendicitis: an analysis of 3392 cases Ulus Travma Acil Cerrahi Derg. 2016 Mar;22(2):155-62.
View at Publisher | View at Google Scholar - Oliak D1, Yamini D, Udani VM, Lewis RJ, Vargas H, Arnell T et al: Can perforated appendicitis Be diagnosed preoperatively based on admission factors? J Gastrointest Surg. 2000 Sep-Oct;4(5):470-4.
View at Publisher | View at Google Scholar - Augustin T1, Cagir B, Vandermeer TJ: Characteristics of perforated appendicitis: effect of delay is confounded by age and gender. J Gastrointest Surg. 2011 Jul;15(7):1223-31.
View at Publisher | View at Google Scholar - Gofrit ON1, Abu-Dalu K: Perforated appendicitis in the child: contemporary experience. Isr Med Assoc J. 2001 Apr;3(4):262-5.
View at Publisher | View at Google Scholar - Findlay JM, Kafsi J el, Hammer C, Gilmour J, Gillies RS, Maynard ND. Nonoperative Management of Appendicitis in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Am Coll Surg. 2016 Dec 1;223(6):814-824.e2.
View at Publisher | View at Google Scholar - Bundy DG, Byerley JS, Liles EA, Perrin EM, Katznelson J, Rice HE. Does this child have appendicitis? JAMA. 2007 Jul 25;298(4):438–51.
View at Publisher | View at Google Scholar - Omari AH, Khammash MR, Qasaimeh GR, Shammari AK, Yaseen MKB, Hammori SK. Acute appendicitis in the elderly: risk factors for perforation. World J Emerg Surg WJES. 2014 Jan 15;9(1):6.
View at Publisher | View at Google Scholar - Panagiotopoulou IG, Parashar D, Lin R, Antonowicz S, Wells A, Bajwa F, et al. The diagnostic value of white cell count, C-reactive protein and bilirubin in acute appendicitis and its complications. Ann R Coll Surg Engl. 2013 Apr 1;95(3):215–21.
View at Publisher | View at Google Scholar - Sand M, Bechara FG, Holland-Letz T, Sand D, Mehnert G, Mann B. Diagnostic value of hyperbilirubinemia as a predictive factor for appendiceal perforation in acute appendicitis. Am J Surg. 2009 Aug 1;198(2):193–8.
View at Publisher | View at Google Scholar - Leung Y, Chan CP, Graham CA, Rainer TH. Acute appendicitis in adults: Diagnostic accuracy of emergency doctors in a university hospital in Hong Kong. Emerg Med Australas. 2017;29(1):48–55.
View at Publisher | View at Google Scholar - Balogun OS, Osinowo A, Afolayan M, Olajide T, Lawal A, Adesanya A. Acute Perforated Appendicitis in Adults: Management and Complications in Lagos, Nigeria. Ann Afr Med. 2019;18(1):36–41.
View at Publisher | View at Google Scholar - Hanson KA, Jacob D, Alhaj Saleh A, Dissanaike S. In-hospital perforation risk in acute appendicitis: Age matters. Am J Surg. 2019 Jun 5.
View at Publisher | View at Google Scholar - Naderan M, Babaki AES, Shoar S, Mahmoodzadeh H, Nasiri S, Khorgami Z. Risk factors for the development of complicated appendicitis in adults. Turk J Surgery Ulusal Cerrahi Derg. 2016 Mar 1;32(1):37–42.
View at Publisher | View at Google Scholar - Bickell NA, Aufses AH, Rojas M, Bodian C. How time affects the risk of rupture in appendicitis. J Am Coll Surg. 2006 Mar;202(3):401–6.
View at Publisher | View at Google Scholar - Papaziogas B, Tsiaousis P, Koutelidakis I, Giakoustidis A, Atmatzidis S, Atmatzidis K. Effect of time on risk of perforation in acute appendicitis. Acta Chir Belg. 2009 Feb;109(1):75–80.
View at Publisher | View at Google Scholar - Narsule CK, Kahle EJ, Kim DS, Anderson AC, Luks FI. Effect of delay in presentation on rate of perforation in children with appendicitis. Am J Emerg Med. 2011 Oct;29(8):890–3.
View at Publisher | View at Google Scholar
