

Case Report | DOI: https://doi.org/10.31579/2835-9291/014
Pembrolizumab-Associated Steven Johnson Syndrome in a Patient with Metastatic Non-Squamous Lung Cancer: A Rare Presentation and Review of the Literature
Department of Internal Medicine, SUNY Upstate Medical University, 750 East Adams Street, Syracuse, NY, 13210, USA.
*Corresponding Author: Binod KC, Department of Internal Medicine, SUNY Upstate Medical University, 750 East Adams Street, Syracuse, NY, 13210, USA.
Citation: Binod KC, MBBS, Moeed R. Chohan, MD, Michael Sandhu, Jensih Bhandari, Harvir Gambhir, MD, (2023), Hemoperitoneum Due to Trauma in the Superior Pancreatic Artery, International Journal of Clinical Case Studies,2(6); DOI:10.31579/2835-9291/014
Copyright: © 2023, Binod KC. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 November 2023 | Accepted: 04 December 2023 | Published: 29 December 2023
Keywords: immunotherapy related adverse effects; pembrolizumab; toxic epidermal necrolysis
Abstract
We present a rare case of Stevens-Johnson Syndrome (SJS) occurring in a 75-year-old female, fourteen days after receiving the first dose of Pembrolizumab therapy to treat stage IV non-small cell carcinoma of lungs with metastasis to the brain. Pembrolizumab is a monoclonal antibody that binds to the programmed death-1 receptor and is approved for treatment of several malignancies. Although pruritus and papular, erythematous rash are documented after its use, severe reactions such as Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis (TEN) are rare. This case highlights the phenomenon of SJS and TEN-associated adverse reactions, even after the first dose, for patients receiving pembrolizumab.
Introduction
SJS and TEN are severe cutaneous drug eruptions characterized by extensive necrosis and detachment of the epidermis. Mortality from this can be as high as 35% and most often presents as an adverse drug reaction. [1], [2] Medications most commonly associated with SJS/TEN include Beta-Lactams, NSAIDs, anticonvulsants, barbiturates, and allopurinol. They are rarely reported with immune checkpoint inhibitors (ICIs) such as pembrolizumab. [2]. Our patient presented with SJS only fourteen days after receiving the first dose of pembrolizumab therapy for the treatment of metastatic stage IV non-small cell carcinoma of lungs.
Case presentation
A75-year-old female with stage IV non-small cell lung cancer complicated by multiple metastatic brain lesions presented to the hospital with new-onset rash. She received whole-brain radiotherapy for brain metastasis thirty days before the first dose of pembrolizumab 200 mg intravenously.
Fourteen days after the first dose of pembrolizumab, she noticed a rash and itching. The rash began over the lower extremities and eventually progressed to the upper abdomen, back, and upper extremities, subsequently blistering. She then developed significant pain and presented to the oncology clinic. Here she received intravenous methylprednisolone 60 mg once, followed by prednisone 60 mg daily and was advised to continue prednisone until the next office visit. However, her symptoms continued to worsen, and she presented to an outside hospital. She was transferred to our institution for comprehensive dermatology evaluation and further management.
Upon presentation, physical examination revealed widespread erythematous papules and papulovesicular changes involving bilateral upper and lower extremities as well as the abdomen. She had blistering lesions, most prominent on the feet and thigh. She also had sloughed-off skin on the upper back and bilateral shoulders, demonstrated in figures 1–4 below. Conjunctival injection of both eyes involvement of the oral mucosa was appreciated, and there was no genital mucosa involvement. Skin punch biopsies from the abdomen were obtained which showed normal stratum corneum, vacuolar interface dermatitis, individual cell necrosis, and subepidermal bulla formation (Figure 5), which support a diagnosis of Erythema Multiforme/SJS/TEN. Due to the patient’s rapid progression, clinical morphology, and pathology consistent with SJS, the decision to initiate treatment for SJS was made. The patient was treated with intravenous immunoglobulin (IVIG) 1gm/kg/day for three days followed by methylprednisolone IV 60mg daily for eight days alongside ongoing supportive care. Her methylprednisolone was transitioned to oral prednisone 60 mg and tapered over thirty days. She also received Sulfamethoxazole-Trimethoprim 800-160 mg oral daily for Pneumocystis carinii (PCP) prophylaxis during her hospital stay. At the time of discharge, her rash and symptoms had improved significantly.
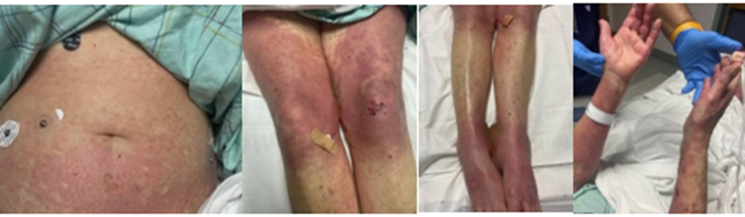
Figure - 1 Figure - 2 Figure- 3 Figure- 4
Figure 1- 4: Widespread erythematous cutaneous papules and patches with the detachment of large sheets of necrolytic epidermis over the abdomen, lower and upper extremities involving more than 30% BSA.
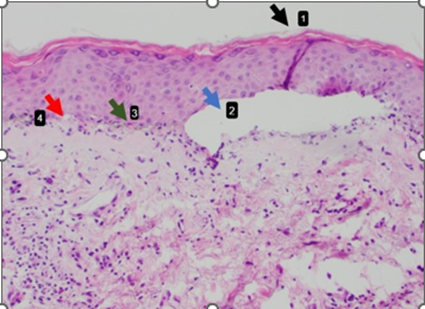
Figure 5. Abdomen skin biopsy shows 1. Normal stratum corneum, 2. subepidermal bulla formation, 3. individual cell necrosis, 4. vacuolar interface dermatitis
Discussion
Pembrolizumab is a commonly used humanized monoclonal IgG4 antibody approved as a therapy for various malignancies, including non-small cell lung cancer (as used in our patient), Hodgkin lymphoma, late-stage melanoma, and gastric cancer. The mechanism of action of this drug involves disruption of the interaction between the programmed cell death (PD-1) receptor and PD-1 ligands (PDL-1)- [1]
Adverse effects of pembrolizumab vary from commonly seen mild effects such as pruritus and papulo-erythematous rash to severe and rarely encountered reactions including SJS/TEN as presented in our patient [3], [4] Clinically, discussing the spectrum of SJS/TEN: SJS involves 10% of the body surface area (BSA), SJS/TEN overlap involves 10%–30% BSA, and TEN involves 30% BSA.[2]. TEN is a life-threatening drug reaction that usually begins as painful red coalescent erythema and progresses to bulla formation with areas of epidermal detachment with mucosal involvement [2].
The severity if SJS/TEN is defined based on the Severity of Illness Score for Toxic Epidermal Necrolysis (SCORTEN). SCORTEN is used to estimate mortality in patients presenting with SJS/TEN based on the patient’s history, current vital signs, and laboratory values. In our case, our patient’s initial SCORTEN was a 3, consistent with an estimated mortality of 35.3%.
The interval between drug initiation and SJS/TEN is approximately 5 to 28 days. [4]. Clinical correlation with histopathological findings such as full-thickness epidermal necrolysis, subepidermal bulla formation, individual cell necrosis, and vacuolar interface dermatitis is essential in making the diagnosis of SJS/TEN. In our case, the cutaneous eruption started fourteen days after the first dose of pembrolizumab. The differential diagnosis based on histology included SJS/TEN, erythema multiforme, severe graft versus host disease, and a bullous fixed drug eruption. The decision to promptly initiate IVIG was made in consultation with dermatology due to the rapid progression and lack of improvement with outpatient steroid treatment, most consistent with SJS. Our patient also exhibited oral mucosal involvement and conjunctival involvement, however, did not exhibit genital mucosal involvement.
The management of SJS/TEN secondary to immunotherapy is mainly supportive and includes discontinuing the offending drug, initiating short-term pulse-dosed corticosteroids, cyclosporine, intravenous methylprednisolone at 1– 2 mg/kg/day, and close monitoring for acute complications of fluids and electrolyte imbalance, renal failure, bacteremia, hypercatabolic state, insulin resistance, and multiple organ dysfunction syndromes. In severe cases, IVIG can be used. Upon complete re-epithelialization, corticosteroid therapy should be tapered over a minimum of four weeks. [2][3][5]. Therefore, we present a rare yet life-threatening complication of SJS seen with the immune checkpoint inhibitor, pembrolizumab, as well as its management with IVIG and long-term corticosteroids.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- R. Abe, “Immunological response in Stevens–Johnson syndrome and toxic epidermal necrolysis,” The Journal of Dermatology, vol. 42, no. 1, pp. 42–48, Jan. 2015
View at Publisher | View at Google Scholar - S. Robinson, J. Saleh, J. Curry, and K. Mudaliar, “Pembrolizumab-Induced Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis in a Patient with Metastatic Cervical Squamous Cell Carcinoma: A Case Report,” American Journal of Dermatopathology, vol. 42, no. 4, 2020,
View at Publisher | View at Google Scholar - R. Kumar and S. Bhandari, “Pembrolizumab induced toxic epidermal necrolysis,” Current Problems in Cancer, vol. 44, no. 2, 2020,
View at Publisher | View at Google Scholar - Z. R. Cai et al., “Toxic epidermal necrolysis associated with pembrolizumab,” Journal of Oncology Pharmacy Practice, vol. 26, no. 5, 2020,
View at Publisher | View at Google Scholar - P. C et al., “Treatment of toxic epidermal necrolysis with high-dose intravenous immunoglobulins: multicenter retrospective analysis of 48 consecutive cases,” Archives of dermatology, vol. 139, no. 1, pp. 26–32, Jan. 2003,
View at Publisher | View at Google Scholar
