

Research Article | DOI: https://doi.org/10.31579/2835-835X/067
Pancreatic tuberculosis presenting as unusual presentation of obstructive jaundice mimicking pancreatic malignancy: surgeon's dilemma
1 Senior Professor, General Surgery, ESIC MCH, Faridabad, Haryana.
2 Postgraduate student, General Surgery, ESIC MCH, Faridabad, Haryana.
3 Senior Professor, General Surgery, ESIC MCH, Faridabad, Haryana.
*Corresponding Author: Sunder Goyal, Senior Professor, General Surgery, ESIC MCH, Faridabad, Haryana.
Citation: Sunder Goyal, Renu, Vimal Bhandari, (2024), Pancreatic tuberculosis presenting as unusual presentation of obstructive jaundice mimicking pancreatic malignancy: surgeon's dilemma, Clinical Trials and Case Studies, 3(4); DOI:10.31579/2835-835X/067
Copyright: © 2024, Sunder Goyal. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 April 2024 | Accepted: 22 May 2024 | Published: 22 July 2024
Keywords: extrapulmonary tuberculosis; pancreas
Abstract
Introduction: Tuberculosis (TB) can affect any organ in the human body. Abdominal tuberculosis forms an important type of extrapulmonary tuberculosis, which commonly affects the ileocecal region. Organs like the liver, spleen, and kidneys also tend to be affected by the disease. Pancreatic tuberculosis, however, is an extremely rare form of TB, especially in isolated form. When it occurs in the pancreas, it can mimic autoimmune pancreatitis, pancreatic abscess or pancreatic carcinoma clinically as well as radiologically. Only a few cases where Pancreatic TB presents as an unusual presentation of obstructive jaundice mimicking pancreatic malignancy have been reported till now. Here, we describe a case of pancreatic TB presenting as a unique presentation of obstructive jaundice mimicking pancreatic carcinoma, which was effectively treated with antitubercular medications.
Case report: A 39-year-old female presented to the Surgery OPD with a dull ache in the epigastric region and yellowish discolouration of her eyes. There was also H/O loss of appetite & weight, dark-coloured urine and clay-coloured stool. The clinical examination revealed a soft, non-tender, vague mass palpable in the epigastric region. USG's abdomen showed a mass in the area of the head of the pancreas with dilated CBD and peri-pancreatic lymphadenitis. Hence, a CECT scan of the abdomen was done, which showed a heterogeneously hyper-enhancing ill-defined lesion involving the peri-ampullary region with significant retroperitoneal lymph adenopathy. Blood tumour markers were within normal levels. The PET scan did not reveal any metastasis. As the pancreatic mass was resectable, the patient was planned for exploratory laparotomy with proceed. Intraoperative frozen sections of doubtful peripancreatic lymph node and pancreatic mass, which showed epithelioid granulomas surrounded by lymphocytic infiltrates, were sent. Ziehl-neelsen (ZN) stain was positive for Acid Fast Bacilli. Hence, a diagnosis of tuberculosis was made, and she was put on Antitubercular treatment.
Conclusion: Pancreatic tuberculosis is rare but a possible differential for a patient presenting with an unusual presentation of obstructive jaundice mimicking pancreatic malignancy.
Introduction
Tuberculosis (TB) is present worldwide and in all age groups. Worldwide, TB is the second main infectious killer after COVID-19 (above HIV and AIDS). In 2022, an estimated 10.6 million people suffered from TB worldwide. The incidence rate of TB increased by 3.6% in 2021 relative to 2020. But in Bharat, TB patients fell marginally to 2.23 million in 2023 from 2.42 million in 2022. Incidence of extrapulmonary TB was 17% among total diagnosed TB cases globally and most commonly involves LN, pleura, GIT or abdomen.1 Involvement of the pancreas is rare, and its reported incidence is only 0.46% among patients with TB. [1] Pancreatic TB is a rare condition that can mimic pancreatic carcinoma clinically as well as radiologically. [2] Most cases are diagnosed with a high index of suspicion in mind and confirmed only after histopathological study as the clinical symptoms are vague, such as acute pancreatitis, gastrointestinal bleeding, obstructive jaundice or an isolated pancreatic mass resembling pancreatic carcinoma. All this makes pancreatic TB a very challenging diagnosis for treating surgeons. A few cases of coexisting pancreatic TB and carcinoma have been reported in the literature. [3] The development of abdominal TB can be independent of pulmonary involvement and mostly involves the liver, bowels, spleen, peritoneum, and mesenteric lymph nodes (LN). Undoubtedly, the pancreas is relatively immune to tuberculosis due to its retroperitoneal position and antibacterial pancreatic factors in its secretions; still, isolated cases of pancreatic TB can occur.[2] As TB can be effectively treated with antitubercular treatment, awareness of TB involvement in the pancreas could help in disease management and unnecessary Whipple's pancreaticoduodenectomy.[4]
Case Report
A 39-year-old female presented to the Surgery OPD with upper abdominal pain and yellowish discolouration of eyes associated with loss of appetite, significant weight loss of 12 kg in 3 months duration, dark-coloured urine and clay-coloured stool. There was no history of itching or melena. The patient did not have any comorbidities or a history of past surgeries. All vitals were within normal limits. The abdominal examination revealed a soft, non-tender abdomen with an ill-defined mass palpable in the epigastric region. Her complete blood counts, renal function and coagulation profile were within normal limits. Her liver function shows increased total bilirubin, direct bilirubin and alkaline phosphatase. USG's abdomen reported a mass in the area of the head of the pancreas with dilated CBD and dilated gall bladder with a polyp and peri-pancreatic lymphadenitis. Hence, a CECT scan (Fig-1) of the abdomen was done, which showed a heterogeneously hyper-enhancing ill-defined lesion involving the peri-ampullary region at the distal end of CBD, causing upstream dilatation. Blood tumor marker levels, including CA 19-9 and CEA, were within the the normal range. A PET scan was done, which showed no metastasis. As the pancreatic mass was resectable, the patient was planned for exploratory laparotomy with proceed. Intraoperative frozen sections of peripancreatic lymph node and pancreatic mass were sent, which showed epithelioid granulomas surrounded by lymphocytic infiltrates (Fig-2). Ziehl-neelsen (ZN) stain done was positive for Acid Fast Bacilli. Hence, a diagnosis of tuberculosis was made, and she was put on Antitubercular treatment. At the 3-month follow-up, the patient was asymptomatic and was doing well, and radiological imaging showed complete resolution of the lesion.
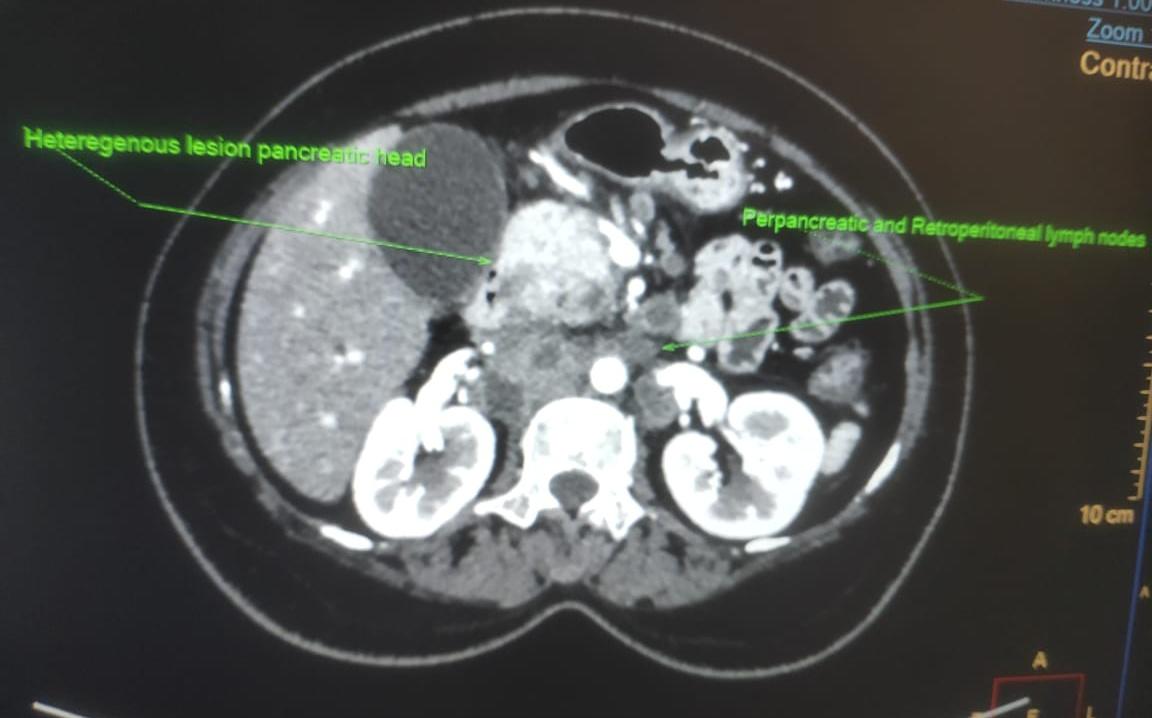
Figure 1: Axial CECT view showing pancreatic mass with enlarged retroperitoneal LNs
Discussion
The incidence of TB is still high in developing countries as well as in people with compromised immunity. Incidence of extrapulmonary TB was 17% among total diagnosed TB cases globally and most commonly involves LN, pleura, GIT or abdomen. Involvement of the pancreas is rare and is about 0.4% of total TB patients. Pancreatic tissue is relatively immune to infection by Mycobacterium tuberculosis due to its retroperitoneal location, thus protected from direct exposure and also due to antimycobacterial effects of pancreatic secretions full of enzymes like lipase and deoxyribonuclease extracts. [5] The possible mechanisms by which the pancreas is involved are:[6]
- Haematogenous spread (miliary tuberculosis) of tubercle bacilli from lungs or other abdomen organs to the pancreas.
- In cases of isolated pancreatic TB- Direct spread from contiguous retroperitoneal lymph nodes as possible in our case. Here, the main cause can be M. bovis.
- Isolated localized pancreatic TB -may be due to the spread of Ileocaecal TB [7]
In 1944, Auerbach reported that only 4.7% (14 of 1656 autopsies of tuberculous patients) of cases had pancreatic involvement.[8] However, Nagar et al. (1999–2004) reported an incidence of pancreatic TB in about 8.3% of patients diagnosed with abdominal TB.[9]
In various studies done, pancreatic TB is most commonly seen in young people, especially females (as in this case), while pancreatic tumours are mostly seen in older people. Pancreatic TB is also mainly seen in patients who live in TB-endemic areas in less developed nations and immunocompromised patients. The main symptoms consist of abdominal pain (75%–100%), loss of appetite and weight (69%), fever with night sweats (50%), anaemia (50%), and obstructive jaundice (30%).[5] and gastrointestinal bleeding in a few cases. Diagnostic techniques used for pancreatic TB can be invasive and noninvasive. Pancreatic mass can be diagnosed by USG or CT scan. However, it has low helpfulness in the diagnosis of pancreatic TB. The diagnosis can be confirmed only after the biopsy specimen is studied after exploratory laparotomy, as in this case. There should be a high index of clinical suspicion where the retroperitoneal lymph nodes are caseated or calcified. A CT-guided FNAC of mass or laparoscopic biopsy can avoid unnecessary laparotomy. Thus, for final diagnosis, microbiological and histopathological confirmation is essential. Therefore, the most vital factor in the diagnosis of pancreatic TB mass is a high index of suspicion, particularly in younger female patients, because the symptoms and imaging findings may resemble pancreatic carcinoma.
Pancreatic TB is very difficult to diagnose, but once diagnosed, it is easy to treat as it responds well to standard ATT as for any other extrapulmonary TB. [10] Standard ATT involving at least four drugs remains the keystone of therapy.[6]
Conclusion
Abdominal TB has varied and non-specific symptomatology, so, most of the time, pancreatic TB is usually difficult to diagnose, needing a high index of clinical suspicion. Hence, TB should always be considered the differential diagnosis of pancreatic masses.
References
- K Bharat, C Vijayakumar, TP Elamurugan, Sudharsanan S, Sadasivan J (2019). Primary Pancreatic Tuberculosis: A Rare Case Report. Adv Res Gastroentero Hepatol; 13(2): 555858.
View at Publisher | View at Google Scholar - Dr. Richa Shrestha., Prof. Dr. Anup Sharma., Dr. Pooja Baidya., Dr. Milan Adhikari 1 JNGMC Vol. 21 No. 1 July 2023.
View at Publisher | View at Google Scholar - Z.-J. Zneng, H. Zhang, G.-M. Xiang, et.al (2011). Coexistence of pancreatic carcinoma and pancreatic tuberculosis; case report. Gutand Liver, vol 5, no. 4, pp. 536-538.
View at Publisher | View at Google Scholar - Shahrokh S, Miri MB, Safari MT, Alizadeh AH (2015). Pancreatic tuberculosis: An overview. J Pancreas Online; 16:232–8.
View at Publisher | View at Google Scholar - Abbaszadeh M, Rezai J, Hasibi M, Larry M, Ostovaneh MR, et al (2017). Pancreatic tuberculosis in an immunocompetent patient: A case report and review of the literature. Middle East J Dig Dis; 9:239–41.
View at Publisher | View at Google Scholar - Jethwani U, Singh G, Mohil RS, Kandwal V, Chouhan J, et al (2013). Pancreatic tuberculosis: A case report. OA Case Report; 2:41.
View at Publisher | View at Google Scholar - Elizondo ME, Arratíbel JA, Compton CC, Warshaw AL(2001). Tuberculosis of the pancreas. Surgery; 129:114–16.
View at Publisher | View at Google Scholar - Auerbach O (1944). Acute generalized miliary tuberculosis. Am J Pathol ;20: 121–36.
View at Publisher | View at Google Scholar - Nagar AM, Raut AA, Morani AC, Sanghvi DA, Desai CS,et.al (2009). Pancreatic tuberculosis: A clinical and imaging review of 32 cases. J Comput Assist Tomogr ;33:136–41.
View at Publisher | View at Google Scholar - Kim JB, Lee SS, Kim SH, Byun JH, Park DH,et al (2014). Peripancreatic tuberculous lymphadenopathy masquerading as pancreatic malignancy: A single-centre experience. J Gastroenterol Hepatol; 29:409–16.
View at Publisher | View at Google Scholar
