

Review Article | DOI: https://doi.org/10.31579/2835-2882/040
Pain Management During Pregnancy and Lactation
1Riggs Pharmaceutical Karachi, Pakistan
2Head of the Department of Pharmacology,
3Fazaia Ruth Pfau Medical College, Shahrahe Faisal Karachi,
4Department of Microbiology, University of Karachi, Pakistan,
5GD Pharmaceutical Inc OPJS University Rajasthan
6Assistant Professor Dow University of Health sciences
*Corresponding Author: Rehan Haider, Riggs Pharmaceutical Karachi, Pakistan.
Citation: Rehan Haider, Asghar Mehdi, Fazaia Ruth Pfau, Anjum Zehra, Geetha Kumari, et al. (2023), Pain Management During Pregnancy and Lactation, Clinical Research and Studies, 2(6); DOI:10.31579/2835-2882/040
Copyright: © 2024, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 December 2023 | Accepted: 15 December 2023 | Published: 22 December 2023
Keywords: pain management; pregnancy; lactation; pharmacological interventions non-pharmacological interventions; fetal development; breastfeeding; maternal health; opioid use; interdisciplinary approach
Abstract
Pregnancy and lactation are important stages in a woman's existence, and pain management becomes a difficult problem at some point. The well-being of each mother and the growing fetus or breastfeeding toddler must be cautiously considered when selecting appropriate pain management techniques. This abstract evaluates modern knowledge and guidelines for pain control during pregnancy and lactation, focusing on the dangers and advantages of numerous pharmacological and non-pharmacological interventions.
During pregnancy, women usually experience physiological changes that may exacerbate their current pain conditions or result in new ones. The use of certain pain medications, especially nonsteroidal anti-inflammatory capsules (NSAIDs) and opioids, has been linked to potentially destructive effects on fetal development. Consequently, healthcare providers often choose non-pharmacological interventions, including physical therapy, acupuncture, and relaxation techniques, as first-line remedies. Furthermore, a thorough evaluation of the risk-to-benefit ratio is essential when considering the use of any medication throughout pregnancy, and a session with a healthcare expert is important.
During the lactation period, the ability to transfer medication through breast milk to infants raises issues regarding the protection of medications used for pain management. Healthcare companies have to remember the drug's pharmacokinetics, its potential effect on the little one's health, and the mother’s potential to care for the infant while on medicine. Opioid use at some point during breastfeeding is a concern because of the hazards of sedation, respiratory despair, and withdrawal signs inside the infant. In comparison, a few medicines are considered, especially those that are safe throughout lactation, and alternative non-pharmacological interventions have to be explored where possible.
An interdisciplinary approach involving obstetricians, anesthesiologists, pediatricians, and lactation consultants is essential for developing comprehensive pain control plans during pregnancy and lactation. Alternatively, pain relief for the mother is critical to ensuring her well-being and a successful bond with the little one. Concurrently, minimizing any capacity risk to the fetus or breastfeeding infants is of maximum significance. Moreover, affected person education and shared selection-making play a critical role in supporting ladies to make informed choices about pain management strategies that stabilize their pain alleviation wishes and the safety of their unborn or breastfeeding child
Introduction
Pain lawsuits commonly arise in both pregnant and lactating women. Nonpharmacologic methods to treat pain throughout pregnancy and lactation, these factors need to be taken into consideration before turning to pharmacologic retailers, due to the fact nearly all pills administered to the mother pass the placenta to the fetus or are secreted in breast milk.{1} The mechanisms of drug delivery are much like the shipping of medication across any membrane. {2, 3} Diffusion is more often than not passive and the drug awareness inside the umbilical vein or breast milk relies upon the concentration gradient, drug lipid solubility, diploma of ionization and protein binding, and the diffusion ability of the membrane (this might also trade as pregnancy progresses).{4} The consequences for The fetus or nursing infant will rely on the gestational or post-conceptual age, as well as the quantity and duration of drug publicity, and the unique drug inside the United States of America; non-opioid and opioid analgesics are typically ingested throughout pregnancy. {5,6} The benefit of analgesic medicines must justify the hazard (e.g., the untreated illness may pose a greater hazard to the fetus than the medicines used to deal with the illness) and the minimum powerful dose that needs to be used. Attention must be paid to the use of Nonpharmacological methods of pain control or the use of non-systemic techniques of drug administration.
Drugs During Pregnancy Pharmacokinetic Changes During Pregnancy
The myriad physiologic changes of pregnancy influence drug absorption, distribution, and elimination.{7} Changes in gastrointestinal function can alter oral drug absorption. Renal elimination generally increases because of an increase in glomerular filtration rate. Hepatic metabolism may be increased, unchanged, or decreased, and an increase in total body water may alter drug distribution and peak concentrations. Protein binding usually decreases; however, the free drug concentration may remain unchanged because of increased drug clearance.
Transfer Of Drugs Across the Placenta
The amount of drug that crosses the placenta depends on maternal cardiac output, fetal cardiac output, placental binding, and placental metabolism, as well as factors that influence passive diffusion across the placenta.{8} Maternal plasma levels of a drug depend on the site of administration (e.g., oral, intra-vascular, or epidural space), the total dose, the dosing interval, and other drugs that may
be co-administered (e.g., epinephrine). The amount of drug to which the fetus is exposed also depends on fetal metabolism (fetal blood carrying drugs away from the placenta passes first through the fetal liver), fetal protein binding (about half of maternal protein binding), and the
distribution of fetal cardiac output (fetal distress results in redistribution of blood flow to the vital organs).{9} In general, studies on human placental drug transfer and fetal exposure are limited. Inter-species differences in placental anatomy and function make comparisons with humans risky for animal models. However, ethical concerns have limited studies on pregnant women. Most studies of the Placental transfer of anesthetic agents administered to the mother intra partum reports single measurements of drug concentration in the maternal and umbilical vein serum at the time of delivery (the fetal-to-maternal or F/M ratio). The measured fetal concentration does not reflect the effects
of drug passage through the fetal liver, or the possibility of altered pharmacokinetics and pharmacodynamics in the fetus compared with the mother
Teratogenicity
Possible adverse effects on the fetus of in utero drug exposure include structural malformations, intrauterine fetal death, altered fetal growth, neuro behavioral teratogenicity, acute neonatal intoxication, or neonatal abstinence syndromes.2 is A major determinant of the effect of a drug on the fetus. However, functional and behavioral effects are also likely to
occur and are much harder to identify because the effects of fetal drug exposure may be delayed and only apparent later in life.2 The mechanisms by which drugs cause teratogenicity are poorly understood and may be direct or indirect (direct effect on the mother indirectly affects the fetus). There is inter-species variation in the ability of a drug to cause a specific congenital defect (e.g., thalidomide is not teratogenic in non-primates).
The period of classic teratogenesis corresponds with the critical period of organogenesis and begins approximately 31 days after the first day of the last menstrual period until about 71 days after the last period.{10}: Exposure to teratogens before 31 days results in an all-or-no effect (survival without a defect or loss of pregnancy). Fetal development, particularly that of the central nervous system, continues into the second and third trimesters, and indeed after birth. Therefore, fetal drug exposure at this time was not risk-free. Information on the teratogenic potential of many drugs has been obtained from large survey studies. These studies are often flawed because of reporting bias. They often do not control for other variables, including environmental exposures, exposure to multiple drugs (including alcohol, tobacco, nonprescription and illicit drugs), and the influence of the disease itself. Case reports of an association between in utero drug exposure and fetal anomalies are more likely to be published than if no anomaly occurred.{11}
Food And Drug Administration Risk Classification
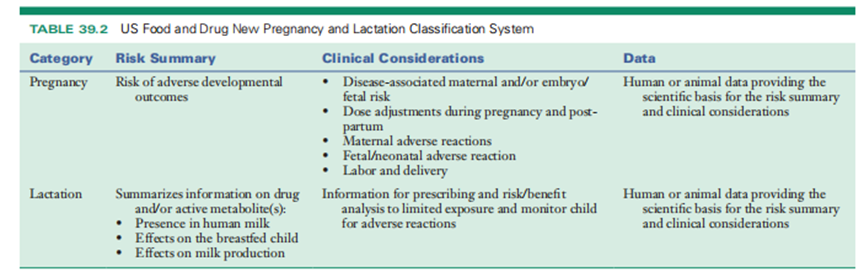
The US Food and Drug Administration (FDA) previously required labeling of drugs using the Pregnancy Category System (Table 39.1). The FDA has recognized that this system is often not helpful for prescribing physicians and pregnant patients. Starting in 2015, the FDA mandated a new drug labeling system (Pregnancy and Lactation Labeling Rule, or “Final The Rule”), which requires three new subsections in the pregnancy and lactation sections of the package insert risk summary, clinical considerations, and data sections (Table 39.2).{12}
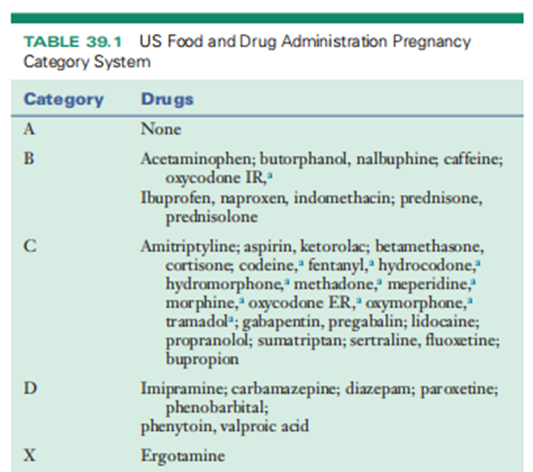
A Opioid agonists and agonist–antagonists are considered risk category D when used at high doses near term.
Specific Drugs
Aspirin use before birth concedes the possibility of an increased risk of gastroschisis, and significant girls seldom use anesthetics (>150 mg/day).13 Ibuprofen and naproxen all the while in the first trimester do not give the impression of being teratogenic.13 Prostaglandin inhibitors have happened to guide the shortening of the way a person writes arteriosus in utero. This effect increases with gestational age, even though it performs erratically when the drug is interrupted.2,13 Aspirin and other prostaglandin inhibitors concede the possibility of decreased amniotic fluid capacity subordinate to curtailed before-birth urine manufacturing, and they
concede the possibility of extended gestation and labor. A raised incidence of neonatal intracranial bleeding has happened in rash babies whose founders’ ingested anesthetics before beginning.
Therefore, entire-measure anesthetic and nonsteroidal anti-angiogenic drug (NSAID) analysis should be prevented in the triennial trimester.2,{13} If a mild painkiller is registered before birth, acetaminophen is the drug of choice. `14% of significant wives fill an opioid prescription all along their gestation. Chronic in-utero opioid discovery can bring about neonatal self-restraint disease. and maternal opioid use can be underrated in some way. {14} Neonatal frugality disease presents at 24–72 hours of life.14 Infants have changeable facial characteristics and performances, containing principal nervous system energetic irascibility (that is, overdone weeping, tremors, increased influence pitch); unrestrained politically central nervous system dysfunction (that is, nasal stuffiness, yawp, sweaty); and gastrointestinal disturbances. {14}
There is no evidence that opioid agonist or agonist-foe uncovering before birth is teratogenic.2 Opioid analgesics should be reserved for cases accompanying moderate to Bupivacaine and lidocaine have not reduced the risk of teratogenicity in the Collaborative Perinatal Project. 2, 9 The occurrence of before-birth anomalies raised diploid in daughters who were unprotected from mepivacaine; however, this group contained very few mothers, so it is troublesome to draw some conclusions from the dossier. Several studies have erected a partnership between two points: maternal steroid use and oro-facial clefts, while possible choices are destitute.2 A restricted trial of epidural steroid healing is seemingly associated with the slightest before-birth risk after the first Antidepressant drugs are commonly used to treat chronic pain. There is no evidence that tricyclic antidepressant drugs are teratogenic.2 First-trimester uncovering to most discriminating serotonin reuptake inhibitors (SSRIs) performs to have complementary rates of inborn malformations as the general state.{15,16} Paroxetine is the only SSRI that guides and raises the risk of bigger inborn heart oddities.15 There is a restricted dossier, but studies accompanying duloxetine imply it may increase rates of impulsive failure in the first trimester.16 Exposure to SSRIs in the tertiary trimester before childbirth grants permission to lead to neonatal retraction conditions (15) and temporary QT pause extensions (17). However, the long-term, dispassionate results of these changes are obscure. The noradrenergic and particular serotonergic antidepressants venlafaxine and the serotonin-noradrenaline reuptake inhibitors, in the way that Mirtazapine, appear to award no risk of deformity or neonatal removal disease, but these are more recent drugs with minute studies. Data on the teratogenicity of bupropion in significant girls are restricted but imply an increased risk of cardiac malformations. {18,19} very
Anticonvulsants are involved in before-birth development limits and congenital malformations. The Medical Birth Registry of Norway distinguished 2600 toddlers unprotected from antiepileptics, accompanying 771,412 unfound youngsters.20 Carbamazepine, lamotrigine, oxcarbazepine, gabapentin, and Pregabalin had low deformity rates, analogous to the approximate state {.20,21} Topiramate raised fetal progress
limit and microcephaly, and valproic acid raised the risk of hypospadias and septal essence defects.20 Children of mothers with muscle spasms who take anticonvulsants have a larger risk of enlightening delay and intelligence impairment than those who do not demand medicine before birth. Human studies display that phenytoin and valproic acid have the highest potential for neurodevelopmental disorders since lamotrigine and carbamazepine are the smallest inclined to bring about these antagonistic outcomes.{22}
Ergot amine is contraindicated in gestation, may be teratogenic, and further causes uterine shortenings {.23} There is no evidence that testing blockers are teratogenic; however, they concede the possibility of an intrauterine progress delay.{24},
Drugs During Laction
The amount of drug that a baby is exposed to along with the removal of liquid depends on various motherly and baby factors. Maternal determinants include motherly measures and drug break, elimination half-existence of the drug, baby sucking pattern (capacity and organization), and amount of drug that crosses into breast milk.2,3 The milk-to-skin (M:P) percentage is an index of the amount of drug discharged into the milk. Breast milk is somewhat more acidic than body tissue; thus, lifeless spread favors drugs that are feeble bases, lipid-soluble and have depressed protein binding.3 The amount of drug with which the baby is unprotected depends on baby pharmacokinetics, which may differ from motherly pharmacokinetics. The average baby quantity is mainly 1%–2% of the maternal measurement.3 Even when the M:P percentage approaches the individual, the baby skin concentration exceptionally accomplishes healing levels because the book of colostrum is small, and tending neonates are unprotected from the slightest amounts of the drugs administered to the parent in the postpartum period. 3 Most milk is made all along and promptly follows suckling. Administration of drugs quickly following in position or time nursing and preventing long-acting drugs grant permission help underrate baby uncovering. For the mother's attractive incessant drugs, the in-utero uncovering was more the exposure all the while removal of liquid. In general, hostile direct prescription concedes the possibility of being used, and earlier drugs accompanying an experience of extensive use concede the possibility of being chosen.3 It is best to use drugs that do not HAVE A LIVE METABOLITE.
American Academy of Pediatrics
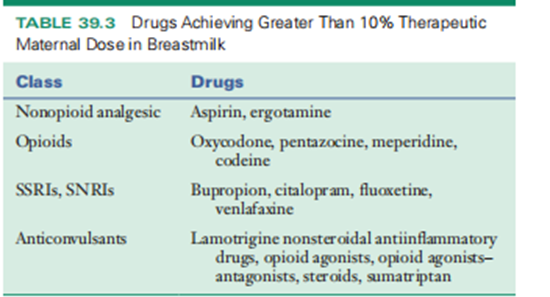
The American Academy of Pediatrics believes that the benefits of breastfeeding generally outweigh the risks of drug discovery in breast milk. The Committee on Drugs earlier filed drugs that may be secondhand cautiously during the removal of liquid and their belongings from babies and/or the removal of liquid. This jury immediately refers to practitioners in a more inclusive and current table at Lactmed (http://toxnet.nlm.nih.gov). A summary of analgesics that concede the possibility of being prevented by breastfeeding founders is presented in Table 39.3.
The following should be thought out when prescribing Drugs for lactating women Is a drug remedy inevitable?
The surest drug and lowest healing prescription should bepreferred, for instance, acetaminophen rather than anesthetic, for gentle dullness.
Preterm babies or neonates grant permission to be more sensitive to adverse occurrences by way of young tool function or healing conditions.
If skilled is a feasible risk to the baby, the individual concedes the possibility be considered listening to the baby's antitoxin levels of the drug.
Specific Drugs
Acetaminophen is expected to be the safest anodyne for fostering founders. The baby of a parent taking acetaminophen 4 g/day was unprotected to inferior 5% of the healing baby
receiving Dose {.25} The use of anesthetics by nursing inventors is dubious. Intermittent use does not pose a risk, but babies of founders receiving incessant anesthetic treatments should be aware of adverse reactions.{26} NSAIDs are thought-out and agreeable to accompanying feeding.13,{27}
Opioid agonists and antagonists can cross freely into breast milk. The American Academy of Pediatrics considers opioids agreeable to accompanying breastfeeding because most of the ruling class go through meaningful first-pass metabolism in babies. However, oxycodone, pentazocine, meperidine, and narcotics are not recommended for lactating founders, causing clinically therapeutic levels to be realized and producing unfavorable outcomes in breastfeeding babies.27 The babies of nursing founders ingesting opioids concede the possibility of being listened to for unfavorable belongings; less than 1% of the motherly measurement of prednisone or prednisolone is renewed in bosom milk.2 Even at extreme motherly doses, this is unlikely to be enough to restrain baby adrenal function. 11
SNRIs, Serotonin-norepinephrine reuptake inhibitors; SSRIs, selective serotonin reuptake inhibitors
Current guidelines suggest that the choice of a specific antidepressant or anticonvulsant is based on maternal clinical factors, particularly previous effective therapies. The
American Academy of Pediatrics warns that infant plasma concentrations that exceed 10% of therapeutic maternal plasma concentrations have been reported in several of
These drugs should be avoided by nursing mothers if possible (bupropion, fluoxetine, citalopram, venlafaxine, and lamotrigine).27 The anticonvulsants carbamazepine, phenytoin, and valproic acid may be used safely during lactation. Low and undetectable serum concentrations of many
antidepressants are detected in the serum of nursing infants, but long-term studies are lacking.28 Sertraline, duloxetine, and paroxetine are preferred in lactating women who require antidepressant drugs for the first time.15,16,{28}
Maternal administration of beta-blockers results in sub-therapeutic levels in nursing infants.26 Serum concentrations of propranolol in the nursing infant are less than 1% of the therapeutic dose 26 There is no data regarding the use of gabapentin or pregabalin during lactation {.29}
Ergot amine has been associated with neonatal convulsions and gastrointestinal disturbances and should not be used in nursing mothers.2,26 Sumatriptan is the most studied tryptophan during lactation.26 It is present in low concentrations in breast milk and has poor oral bioavailability, so the American Academy of Pediatrics considers sumatriptan compatible with breastfeeding. [26,27].
Imaging During Pregnancy
The two factors that determine the possible effects of radiation exposure on the developing fetus are gestational age and the fetal dose of absorbed radiation. Risks of fetal radiation
Exposures include abortion, genetic mutation, and carcinogenesis.{30} At doses of less than 50 mGy, the risk of abnormalities is thought to be negligible; the significant risk of malformation
is increased only at doses greater than 150 mGy.{31} Although radiation exposure from imaging studies generally falls below 50 mGy, exposure should be avoided if possible until after the
15th week of gestation, since radiation can be lethal to the fetus or cause severe defects with doses as low as 50 mGy. Although there is a theoretical risk associated with using magnetic resonance imaging (MRI), no detrimental effects on the fetus have been reported. been documented. MRI is indicated during pregnancy when other non-ionizing imaging methods (e.g., ultrasonography)
are unsatisfactory, and the information obtained would otherwise require exposure to ionizing radiation.30 Normal fluoroscopy can deliver 10–50 mGy/min of exposure time, so it should be avoided during pregnancy if possible.31
Pain Syndromes During Pregnancy and Lactation Pelvic Girdle Pain and Low Back Pain
Although definitions differ, the term pelvic girdle pain is used to describe pain in the regions of one or both sacroiliac (SI) joints and the gluteal region, sometimes involving the symphysis pubis, whereas pregnancy-related low back pain refers to pain in the lumbar region.{32–34} The incidence of these syndromes during pregnancy is about 45% and around 25% in the postpartum period.33 Risk factors include strenuous work, previous low back pain, or pain syndromes in a previous pregnancy.32 The etiology of pelvic girdle pain and low back pain (LBP) is likely related to mechanical, traumatic, hormonal, metabolic, or degenerative changes during pregnancy. The pain usually begins in the second trimester and resolves for most women within several weeks to months of delivery.32 About 10% of women continue to have chronic pain.33
Pelvic girdle pain is usually located between the posterior iliac crests near the SI joints. It may occur in conjunction with symphysis pubis pain and radiate into the posterior thighs.32,34 Few treatments have undergone rigorous scientific scrutiny. Patient education, pelvic belts,
Physiotherapy and acupuncture may be of benefit to some patients.32,{35} Pregnancy-related LBP is described as pain in the lumbar region, above the sacrum, and it may radiate into the leg. The pain is often dull and exacerbated by forward flexion.33 It is important to distinguish low-back pain from posterior pelvic joint pain using specific provocation tests to optimize physical therapy and exercise recommendations. [32,33]
If pharmacologic agents are required, acetaminophen and cyclobenzaprine are the drugs of choice for minor pelvic and back pain. The short-term use of NSAIDs may be appropriate during the first and second trimesters. Severe back pain may require opioid therapy.
Epidural Steroid injection(s) may be indicated for acute radicular pain, consistent with lumbar nerve root compression.
Neuropathic Pain: Carpal Tunnel Syndrome
The incidence of carpal tunnel syndrome ranges from 7% to 62% and is attributed to hormonal changes and tissue edema that occur during pregnancy.{36} Conservative management with nighttime splinting, physical therapy, or local injections with local anesthetic and steroid medications is effective in most cases. Surgery is reserved for severe cases of neurologic injuries. {37}
Headache
Migraine headaches are unusual during pregnancy.26 The initial presentation of a migraine-like headache in pregnancy should prompt a search for another serious cause.{38}
Key factors
Pain is common throughout pregnancy and lactation. Many girls are afflicted by pelvic girdle pain and back pain.
l Physiologic changes at some stage in pregnancy can also modify drug pharmacokinetics and pharmacodynamics.
l maximum drugs pass the placenta and cross into the breast milk.
l Drug consequences on the fetus may be direct or indirect (effect on the mom).
lEfforts must be made to minimize maternal exposure to tablets during pregnancy and lactation.
l viable destructive effects of in-utero drug exposure include structural malformations, intrauterine fetal dying, altered fetal growth, neuro behavioral teratogenicity, acute Neonatal intoxication, and neonatal abstinence syndromes.
lthe consequences of medicine on the fetus or nursing toddler rely on the gestational or post-conceptual age, the type/quantity of the drug, and the period of exposure.
lDrug pharmacokinetics and pharmacodynamics are altered inside the fetus and neonates compared with the older child and adult.
l information approximately fetal and neonatal effects of drugs administered to moms is regularly incomplete, however, new FDA labeling necessities can also be a useful resource in scientific
selection making.
l The selection to apply pills to deal with aches at some point during pregnancy and lactation ought to contain a hazard: gain analysis.
Research Method:
Study techniques: This observation has been designed to research the specific pain comfort techniques to be had for the duration of pregnancy and lactation and their protection. At some stage in this period, a complete literature evaluation was performed to collect applicable studies and information on normally used ache manipulation alternatives. The literature seeks protected clinical databases and authoritative assets until the stop of information collection in September 2021. Each animal and human study has been included in the evaluation.
Results:
This takes a look at several pain management techniques that are typically considered easy and effective sooner or later, including pregnancy and lactation. The strategies covered non-pharmacological interventions together with bodily remedies, acupuncture, and rubdowns. In addition, certain over-the-counter analgesics, collectively with acetaminophen (paracetamol), had been determined to have a particularly favorable safety profile when used at endorsed doses.
Discussion:
Being pregnant and lactating poses precise and worrying conditions for pain management due to the potential risks that a few medicinal drugs can also pose to the developing fetus or breastfeeding child. As a result, healthcare providers frequently search for alternative pain relief options that prioritize safety for every mom and her toddler. The research supports the usage of non-pharmacological interventions as a first-line method, as they commonly have minimal to no bad outcomes and may be useful for handling pregnancy-related pain. Concerning pharmacological options, acetaminophen stands proud as a reasonably secure choice when used judiciously. But exclusive normally used pain medicines, which include nonsteroidal 07b031025f5f96dfa8443f843db463b6 capsules (NSAIDs) and opioids, should be used with caution sooner or later all through pregnancy and lactation due to the potential risks to the little one. It's crucial to emphasize that individual instances might also vary, and every pregnant or breastfeeding female has to visit her healthcare provider to determine the most appropriate pain management plan primarily based on her unique health situation and wishes.
Conclusion:
The examination underscores the significance of safe and effective pain management at some point in pregnancy and lactation. Non-pharmacological tactics like bodily therapy, acupuncture, and rubdowns have to be prioritized on every occasion feasible due to their generally favorable safety profiles. For times when pharmacological intervention is important, acetaminophen can be taken into consideration as a cozy preference when used in line with recommended guidelines. However, the use of special pain medicines must be approached with caution, and selections need to be made in consultation with healthcare specialists to ensure the well-being of both the mom and her baby. In addition, studies and clinical trials are warranted to enlarge our knowledge of pain control alternatives at some stage in pregnancy and lactation and to provide extra proof-based tips for healthcare providers.
Acknowledgment
The completion of this research project would not have been possible without the
contributions and support of many individuals and organizations. We are deeply
grateful to all those who played a role in the success of this project
We would also like to thank My Mentor [. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project
Declaration of Interest
I at this moment declare that:I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript
References
- Shah S, Banh ET, Koury K, et al. (2015). ache control in being significant: multimodal processes. Pain Res Treat: 987483.
View at Publisher | View at Google Scholar - Briggs G, Freeman R, (2015). Drugs in Being Meaningful and Lactation: A Reference to Fetal and Neonatal Hazards, Ed. 10. Philadelphia: Wolters Kluwer/Lippincott, Williams & Wilkins Health
View at Publisher | View at Google Scholar - Newton ER, Hale TW, (2015). drugs in feelings milk Clin Obstet Gynecol 58:868–884,
View at Publisher | View at Google Scholar - Anderson GD,(2006). the use of pharmacokinetics to envision the results of gestation andmotherly-baby transfer of drugs at a few points in the removal of liquid professional Opin Drug MetabToxicol 2:947–960,
View at Publisher | View at Google Scholar - uideBateman BT, Hernandez-Diaz S, Rathmell JP, et al. (2014). patterns of opioid exercise in gestation in an abundant disciple of mechanical security benefits in the US. Anesthesiology a hundred and 20: 1216–1224,
View at Publisher | View at Google Scholar - Ayad M, Costantine MM, (2015). Epidemiology of cure use in gestation Semin Perinatol 39:508–511.
View at Publisher | View at Google Scholar - Feghali M, Venkataramanan R, and Caritis S (2015). Pharmacokinetics of cure in being significant, Semin Perinatol 39:512–519,
View at Publisher | View at Google Scholar - Syme MR, Paxton JW, and Keelan JA (2004). Drug transfer and absorption by way of the human amniotic sac, Clin Pharmacokinet 43:487–514,
View at Publisher | View at Google Scholar - Bucklin B., Santos A. (2014). nearby sleep-inducers and opioids In Chestnut D, Polley LS, Tsen LC, and Wong C, editors: Chestnut’s Obstetric Anesthesia flags and exercise, ed. 5, Philadelphia, Elsevier Saunders.
View at Publisher | View at Google Scholar - Lancaster, PA (2011). causes of origin defects: communication from records Congenit Anom (Kyoto) 51:2–5,
View at Publisher | View at Google Scholar - Rayburn WF (1998). Connective fabric issues and gestation tips for prescribing. J Reprod Med quadragenarian-three:341-349,
View at Publisher | View at Google Scholar - (2014). outline of Sections 8.1–8.3 on Drug Labeling the United States of America: Food and Drug Management, America's Branch of Fitness and Human Offerings.
View at Publisher | View at Google Scholar - Bloor M., Paech M (2013). Nonsteroidal antagonistic-angering drugs at a few points of gestation and the start of liquid removal. Anesth Analg 116:1063–1075,
View at Publisher | View at Google Scholar - Stover MW, Davis JM (2015). Opioids in being meaningful and Neonatal Abstinence Syndrome, Semin Perinatol 39:561–565,
View at Publisher | View at Google Scholar - Sie SD, Wennink JM, truck Driel JJ, et al. (2012). Maternal use of SSRIs, SNRIs, and NaSSAs: proficient tips at few stages in being significant and removal of liquid Arch Dis baby Fetal Neonatal Ed. 97: F472–F476,
View at Publisher | View at Google Scholar - Andrade C (2014). Safety of duloxetine before birth and removal of liquid Jay Clean Psychiatry 75: e1423–e1427.
View at Publisher | View at Google Scholar - Dubnov-Raz G., Yurlink D.N., Fogelman R., et al. (2008). Optional fetal use Serotonin reuptake inhibitors and QTc extension in neonates Pediatrics 122: e710–715,
View at Publisher | View at Google Scholar - Cole JA, Modell JG, Haight BR, et al. (2007). incident of bupropion and inborn malformations ingestation Model JG, Haight BR, and others: Prevalence of bupropion and Pharmaco epidemic drugs, Saf16:474–484;
View at Publisher | View at Google Scholar - Louick S., Kerr S., and Mitchell A.A. (2014). Early gestation bupropion uncovering and risks soul defects. Pharmacoepidemiol Drug Saf 23:1066–1075,
View at Publisher | View at Google Scholar - Weibi G., Daltveit A.K., Engelsen B.A., et al. (2014). before birth progress delay and transmittal Defects of new and traditional antiepileptic drugs before birth. Jay Nerol 261:579–588.
View at Publisher | View at Google Scholar - Guttuso Jr. T., Shaman M., Thornburg LL. (2014). Possible motherly syndromes Overview of the benefits and security of gabapentin before birth European Journal of Obstetrics and Gynecology Regeneration Biol 181:280–283.
View at Publisher | View at Google Scholar - Verrotti A, Scaparrotta A, and Cofini M (Developmental neurotoxicity to a degree; Anticonvulsants: visualize in some way. Reprod Toxicol 48:72–80,
View at Publisher | View at Google Scholar - Banhidy F, Acs N, Puho E, et al. (2007). Ergot a situation before birth Low beginning pressure and extreme preterm beginning rates. Br J Pure Pharmacol 64:510–516.
View at Publisher | View at Google Scholar - Ruys TP, Maggioni A, Johnson MR, et al. (2014). Cardiac drugs before birth, ROPAC dossier, Int J Cardiol 177:124–128.
View at Publisher | View at Google Scholar - Xie RH, Guo Y, Krewski D, et al. (2014). Beta-blockers increase the risk of bearing a baby. limited for gestational age or standardized in babyhood. Movie Arena 121:1090–1096.
View at Publisher | View at Google Scholar - Davanzo R, Bua J, Paloni G, et al. Breastfeeding and Migraine Medications Your Clin Pharmacol 70:1313–1324;
View at Publisher | View at Google Scholar - Sachs HC (2013). Drug Commission: Transfer of Medicines and Therapeutic Breastfeeding: An Update on a Selected Topic Pediatrics 132: e796–e809.
View at Publisher | View at Google Scholar - Lanza di Scalea T; Wisner KL (2009). Antidepressant use all along breastfeeding, Clin Obstet Gynecol 52:483–497.
View at Publisher | View at Google Scholar - Van der Meer DH, Wieringa A, Wegner I, et al. (2015). Anticonvulsant tests concurrently with an activity removal of liquid: an acceptable review Br J Clin Pharmacol79:558–565.
View at Publisher | View at Google Scholar - Patel SJ, Reede DL, Katz DS, et al. (2007). Maternal Imaging in Non-Obstetric positions: Algorithms and Dose concerns 27:1705-1722.
View at Publisher | View at Google Scholar - Mahesh M (2001). Fluoroscopy: patient someone questions in radiography, 21:1033–1045.
View at Publisher | View at Google Scholar - Vermani E, Mittal R, et al. (2010). Pelvic and lower back ache inside the way of being meaningful: a review of ache Pract 10:60-71
View at Publisher | View at Google Scholar - Casagrande D., Gugala Z., and Clarke S.M. et al. (2015). backache and loin pain in the intervening time of being significant J Am Acad Orthop Surg 23:539–541.
View at Publisher | View at Google Scholar - burning Albert Hb Coastguard HChc, et al. (2008). European hints judgment and treatment of pelvic pain and erect spine J. 17:794-819.
View at Publisher | View at Google Scholar - Snig DB, Bendo JA (2007). repeated, pain had a connection with being meaningful Orthopedics 30: 46–47 839–845,
View at Publisher | View at Google Scholar - Padua L, di Pasquale, Pizzaiola C, et al. (2010). A orderly judgment of gestation-connected repetitive stress injury, 42:697–702.
View at Publisher | View at Google Scholar - Klein A. (2013). Peripheral nerve issues at few points before birth, Clin Obstet Gynecol 56:382–388.
View at Publisher | View at Google Scholar - Spierings EL, Sabin TD (2016). New confusions in gestation and postpartum, Neurologist 21:1–7.
View at Publisher | View at Google Scholar
