

Research Article | DOI: https://doi.org/10.31579/2834-796X/072
Overview of Endovascular Treatment of Infra Renal Abdominal Aortic Aneurysms Over the Last 21 Years in Brazil
- Sara Garcia Menezes
- João Victor Fragoso Dorea Silva
- Isabela Pereira de Farias
- Gustavo Novaes Lima
- David Bastos Oliveira Diniz Carvalho
- Wagner Ramos Borges *
3rd year Medical Student, Bahiana School of Medicine and Public Health, Bahia; Applied Regional Anatomy Academic Monitoring, Brazil
4rd year Medical Student, Bahiana School of Medicine and Public Health, Bahia; Applied Regional Anatomy Academic Monitoring, Brazil
Doctor Adjunct Professor of Escola Bahiana de Medicina e Saúde Pública, Salvador, Bahia; PhD in Medicine and Health - Faculdade de Medicina da Bahia/Universidade Federal da Bahia; Vascular Surgeon, full member of Sociedade Brasileira de Angiologia e de Cirurgia Vascular and Colégio Brasileiro de Cirurgiões, Brazil.
*Corresponding Author: Wagner Ramos Borges, Universidade Federal da Bahia; Vascular Surgeon, full member of Sociedade Brasileira de Angiologia e de Cirurgia Vascular and Colégio Brasileiro de Cirurgiões, Brazil.
Citation: Sara G. Menezes, Dorea Silva JVF, Isabela Pereira de Farias, Gustavo N. Lima, Diniz Carvalho DBO, et al, (2024), Overview of Endovascular Treatment of Infra Renal Abdominal Aortic Aneurysms Over the Last 21 Years in Brazil, International Journal of Cardiovascular Medicine, 3(4); DOI:10.31579/2834-796X/072
Copyright: © 2024, Wagner Ramos Borges. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 July 2024 | Accepted: 19 July 2024 | Published: 05 August 2024
Keywords: aorta, aneuryms, evar
Abstract
Introduction: Endovascular treatment of abdominal aortic aneurysms (EVAR) has emerged as an innovative therapeutic alternative with significant growth potential. Despite its advantages, factors such as costs, short- and long-term benefits and patient characteristics are still being analyzed and make it difficult to increase the number of these procedures when compared to the traditional open technique.
Objectives: To describe the statistical behavior of endovascular treatment for AAA repair over the last 21 years in Brazil.
Materials and Methods: Retrospective and descriptive study of data available in the DataSUS database, where variables relating to the number of hospitalizations, number of deaths, average length of stay and hospital and professional costs were analyzed.
Results: Among the 1,618 hospitalizations for endovascular treatment of abdominal aortic aneurysms in Brazil between 2002 and 2023, 680 occurred in the South region, followed by the Southeast region with 674 hospitalizations. The mortality rate was 7.94% in this period and the number of deaths was 130. The highest number of deaths was recorded in the Southeast, while the highest mortality rates were in the North and Midwest, 66.67 and 47, respectively.
Discussion: The results showed regional inequalities and the influence of socio-economic indices on access to healthcare in Brazil, so that the more economically developed regions showed better results in terms of hospitalizations and mortality.
Conclusion: Although the study has limitations, it showed a growing trend in the use of EVAR in Brazil, with the South and Southeast regions having better results in terms of hospitalizations and mortality, while the North and Midwest regions had lower hospitalization rates and higher mortality rates, pointing to underreporting and limited access to advanced treatments.
Introduction
The infrarenal abdominal aortic aneurysm (AAA) is a growing pathology in Brazil due to the aging of the population1 and is, in most cases, asymptomatic until it ruptures, leading to unexpected death in around 65% of patients2. This disease can be treated by clinical management and by surgery, which is essentially characterized by two techniques: open and endovascular. Open surgery, characterized by a long hospital stay, may require blood transfusions, and perioperative mortality is considerable (4.7%). Until the 1990s, it was the only form of treatment available3. Endovascular treatment for abdominal aortic aneurysm repair has emerged as an innovative therapeutic alternative with significant growth potential.
Endovascular treatment for infrarenal abdominal aortic aneurysm (EVAR) is a minimally invasive approach. It involves an endoprosthesis that is expanded, providing structural support to the aortic wall and excluding the aneurysm from blood circulation12.
This method generally results in faster recovery, less post-operative pain and shorter hospital stays compared to traditional open surgery. As of 2017, EVAR was prioritized in the Brazilian Guideline for the Treatment of Abdominal Aortic Aneurysm due to lower rates of rupture, length of hospital stays, complications and short-term perioperative mortality, but there are still concerns about ruptures and doubts about the long-term benefit4. However, despite the fact that endovascular treatment rates have increased over the last three decades, the open technique is still used in Brazil. Nevertheless, endovascular treatment has high rates of reintervention5,6 and medium and long-term mortality7.
From an international perspective, the perioperative mortality rate is 1.6%, with rates in randomized studies such as EVAR I, DREAM and OVER ranging from 0.5% to 1.6%9. However, a meta-analysis showed a loss of survival advantage after 2 years of follow-up10. One of the studies analyzed, which followed patients undergoing both techniques for 15 years, found that the survival rate was higher in the group that underwent open surgery, while the long-term mortality rate with EVAR was 5 times higher9. In the Brazilian context, a study carried out in 2009 showed an annual mortality rate of 7.8% in patients undergoing endovascular treatment3.
Factors such as length of stay and financial costs related to the endovascular technique are considered relevant to understanding the use of the technique in Brazil. Studies have shown that EVAR is characterized by an average hospital stay of 5 days, less blood loss and need for mechanical ventilation and fewer post-operative complications13,14,15, associated with an average cost of $ 9,000, which is 436% more expensive than the open method. Endoprostheses and adjuvant materials were identified as the main factor responsible for the increase in costs11. In addition, the need for reintervention can cause a substantial increase in financial expenses10.
It is also important to highlight the epidemiological profile of AAA in Brazil, which is facing an increase in cases due to population aging.16 A Brazilian study identified 65% of cases in men17, with a higher mortality rate between the ages of 65 and 80 and 2 to 3 times more cases in white men than in Hispanic, Asian and black men18.
On the other hand, despite the higher incidence of AAA in men, the risk of rupture is 4 times higher in women19 with mortality predominantly above the age of 8020 and incidence mainly after the menopause due to the drop in endogenous estrogen, a hormone that some studies suggest influences protection against abdominal aortic aneurysms21, which corroborates the higher prevalence in men.
To date, there is still controversy about the indication of EVAR due to the risks, given the lack of level A evidence and its indication being based essentially on non- inferiority in relation to open surgery8.
This study describes the panorama of AAA in Brazil, taking into account data from the DataSUS system, exploring its use over the years, regional distribution, mortality rates and public spending on the procedure.
Materials and Methods
This is an observational, retrospective and descriptive study of secondary data extracted from the Hospital Information System of the Unified Health System (SIH/SUS), available in the Data SUS database, referring to hospitalized patients diagnosed with AAA in Brazil, from the years 2002 to 2023, by place of residence. Due to platform limitations, the data for the years 2002 to 2007 were computed by year of processing, while those for the years 2008 to 2023 were computed by year of care.
Data was collected on hospital admissions during the period in question, taking into account the following variables: number of admissions; hospitalization coefficients; mortality rate; number of deaths; total days of hospitalization; average number of days of hospital stay per hospitalization and amounts spent associated with EVAR. These variables were analyzed according to their distribution among the Brazilian demographic regions (North, Northeast, Midwest, Southeast and South) and their temporal dispositions, between 2002 and 2023.
The data obtained was then processed using Microsoft Excel software to create tables and graphs. This information can be checked via the TabNet portal, at the following access link: https://datasus.saude.gov.br/.
To calculate the hospitalization coefficient, the number of hospitalizations was divided by the resident population in the respective year and region and multiplied by 100,000. The data on the resident population was taken from the demographic and socio- economic indicators in the "Study of Population Estimates by Municipality, Sex and Age-2000-2021", available on the Data Sus database.
In order to analyze the amounts spent on the EVAR procedure, as well as its distribution among hospital services and professionals, all the data was converted into dollars, which were quoted on 26/03/2024 (R$4.99). The source used was the Central Bank of Brazil. This information can be found at the following link: https://www.bcb.gov.br/.
As it is a public data source, authorization from the Ethics Committee was not required.
Results
Between 2002 and 2023, there were 1,618 hospitalizations recorded for EVAR. During the 21 years, an upward trend in the number of hospitalizations was observed. The mortality rate related to this treatment in Brazil was 7.94% and there was an oscillating pattern during this period. (Table 1)
It was observed that the South had the highest number of hospitalizations, totaling 680 (41.92%), followed by the Southeast and Northeast, 41.55% and 10.11%, respectively. At the same time, when calculating the hospitalization coefficient per 100,000 inhabitants, between 2002 and 2021, the South region also leads significantly among the other regions with a total of 0.115, so that it has a value that represents more than 3 times that associated with the Southeast region (second highest hospitalization coefficient) and more than 6 times that of the Midwest region (third highest hospitalization coefficient). (Table 1)
In the years between 2002 and 2023, 130 EVAR-related deaths were recorded. Approximately half of this number is concentrated in the Southeast (48.46%). This is followed by the South with a record of 49 deaths (37.69%), the Northeast with 10 (7.6%), the Midwest with 6 (4.6%) and the North with 2 (1.5%) (Table 1).
It was noted that the highest mortality rate was in the North (66.67). However, there was only one year in which both death (2 deaths in 2017) and mortality data were recorded in the region. The Central-West region, in second place as the region with the highest mortality rate for the procedure (47.00), like the North, had an underreporting of deaths (only 5 of the 21 years analyzed). The mortality rates for the other regions did not exceed 15.16. (Table 1)
The average length of stay was 8.49 days, with a downward trend over this period, with the highest average length of stay in the North with 20.06 days, followed by the Midwest with 11.88 days (Table 1).
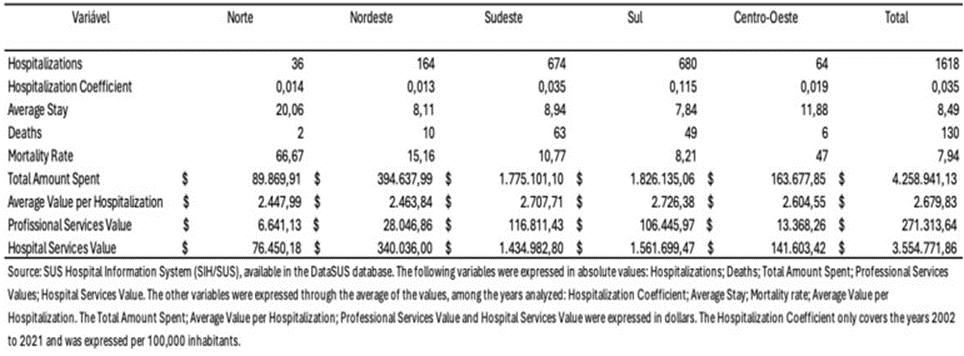
Table 1. Regional distribution of the statistical behavior of hospitalization for endovascular repair of abdominal aortic aneurysms between 2002 and 2023, in Brazil
The total cost from 2002 to 2023 was U$4,258,901.13, with the South region responsible for 42.8% of this amount, followed by the Southeast with 41.6%.
There was a clear upward trend in the total amount spent over time, with a significant increase between the years 2021 and 2022 (78.5% increase) (Table 1); (Graph 1)
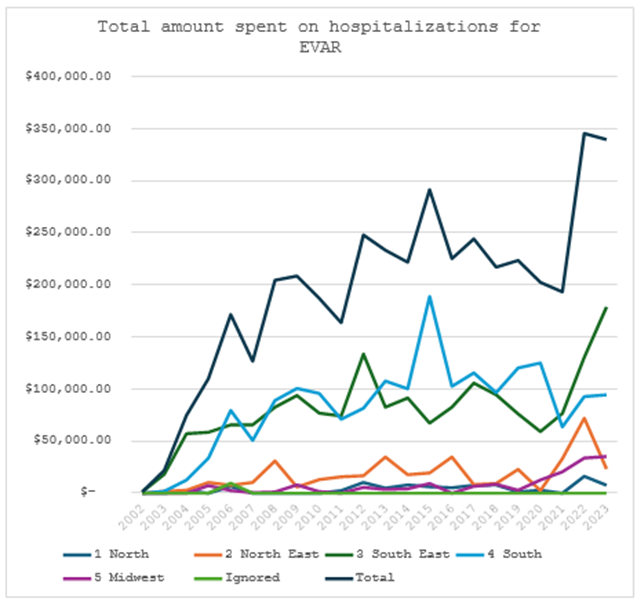
Graphic 1
The average cost per hospitalization in the five Brazilian regions from 2002 to 2023 was U$2,679.83, with little variation between 2004 and 2021, with the biggest increases in 2004 and 2022, 42% and 26% respectively. In a comparative analysis, the Center-West and North regions differed most from the other regions (Table 1); (Graph 2). Taking into account the time frame of the average costs per hospitalization, the overall picture shows an increase in the average cost per hospitalization when comparing 2007 and 2023 of U$ 1,014.56 (42.5%), with a significant difference between the North region and the other regions, which showed an increase of 13%, unlike the other regions, which showed an increase of between 39-54% (Table 1); (Graph 2).
Furthermore, there was a low average cost in the Center-West region in 2007, 2008 and 2010, with a drop of around 80% compared to the previous year, in a disproportionate scenario compared to the other regions (Graph 2).
It can be said that, as with the analysis of the number of deaths and the mortality rate, the North was the region with the most underreported data (a total of 5 years without any record of the average cost per hospitalization). (Graph 2)
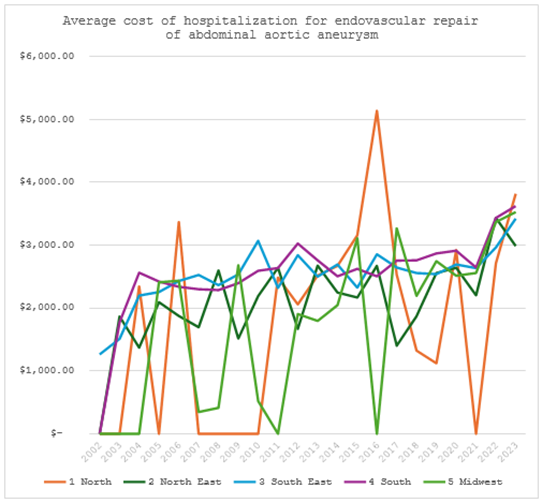
Graphic 2
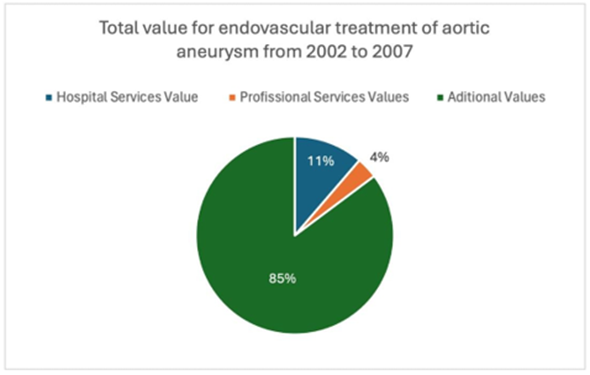
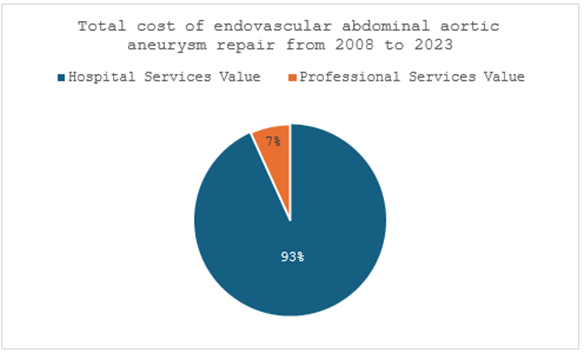
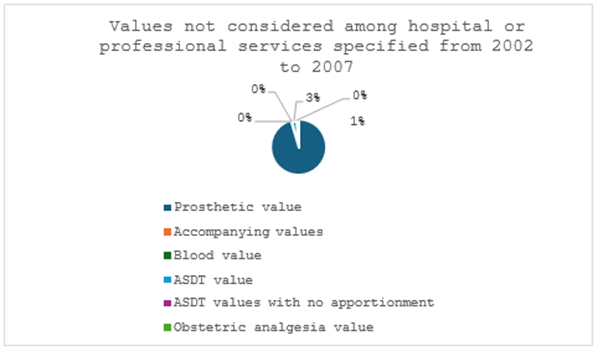
The distribution of the costs involved in EVAR from 2002 to 2007 and from 2008 to 2023 between hospital services, professionals and other additional materials/services was evaluated. There was a discrepant distribution between these services between the periods, so that between 2002 and 2007 the additional values were responsible for 85% of the costs, followed by hospital services with 11% of the costs. Among the additional costs, 92% were related to the value of prostheses, totaling 78% of the total costs between 2002 and 2007. Between 2008 and 2023, the additional costs were not broken down in DATASUS and hospital services accounted for 93% of the total (Graphs 3 and 4).
Graphic 3
Graphic 4
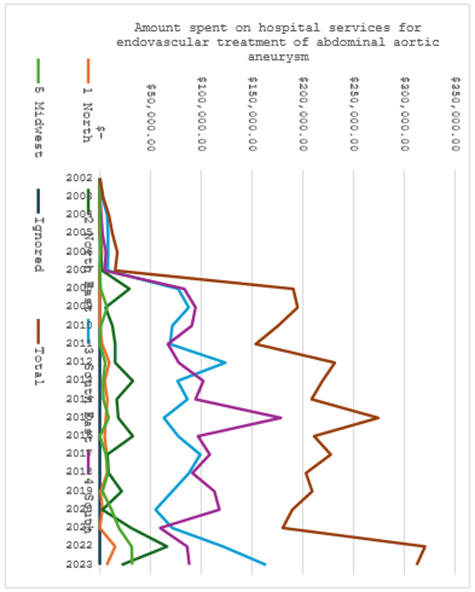
The distribution of spending on hospital services analyzed by region follows a similar trend to that of total costs. In addition, the graph showed a similarity to that of total costs with the sharp increase in 2022 of 77.7% compared to 2021. (Graph 5). In addition, a significant increase of 1,167% in the costs of hospital services was noticeable between 2007 and 2008, the year in which the additional values were no longer specified in the database used, as well as a slight oscillation in hospital costs until 2021, when they increased by 77.8% in 2022. (Graph 5)
Graphic 5
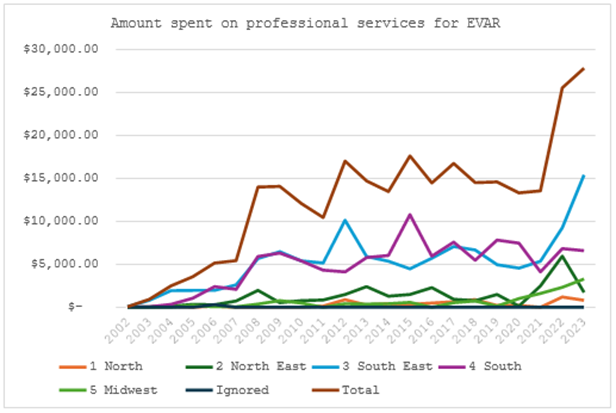
As for professional services, they accounted for 3% of total costs between 2002 and 2007 and 7?tween 2008 and 2023 (Graphs 3 and 4). The upward trend in professional services costs converges with the graph of total costs and hospital services. This shows a considerable increase of 56.8% in 2008 compared to 2007, and another sharp increase of 88.6% in 2022 compared to 2021. (Graph 6)
Graphic 6
Between 2002 and 2007, the total value is divided by DataSus into 8 variables: hospital services value, professional services value, prosthesis/orthotics value, companion value, blood value, SADT value, SADT value without apportionment and obstetric analgesia value, which in Graph 3 have been condensed as additional values. Thus, from 2002 to 2007, the values for these variables added up to a total of $431,987.64, corresponding to 85% of the total cost of EVAR hospitalizations (Graph 3).
It is notable that prostheses accounted for $412,903.92, 96% of the additional costs from 2002 to 2007, followed by SADT costs with $10,573.66 (2%). From 2008 onwards, these variables ceased to exist and the costs were divided up into hospital and professional services only (Graph 7).
Graphic 7
Discussion
The data obtained on EVAR in Brazil between 2002 and 2023 reveals important trends and regional patterns that deserve in-depth analysis. The growing trend in the number of hospitalizations suggests an increase in the adoption of the EVAR technique, as it is less invasive compared to traditional open surgery. The literature supports this observation, highlighting that EVAR has become a preferred choice due to its lower complication rate and shorter recovery time, but the risk of rupture remains a postoperative concern and the long-term survival rate is an advantage only among young patients3,4,22.
The data varied during the years of the Covid-19 pandemic, with a decrease in hospitalizations in 2020 and maintenance in 2021, followed by an increase in hospitalizations in 2022 and maintenance in 2023. These results reflect a possible influence of the Covid-19 pandemic, which peaked in 2020 and 2021, a period marked by an overload of the Unified Health System (SUS), and consequent impairment of screening tests, underdiagnosis and a decrease in abdominal aortic aneurysm treatments. The increase in hospitalizations for the procedure in 2022, the year in which the country's health situation returns to normal, reinforces the relationship between the fall in the number of hospitalizations for aortic aneurysm repair and the Covid-19 pandemic.
According to the literature, there is a downward trend in the number of deaths caused by AAA in Brazil, due to reduced exposure to risk factors, greater use of cardioprotective and antihypertensive drugs, greater availability of diagnostic imaging and greater availability of innovative and minimally invasive endovascular treatment.23 However, when taking into account the number of deaths resulting from the pathology correction procedure, an oscillating and growing pattern was noted in the years analyzed, given the significant increase in hospitalizations for endovascular treatment of AAA in the period. Around half of this number is concentrated in the Southeast (48.46%), which can be explained by the significant proportion of Brazilians who live in this region, and in the South (37.69), which is justified by the greater number of patients who have undergone this procedure, due to economic and social advances in this region, thus facilitating the diagnosis, treatment and notification of AAA.
The mortality rate observed in Brazil was 7.94%, which is in line with international studies, which report mortality rates varying between 1% and 10%, depending on the complexity of the cases and the experience of the medical centers24. Although the South, Southeast and Northeast had the highest number of hospitalizations, it was the other regions, the North and Midwest, which led this variable, with a mortality rate of 66.67 and 47.00, respectively. This rate is very divergent in Brazil as a whole. However, it is worth noting that both have significant underreporting, which hinders a more precise and detailed analysis of these regions. Furthermore, the oscillation in the mortality rate of EVAR in Brazil over the period studied may reflect variations in the quality of health care, technological advances and accumulated clinical experience.
The average length of stay in this study differed from that found in the literature, since the average for EVAR is 5 days3,15, 69.8% less time than that found in the country's records. In addition, this percentage becomes much higher and closer to the average length of stay for the open technique15 when evaluating the North and Central-West regions, which have the highest average lengths of stay, possibly due to the worsening of cases because of the difficulty in accessing health care and the compromise of post- operative rest with the return home due to the territorial extension.
Regional analysis reveals a significant disparity in the distribution of hospitalizations. The southern region of Brazil, with 680 hospitalizations (41.92%), stands out significantly. This finding is corroborated by the hospitalization coefficient, which is substantially higher in the South (0.115 per 100,000 inhabitants) compared to other regions. This predominance can be attributed to various factors, including a greater concentration of centers specializing in EVAR and greater availability of medical resources.25
The Southeast, although close in terms of the absolute number of hospitalizations, has a significantly lower hospitalization coefficient. This may indicate a larger population with better access to preventive care, resulting in a lower proportional need for emergency interventions. The Northeast region, on the other hand, has a much lower hospitalization coefficient, suggesting possible barriers to accessing advanced treatment, such as inadequate medical infrastructure and socioeconomic inequalities26.
These regional disparities are consistent with the literature on health inequalities in Brazil, where more economically developed regions tend to have better access to advanced medical treatment27. The higher concentration of hospitalizations and the higher hospitalization coefficient in the South region may also reflect more effective regional health policies in the detection and treatment of abdominal aortic aneurysms.
In terms of total costs, the South region's lead reflects the higher number of hospitalizations for EVAR. In the national scenario, the overall increase of 78.5% in 2022 compared to the previous year can be explained by the increase in the number of cases and the average cost per hospitalization compared to the previous year. Although the average cost has fallen occasionally, overall, there have been no significant differences over the years analyzed, unlike the distribution of the costs involved in EVAR.
Regarding additional costs, between 2002 and 2007, the values of materials and/or exams, as well as the costs of hospital services and professionals are detailed in DataSUS. Additional costs relating to materials and/or exams accounted for 85% of the total, with 78% corresponding to the value of prostheses, data that corroborates what has been reported in the literature, since they accounted for most of the cost of EVAR and are the main factor responsible for the high cost of endovascular treatment when compared to the open technique11.
On the other hand, in 2008, there was an increase of 1,167% in the cost of hospital services and 156% in the cost of professional services, maintaining the average absolute values until 2023. This information, when coupled with the fact that since 2008 data on the cost of materials and/or exams - including the value of prostheses - has not been described in DataSUS, suggests a change in the criteria for distributing and categorizing costs, including the cost of prostheses and other materials and/or services as hospital and/or professional.
The data indicates a growing trend in the use of the EVAR technique in Brazil, reflecting greater adoption due to its benefits, such as less invasiveness and shorter recovery time. Analysis over the years shows an interruption in the trend during the Covid-19 pandemic, with a subsequent recovery in hospitalizations as the Brazilian public health situation normalized.
Mortality associated with EVAR in Brazil is in line with international standards, despite regional variations. This suggests that the technique is effective, but there are still caveats about cost-effectiveness, patient profiles in terms of age, risk factors and anatomical variations, as well as facing challenges in terms of access and equity in healthcare.
The regional disparities revealed by the data highlight the need for health policies that address these inequalities. Regions like the South and Southeast, which have greater access to medical resources and specialized centers, show better results in terms of hospitalizations and mortality. On the other hand, regions like the North and Midwest, with lower hospitalization rates and higher mortality rates, point to underreporting and limited access to advanced treatments.
Future studies should focus on investigating the specific factors that contribute to these disparities and evaluate interventions that can guarantee more equitable access to highly complex treatments throughout Brazil.
This study has limitations, as it relies on secondary data from the SUS Hospital Information System (SIH/SUS), which can result in underreporting or inconsistencies in the records, especially in regions with less health infrastructure, such as the North and Midwest, as well as the absence of data, which limited the analysis to the last 21 years in Brazil and prevented the comparative study of age group, gender and color/race. In addition, the data on EVAR was not distinguished from endovascular treatment for abdominal aortic dissection as well as aneurysm or dissection of the iliac arteries, particularly the common iliac arteries, which can be treated in the same way as an AAA. In the period from 2004 to 2023, the type of prosthesis used was not specified for the data from 2004 to 2007, nor was there a distinction between AAA or iliac artery aneurysm/dissection for the data from 2002 and 2003. In addition, the registry is restricted to public services provided through the SUS or those affiliated with it, without considering private services that are not affiliated, and the analysis does not take into account external factors that may influence hospital costs, such as changes in health policies and economic variations. Although it is possible to outline the panorama shown in the study, these limitations must be taken into account.
References
- Bengtsson H, Sonesson B, Bergqvist D. Incidence and prevalence of abdominal aortic aneurysms, estimated by necropsy studies and population screening by ultrasound. Ann N Y Acad Sci 1996; 800: 1-24.
View at Publisher | View at Google Scholar - Kniemeyer HW, Kessler T, Reber PU, Ris HB, Hakki H, Widmer MK. Treatment of ruptured abdominal aortic aneurysm, a permanent challenge or a waste of resources? Prediction of outcome using a multi-organ- dysfunction score. Eur J Vasc Endovasc Surg 2000; 19: 190-96.
View at Publisher | View at Google Scholar - Novero ER, Metzger PB, Angelieri FMR, Colli MB de O, Moreira SM, Izukawa NM, et al. Endovascular repair of abdominal aortic aneurysm: analysis of single-center outcomes. Radiol Bras. 2012 Feb;45(1):1-6.
View at Publisher | View at Google Scholar - Li B, Khan S, Salata K, Hussain MA, de Mestral C, Greco E, et al. A systematic review and meta-analysis of the long-term outcomes of endovascular versus open repair of abdominal aortic aneurysm. J Vasc Surg. 2019 Sep;70(3):954-969.e30.
View at Publisher | View at Google Scholar - Cao, P., Verzini, F., Parlani, G., Romano, L., De Rango, P., Pagliuca, V., & Iacono, G. (2004). Clinical effect of abdominal aortic aneurysm endografting: 7-Year concurrent comparison with open repair. Journal of Vascular Surgery,40(5),841-848.
View at Publisher | View at Google Scholar - Carpenter, J. P., Baum, R. A., Barker, C. F., Golden, M. A., Velazquez, O. C., Mitchell, M. E., & Fairman, R. M. (2002). Durability of benefits of endovascular versus conventional abdominal aortic aneurysm repair. Journal of Vascular Surgery, 35(2), 222-228.
View at Publisher | View at Google Scholar - Brito CJ de, Murilo R, Loureiro E. Cirurgia Vascular: Cirurgia Endovascular- Angiologia. 4th ed. Vols. I; II. Rio de Janeiro: Thieme Revinter ; 2020.
View at Publisher | View at Google Scholar - Coelho, A., Lobo, M., Gouveia, R., Sousa, P., Campos, J., Augusto, R., & Canedo, A. (2016). Abdominal aortic aneurysm - epidemiological study of patients treated in a center for a period of 8 years with the aim of promoting population screening. Angiologia e Cirurgia Vascular, 12(3), 187-193.
View at Publisher | View at Google Scholar - KIM, H. O. et al. Endovascular Aneurysm Repair for Abdominal Aortic Aneurysm: A Comprehensive Review. Korean Journal of Radiology, v. 20, n. 8, p. 1247, 2019.
View at Publisher | View at Google Scholar - Carino, D., Sarac, T. P., Ziganshin, B. A., & Elefteriades, J. A. (2018). Abdominal Aortic Aneurysm: Evolving Controversies and Uncertainties. In International Journal of Angiology (Vol. 27, Issue 2, pp. 58-80). Thieme Medical Publishers, Inc.
View at Publisher | View at Google Scholar - Mendonça CT, Moreira RCR, Timi JRR, Miyamotto M, Martins M, Stanischesk IC, et al. Comparison between open and endovascular treatment of abdominal aortic aneurysms in high surgical risk patients. J Vasc Bras. 2005 Sep;4(3):232-42.
View at Publisher | View at Google Scholar - Brown LC, Powell JT, Thompson SG, Epstein DM, Sculpher MJ, Greenhalgh RM; UK EVAR Trial Investigators. The UK EndoVascular Aneurysm Repair (EVAR) trials: randomized trials of EVAR versus standard therapy. Health Technol Assess. 2012;16(9):1-218
View at Publisher | View at Google Scholar - Antoniou GA, Antoniou SA, Torella F. Editor's Choice - Endovascular vs. Open Repair for Abdominal Aortic Aneurysm: Systematic Review and Meta-analysis of Updated Peri-operative and Long-Term Data of Randomized Controlled Trials. Vol. 59, European Journal of Vascular and Endovascular Surgery. 2020.
View at Publisher | View at Google Scholar - Greenhalgh, R. (2004). Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30- day operative mortality results: randomized controlled trial. The Lancet, 364(9437), 843-848.
View at Publisher | View at Google Scholar - REN, S. et al. Long-Term Outcomes of Endovascular Repair versus Open Repair of Abdominal Aortic Aneurysm. Annals of Thoracic and Cardiovascular Surgery. v. 18, n.3: p. 222-27, 2012
View at Publisher | View at Google Scholar - Law M. Screening for abdominal aortic aneurysms. Br Med Bull 1998;54(4):903- 13.
View at Publisher | View at Google Scholar - da Silva ES, Rodagues AJ Jr, Castro de Tolosa EM, Bueno Pereira PR, Zanoto A, Martins J.
View at Publisher | View at Google Scholar - Dias RR, Camurça, FD, Alves CMR. True aortic aneurysms: pathogenesis, natural history, medical treatment and timing of surgical indication. In: Serrano Jr. CV; Timerman A; Stefanini, E. Tratado de cardiologia: SOCESP. Barueri: Editora Manole, 2nd Ed; 2009. p. 2010-16.
View at Publisher | View at Google Scholar - Scott RA, Bridgewater SG, Ashton HA. Randomized clinical trial of screening for abdominal aortic aneurysm in women. Br J Surg. 2002 Mar;89(3):283-5. doi: 10.1046/j.0007-1323.2001.02014.x. PMID: 11872050.
View at Publisher | View at Google Scholar - Ladich, E., Yahagi, K., Romero, M. E., & Virmani, R. (2016). Vascular diseases: aortitis, aortic aneurysms, and vascular calcification. Cardiovascular Pathology,25(5), 432-441.
View at Publisher | View at Google Scholar - Norman, P. E., & Powell, J. T. (2007). Abdominal aortic aneurysm: The prognosis in women is worse than in men. In Circulation (Vol. 115, Issue 22, pp.2865-2869).
View at Publisher | View at Google Scholar - Lederle FA, Freischlag JA, Kyriakides TC, Matsumura JS, Padberg FT, Kohler TR, et al. Long-Term Comparison of Endovascular and Open Repair of Abdominal Aortic Aneurysm. New England Journal of Medicine. 2012 Nov 22;367(21):1988-97.
View at Publisher | View at Google Scholar - F. Lilja, K. Mani, A. Wanhainen,(2017). Editor's Choice - Trend-break in Abdominal Aortic Aneurysm Repair With Decreasing Surgical Workload,European Journal of Vascular and Endovascular Surgery, 53(6): 811-819
View at Publisher | View at Google Scholar - Karthikesalingam A, Grima MJ, Holt PJ, Vidal-Diez A, Thompson MM, Wanhainen A, et al. Comparative analysis of the outcomes of elective abdominal aortic aneurysm repair in England and Sweden. British Journal of Surgery. 2018 Mar 30;105(5):520-8.
View at Publisher | View at Google Scholar - Varino, J., Vale-Pereira, R., Moreira, M., Pereira, B., Correia, M., Lima, P.,... & Gonçalves, Ó. (2019). Impact of Patient Transfer after Abdominal Aortic Aneurysm Rupture. Rev Port Cir Cardiotorac Vasc, 26, 273-77
View at Publisher | View at Google Scholar - Oliveira RAD de, Duarte CMR, Pavão ALB, Viacava F. Barriers to access to services in five Health Regions of Brazil: perception of managers and professionals of the Unified Health System. Cad Saude Publica. 2019;35(11).
View at Publisher | View at Google Scholar - Arruda NM, Maia AG, Alves LC. Inequality in access to health care between urban and rural areas in Brazil: a decomposition of factors between 1998 and 2008. Cad Saude Publica. 2018 Jun 21;34(6).
View at Publisher | View at Google Scholar
