

Short Communication | DOI: https://doi.org/10.31579/2834-8761/031
Out Of the Comfort Zone - Dealing with The Emotion of Pain in Everyday Medical Treatment
- Peter Besuch *
Medical Director; for anesthesiology, ZB spec. Pain therapy, e.g. palliative medicine; Institute: MVZ of the Dessau Municipal Hospital.
*Corresponding Author: Peter Besuch, Medical Director; for anesthesiology, ZB spec. Pain therapy, e.g. palliative medicine; Institute: MVZ of the Dessau Municipal Hospital.
Citation: Peter Besuch, (2023), Out Of the Comfort Zone - Dealing with The Emotion of Pain in Everyday Medical Treatment, Clinical Endocrinology and Metabolism 2(5) DOI:10.31579/2834-8761/031
Copyright: © 2023, Peter Besuch, Bernardino. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 October 2023 | Accepted: 10 November 2023 | Published: 15 November 2023
Keywords: chronification; psychological; biopsychosocial disease
Abstract
If no somatic correlate is identified for the symptom of pain in daily practice that adequately explains the cause and on the basis of which promising therapy concepts can be created, this leads to helplessness for both practitioners and patients. The often-resulting therapeutic recommendation to accept the pain is difficult for those affected to implement. In pain research, the aim is to differentiate between types of pain based on different perspectives in order to realize mechanism-based therapy. (7) The importance of both somatopsychic and psychosomatic connections in the sense of a biopsychosocial disease model of the development and maintenance of pain finds its way into established treatment processes. (11) Due to the high expenditure of resources and the patients' expectations of the therapy as well as the therapist's needs to provide services in line with these expectations, unsatisfactory therapy courses often occur. (5) One of the most common types of pain in medical practice is back pain. With a lifetime prevalence of around 80%, back pain affects most people at least once in their lives. They are the most common reason for early retirement. Due to its economic impact, the phenomenon is one of the most pressing health problems in our society. (2) This article aims to formulate suggestions for possible changes in the diagnosis and treatment of pain in everyday treatment.
Introduction
Established treatment routines and their consequences Various reasons lead to premature allocation of patients to technical diagnostic measures that do not comply with the guidelines. The consequences of a general lack of physical activity, stress and job dissatisfaction are answered with diagnostic imaging, medication and operations. Patient satisfaction increases with the number of prescriptions. There is a risk of finding yourself in a satisfaction trap, because more prescriptions and more satisfaction do not automatically mean an improvement in the suffering. (9) It is necessary to understand pain as an emotion. Distinguishing complaints categorically according to physical or psychological origin or as acute or chronic means that in clinical practice, psychosocial accompanying factors are usually taken into account too late or not at all in the early course of the disease. Chronification has already occurred before patients receive and/or take advantage of a corresponding offer. (11) The goal is to influence the patient's learned use of the medical system as well as the physical processing and training of complaints as a consequence of the experiences in the diagnostic and therapeutic process and to strengthen the self-efficacy expectations and beliefs that are important for the success of the therapy. (6)
Illness and pain lead to disruption of daily life routines. Patients visit the doctor with the desire for restitutio ad integrum as quickly as possible. Therapy expectations are often focused on passive measures. Experiences are made that weaken confidence in the ability to regenerate. Fears, disappointments and insults associated with the limitations associated with the illness are often not communicated by patients themselves. You don't perceive the pain as a warning signal. Necessary resulting adjustments in behavior do not take place.
Alternative view
Pain is a highly subjective phenomenon with a so-called privileged access. This means that the experience is only directly accessible to those who have it. Those who feel pain cannot be mistaken about having pain, and there is no external, objective criterion for pain that can correct the belief that they are in pain. (1) In order to counteract the risk of chronicity, specific questions should be asked about impairments in different areas of life. This is possible by asking questions such as: “Which activities in everyday life do pain particularly get in the way of?” “or “In which activity is it particularly important for you to improve?”
Discuss with the patient temporary changes to everyday routines to enable regeneration and possible supportive measures, both medicinal and non-medicinal. If you are interested in the patient's causal concept, you will receive information about therapy expectations and this will result in a willingness to get involved in suggested therapy concepts. Patients are primarily interested in the possibilities of influence and not in the absence of correlates for the complaints in imaging diagnostics. Patients often equate the statement that “fortunately” nothing came out of an examination carried out with the assumption of simulated pain. It is important to “pick up” the patients where they are in order to have a common start to the treatment path. (6)
Expectations are a significant predictor of pain therapy, as they can influence the outcome of therapy both positively and negatively. Positive expectations are considered a protective factor in the transition from acute to chronic pain. Positive expectations also have a positive influence on chronic pain. (12)
Give patients confidence in the diagnosis you have made and offer the prospect of improvement in their symptoms. It is essential to emphasize the high importance of regular physical activity. It is the responsibility of the patient to realize this. This means that those affected have a significant share in the success of the therapy. If patients express concerns about taking analgesics regularly, do not see this as a disregard for your competence. This opens up the possibility of focusing on non-medicinal pain-relieving procedures such as the use of local cold or heat, TENS and movement therapy.
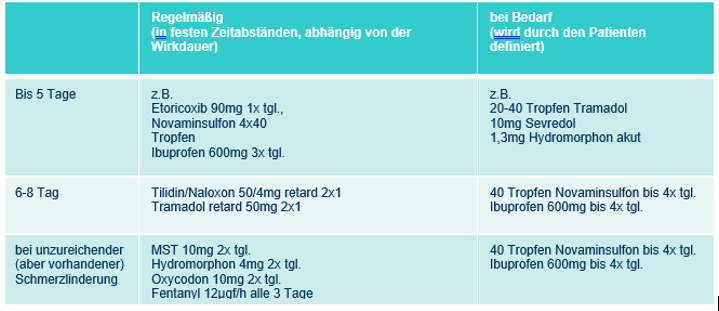
It is possible to achieve sufficient analgesia with tolerable side effects for acute pain in an outpatient setting with consistent application of existing treatment concepts. (4) If mechanism-based analgesics and co-therapeutics are selected on the basis of the WHO-scheme, a sensible introduction to drug pain therapy is possible. The aim of analgesic medication is to achieve sufficient therapeutic ability in order to avoid a lasting impairment of the quality of life, including a decrease in work effectiveness, and to prevent chronicity with its far-reaching consequences (8).
The principle of causal treatment remains undisputed even for non-acute pain. The symptom-related clinical examination contributes to the verification and classification of the complaints described in the conversation and promotes the formation of a resilient therapeutic relationship. Sufficient attention to the disease and the patient's individual concerns makes it possible to communicate and implement diagnostic and therapeutic strategies that deviate from existing expectations. (9) Evaluating pain as a warning signal in the event of impending or manifest physical and/or emotional overload gives patients the opportunity to view pain as an indication of the need for behavioral change to avoid harm.
A low-threshold offer to initiate regular physical activities is made possible by prescribing active physiotherapy. The aim here is not primarily to ensure long-term physical training in the context of, for example, physiotherapy. It should be agreed with the patient at the start of the prescription to use the duration of the possible prescription volume to integrate regular activities into everyday life. There is also the option of for example taking advantage of rehabilitation sports. If patients observe a training effect with consecutive improved mobility and performance as well as a decrease in impairment in carrying out activities of daily living, the result is often an increase in motivation to maintain self-effective measures. The physical activities carried out under supervision enable the patient to assess their current level of performance and to develop training options adapted to this. Anxiety-avoidance behavior due to the fear of harmful effects of exercise can be reduced. The effect of pain therapy should be monitored and the patients should be supported in observing behavior towards benefit orientation If so-called yellow flags occur, it makes sense to consult a pain specialist in good time. It is possible to see a pain specialist as part of the pain conferences that are mandatory in outpatient pain therapy facilities. Resulting suggestions can initially be implemented by the presenting practitioner. Requirements for inpatient pain therapy can be examined and, if indicated, suitable facilities can be recommended.
Yellow flags“ psychosocial risk factors for chronicity (10

Conclusion
In order to ensure an individualized, mechanism-based therapy for pain, it is helpful to abandon the rigid classification of acute or chronic, mental or physical and the resulting expectation of standardized treatment concepts.
Therefore, emotional factors should be integrated by addressing the patient's conflict zones in different areas of life, which have a pain-modulating effect and are influenced by pain. Opening up to the emotional world of those affected and enduring the affects that arise means leaving the comfort zone of the technically neutral physician-patient relationship. There is potential for improvement in the treatment of pain through guideline-based, targeted diagnostics and increased psychological and psychosocial screening. (3) As part of pain conferences, for example, therapy impulses can be given or, if necessary, options for specialized treatment can be shown.
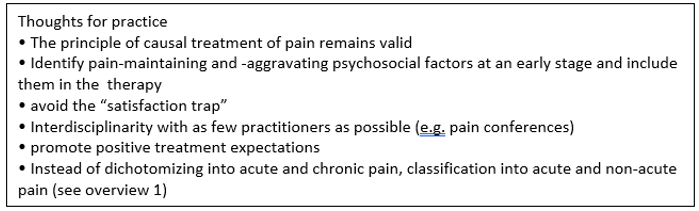
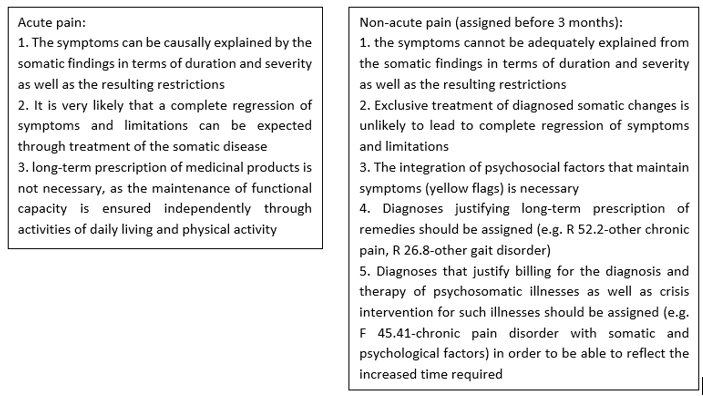
Overview 1
References
- Kurthen,M. (2006). Psychiatrie und Neurologie 4, Neurophilosophie des Schmerzes Teil 1, 44-50
View at Publisher | View at Google Scholar - Michalski, D., Hinz, A. Schmerzchronifizierung bei ambulanten Rückenschmerzpatienten. Schmerz 20, 198–209
View at Publisher | View at Google Scholar - Maschewsky-Schneider, U., Klärs, G., Ryl, L. et al. (2009). gesundheitsziele.de . Bundesgesundheitsbl. 52, 764–774
View at Publisher | View at Google Scholar - Gralow, I., (2010). Anästhesiologie, Intensivmedizin, Notfallmedizin, Schmerztherapie , 45, Ambulante Schmerztherapie-Pharmakotherapie bei Tumorschmerzen, 34-41
View at Publisher | View at Google Scholar - Maschewsky-Schneider, U., Gocke, M., Hölscher, U. et al. (2013). Gesundheitsziele.de. Bundesgesundheitsbl. 56, 1329–1334
View at Publisher | View at Google Scholar - Gaul, C., Bundes Gesundheits Blatt 57, (2014). Kopfschmerzen-Patientenschulung als Baustein multimodaler Therapieprogramme , 961-966,
View at Publisher | View at Google Scholar - Maier, C., Baron, R. & Sommer, C. Neuropathischer Schmerz. Schmerz 29, 479–485 (2015)
View at Publisher | View at Google Scholar - Schwarze, C., Zenz, D., Orlowski, O. et al. Erhebung von Schmerzen nach ambulanten Operationen. Schmerz 30, 141–151 (2016)
View at Publisher | View at Google Scholar - Schiltenwolf, M. , Schwarze ,M. , (2020). Bundesgesundheitsbl. 63 Diagnostik und Therapie von Rückenschmerzen: Was ist empfehlenswert? Was sollte unterbleiben und warum wird es dennoch gemacht? : 527-534
View at Publisher | View at Google Scholar - Geber, C., Kappis, B., Bäsch, T. et al. (2021). Schmerzprävention in der Grundversorgung. Schmerz 35, 5–13
View at Publisher | View at Google Scholar - Kaiser, U., Nagel, B., Petzke, F. et al. (2021). Vermeidung chronischer Schmerzen in der deutschen Gesundheitsversorgung. Schmerz 35, 45–52
View at Publisher | View at Google Scholar - Stuhlreyer, J., Klinger, R. (2022). Behandlungserwartungen bei postoperativen Schmerzen. Schmerz 36, 157–165
View at Publisher | View at Google Scholar
