

Case Report | DOI: https://doi.org/10.31579/2835-8295/057
Optimizing Endometrial Thickness and Pregnancy Outcomes through Subendometrial Injection of Selectively Enriched Angiogenic Precursor Cells and Growth Factors Derived from Autologous Peripheral Blood: A Novel Approach for Treating Refractory Thin End
1A4 Hospitals & Fertility Centre- Fertility Care and IVF, Chennai- India
2Seragen Biotherapeutics Pvt Ltd, Regenerative Medicine, Bengaluru, India.
*Corresponding Author: Vasanthi Palanivel, Seragen Biotherapeutics Pvt Ltd, WFF4, Bangalore Bioinnovation Centre, Helix Biotech Park, Electronics City Phase 1, Bangalore, Karnataka 560100, India.
Citation: Aruna Rajan, S. Sharmila, Vasanthi Palanivel, Shrinivas Chari, (2024), Optimizing Endometrial Thickness and Pregnancy Outcomes through Subendometrial Injection of Selectively Enriched Angiogenic Precursor Cells and Growth Factors Derived from Autologous Peripheral Blood: A Novel Approach for Treating Refractory Thin Endometrium – A Case Report, International Journal of Clinical Reports and Studies, 3(2); DOI:10.31579/2835-8295/057
Copyright: © 2024, Vasanthi Palanivel. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 March 2024 | Accepted: 02 April 2024 | Published: 09 April 2024
Keywords: intravenous glutathione; adjuvant therapy; expert opinion
Abstract
In the field of assisted reproductive techniques (ART), thin endometrium remains a sub- stantial obstacle, often resulting in diminished chances of pregnancy. This study explores a innovative method involving the hysteroscopic administration of G-CSF mobilized progenitor cells coupled with concentrated platelet-derived growth factor, an Autologous Blood Cell Derivative - ABCD-Endosera, aiming to treat thin endometrium, particularly in a patient burdened with multiple risk factors. Our subject, a 48-year-old woman who had been married for 16 Years, was experiencing low menstrual flow for the past eight years.Her medical record was complex, featuring a unicornuate uterus, fibroid, jugular vein thrombosis, hypertension, diabetes, and hypothyroidism, along with a history of six un- successful embryo transfers who had to consider surrogacy as last option. The patient was administered ABCD-Endosera hysteroscopically into the subendometrial region. This innovative approach yielded remarkable improvements in endometrial thickness, ultimately leading to a successful pregnancy and birth of healthy uneventful full-term baby. These outcomes indicate that the hysteroscopic application of progenitor cells with ABCD- Endosera could potentially offer new hope for women who, despite having undergone prior treatments, still struggle with suboptimal endometrial thickness. By boosting endometrial thickness, encouraging tissue remodeling, and ensuring smooth gestation and live birth, this method may open up new avenues in treating thin endometrium.
Introduction
Successful embryo implantation during an IVF cycle necessitates well-timed embryonic development in tandem with a receptive endometrium that is at least 7 mm thick by the end of the follicular phase. Patients with chronically thin endometrium that does not respond to standard treatments pose significant challenges in assisted reproductive techniques (ART). They may experience multiple costly IVF cycles, canceled cycles, unexpected cryopreservation of embryos, and, in extreme cases, may resort to the use of gestational carriers. Currently, no clinically approved treatment exists for thin endometrium. Previous strategies, such as hysteroscopic adhesiolysis, estrogen and gonadotropin-re- leasing hormone agonist treatment, vasoactive agents, and uterine infusion of growth factors like G-CSF have had minimal impact on successful pregnancies.However, recent advances in regenerative medicine have shown promise. Studies have successfully utilized stem cells or platelet-rich plasma (PRP) to rejuvenate reproductive tissues and treat organ failure. The presence of stem cells in the endometrium, first evidenced in 2004, have high proliferative potential and bone marrow-derived stem cells (BMDSCs) appear instrumental in endometrial regeneration [1]. Endometrial stem cells, residing in the basal layer, are likely the progenitors of endometrial cells and play a crucial role in rapid endometrial regeneration for gestation. Some clinical studies suggest that these stem cells could originate from the bone marrow [2]. Hence, bone marrow stem cells (BMSCs) may have an integral role in endometrial rebuilding, involving cell ex- changes and inflammatory stimuli [3].
Because the endometrium is a dynamic tissue, physiological angiogenesis, or the forma- tion of new blood vessels, is vital to endometrial regeneration. Angiogenesis occurs from endothelial cells of nearby blood vessels or progenitor cells released from bone marrow into peripheral blood [4-7]. Initially, hematopoietic stem cells (HSC) were harvested only from bone marrow. In the mid-1990s, HSC were mobilized from bone marrow into peripheral blood using granulocyte colony-stimulating factor (G-CSF) in healthy donors. These hematopoietic stem cells and endothelial progenitor cells, which promote angiogenesis, can be derived from peripheral blood or via bone marrow flushing. The latter yields a higher number of CD34+ endothelial progenitor cells but is more invasive [8-10].
However, using G-CSF to stimulate the release of these cells provides a less invasive approach with a high yield of CD34+ cells. Collection of these cells does not require hospitalization and is less demanding on the patient. Moreover, G-CSF plays a role in endometrial function by expressing various cellular factors, which justify its use prior to peripheral blood withdrawal in our patients. Recent trials involving cell therapies for endometrial pathologies have shown promising results, with a temporary improvement in the intrauterine environment and an increase in endometrial thickness when combined with Platelet-rich Plasma (PRP)[11]. PRP, a centrifuged human blood with high platelet concentration, has been shown to enhance endometrial thickness and vascularity through the release of various growth factors [12-15].
With this, we propose a new approach that involves hysteroscopic instillation of G-CSFmobilized progenitor cells along with a concentration of platelet-derived growth factor (Endosera) in the sub-endometrial region. This novel method aims to improve endometrial quality in terms of thickness and vascularity.
Case Presentation
We report the case of a 48-year-old Australian woman with a complex clinical history including menstrual irregularities, reproductive difficulties, and multiple concur- rent medical conditions. She had been married for 16 years and sought medical attention following the failure of 6 consecutive embryo transfers. The patienthad been dealing with menstrual irregularities for the preceding eight years. This was complicated by the presence of a unicornuate uterus and uterine fibroids, conditions that pose significant challenges to successful pregnancy. Further, she has suffered from Jugular Vein Thrombosis (JVT), a relatively rare and potentially life- threatening condition. Her clinical scenario was further complicated by several other comorbidities. The patient had a long-standing history of hypertension and diabetes mellitus, both of which needed ongoing medical management. Additionally, she was diagnosed with hypothyroidism, adding another layer of complexity to her overall health status was recommended surrogacy. Despite these health challenges, she and her partner had been trying to conceive, but experienced the failure of six consecutive embryo transfers, under- scoring the substantial fertility difficulties they faced. Informed consent was obtained from the patient for the report of her clinical data and case details.
Investigations
Upon referral to our team, the patient had already been subjected to a comprehensive range of diagnostic procedures. Our subsequent medical interventions included a laparoscopic myomectomy complemented by tubal clipping and hysteroscopy, performed in January 2020. These procedures revealed a right unicornuate uterus, in addition to a left rudimentary horn and streak ovaries on the left side. The Endometrial Receptivity Array (ERA), a test critical for enhancing reproductive success rates, was also done. The resulting diagnosis confirmed the endometrial receptivitystage to be P+4 ½.
Progenitor Cell Administration
The patient was administered Granulocyte Colony-Stimulating Factor (G-CSF) subcutaneously over two consecutive days (MCD 5&6). On the subsequent day, she underwent a progenitor cell administration procedure. Sixty milliliters of venous blood was collected and then processed in a sterile environment, using Seragen's Selective Enrichment Protocol, to enrich the mobilized progenitor cells and concentrate the platelet-derived growth factors (16-18). The implantation procedure involved the use of a 2.9 mm hysteroscope with an operating channel. An ovum pick-up needle with a single lumen was affixed to it for the stem cell implantation. The harvested cells and growth factors were then implanted in the sub-endometrial zone across all four walls of the cavity, with an equal distribution of 1-1.5 mL in each wall (as depicted in Figures 1). Following the procedure, the patient was monitored for four hours and then discharged in a stable condition.
Figure 1: Progenitor Cell Implantation via Hysteroscope: Utilizing a 2.9 mm hysteroscope with an operating channel, stem cells and growth factors are uniformly distributed in
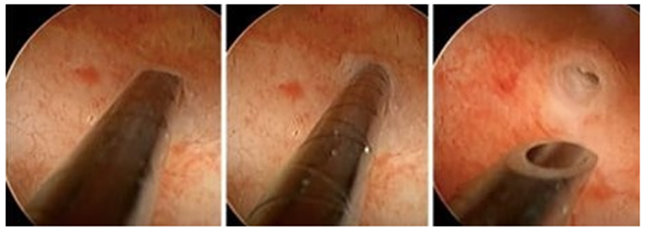
Figure 2: Endometrial thickness reached 7.2mm before ET the sub-endometrial zone's four walls, each receiving 1-1.5 ml.
Treatment Done and Result
Subsequently, the patient underwent her 7th embryo transfer at our facility, which fol- lowed three sessions of platelet derived concentrated growth factor instillation. This course of treatment enhanced the endometrial thickness to 6.8mm, demonstrating a bright triple- layer pattern. Unfortunately, while this embryo transfers initially resulted in a successful pregnancy, it eventually led to a complete spontaneous miscarriage. The patient's 8th embryo transfer, performed in September 2020, did not result in pregnancy. Despite reaching an endometrial thickness of 7mm after three sessions of intrauterine PRP instillations, the transfer did not succeed. As an Australian citizen, the patient was unable to opt for international surrogacy due to India’s latest surrogacy regulations and ban on the practice. Consequently, the remaining alternatives were to improve the endometrial environment or pursue a uterine transplantation. Addressing the challenge of the patient's thin endometrium, we conducted a hysteroscopic subendometrial stem cell instillation in the last week of September 2020. However, the planned embryo transfer was delayed due to a positive COVID-19 test result. Embryo transfer was performed after a month, following the stem cell and PRP instillations. After one cycle, hormone replacement therapy (HRT) commenced in November 2020, in conjunction with three instillations of activated PRP. 9thembryo transfer with two blastocysts was performed when the endometrial thickness reached 7.2mm on the 20th day (Fig 2). Two weeks post-transfer, a positive human chorionic gonadotropin test confirmed the success of her 9th embryo transfer. An ultrasound performed four weeks post-transfer revealed a gestational sac (Fig 3) and fetal heart beat at six weeks. The patient safely returned to Australia at 30 weeks gestation and ultimately delivered a healthy baby at 37 weeks, marking a successful conclusion to a complex and challenging reproductive journey.

Figure 3: An Ultrasound finding: Presence of a gestational sac and fetal heart beat at six weeks.
Discussion
Our study's results align with several previous investigations, suggesting that autologous stem cell implantation and platelet-rich plasma (PRP) therapy may enhance endometrial thickness and improve clinical pregnancy and live birth rates (11-19). In a pioneering human trial (20), patients suffering from Asherman's Syndrome (AS) and refractory thin endometrium exhibited substantial improvements in endometrial thickness and promising pregnancy rates. However, this trial indicated the necessity for interventional radiology assistance for the administration into the uterine arterioles. Yet, evidence supporting the beneficial effects of stem cell therapy in enhancing endometrial receptivity remains inconclusive. More comprehensive studies are needed to substantiate these promising preliminary findings. While data regarding stem cell therapy and endometrial receptivity are growing, robust clinical trials are warranted to definitively elucidate the potential role of this therapeutic strategy in treating endometrial disorders (21,22). In the context of frozen embryo transfer (FET) cycles, few studies have examined potential interventions for thin endometrium. Our case study, despite its limitations as a single-patient report, provides valuable proof of concept data supporting the feasibility of the proposed treatment approach for thin endometrium during FET cycles. Our findings may serve as a catalyst for further research into this potential treatment modality, fostering larger, multi-center studies to corroborate these preliminary results.
Conclusion
The challenge of an endometrial thickness less than 7mm remains a significant obstacle in the field of infertility, leading to reduced implantation rates. This low implantation rate is often attributed to suboptimal endometrial glandular development and impaired angio genesis, resulting in inadequate blood supply to the endometrium. The introduction of au- tologous stem cells presents a potentially promising solution for women who fail to achieve optimal endometrial thickness despite exhausting all available treatment options. This novel therapeutic strategy offers a promising avenue for endometrial regeneration, making it a focal point of contemporary research. The use of stem cells derived from uter- ine or other tissues has been explored as a potential approach to aid in endometrial re- generation. With their inherent capacity to integrate into damaged tissues, bone marrow- derived stem cells (BMSCs) are frequently utilized in cell therapies (19, 21). These cells have demonstrated potential to increase endometrial thickness, restore tissue morpholo- gy, and consequently enhance uterine receptivity in some cases (21). However, the inva- sive nature of BMSC collection remains a significant limitation to their broader use, prompting the search for less invasive stem cell sources. Our case report proposes the combined use of two minimally invasive yet potent therapeutic strategies to enhance en- dometrial receptivity, even when endometrial thickness is not within the optimal range. Despite these promising results, it is crucial to continue researching the safety, effective- ness, and cost of this treatment modality before integrating it into routine IVF procedures. This is especially relevant for women who experience recurrent issues with endometrial thickness during their infertility treatment journeys. In conclusion, our results echo previous findings regarding the potential benefits of autologous stem cell and PRP therapies for improving endometrial thickness and receptivity. Nevertheless, larger, well-designed studies are necessary to to fully comprehend the potential benefits and challenges of this innovative approach and to provide a stronger evidence base to support the broader clinical adoption of these interventions.
References
- Taylor HS. (2004). Endometrial Cells Derived From Donor Stem Cells in Bone Marrow Transplant Recipients. JAMA;292(1):81-85.
View at Publisher | View at Google Scholar - Gargett CE, Nguyen HP, Ye L, et al, (2012). Endometrial regeneration and endometrial stem/progenitor cells. Rev Endocr Metab Disord;13(4):235-251.
View at Publisher | View at Google Scholar - Chan RW, Schwab KE, Gargett CE, et.al. (2004). Clonogenicity of Human Endometrial Epithelial and Stromal Cells. Biol Reprod;70(6):1738-1750.
View at Publisher | View at Google Scholar - Tepper OM, Sealove BA, Murayama T, et al. (2003). Newly emerging concepts in blood vessel growth: recent discovery of endothelial progenitor cells and their function in tissue regeneration. J Invest Med;51(6):353-359.
View at Publisher | View at Google Scholar - iang S, Walker L, Afentoulis M, Anderson DA, Jauron-Mills L, ET ALL., (2004). Transplanted human bone marrow contributes to vascular endothelium. Proc Natl Acad Sci U S A.;101(48): 16891-16896.
View at Publisher | View at Google Scholar - Urbich C, Dimmeler S. (2004). Endothelial progenitor cells. Circ Res;95(4):343-353.
View at Publisher | View at Google Scholar - 7Gargett CE, Schwab KE, Brosens JJ, Puttemans P, ET ALL., (2014). Potential role of endometrial stem/progenitor cells in the pathogenesis of early-onset endometriosis. Mol Hum Reprod;20(7):591-598.
View at Publisher | View at Google Scholar - Baumann I, Testa NG, Lange C, de WE, Luft T, et all., (1993). Haemopoietic cells mobilised into the circulation by lenograstim as alternative to bone marrow for allogeneic transplants. Lancet;341(8845):369.
View at Publisher | View at Google Scholar - Dreger P, Haferlach T, Eckstein V, et al. (1994). G-CSF-mobilized peripheral blood progenitor cells for allogeneic transplantation: safety, kinetics of mobilization, and composition of the graft. Br J Haematol;87(3):609-613.
View at Publisher | View at Google Scholar - 10.Bensinger WI, Weaver CH, Appelbaum FR, et al. (1995). Transplantation of allogeneic peripheral blood stem cells mobilized by recombinant human granulocyte colony-stimulating factor. Blood;85(6):1655-1658.
View at Publisher | View at Google Scholar - Zhang S, Li P, Yuan Z, et al. (2019). Platelet-rich plasma improves therapeutic effects of menstrual blood- derived stromal cells in rat model of intrauterine adhesion. Stem Cell Res Ther;10(1):61.
View at Publisher | View at Google Scholar - Agarwal M, Mettler L, Jain S, Meshram S, Gunther V, Alkatout I. (2020). Management of a Thin
View at Publisher | View at Google Scholar - Endometrium by Hysteroscopic Instillation of Platelet-Rich Plasma Into The Endomyometrial Junction: A Pilot Study. J Clin Med;9(9):2795.
View at Publisher | View at Google Scholar - Tandulwadkar SR, Naralkar MV, Surana AD, Selvakarthick M, Kharat AH. (2017). Autologous Intrauterine Platelet-Rich Plasma Instillation for Suboptimal Endometrium in Frozen Embryo Transfer Cycles: A Pilot Study. J Hum Reprod Sci;10(3):208-212.
View at Publisher | View at Google Scholar - Nazari L, Salehpour S, Hoseini S, et al. (2019). Effects of autologous platelet-rich plasma on endometrial expansion in patients undergoing frozen thawed embryo transfer: A double-blind RCT. Int J Reprod Biomed;17(6):443- 448.
View at Publisher | View at Google Scholar - Maleki-Hajiagha A, Razavi M, Rouholamin S, Rezaeinejad M, Maroufizadeh S, ET ALL., (2020). Intrauterine infusion of autologous platelet-rich plasma in women undergoing assisted reproduction: A systematic review and meta-analysis. J Reprod Immunol; 137:103078.
View at Publisher | View at Google Scholar - Tal R, Shaikh S, Pallavi P, et al. adult bone marrow progenitors become decidual cells and contribute to embryo implantation and pregnancy. PLoS Biol.;17(9): e3000421.
View at Publisher | View at Google Scholar - Singh N, Mohanty S, Seth T, Shankar M, Bhaskaran S, ET ALL., (2016). Autologous stem cell transplantation in refractory Asherman’s syndrome: a novel cell-based therapy. J Hum Reprod Sci. 2014;7(2):93.
View at Publisher | View at Google Scholar - Nagori CB, Panchal SY, Patel H. Endometrial regeneration using autologous adult stem cells followed by conception by in vitro fertilization in a patient of severe Asherman's syndrome. J Hum Reprod Sci. 2011;4(1):43-48.
View at Publisher | View at Google Scholar - Singh N, Shekhar B, Mohanty S, Kumar S, Seth T, Girish B. Autologous Bone Marrow Derived Stem Cell Therapy for Asherman's Syndrome and Endometrial Atrophy: A 5-Year Follow-up Study. J Hum Reprod Sci. 2020;13(1):31-37.
View at Publisher | View at Google Scholar - Mouhayar Y, Sharara FI. G-CSF and stem cell therapy for the treatment of refractory thin lining in assisted reproductive technology. J Assist Reprod Genet. 2017;34(7): 831-837.
View at Publisher | View at Google Scholar - Santamaria X, Cabanillas S, Cervello I, Arbona C, ET ALL., (2016). Autologous cell therapy with CD133+ bone marrow-derived stem cells from refractory Asherman’s syndrome and endometrial atrophy: a pilot cohort study. Hum Reprod;31(5):1087–1109.
View at Publisher | View at Google Scholar - Wang X, Liu L, Mou S, Zhao H, et all., (2019). Investigation of platelet-rich plasma in increasing proliferation and migration of endo- metrial mesenchymal stem cells and improving pregnancy outcome of patients with thin endo- metrium. J Cell Biochem;120(5):7403-7411
View at Publisher | View at Google Scholar
