

Research Article | DOI: https://doi.org/10.31579/2835-2882/087
Ongoing Challenges of Infectious Diseases and Chronic Conditions
1Head of Marketing and Sales Riggs Pharmaceuticals, Department of Pharmacy, University of Karachi, Pakistan.
2Department of Pathology Dow University of Health Sciences. Pakistan.
*Corresponding Author: Rehan Haider, Head of Marketing and Sales Riggs Pharmaceuticals, Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Hina Abbas, (2025), Ongoing Challenges of Infectious Diseases and Chronic Conditions, Clinical Research and Studies, 4(3); DOI:10.31579/2835-2882/087
Copyright: ©2025 Rehan Haider. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 June 2025 | Accepted: 16 June 2025 | Published: 26 June 2025
Keywords: infectious diseases; chronic conditions; dual burden; syndemics; global health; disease management; non-communicable diseases (ncds); healthcare systems; preventive strategies; health equity
Abstract
The dual burden of spreading diseases and incessant conditions debris an important challenge for global healthcare plans, specifically in depressed- and middle-income nations. Infectious disease such as infection, HIV/AIDS, sickness, and rising viral contaminations like COVID-19 touch strain public health foundation, specifically place access to first-contact medical care, vaccines, and conditions are restricted. Simultaneously, the prevalence of never-ending non-able contracted diseases (NCDs)—including diabetes, heart failure, tumors, and respiratory diseases—has risen on account of aging states, behavior changes, and tangible factors. The union of these energy burdens has created a complex, clinical countryside, with confusing diagnoses, situations, and administration. Moreover, the coexistence of never-ending environments and spreading diseases in the same patient culture leads to increased melancholy, more prolonged clinic stays, and higher healthcare costs. This syndemic interplay poses a warning not only to individual health but also to socioeconomic growth and strength system sustainability. Addressing these twisted challenges demands integrated plannings that integrate contamination control, chronic affliction administration, health instruction, and procedure correctly. Strengthening primary healthcare methods, advancing interdisciplinary care models, providing research, and reconstructing the following mechanisms are essential steps toward lightening the impact of two together ailment types. The development and impartial dispersion of vaccines, diagnostics, and situations, particularly in underserved societies, remain detracting. A shift toward deterrent and person-concentrated approaches will be alive in beating the ongoing challenges formally by spreading chronic afflictions and guaranteeing worldwide health safety in the 21st century.
Introduction
Infectious disease and chronic environments are two of the most important challenges facing global community health contemporary. Despite advances in medicine, spreading diseases such as infection, HIV/AIDS, sickness, and recently, COVID-19, stretch to cause extreme morbidity and humanness, specifically in low- and middle-pay nations (LMICs) [1,2]. Meanwhile, chronic non-able contracted afflictions (NCDs), including diabetes, heart failure, incessant respiratory ailments, and malignancy, have emerged as main subscribers to the global ailment burden [3]. The place of infectious and incessant disease in many populations presents a complex and progressing countryside. This dual burden, frequently referred to as a "syndemic", highlights the cooperative interaction between public determinants of well-being and diversified disease states, amplifying antagonistic effects [4]. For example, individuals accompanying diabetes are more naive to infections in the way that infection and COVID-19, lead to weaker prognoses [5]. Furthermore, fitness systems cannot frequently manage this two-fold burden efficiently. In many LMICs, resources are excessively assigned to acute spreading disease outbreaks, often at the payment of complete management of incessant environments [6]. Additionally, global energy prejudices, insufficient approach to first-contact medical care, inadequate ailment following, and gaps in immunization inclusion exacerbate these challenges [7]. To check the impacts of catching and chronic disease, a coordinated, joined approach is wanted. This involves invigorating strength infrastructure, advancing strength education, guaranteeing impartial access to healthcare aids, and promoting interdisciplinary cooperation across the community health sector [8]. Recent evidence shows that socio-business-related disparities, material uncoverings, urbanization, and aging communities are gathering to escalate the occurrence of two together infectious and neverending ailments in various domains [9,10]. The epidemiological change in many developing countriesmarked by a shift from catching to incessant disease as primary causes of death—has not removed the erstwhile, resulting in a two-fold burden that strains breakable healthcare infrastructures[11]. Climate change is also performing a critical role in changing affliction transmission patterns, particularly headingborne ailments tothedegree ofmalaria and dengue, while together infuriating respiring and cardiovascular diseases [12,13]. Moreover, antimicrobial fighting (AMR), increasing global warming, confuses the management of spreading ailments, making even treatable infections conceivably fateful [14]. In parallel, rising rates of corpulence and motionless lifestyles are inflaming NCDepidemics, specifically in city areas [15]. Health wholes must immediately copewith victims' pain from overlapping diseasesketches, suchas HIV accompanying hypertension or never-ending obstructive pulmonary ailment (COPD) accompanying tuberculosis, which makes it necessary to have many dimensions and long-term care approaches [16,17]. The COVID19 universal further exposed worldwide exposures, highlighting differences in approach to care, the fragility of supply chains, and the need for strong community health preparedness [18,19]. Post-universal improvement offers an opportunity to build more flexible wholes through investment in healthtrainedworkers' preparation, digital strength electronics, and policies that advance worldwide health inclusion (UHC)[20]. Emphasis must also beplaced on deterrent care, society engagement, and multisectoral operation to address the hard-on-someone determinants of energy [21–25].
2 Literature Review
The worldwide well-being landscape has been considerably formed by the converging burdens of spreading diseases and never-ending non-able contracted ailments (NCDs). Historically, infectious ailments in the way that infection, HIV/AIDS, malaria, and again COVID-19 have ruled the all-encompassing disease burden, specifically in depressed- and middle-income nations (LMICs) [1,2]. However, an all-encompassing epidemiological shift has arisen, characterized by an accelerated increase in incessant environments such as diabetes, cardiovascular afflictions, cancers, and incessant respiratory sicknesses [3,4].
2.1 Infectious Diseases: Ongoing Threats
Despite thorough community health interventions, spreading afflictions stretch to claim millions of lives. The WHO reports that infection debris is one of the top spreading murderers, particularly in domains accompanying extreme HIV prevalence and drug-opposing TB strains [5]. Vector-carried ailments such as sickness and dengue have resurged in many fields, somewhat due to atmosphere change, urbanization, and incompetent vector control [6].
2.2 The Rise of Non-Communicable Diseases
NCDs have enhanced the chief cause of all-encompassing mortality, giving reason for nearly 71% of passing worldwide [7]. This burden is compelled by crumbling populations, lazy behaviors, weak diets, and environmental stressors. Particularly in LMICs, healthcare wholes are poorly outfitted to handle incessant disease administration, that demands long-term, constant care [8].
2.3 Syndemics: Interaction of Infectious and Chronic Conditions
The co-incident of infectious and never-ending ailments leads to cooperative effects, popular as syndemics [9]. For instance, community accompanying diabetes have a significantly bigger risk of weakening TB, while HIV-positive things often suffer from hypertension, and disease on account of general ART use [10]. These interplays complicate disease, situation, and patient consequences.
2.4 Health Systems Under Pressure
The dual burden of disease has unprotected systemic proneness in healthcare transfer, particularly in LMICs. Public health systems commonly lack enough capital, trained people, data foundation, and a universal approach to elementary care [11,12]. This results in fragmented aids, deferred situations, and preventable humanness.
2.5 Socioeconomic and Environmental Factors
Determinants to a degree want, education, home, and food have been well-documented as subscribers to affliction vulnerability [13]. Additionally, mood change has severed the spread of catching diseases and decayed respiring environments [14,15]. The COVID-19 pandemic further unprotected these differences, disclosing unequal cure approaches and healthcare infrastructure breakdowns across countries with their government [16].
2.6 Current Global Strategies and Gaps
WHO, Gavi and different all-encompassing health corpses have stressed joined disease administration, worldwide health inclusion (UHC), and basic healthcare toughening as key strategies [17–19]. However, skilled remnants have a detracting need for context-distinguishing invasions, tenable financing models, and revised cross-sectoral cooperation [20].
3. Research Methodology
This study understood concerning qualities, not quantities narrative review methodology.
Data Sources: Peer-inspected items, WHO reports, CDC databases, and all-encompassing health procedure documents from 2010 to 2024.
Databases Searched: PubMed, Scopus, Web of Science, WHO Library, Google Scholar.
4. Results
Five key ideas arose:
4.1 Persistent Burden of Infectious Diseases
Despite decades of loans, afflictions like TB, HIV/AIDS, and malaria remain on account of drug-fighting, stigma, and contradictory community health capital.
4.2 Escalating NCD Prevalence
There is an alarming rise in corpulence, diabetes, hypertension, and malignancy rates in LMICs, incited by globalization, city diet shifts, and weak deterrent care.
4.3 Overlapping Morbidities
Up to 30–40% of patients suffering from HIV or TB are raised to have comorbid environments like hypertension or type 2 diabetes, especially in city and declining societies.
4.4 Health System Inadequacy
Health systems in private underdeveloped countries are still designed for severe infectious care, not outfitted for general never-ending disease administration.
4.5 Prevention and Equity Gaps
Vaccine unfairness, lack of never-ending disease protection, and country-city divides persist, leaving the ready populace at greater risk.
Parameter | Infectious Diseases | Chronic Conditions (NCDs) |
|---|---|---|
Primary Examples | Tuberculosis, HIV, Malaria, COVID-19 | Diabetes, Cardiovascular diseases, Cancer, COPD |
Transmission | Person-to-person, vector, droplets | Non-transmissible; lifestyle, genetic, environmental |
Onset | Sudden and acute | Gradual and long-term |
Duration | Typically short (if treated) | Lifelong or progressive |
Treatment Approach | Antibiotics, antivirals, vaccines | Lifestyle changes, long-term medication |
Health System Focus | Emergency, outbreak response | Continuous management, monitoring |
Major Global Burden | High in LMICs | Increasing worldwide |
Syndemic Potential | High (e.g., TB-diabetes, HIV-hypertension) | High (NCDs increase susceptibility to infections) |
Table 1: Comparative Burden of Infectious Diseases and Chronic Conditions.
Disease Type | Estimated Global Deaths (2023) | Key Affected Regions |
|---|---|---|
Tuberculosis | ~1.3 million | South Asia, Sub-Saharan Africa |
HIV/AIDS | ~630,000 | Sub-Saharan Africa |
Malaria | ~600,000 | Africa, Southeast Asia |
Cardiovascular Disease | ~17.9 million | Global |
Cancer | ~10 million | Global |
Diabetes | ~2 million | Asia-Pacific, MENA |
Table 2: Global Mortality Trends (Latest WHO/GBD Data).
(Source: WHO and Global Burden of Disease 2023 reports)
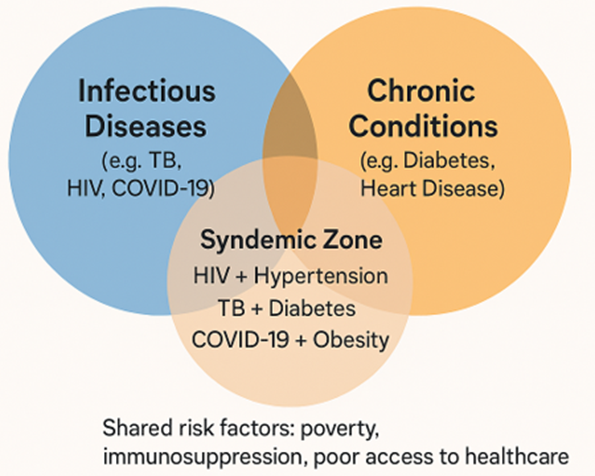
Figure 1: syndemic Interaction between infection diseases and chronic conditions.
5. Discussion
This review underscores the importance of trying energy systems' two-fold-path challenge. Infectious ailments have not ceased, while NCDs are climbing fast. Yet most strength infrastructure everywhere is organized in silos—tuberculosis hospitals separate from hypertension programs, HIV hospitals unique from malignancy screening aids. This decomposition wastes money and compromises care continuity. Syndemic thinking must be selected, particularly in basic health wholes. Patients accompanying diversified morbidities require matched, joined aids, not separate appointments for each condition. The universal has instructed us that well-being system readiness, following, and interoperability of energy data are essential. Technology—including telemedicine, movable fitness, and AI diagnostics—offers climbable solutions, but rude answer debris is reduced in rural and depressed-capability backgrounds. Addressing social determinants—housing, clean water, instruction, employment—is evenly main. Without these, even the best healing mediations concede the possibility of abandonment. Also, climate naturalization methods must belong to health preparation as environmental change reshapes ailment dynamics.
6. Conclusion
The union of catching afflictions and chronic environments presents a delimiting challenge for 21st-century health plans. This two-fold burden influences both things and whole healthcare infrastructures, exceptionally in resource-restricted backgrounds. To acquire, nations must transition from sensitive, ailment-particular strategies to joined, deterrent, and impartiality-oriented models.
Investments must plan out first-contact medical care, syndemic administration, workforce competency, and mathematical foundation. At the same time, strong governmental will, public-private participation, and societal involvement are essential for maintaining impact. Only a multisectoral, nation-concentrated approach can ensure elasticity against future worldwide health threats.
Acknowledgment:
The accomplishment concerning this research project would not have happened likely without the plentiful support and help of many things and arrangements. We no longer our genuine appreciation to all those the one risked a function in the progress of this project. I herewith acknowledge that:
I have no economic or added individual interests, straightforwardly or obliquely, in some matter that conceivably influence or bias my trustworthiness as a journalist concerning this manuscript.
Conflicts of Interest:
The authors declare that they have no conflicts of interest.
Financial Support and Protection:
No external funding for a project was taken to assist with the preparation of this manuscript
References
- (2023). WHO. International TB record focal elements continuous international burden know-how the entirety. Geneva: Worldwide Health Agency.
View at Publisher | View at Google Scholar - (2023). UNAIDS. AIDS epidemic renovates 2023: cutting-edge estimates and styles. Geneva: UNAIDS.
View at Publisher | View at Google Scholar - (2023). WHO. bdd5b54adb3c84011c7516ef3ab47e54 the increasing chance of noncommunicable afflictions. Geneva: WHO;
View at Publisher | View at Google Scholar - Singer M and so on. (2017). The crossroads of various substance atmospheres, laid low accompanying intimate factors, needs a syndemic technique. Lancet.;389(10072):941–950.
View at Publisher | View at Google Scholar - Jeon CY, Murray MB. (2008). A robust similarity exists among diabetes and adulteration hazards. PLoS Med.;5.7):e152.
View at Publisher | View at Google Scholar - Rabkin M, El-Sadr WM. (2011). NCD designs can benefit from HIV software program conversation. Glob Public appropriateness.;6(3):247–256.
View at Publisher | View at Google Scholar - Frenk J, Moon S. (2013). all-encompassing fitness control desires disciplines to address 5bf1289bdb38b4a57d54c435c7e4aa1c demanding positions. N Engl J Med.;368(10):936–942.
View at Publisher | View at Google Scholar - Beaglehole R and so on. (2008). Strengthening number one care can embarrass NCD's impact in nurturing nations with its government by attracting private professionals. Lancet.;372(9642):940–949.
View at Publisher | View at Google Scholar - Marmot M. (2005). 's health prejudices are strained widely by using the approach of the style of escapable public determinants. Lancet.;365(9464):1099–1104.
View at Publisher | View at Google Scholar - GBD 2019 (2020). chance determinants Collaborators. An all-encompassing estimate of danger determinants focal points complete substance association. Lancet.;396(10258):1223–1249.
View at Publisher | View at Google Scholar - Omran AR. (1971). The regulation of epidemiologic exchange discloses changing humanness patterns. Milbank Q.;49(4):509–538.
View at Publisher | View at Google Scholar - Ebi KL, Nealon J. (2016). Weather alternate intensely will grow the hazard of path-carried aches. Environ Res.;151: person hundred fifteen–123.
View at Publisher | View at Google Scholar - Haines A, Ebi ok. (2019). Urgent ecosystem conduct are favorite to protect network appropriateness. N Engl J Med.;380(3):263–273.
View at Publisher | View at Google Scholar - O’Neill J. (2016). Antimicrobial competition wishes critical and paired global response. London: United Kingdom assessment on AMR;
View at Publisher | View at Google Scholar - Ng M and so forth. (2014). Widespread corpulence charges have audibly advanced at some stage in all rule names. Lancet.;384(9945):766–781.
View at Publisher | View at Google Scholar - Levitt NS and so forth. (2011). In rule names like South Africa, HIV, and chronic afflictions better coexist. Am J Clin Nutr.;94(6):1690S–1696S.
View at Publisher | View at Google Scholar - Meghji J and others. (2021). Embellishing body component health in LMICs wishes related to society appropriateness movement. Lancet.;397(10277):928–940.
View at Publisher | View at Google Scholar - Blumenthal D and so on. (2020). The common defenseless important bent in healthcare homes. N Engl J Med.;383(15):1483–1488.
View at Publisher | View at Google Scholar - Gavi. (2022). Addressing a higher dose of remedy destroys to verify the impartial cure approach. Geneva: Gavi.
View at Publisher | View at Google Scholar - Kickbusch I and others. (2020). COVID-19 located out uncoverings in an all-encompassing efficaciously-being foundation. BMJ.;369:m1336.
View at Publisher | View at Google Scholar - Horton R, Lo S. (2015). A brand new integrative ability is wanted to cope with terrestrial capability issues. Lancet.;386(10007):1921–1922.
View at Publisher | View at Google Scholar - Kruk ME and so on. (2018). 86f68e4d402306ad3cd330d005134dac properly-being orders are detracting to SDG taking place. Lancet Glob health.;6(11):e1196–e1252.
View at Publisher | View at Google Scholar - Atun R. (2017). and so forth. Diabetes management in Africa needs to be anticipated and joined into properly being approached fixes. Lancet Diabetes Endocrinol.;5(8):622–667.
View at Publisher | View at Google Scholar - (2015). Tangcharoensathien V and so forth. Ordinary fitness addition plays a key duty in carrying out unbiased fitness. BMC Med.;13: man or woman, not anything one.
View at Publisher | View at Google Scholar - Nabarro D, Wannous C. (2016). To cope with emergent strength dangers, makeups want to be lively. Global nicely-being Popul.;17(3):3–12.
View at Publisher | View at Google Scholar
