

Research Article | DOI: https://doi.org/10.31579/2834-8664/013
Morphological Characteristics of the Duodenum Through the use of Imaging Studies
- María Esther del Toro Rodríguez 1
- Moraima Martell Martínez 2*
- Damary Guerrero Delgado 3
- Emeregildo José González Agüero 4
- Milaris Cabrera Heredia 5
- Adriana Ribacoba Martínez 6
1 Specialist I Degree in Human Anatomy. Department of Medicine. University of Medical Sciences Camagüey, Cuba.
2 Master in Medical Humanities. Associate Research Assistant Professor at the University of Medical Sciences. Camaguey, Cuba.
3 Specialist in I degree of Biochemistry. Assistant Professor Camaguey University of Medical Sciences Cuba.
4 Specialist I Degree Caumatology and Aesthetic Surgery. Assistant teacher. Aspiring researcher. "Martín Chang Puga" Hospital. Camaguey, Cuba.
5 Specialist I Degree in Pharmacology. Department of Medicine. University of Medical Sciences Camagüey. Camaguey, Cuba.
6 Internal Medicine. Professor Instructor Camaguey Medical Sciences University Cuba.
*Corresponding Author: Moraima Martell Martínez, Specialist I Degree in Human Anatomy. Department of Medicine. University of Medical Sciences Camagüey, Cuba.
Citation: Toro Rodríguez MED., Moraima M. Martínez., Damary G. Delgado, González Agüero EJ., et al. (2023) Morphological Characteristics of the Duodenum Through the use of Imaging Studies, International Journal of clinical and Medical Case Reports, 2(1); Doi:10.31579/2834-8664/013
Copyright: © 2023, Moraima Martell Martínez. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 January 2023 | Accepted: 13 January 2023 | Published: 19 January 2023
Keywords: duodenum/anatomy&histology; duodenum/diagnostic imaging; duodenal ulcer/ diagnostic imaging; aged; male
Abstract
Background: the duodenum is the only segment of the intestine that presents a double location, in relation to the peritoneum, behaving as an intra and extra-peritoneal organ, contributing to determine a large number. Objective: to describe the anatomical-clinical modifications of the duodenum, through imaging studies. Methods: a cross-sectional descriptive study was carried out where the universe was constituted by 26 radiological reports of medical indications in contrasted esophageal, stomach and duodenum exams to patients with symptomatology in these organs, showing the results in tables.
Results: in all cases, the situation, relations and portions of the duodenum were maintained. The forms of the duodenum found were: horseshoe and letter C, a predominance of the last. Most cases did not present clinical-radiological alterations, in the rest, a small number of entities: duodenal ulcer and widening of the duodenal frame.
Conclusions: a predominance in the form of letter C as a duodenal frame was observed. When relating these forms with the modifications and clinical entities, the horseshoe showed a greater number. The group of 61 to 70 years predominated at the expense of the male sex. In the study, more than half of the cases did not present clinical-radiological alterations and the frequency of this entities showed the predominance of the duodenal ulcer and the widening of the duodenal frame.
Introduction
The small intestine is a tubular organ about six to seven meters long, with a diameter that tapers from beginning to end, and consists of three portions: duodenum, jejunum, and ileum. Due to the location and small size of the duodenum, the diagnosis of duodenal diseases is sometimes difficult, so it is necessary to know them through optimal use of imaging techniques, which allow an accurate diagnosis and proper management. of the patient [1].
The duodenum is the initial and shortest portion (25 cm) of the small intestine, it is also the widest and most fixed. This organ begins at the pylorus, towards the right side, and ends at the duodenojejunal junction, on the left side. Four portions of it are described: 2 Upper portion (1st portion): (cuts around 5cm), mostly horizontal, and located anterolaterally to the body of the L1 vertebra. Descending portion (2nd portion): Longest (7-10 cm), runs inferiorly along the right side of the L2 and L3 vertebrae and curves around the head of the pancreas; initially it is located to the right and parallel to the inferior vena cava.
The common bile duct and the main pancreatic ducts enter its posteromedial wall through the hepatopancreatic ampulla. Horizontal portion (3rd portion): 6-8 cm long, it crosses anterior to the inferior vena cava and the aorta and posterior to the superior mesenteric artery (SMA) and the inferior mesenteric vein at the level of the L3 vertebra. Ascending portion (4th portion): It is short, measuring about 5 cm, starting to the left of the L3 vertebra and ascending to the upper border of the L2 vertebra, 2-3 cm to the left of the midline. It passes over the left side of the aorta to reach the lower border of the body of the pancreas. Here it curves to join the jejunum at the duodenojejunal junction, which forms an acute angle, the duodenojejunal flexure, supported by the attachment of the suspensory duodenum muscle (ligament of Treitz) [2].
Despite all its connections, the fixation of the duodenum is not absolute, in such a way that this organ descends slightly when the subject goes from the horizontal to the vertical position [3].
The duodenum originates from the caudal portion of the foregut and the cephalic portion of the midgut, the boundary between the two origins being the hepatic bud. Due to the rotation of the stomach it adopts a C shape, during the second month the lumen of the duodenum is obliterated, due to the proliferation of the endodermal cells of its walls; however, soon after it is channeled again by the action of apoptosis. Since the foregut is supplied by the celiac trunk and the midgut by the superior mesenteric artery, the duodenum receives branches from both arteries [4].
The duodenum is made up, like the entire intestinal tube, of four superimposed layers that are, from the outside in, the tunics: serosa and muscularis, the submucosal tissue, and the mucosa [3,5].
The arteries of the duodenum arise from the celiac trunk and the superior mesenteric artery (SMA). The common hepatic artery originates from the celiac trunk, the gastroduodenal artery, the terminal branch of the common hepatic artery, gives rise to the superior pancreaticoduodenal artery, which supplies the duodenum near the entrance of the common bile duct in its descending portion.
The pancreaticoduodenal arteries lie in the curve formed between the duodenum and the head of the pancreas and supply other structures. The anastomosis between the superior and inferior pancreaticoduodenal arteries (ie, between the celiac and superior mesenteric arteries) occurs at the entrance to the common bile duct and the junction of the descending and horizontal portions of the duodenum. At this point an important transition in the blood supply of the proximal digestive tract takes place as it extends orally up to the abdominal portion of the esophagus (inclusive), the blood reaches the digestive tract through the celiac trunk; distally, and extending caudally to the right colic flexure, blood comes from the superior mesenteric artery.
Anatomical relations of the duodenum
The duodenum by its concave edge is related to the pancreas which is encompassed by all portions of the duodenum. The superior portion is related anteriorly to the square lobe of the liver and the gallbladder, while posteriorly it is related to the portal vein, the common bile duct, and the gastroduodenal artery.
The superior border of this portion is related to the common hepatic artery. The descending portion is related in front with the root of the transverse mesocolon, in addition, with the jejunal loops in its inframesocolic part. Said portion behind is related to the right kidney and its pedicle and with the inferior vena cava, in its posterior wall the common bile duct and the main pancreatic duct open, which previously join to form the hepatopancreatic ampulla [4].
According to Prives M et al. [5] In the anatomical description in living man, by radiological examination, the initial portion of the duodenum stands out as a special part called the duodenal bulb, which presents the shape of a triangular shadow with the base directed towards the pylorus, from which it is separated. at the time of contraction of the latter by a clear stripe, which corresponds to the contracted pylorus. The radiographic limits of the duodenum are: from the strip of clarity in the area of the pylorus to the vertex of the triangular opacity; in the cadaver, the corresponding limits are the pyloric valve and the first circular fold of the mucosa. The mucosa of the bulb, like that of the pylorus, presents longitudinal folds, while in the rest of the duodenum, the mucosal folds are circular. These peculiarities of the duodenal bulb are due to the fact that it is not derived from the midgut, like the entire duodenum, but rather from the foregut. Numerous factors intervene in the differences in shape, size and color in the organic systems in the living and in the cadaver: the changes that occur with death, the fixation and conservation processes, among others. In the cadaver the initial portion has the same shape and the same diameter as the rest of the duodenum.
Prives M et al [5]. consider that this organ presents extraordinary variations in its shape and location, but that three fundamental ones can be distinguished: Duodenum in the shape of a horseshoe, located as in the corpse; where it presents the relief of all the portions: superior, descending, horizontal (inferior) and ascending.
The alterations of the duodenum are atresia and stenosis of the intestine: atresias and stenosis can occur anywhere in the intestine, the majority occurring in the duodenum, the smaller proportion in the colon, and an equal number in the jejunum and ileum. Atresias of the upper portion of the duodenum are due to lack of recanalization.
However, in the following portions, it is likely that the stenosis and atresia are caused by vascular disorders that compromise the blood supply of a segment of the intestine, so that it becomes necrotic in that area and causes narrowing or complete loss of that region. These disorders can be caused by abnormal rotation, volvulus, gastroschisis, omphalocele, and other factors [4,6].
Due to the morphological characteristics of the duodenum and the different diseases that this organ can present, as well as the difficulty that exists when a diagnosis is issued due to its anatomical situation, the following objective was raised to describe the anatomoclinical modifications of the duodenum, through imaging studies.
Materials and methods
A descriptive cross-sectional study was carried out in the Imaging Department of the Manuel Ascunce Domenech University Hospital. The universe was made up of 26 radiological reports of medical indications in confirmed examinations of the esophagus, stomach and duodenum in patients with previous endoscopic examinations and symptoms suggestive of disorders in these organs. Radiological examinations that studied the esophagus and stomach were excluded. The data obtained were captured in a model to be summarized in tables, after statistical processing. The results of the radiological reports with the clinical radiological entities detected were recorded in tables, the descriptive statistics of absolute frequency and percentage were applied.
As part of the research ethics, the data and radiological reports were obtained through communication between the Human Anatomy professors of the Faculty of Medical Sciences of Camagüey and the Department of Imaging of the hospital in question. They were used to be presented as results of this research and in scientific events. Those previously described were taken as anatomical norms, modifications were considered when they did not comply with them.
Results and Discussion
When analyzing the 26 radiological reports of medical indications in contrasted examinations of the esophagus, stomach and duodenum in these patients, it was possible to verify the relationship between sex and age group, a predominance of the male sex was observed in five cases for a 31, 25 %, in the age group of 61-70 years, it could be observed that the following groups are 31-40 and 41-50 years each with a total of four cases for 15.38% (table 1).
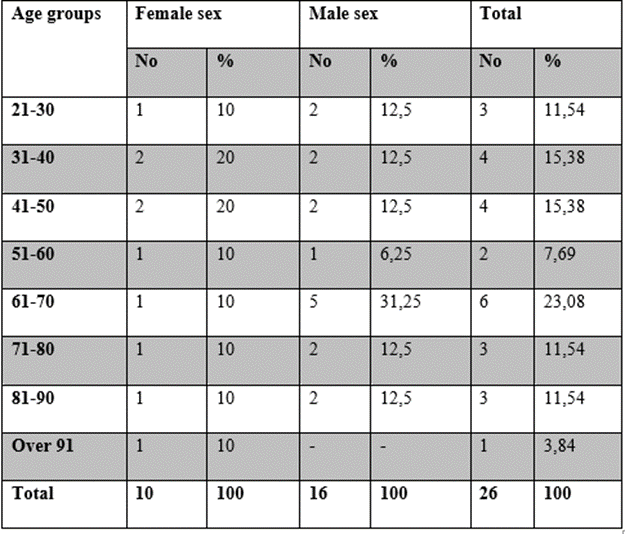
Source: Imaging department statistics book
The frequency of the duodenal frame shape in relation to sex, whose result was the predominant C shape for both sexes equally for a total of 16 cases for 61.5%. When analyzing the female sex, this form of duodenal frame predominated with 72.7% (figure 1). In the horseshoe shape, the male sex behaved with a greater number with seven cases (figure 2). This form of duodenal frame was the one with the least behavior in both sexes with 10 cases for 38.5% (table 2).
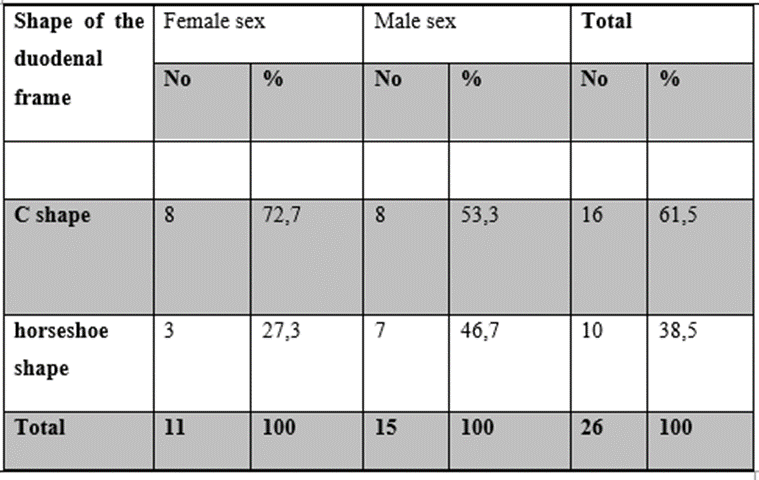
Sources: Book of statistics and radiological images
Regarding the modifications and clinical entities in relation to the forms of the duodenal frame, it is significant to highlight a predominance of radiological images without gastroduodenal alterations in 17 cases for 65.38%. It coincided with the shape of the letter C in 14 cases for 53.8%, and with the horseshoe shape in three cases for 11.5%. The modifications associated with clinical entities corresponded mostly to the horseshoe shapes with seven cases for 26.9% and with the letter C shape 2 cases for 7.6%.
The frequency of the clinical-radiological entities found in the present investigation showed the predominance of two fundamental ones: duodenal ulcer and the widening of the duodenal frame.
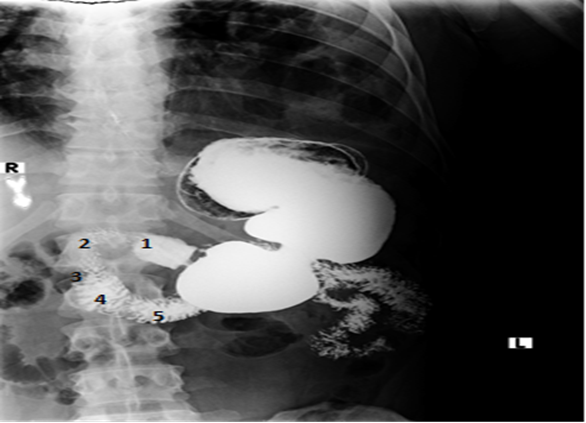
Sources: Radiological image from the database of the Manuel Ascunce Domenech Provincial Teaching Clinical Surgical Hospital
Discussion
In scientific work carried out on tumor diseases of the duodenum, it is suggested that due to their symptoms they appear around 60 years of age, it is more frequent in male patients (68% to 80%). The duodenal location is not common with a prevalence of 5% in case series of gastrointestinal stromal tumors located specifically in the duodenum, the incidence varies between 6% and 29% due to the absence of early clinical manifestations, these duodenal tumors They appear when they have reached a considerable size that produces symptoms related to the mass effect or digestive bleeding.
They are more frequently asymptomatic and are discovered by chance during endoscopic or radiological studies for other causes [7-10,11,12].
The findings found in the investigation coincide with these authors because the tumors predominated in the group of 61-70 years in both sexes, and only one case of the male sex with a duodenal tumor was found, it is a logical and real fact that this group It is the most prone to this type of disease due to cell degeneration, and sometimes even gastric tumors due to the proximity of these organs can extend to the duodenum.
It is stated that the most frequent affections in the duodenum correspond to: gastroduodenal ulcer, duodenitis and benign tumor lesions. It has been known for years that patients with duodenal ulcer as a group have a basal gastric acid secretion and high stimulation with a longer secretory response to food than healthy individuals.
This hypersecretion of acid has been attributed to an increase in parietal cell mass, vagal hypertonia, increased sensitivity of the parietal cell to secretagogues, or impaired reflex inhibitory gastrin release and acid secretion. In addition, it is stated that according to statistics, the anterior wall of the bulb is the most common location of duodenal ulcer, the reason for this higher frequency is unknown, although some believe that it is because it is the portion that most directly receives the acid content of the duodenal ulcer. stomach as it is more aligned with the antrum [13].
In general, they are found concomitant with gastric and duodenal ulcers, due to the proximity of these portions in each of the organs and the morphophysiological characteristics of the mucosa in said areas, and that is why the so-called radiologically described gastroduodenal ulcers.14 Studies carried out on gastroduodenal stromal tumors suggest that they are rare, with a prevalence of 5 to 7%, however, they represent 30% of all primary duodenal tumors. Most of the publications on these gastroduodenal tumors are case reports or case series. Consequently, the clinical manifestations, study and treatment are matters of controversy [14,15,17,18,19,20].
Gastrointestinal tumors usually show late symptoms, making early treatment difficult. The majority of classical anatomists agree that the most frequent form of the duodenal frame is C, although some describe others, according to the inflections of its four parts, or the absence of any of them, as well as, these include the head of the pancreas and is attached to the posterior abdominal wall. Others describe that the duodenum forms a horseshoe or an incomplete ring that includes above, to the right and below the head and, in part, the body of the pancreas [3,521,22].
All of which coincides with what was reported in the investigation where all the cases studied maintained the four classic portions that are described, perhaps in a larger sample it was possible to find another type of shape or some alteration of the duodenal framework due to manifestations of such a close relationship with the head of the pancreas. In the available literature these are the most frequent forms described. Imaging specialists, when making the radiological report, believe that the thickening or widening of the duodenal wall is due to the relationship that this organ has with the head of the pancreas that displaces it, Prives M et al. [5] describe the close relationship that these organs present that can influence their morphological alterations. Coinciding fact that was found in the investigation where the thickening of the duodenal frame was observed in a patient with a robust physical complexion and the head of the pancreas was attached to the entire frame, widening its walls, also in both cases the shape was horseshoe due to what was previously stated.
Studies carried out on morphological alterations of the walls of this organ suggest that it is important to take into account that histologically, Dieulafoy's lesion is a small submucosal defect with fibrinoid necrosis at its base, which covers a tortuous artery with thick walls due to thickening of the muscularis mucosa and subintimal fibrosis, characterized by the absence of inflammation or ulcers in the surrounding mucosa. It usually presents in adults and is twice as common in men than in women [23-26,27].
Conclusions
At the end of the investigation, a predominance was found in the shape of the letter C as the duodenal frame. When relating these forms with the modifications and clinical entities, the horseshoe presented a greater number. The group from 61 to 70 years predominated at the expense of the male sex. In the study, more than half of the cases did not present clinical-radiological alterations and the frequency of these entities revealed the predominance of duodenal ulcer and widening of the duodenal frame.
References
- Drake RL, Voge AW, Mitchell AWM. Gray's anatomy for students. 2nd Ed. Barcelona: Elsevier; 2010
View at Publisher | View at Google Scholar - Moore KL, Dalley AF, Agur AMR. Abdomen. In: Moore KL, Dalley AF, Agur AMR, Editores. Moore clinically oriented anatomy. 7ed. Philadelphia: Wolters Kluwer/ Lippincott Williams & Wilkins; 2013. p. 181-325.
View at Publisher | View at Google Scholar - Rouvière H, Delmas A. Abdomen. En: Rouvière H, Delmas A. Descriptive, topographic and functional human anatomy. 10 ed. T2. Barcelona: Masson SA; 2002. p.316-379.
View at Publisher | View at Google Scholar - Castillo GL, González AV, Espinosa QD. Morphophysiology. 2nd ed. T 3. Havana: Ecimed; 2018.
View at Publisher | View at Google Scholar - Prives M, Lisenkov N, Bushkovich V. Midgut derivatives. In: Prives M, Lisenkov N, Bushkovich V, editors. Human anatomy. 5 ed. T2. Moscow: Mir; 1989.p.64.
View at Publisher | View at Google Scholar - SadlerTW. langman. Clinically oriented medical embryology. 13. ed. Philadelphia: Wolters Kluwer; 2017.
View at Publisher | View at Google Scholar - Beltran MA. Gastrointestinal stromal tumors (gist) of the duodenum: clinical presentation, diagnostic study, and current treatment.
View at Publisher | View at Google Scholar - Yang F, Jin C, Du Z, Subedi S, Jiang Y, Li J, et al. Duodenal gastrointestinal stromal tumor: Clinicopathological characteristics, surgical outcomes, long term survival and predictors for adverse outcomes. Am J Surg [Internet]. 2013 [cited 13 Nov 2022];206(3):[aprox. 7 p.]. Disponible en:
View at Publisher | View at Google Scholar - García Luna PP, López Gallardo G. Evaluation of intestinal absorption and metabolism. Nutr Hosp [Internet]. May 2007 [cited 13 Nov 2022];22(Suppl 2):[approx. 8 p.].
View at Publisher | View at Google Scholar - Rodriguez Olaso X, Olano Gossweiler C, Lopez Gonzalez V. Use of new endoscopic techniques and procedures in the diagnosis and monitoring of celiac disease.
View at Publisher | View at Google Scholar - Beham A, Schaefer IM, Cameron S, von Hammerstein K, Füzesi L, Ramadori G, et al. Duodenal GIST: a single center experience. Int J Colorectal Dis. 2013 Apr;28(4):581-90.
View at Publisher | View at Google Scholar - Agaimy A, Vassos N, Croner RS. Gastrointestinal manifestations of neurofibromatosis type 1 (Recklinghausen's disease): Clinicopathological spectrum with pathogenetic considerations. Int J Clin Exp Pathol [Internet]. 2012 [cited 13 Nov 2022];5(9):[aprox. 10 p.].
View at Publisher | View at Google Scholar - Hernandez HRG. Diagnostic Upper Digestive Endoscopy Manual.
View at Publisher | View at Google Scholar - Gomez Zuleta MA. Echoendoscopy in the evaluation of duodenal subepithelial lesions. Rev Col Gastroenterol [Internet]. Jun 2015
View at Publisher | View at Google Scholar - Armstrong D, Barkun A, Bridges R, Carter R, de Gara Ch, Dubé C, et al. Canadian Association of Gastroenterology consensus guidelines on safety and quality indicators in endoscopy. Can J Gastroenterol [Internet]. 2012 Jan [cited 13 Nov 2022];26(1):[aprox. 14 p.].
View at Publisher | View at Google Scholar - Buscaglia J, Nagula S, Jayaraman V, Robbins D, et al. Diagnostic yield and safety of jumbo biopsy forceps in patients with subepithelial lesions of the upper and lower GI tract. Gastrointest Endosc [Internet]. 2012 [cited 13 Nov 2022];75:[aprox. 5 p.].
View at Publisher | View at Google Scholar - Larghi A, Fuccio L, Chiarello G, Attili F, Vanella G, Paliani GB, et al. Fine-needle tissue acquisition from subepithelial lesions using a forward -viewing linear echoendoscope: Endoscopy [Internet]. 2014 [cited 13 Dic 2022];46(1): [aprox. 6 p.].
View at Publisher | View at Google Scholar - Hamada T, Yasunaga H, Nakai Y, Isayama H, Horiguchi H, Matsuda S, et al. Rarity of severe bleeding and perforation in endoscopic ultrasound-guided fine needle aspiration for submucosal tumors. Dig Dis Sci [Internet]. 2013 [cited 13 Dic 2022];58(9):[aprox. 4 p.].
View at Publisher | View at Google Scholar - Waisberg J, Joppert Netto G, Vasconcellos C, Sartini GH, Miranda LS, Franco MI. Carcinoid tumor of the duodenum: a rare tumor at an unusual site. Case series from a single institution. Arq Gastroenterol [Internet]. 2013 [cited 13 Dic 2022];50(1):[aprox. 6 p.].
View at Publisher | View at Google Scholar - Utku Yilmaz T, Kozan R. Duodenal and jejunal dieulafoy´s: optimal management. Clin Exp Gastroenterol [Internet]. 2017 [cited 13 Dic 2022];10: [aprox. 8 p.].
View at Publisher | View at Google Scholar - Sinelnikov RD. Atlas de Anatomía Humana. T2. 4 ed. Moscú: Mir; 1979.
View at Publisher | View at Google Scholar - Latour Ramos R. Embriología, anatomía, histología y fisiología del estómago y duodeno. Paniagua Estévez ME, Piñol Jiménez FN. Gastroenterología y hepatología clínica. T.3. La Habana: Ciencias Médicas; 2015.
View at Publisher | View at Google Scholar - Rojas A, Carvajal GD, Prieto RG, Aponte DM. Lesión de Dieulafoy de duodeno: hallazgo inusual. Rev Col Gastroenterol [Internet]. 2016 Sep [cited 13 Dic 2022];31(3):[aprox. 4 p.].
View at Publisher | View at Google Scholar - Córdova H, Sánchez-Montes C, Delgado Guillena PG, Morales VJ, Sendino O, González Suárez B. Quality indicators for esophagogastroduodenoscopy: A comparative study of outcomes after an improvement programme in a tertiary hospital. Gastroenterol Hepatol [Internet]. 2017 Nov [cited 13 Dic 2022];40 (9):[aprox. 7 p.].
View at Publisher | View at Google Scholar - Buils Vilalta F, Martínez Ramos D, Sánchez Cano JJ, Domenech Calvet J, Vives Espelta M, Socías Seco M, et al. Laparoscopic treatment of a patient with perforated jejunal diverticulitis. Andalusian Rev Patol Dig [Internet]. 2013 [cited 13 Dic 2022];36: [aprox. 3 p.].
View at Publisher | View at Google Scholar - Parra Blanco A. Submucosal lesions of the digestive tract. Rev esp enferm dig [Internet]. 2012 Dec [cited 13 Nov 2022];104(11): [approx. 1 p.].
View at Publisher | View at Google Scholar - Mohammed I, Wagholikar GD. Dieulafoy’s lesion of duodenum: a case report. BMC Gastroenterology [Internet]. 2003 [cited 13 Dic 2022];(3):[aprox. 12 p.].
View at Publisher | View at Google Scholar
