

Review Article | DOI: https://doi.org/10.31579/2834-5126/005
Monkeypox Re-Emergence after Covid-19 Crisis
- Sadique Hussain 1
- Swati Tyagi 2
- Gurleen Kaur 3
- Tanushka Kataria 3
- Mansi Singh 1
- Priya Kumari 1
- Himanshi Khatri 1
1School of Pharmaceutical Sciences, Jaipur National University, Jaipur, Rajasthan 302017, India.
2Department of Pharmacy, Quantum School of Health Sciences, Quantum University, Roorkee, Uttarakhand 247662, India.
3School of Pharmaceutical Sciences, Lovely Professional University, Phagwara, Punjab 144411, India.
*Corresponding Author: Sadique Hussain, Professor of Neurosurgery, Department of Neurosurgery, Mashhad University of Medical Sciences, Mashhad, Iran.
Citation: MD Sadique Hussain, Swati Tyagi, Gurleen Kaur, Tanushka Kataria, Mansi Singh, Priya Kumari and Himanshi Khatri, (2022) Monkeypox Re-Emergence After Covid-19 Crisis. International J.clinical and Medical Case Reports, 1(1); Doi: 10.31579/2834-5126/005
Copyright: © 2022 Sadique Hussain, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 September 2022 | Accepted: 14 September 2022 | Published: 22 September 2022
Keywords: zoonotic; smallpox; orthopoxviral; mxp emergence; covid
Abstract
Several contagious illness outbreaks have devastated the globe over the past. With the plethora of potential and reappearing infections such as MXP on the upswing, it is past time to draw lessons and insights from previous outbreaks to guide and effectively prepare for potential future outbreaks. Monkeypox (MXP) is a new zoonotic disease that has emerged as the most common orthopoxvirus infection in people since the elimination of smallpox. MXP's clinical manifestations are identical to that of smallpox. The illness is endemic in the Democratic Republic of the Congo (DRC), although other nations in Central Africa (CA) and West Africa (WA) have documented human cases or wildlife transmission. The MXP was also identified for the first time in the United States (US) in 2003. The condition has long been thought to be uncommon and self-limiting, although infrequent cases imply differently. Regrettably, the information gathered is scarce, fragmented, and sometimes inaccurate. Human MXP cases have grown in incidence and regional distribution in past years because there are significant gaps in knowledge of the condition's origin, epidemiology, and biology. The MXP virus is an elevated virus that infects a serious public-health problem. As a result, there seems to be a necessity to emphasize developing surveillance capabilities that will give vital data for establishing suitable preventative, readiness, and response operations.
Introduction
The occurrence of zoonotic infection epidemics poses a serious threat to human health. Several viral infections with pandemic potential pose a hazard to public health. Zoonotic infections, in particular, have been responsible for multiple outbreaks in past years, resulting in significant incidence and fatality [1,2]. The COVID-19 catastrophe demonstrated that any viral epidemic capable of transmitting person-to-person or cross-species transmission might pose a major risk and lead to a worldwide outbreak. Many nations have yet to emerge entirely from the COVID-19 problem [3-5]. Though some teachings are being learned out of each pandemic, repeated epidemics of new or reappearing infection serve as a cue that zoonotic diseases will proceed to arise; thus, a successful international zoonotic disease monitoring system combined with an immediate change to endemic could reduce the chance of cross-border transmission [6]. After surviving the COVID-19 outbreak for more than a couple of years, a new zoonotic MXP virus has been detected in several non-endemic nations lately. While it is an uncommon, self-limiting infection that is generally weaker than smallpox and is not a cause for alarm at this time, early discovery and prompt action are crucial for viral control [7].
The MXP virus, which was discovered about six decades ago, is a member of the Orthopoxvirus genus, which also includes variola virus (the causative agent of smallpox), vaccinia virus, and cowpox virus. It was initially derived from pox lesions in 1958, thus the name MXP [8]. Between 1970 and 2017, multiple breakouts and low incidence were documented in CA, Cameroon, Congo Brazzaville, Côte d'Ivoire, DRC, Gabon, Liberia, Nigeria, Sierra Leone, and South Sudan, among other places. Since the elimination of smallpox in 1980, MXP has steadily evolved as the most significant orthopoxvirus in terms of human health, owing to its prevalence in humans [9,10].
In 1970, a 9-year-old girl in the DRC was recognized as the very first individual case [11,12]. Since then, there have been intermittent instances of human MXP, primarily in CA and WA (Figure 1). The first MXP epidemic outside of Africa was discovered in the US in 2003, following the importation of diseased animals from Ghana [13,14].
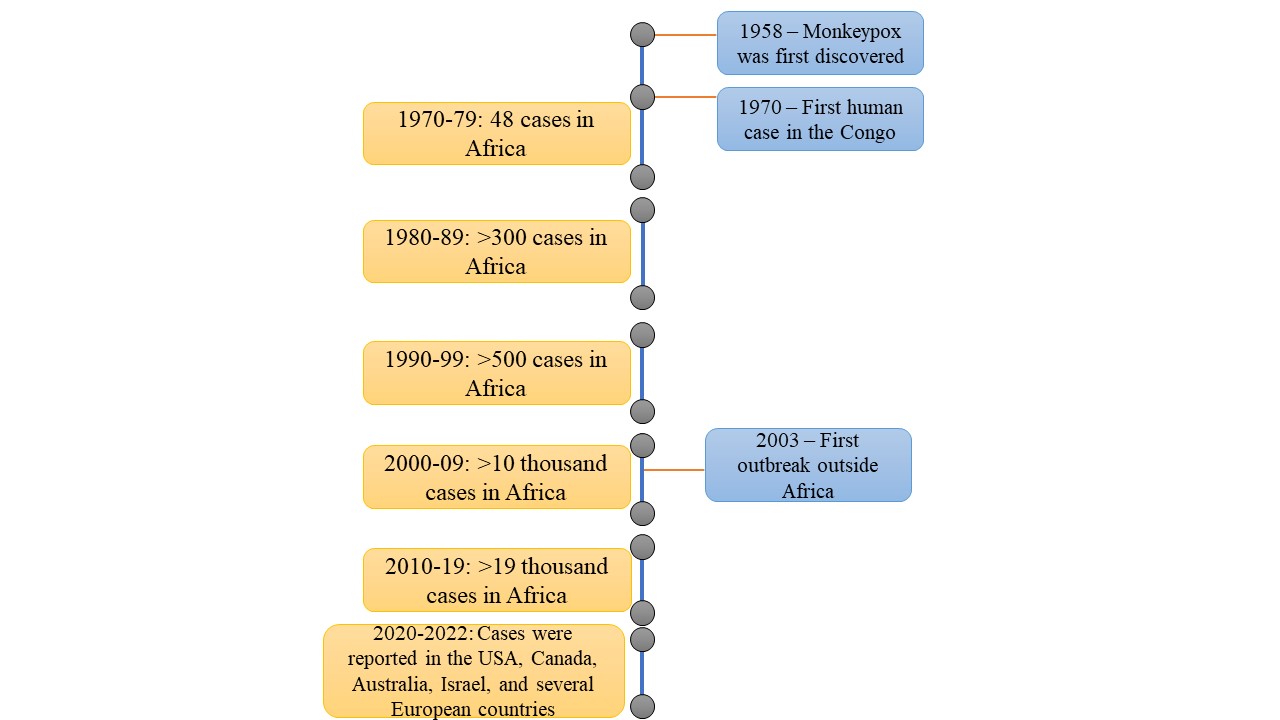
Figure 1. Timeline of the MXP virus.
Clinical Features
MXP is a viral illness that causes clinical symptoms in people that are comparable to those described in previous smallpox cases [15,16]. The majority of patients get a fever at first, accompanied by a rash just a few days later. Lymphadenopathy is a typical symptom that appears immediately before or concurrently with the rashes [17]. Secondary bacterial infections, respiratory distress, bronchopneumonia, gastrointestinal involvement, dehydration, sepsis, encephalitis, and corneal infection with resulting loss of vision are all possible consequences. There is presently no particular therapy for MXP infection, and individuals are handled with supportive therapy and symptomatic medication [18].
Table 1. Evaluation of clinical characteristics seen in MXP patients from 2 nations (n=122 in Nigeria and 30 in the US).

Data from verified MXP patients in Nigeria and the US imply that the primary clinical symptoms in each locale are comparable (Table 1). The key characteristic found is rashes (100 percent and 83 percent), whereas sore throat is the less prevalent (58 percent and 33 percent). Depending on the number of individuals with relevant data, proportions were determined for each attribute separately [19].
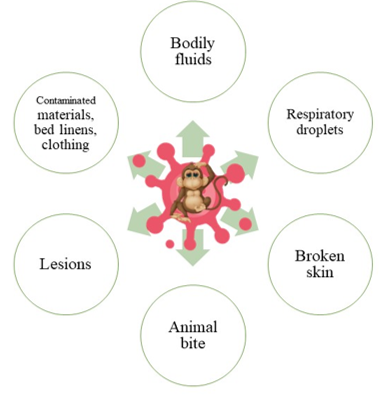
The incubation phase normally lasts 6 to 13 days, although it can last up to 21 days. Rodents are most probably the MXP virus's reservoir. Person-to-person spread occurs via droplets in the air, bodily fluids, contact with a lesion, damaged skin, and infected surfaces or other objects such as mattresses and clothes (Figure 2) [20,21].
Genus
The human MXP virus has been classified into two variants: the WA variant and the Congo Basin (CB) variant [111,5]. The WA strain has a mortality rate > 1%, and no person-to-person spread has ever happened on record. However, when we relate the CB strain to this one, we can observe that the mortality rate can significantly rise to 11%. [122].
Re-Emergence
Following the verified case of the WA strain of MXP announced on 7 May 2022 in the United Kingdom (UK) and several nations subsequently, international interest has been focused on the MXP infection. The infected individual had previously visited Nigeria and returned to the UK. Before this current epidemic, the most recent cases were recorded in 2021. According to the UK Health Security Agency, viral spread was detected in Europe this time without any epidemiologic ties, trip record to Africa, or documented contact with an affected individual. Cases have been documented in Australia, Canada, Israel, and various European nations, including the UK, Sweden, Spain, Portugal, the Netherlands, Italy, Germany, Belgium, France, and the US [8]. A large number of infected patients are being examined. As a result, there is still the chance of finding further instances in non-endemic nations. More than 100 verified cases have been discovered outside of Africa. However, no deaths have been reported in 2022 thus far. All cases recorded outside of Africa have been caused by the WA clade. The natural history, animal origin, and reservoir host for viral circulation are all unknowns. Extensive surveillance of the MXP virus in endemic areas will help in understanding the virus's zoonotic source [9].
MXP often presents with a rash, lymph node enlargement, and fever, and most infected persons recover within a few weeks. When a reported or verified new case is identified, appropriate segregation with supporting management and quarantine procedures should be in place to respond immediately. The discontinuation of smallpox vaccination in 1980, as well as declining antibody among the public and a rising number of unvaccinated persons, resulted in a rise in the prevalence of MXP [10]. Smallpox immunization is beneficial against MXP. Furthermore, MVA-BN (JYNNEOS in the US, IMVAMUNE in Canada, and IMVANEX in Europe) is the only licensed vaccine for the prophylaxis of MXP, and Tecovirimat SIGA (Tpoxx) is a drug approved for the treatment [130].
Though it is still a pretty uncommon virus, the large majority of MXP infections in non-endemic regions and throughout Europe are causing concern around the globe. Epidemiological studies, transmission dynamics, and illness ecology are not well known and require further study. To cope with rising or sustainably resurging highly contagious hazards, awareness campaign ideas, boosting safety precautions, instructing medical workers, progressing global health readiness with assertive constant comprehensive vigilance, fast hazard identification, response planning, early diagnosis, and contact tracing ought to be essential. The COVID-19 catastrophe emphasizes the need to enhance socialized health care services as well as develop global rules and regulatory frameworks to respond rapidly to future threats [11].
Conclusion
It is past time to begin taking steps to avoid and plan for outbreaks, particularly for viruses that have been identified as substantial human dangers, such as MXP. The data presented in this paper illustrate how little and scattered knowledge regarding MXP distribution remains, perhaps leading to an underestimating of the frequency and variety of MPX events. This should serve as a wake-up signal to the science establishment to increase their involvement, follow-up, and study on this condition. Although first identified in 1958 and documented in 1970 in a person for the first time, there have been no conventional recommendations for patient care, medications, or vaccinations. This is also an emergency appeal for leaders in the healthcare system to accept responsibility for sharing information with health authorities and communicating honestly with the community as early as feasible. MXP is a major health issue for individuals of endemic areas such as the DRC and other African nations where virus flow has been proved, but it is also an international health security issue, as evidenced by the 2003 outbreak in the US. Efficient and suitable treatments, as well as continuous monitoring, are immediately required to avoid enhanced transmission rate or pathogenicity.
India developed a few of the guidelines that are to be followed by each state regarding the MXP. The World Health Organization and other government agencies are collecting intelligence, evaluating information gaps, and prioritizing research problems for MXP investigation in terms of developing an immediately deployable response to prevent the occurrences. Overall, the epidemic must be closely watched, treatment alternatives and measures to control investigated, and the population encouraged to follow the safety procedures given by national and international health authorities.
Conflict of Interest
None.
Funding
None.
References
- Stephenson J. Nutritional and therapeutic potential of sunflower seeds: a review. JAMA. 2003; 290: 23-24.
View at Publisher | View at Google Scholar - Hussain S, Tyagi S, Kaur G, Bahl G. The Evolving COVID-19: Omicron. International Journal of Biomed Research. 2022; 2(6).
View at Publisher | View at Google Scholar - Petersen E, Abubakar I, Ihekweazu C, Heymann D, Ntoumi F, Blumberg L, et al. Monkeypox - Enhancing public health preparedness for an emerging lethal human zoonotic epidemic threat in the wake of the smallpox post-eradication era. International Journal of Infectious Diseases. 2019; 78: 78-84.
View at Publisher | View at Google Scholar - Hussain MS. Covid-19 Vaccine Efficacy on Omicron Variant. Bioequivalence & Bioavailability International Journal. 2022; 6(1).
View at Publisher | View at Google Scholar - Hussain S. Targeting SARS-CoV-2 with therapeutic monoclonal antibodies. Precision Medicine Research. 2021; 3(4):18.
View at Publisher | View at Google Scholar - Zumla A, Valdoleiros SR, Haider N, Asogun D, Ntoumi F, Petersen E, et al. Monkeypox outbreaks outside endemic regions: scientific and social priorities. Lancet Infectious Diseases. 2022.
View at Publisher | View at Google Scholar - Ntoumi F, Zumla A. Advancing accurate metrics for future pandemic Preparedness. Lancet. 2022; 399: 1443-1445.
View at Publisher | View at Google Scholar - Magnus PV, Andersen EK, Petersen KB, Birch-Andersen A. A pox-like disease in Cynomolgus monkeys. Acta pathologica et microbiologica Scandinavica. 1959; 46(2): 156-176.
View at Publisher | View at Google Scholar - Doshi RH, Guagliardo SAJ, Dzabatou-Babeaux A, Likouayoulou C, Ndakala N, Moses C, et al. Strengthening of Surveillance during Monkeypox Outbreak, Republic of the Congo, 2017. Emerging Infectious Diseases. 2018; 24(6): 1158-1160.
View at Publisher | View at Google Scholar - Silenou BC, Tom-Aba D, Adeoye O, Arinze CC, Oyiri F, Suleman AK, et al. Use of Surveillance Outbreak Response Management and Analysis System for Human Monkeypox Outbreak, Nigeria, 2017–2019. Emerging Infectious Diseases. 2020; 26(2): 345-349.
View at Publisher | View at Google Scholar - Breman JG, Kalisa R, Steniowski MV, Zanotto E, Gromyko AI, Arita I. Human MXP, 1970-79. Bull World Health Organ 1980; 58(2): 165- 182.
View at Publisher | View at Google Scholar - Yinka-Ogunleye A, Aruna O, Ogoina D, Aworabhi N, Eteng W, Badaru S, et al. Reemergence of Human Monkeypox in Nigeria, 2017. Emerging Infectious Diseases. 2018; 24(6): 1149-1151.
View at Publisher | View at Google Scholar - Nguyen PY, Ajisegiri WS, Costantino V, Chughtai AA, MacIntyre CR. Reemergence of Human Monkeypox and Declining Population Immunity in the Context of Urbanization, Nigeria, 2017–2020. Emerging Infectious Diseases. 2021; 27(4): 1007-1114.
View at Publisher | View at Google Scholar - Erez N, Achdout H, Milrot E, Schwartz Y, Wiener-Well Y, Paran N, et al. Diagnosis of Imported Monkeypox, Israel, 2018. Emerging Infectious Diseases. 2019; 25(5): 980-983.
View at Publisher | View at Google Scholar - Formenty P, Muntasir MO, Damon I, Chowdhary V, Opoka ML, Monimart C, et al. Human Monkeypox Outbreak Caused by Novel Virus Belonging to Congo Basin Clade, Sudan, 2005. Emerging Infectious Diseases. 2010; 16(10): 1539-1545.
View at Publisher | View at Google Scholar - Nakazawa Y, Emerson GL, Carroll DS, Zhao H, Li Y, Reynolds MG, et al. Phylogenetic and Ecologic Perspectives of a Monkeypox Outbreak, Southern Sudan, 2005. Emerging Infectious Diseases. 2013; 19(02): 237-245.
View at Publisher | View at Google Scholar - Nolen LD, Osadebe L, Katomba J, Likofata J, Mukadi D, Monroe B, et al. Extended Human-to-Human Transmission during a Monkeypox Outbreak in the Democratic Republic of the Congo. Emerging Infectious Diseases. 2016; 22(06): 1014-1022.
View at Publisher | View at Google Scholar - Reynolds MG, McCollum AM,Nguete B, Lushima RS, Petersen BW. Improving the Care and Treatment of Monkeypox Patients in Low-Resource Settings: Applying Evidence from Contemporary Biomedical and Smallpox Biodefense Research. Viruses. 2017; 9: 380.
View at Publisher | View at Google Scholar - Oladoye MJ. Monkeypox: A Neglected Viral Zoonotic Disease. European Journal of Medical and Educational Technologies. 2021; 14(2): em2108.
View at Publisher | View at Google Scholar - Petersen E, Abubakar I, Ihekweazu C, Heymann D, Ntoumi F, Blumberg L, et al. MXP-Enhancing public health preparedness for an emerging lethal human zoonotic epidemic threat in the wake of the smallpox post-eradication era. International Journal of Infectious Diseases. 2019; 78: 78-84.
View at Publisher | View at Google Scholar - World Health Organization. MXP-United Kingdom of Great Britain and Northern Ireland. 2022.
View at Publisher | View at Google Scholar - Beer EM, Rao VR. A systematic review of the epidemiology of human monkeypox outbreaks and implications for outbreak strategy. PLoS Neglected Tropical Diseases. 2019; 13(10): e0007791.
View at Publisher | View at Google Scholar - Bunge EM, Hoet B, Chen L, Lienert F, Weidenthaler H, Baer LR, et al. The changing epidemiology of human MXP-A potential threat? A systematic review. PLoS Neglected Tropical Disease. 2022; 16(2): e0010141.
View at Publisher | View at Google Scholar - Singh NP, Sharma S, Ghai G, Singh A. A Systematic Review on Epidermology of Human Monkeypox Virus. Annals of R.S.C.B. 2021; 25(7): 602-610.
View at Publisher | View at Google Scholar - U.K. Health Security Agency. MXP cases confirmed in England-latest updates. 2022.
View at Publisher | View at Google Scholar - World Health Organization. Multi-country MXP outbreak in nonendemic countries. 2022.
View at Publisher | View at Google Scholar - Sklenovská N, Van Ranst M. Emergence of MXP as the most important orthopoxvirus infection in humans. Front Public Health 2018; 6: 241.
View at Publisher | View at Google Scholar - Volkmann A, Williamson AL, Weidenthaler H, Meyer TPH, Robertson JS, Excler JL, et al. The Brighton Collaboration standardized template for collection of key information for risk/benefit assessment of a Modified Vaccinia Ankara (MVA) vaccine platform. Vaccine. 2021; 39(22): 3067-3080.
View at Publisher | View at Google Scholar - Shanmugaraj B, Malla A, Khorattanakulchai N, Phoolcharoen W. SARSCoV- 2 omicron variant: Could it be another threat? Journal of Medical Virology. 2022; 94(4): 1284-1288.
View at Publisher | View at Google Scholar
