

Research Article | DOI: https://doi.org/10.31579/2835-8295/091
Microwave Therpy of the Prostate Gland: an Update
*Corresponding Author: Anthony Kodzo-Grey Venyo, The Petro Mohyla Black Sea State University, Nikolaev, Ukraine,
Citation: Konstantin A. Bugaevsky, (2025), Microwave Therpy of the Prostate Gland: an Update, International Journal of Clinical Reports and Studies, 4(1); DOI:10.31579/2835-8295/091
Copyright: © 2025, Anthony Kodzo-Grey Venyo. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 November 2024 | Accepted: 17 February 2025 | Published: 24 February 2025
Keywords: microwave therapy of prostate gland; microwave ablation of prostate gland; computed tomography scan; magnetic resonance imaging scan; prostate biopsy; targeted therapy; histopathology; serum psa; follow-up assessment; local anaesthesia
Abstract
Disease of the prostate gland whether it is a benign disease or a malignant lesion is relatively common in men who over 50 years of age throughout the world. The anatomical location of the prostate gland enables utilisation of a variety of options of approach to be utilised for the treatment of any localized prostatic affliction with hyperthermia. Intracavitary approaches to the prostate gland are possible via either the rectum or urethra. Furthermore, implants could be inserted into the prostate gland interstitially utilising a perineal approach. Even though the biological rationale for treating malignant tumours with hyperthermia had been well established, recent evidence had indicated that hyperthermia might also be useful in the management of symptomatic benign prostatic hyperplasia. Cancer of the prostate is the second most common tumour in men who are older than 55 years of age and the third leading cause of death in males from cancer. Almost all prostate cancers are adenocarcinoma, which generally tend to be located within the periphery and posterior aspects of the prostate. The prostate is accessible through two intracavitary approaches: hyperthermia applicators may be inserted either through the rectum or through the urethra. Microwave ablation is recognised as one of the thermotherapy heating cancer cells within the human body. Elevating the temperature is iterated to emanate in the damage of tumour cells with cell membrane damage, which, in turn, leads to the destruction of cancer cells. Microwave ablation had been proven to be a safe and effective treatment for kidney cancer; nevertheless, there had been only few case reports regarding utilization of microwave therapy in the treatment of prostate cancer. Some authors had iterated that in 1999, the first report to have documented utilization of percutaneous microwave ablation to treat a case of primary prostate cancer, was published without any treatment-related complications. Subsequently another group of authors had undertaken percutaneous microwave ablation in patients in whom the undertaking of external beam radiotherapy had not been successful. These authors as would be demonstrated in the chapter had pursuant to the microwave ablation of the prostate cancer had reported that the frequency of negative biopsy findings at 24 weeks was 64%. In view of the fact that these previous reports had been documented in the era that preceded the evolved multiparametric MRI scan procedure for the early detection of prostate cancer, effectiveness of microwave ablation for prostate cancer would need to be re-evaluated by utilising recent evolved technology including MRI, serum PSA, and targeted biopsy if indicated. Like the role of microwave therapy for the eradication of cancer of the kidney, some authors had already postulated that technology of microwave could be a suitable option of treatment for the targeting of cancer cells within for localized prostate cancer. Considering that microwave therapy is not available in every health care establishment within the world, it would be envisaged that many clinicians would not be familiar with the use of microwave therapy of the prostate gland in the scenarios of benign prostate hyperplasia, localised prostate cancer and prostatitis. The ensuing chapter has provided a detailed documentation of summations and discussions from some case reports, case series, and studies related to utilisation of microwave ablation of the prostate gland.
Introduction
It has been pointed out that trans-urethral resection of the prostate (TURP) gland has remained the gold standard for the treatment of benign prostatic hyperplasia (BPH) and that generally, while this procedure is safe, patients require a spinal, epidural, or general anaesthesia as well often several days of hospital stay, as well as that the potential morbidity and mortality has tended to limit utilisation of TURP in high-risk patients. [1] It has been iterated that pharmacotherapy had been recommended as a first-line therapy for all patients who have mild to moderate symptoms. [1] Nevertheless, the long-term outcomes are not fully elucidated, and patients need to adhere to a strict medication schedule, and outcome indicators are not reached as well or as reliably as TURP. [1] Despite these inadequacies, many patients are iterated to choose medications over surgery because of the perceived reduced risk of adverse events and the desire to avoid surgery. [1] This trade-off of risk for efficacy is a common thread running through all elective treatments for BPH. [1] Newer modalities of treatment had been aimed at providing alternatives to pharmacotherapy or watchful waiting. [1] Patients are stated to be often enthusiastic if they are offered a one-time method to treat lower urinary tract symptoms secondary to BPH, provided that the method is associated with reduced risk and enables an efficacy equal to that of medical therapy. One such method is iterated to be trans-urethral microwave thermotherapy (TUMT). TUMT entails the insertion of a specially designed urinary catheter with a microwave antenna, which heats the prostate and destroys hyperplastic prostate tissue. TUMT enables the avoidance of general or regional anaesthesia, and results in minimal blood loss and fluid absorption. Clinical trials within the United States of America (U.S.A.) and Europe had demonstrated this mode of treatment to be safe and effective, with excellent symptomatic relief seen in as little as one outpatient setting using only local anaesthesia. Nevertheless, there had been the report of less improvement in urinary functioning that is observed than with TURP patients, and long-term follow-up data had not yet been available. Clinical indications and treatment parameters for TUMT would still continue to evolve as technology advances and more experience is gained. [1]
In the 1980s, utilisation of heat to treat BPH had regained clinical interest as alternatives to TURP and open prostatectomy were being explored. The modern use of microwaves had been accredited to Yerushalami et al. [2]. In 1982, they undertook microwave therapy on a patient who was afflicted by adenocarcinoma of his prostate gland [2] and they subsequently had reported the therapeutic utilisation of microwaves by the trans-rectal route to treat patients with BPH who were poor operative candidates [3].
The first machines to undergo clinical trials utilising hyperthermia had utilised a trans-urethral catheter in a series of ten 1-hour sessions. Software and instrumentation had enabled only a limited and often interrupted delivery of energy to the prostate gland, with intra-prostatic temperatures reaching 40-45ºC. Patients had reported improved symptomatology, likely due to destruction of the alpha-adrenergic nerve fibres around the prostate gland, even though an objective improvement of voiding parameters had not been observed [4], and prostatic cells were reportedly not been destroyed.
To reliably destroy cells, temperatures greater than 45ºC were necessary, which was coined "thermotherapy" [5]. Cells would slough away over a period of weeks to months. [1] Unfortunately, the urethral pain threshold was realized to be 45ºC. [1] The introduction of urethral cooling enabled these higher temperatures to be utilised. Even though heat treatment pattern had differed from device to device, antennae were designed to enable heat to generally follow the anatomical borders of the transition zone. Both objective and subjective measures had produced significant improvement. Nevertheless, patients had invariably had severe prostatic oedema and urinary retention, that necessitated the use of a urinary catheter, which became standard practice after a TUMT. [1]
To improve upon the outcomes of microwave therapy, even further, high-energy thermotherapy was introduced. [1] Temperatures greater than 70ºC were reached, causing thermos-ablation of prostatic tissue. It has been pointed out that these days, many different microwave devices are in use around the world, including the Targis (Urologix, Inc., Minneapolis, Minnesota, USA), Prostatron (Technomed Medical System, Lyons, France), Prostalund (Lund Instruments AB, Lund, Sweden), Prostcare (Bruker Medical, Wissembourg, France), Urowave (Dornier MedTech America, Kennesaw, Georgia, USA), PRIMUS U+R (Tecnomatix, Monheim, Germany), and the LEO Microthermer (Laser Electro Optics, London, UK). [1]
Microwave therapy is used sporadically these days in different departments in various established and well-endowed units to treat various afflictions of the human body. With regard to the prostate gland microwave therapy has tended to be used to treat various afflictions of the prostate gland including: symptoms related to benign prostatic hyperplasia; treatment of localised prostate cancer, and prostatitis. Due to the fact that most Urology Departments in the world do not use microwave to treat afflictions of the prostate gland, it would be envisaged that majority of clinicians all over the world would not be familiar with the use of microwave therapy to treat afflictions of the prostate gland. The ensuing chapter has provided an updated information related to miscellaneous narrations and discussions from some case reports, case series and studies related to microwave therapy of miscellaneous pathologies of the prostate gland.
Aim
To provide an update on microwave therapy of the prostate gland
Methods
Internet databases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Microwave therapy of prostate gland; Microwave therapy of prostate gland. Thirty-five (35) references were identified which used to update the literature in the format of miscellaneous narrations and discussions from some case reports, case series, and studies related to microwave therapy of the prostate gland.
Results
Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, And Studies Related to Microwave Therpy of Prostate Gland
Rubeinstein et al. [1] in 2003, made the ensuing iterations:
- Transurethral resection of the prostate (TURP) gland had remained the gold standard for treatment of benign prostatic hyperplasia (BPH).
- Generally, while TURP procedure is safe, patients do require a spinal, epidural, or general anaesthesia and often several days of hospital stay; the potential morbidity and mortality limits the use of TURP in high-risk patients.
- Pharmacotherapy had been recommended as a first-line treatment option for all patients with mild to moderate symptoms.
- Patients sometimes tend to be often enthusiastic to be offered a one-time method to treat their lower urinary tract symptoms secondary to BPH, provided that the method does provide reduced risk and enables an efficacy that is equal to that of medical treatment.
- One such method is transurethral microwave thermotherapy (TUMT).
- TUMT entails the insertion of a specially designed urinary catheter with a microwave antenna, which heats the prostate and destroys hyperplastic prostate tissue.
- TUMT enables the avoidance of general or regional anaesthesia, and results in minimal blood loss and fluid absorption.
- In this review, they had reflected upon the current indications and outcome of TUMT, including the history of the procedure, the mechanism of action, the indications for TUMT, the pre-operative considerations, the patient selection, the results in terms of efficacy, by comparing TUMT versus. Sham, TUMT versus. Alpha-blocker and TUMT versus. TURP. Based upon their reflections and deliberations of their review of the literature, at the time of publication of their article, they had concluded that TUMT is a safe and effective minimally invasive alternative to treatment of symptomatic BPH.
Yerushalmi et al. [2] reported the following:
- Following extensive experiments on animals, they had concluded a study on the treatment of 15 patients with prostatic carcinoma using localized deep microwave hyperthermia (LDMWH; 2.45 GHZ), either alone or in combination with radiotherapy or hormonal therapy.
- The results of this pilot trial were encouraging and are herewith presented.
Yerushalmi et al. [2] summated the results as follows:
- A total of 146 LDMWH treatments were administered.
- All of the patients had tolerated the treatments well, and there were no complications; the condition of the rectal mucosa was checked routinely by rectoscopy.
- A pronounced and rapid subjective and objective response was recorded in all cases, as noted by reduction in the size of the tumour size, regression of ureteral or urethral obstruction, disappearance of pelvic pain and improvement in well-being.
Yerushalmi et al. [2] made the ensuing conclusions:
- LDMWH was effective by itself and had appeared to potentiate the effects of radiotherapy or hormonal therapy.
- Even though LDMWH had seemed to be a promising and a safe new method of treatment of prostatic cancer, either alone or in combination with other accepted forms of therapy, more controlled studies, which were at the time of publication of their article underway, were needed to draw more definite conclusions.
Yerushalmi et al. [3] reported that non-invasive localized deep microwave hyperthermia was applied as an alternative treatment to surgery in 29 patients with contraindications for prostatectomy. The reported patients were treated twice weekly, on Mondays and Thursdays, for 1 hour, without sedation on an outpatient basis. All of the patients had tolerated the treatment well without secondary effects. Yerushalmi et al. [3] concluded that: The results indicated that localized deep microwave hyperthermia applied by this method is safe and effective in the treatment of benign prostatic hyperplasia.
Sapozink et al. [4] reported a total of 21 patients with biopsy proven benign prostatic hyperplasia had undergone treatment on a pilot protocol involving intracavitary transurethral radiating microwave (630 or 915 MHz.) antenna hyperthermia. Sapozink et al. [4] summated the results as follows:
- Acute and subacute toxicity was mild and had consisted primarily of bladder spasm in 26% of the patients, haematuria in 23% of the patients and dysuria in 9% the patients, none of which had significantly limited the achievement of desired temperatures during the treatment sessions.
- No chronic treatment-related morbidity or mortality was identified.
- Detailed thermal mapping, which was undertaken along the course of the prostatic urethra, had recorded temperatures of 43C or more at greater than 75% of the loci.
- Highly significant increases in urine flow rate, decrease in post-void residual urine capacity and decrease in frequency of nocturia noted.
- A marginally significant decrease in prostate volume was noted and, with a median follow-up assessment of 12.5 months, only 3 patients had required subsequent prostatic resection.
Sapozink et al. [4] made the ensuing conclusions:
- Transurethral hyperthermia represents a safe and promising outpatient approach for the treatment of benign prostatic hyperplasia, particularly for patients who are not candidates for conventional surgical approaches because of medical or personal reasons.
- Further studies with the goal of optimizing the technique appear to be warranted, although long-term results would be best evaluated with prospective phase 3 trials.
Brehmer and Svensson [5] undertook a study to ascertain whether heat, that is used in transurethral microwave thermotherapy (TUMT) for benign prostatic hyperplasia and which causes necrotic lesions within the adenoma, induces apoptosis in benign human prostatic stromal cells. Brehmer and Svensson [5] cultured prostatic stromal cells from benign human prostatic tissue. The origin of the cells was identified by immunohistochemical staining and transmission electron microscopy. The cell cultures were exposed to moderate hyperthermia (47 degrees C) for 1 hour and any apoptosis was detected by light microscopy, transmission electron microscopy and the measurement of induced caspase-3-like activity. Brehmer and Svensson [5] summated the results as follows:
- The cultures contained a mixed population of smooth muscle cells and myofibroblasts.
- Twenty-four hours after heat exposure, 76% of the cells were apoptotic and the caspase activity had increased, whereas only 14% of the cells were necrotic.
Brehmer M, Svensson [5] concluded that:
- Moderate hyperthermia induces apoptosis in cultured human prostatic stromal cells.
Goldfarb et al. [6] in 1995, made the ensuing iterations:
- Thermotherapy of the prostate had proven to be a safe and effective treatment for patients with symptomatic prostatism secondary to BPH.
- Present treatment regimens do yield results and side effects that are intermediate between drug therapy and prostatectomy.
- Future enhancements of the thermotherapy technique would likely be able to improve its results to the level of surgery.
Neĭmark et al. [7] reported the treatment outcomes that were available for 502 patients with benign prostatic hyperplasia who had been exposed to transurethral microwaves (TUMW) on Prostatron unit. They reported that out of the patients whose age had ranged from 55 years to 84 years, 328 had stage I disease, the rest stage II. 32 patients had previously undergone cystostomy. Neĭmark et al. [7] summated the results as follows:
- Acute urine retention was registered in 67 patients on day1 to 4 after the microwave therapy because of oedema of the tumour.
- To remove the urine, cystostomy and catheter were placed in 18 and 49 patients, respectively.
- In half a year a positive effect had occurred in 80% of cases.
Neĭmark et al. [7] concluded that:
- As microwave therapy relieves symptoms, increases the quality of life, improves urine flow and reduces the size of the tumour, it could be recommended for the treatment of benign hyperplasia of the prostate.
Kawamura et al. [8] reported that trans-urethral microwave thermotherapy (TUMT) of the prostate gland was administered to 10 patients with urinary bladder outlet obstruction due to benign prostatic hyperplasia. The mean age of the reported patients was 74.4 years and their ages had ranged between 63 years and to 85 years. The Prostatron device, which provides microwave heating of the prostate and conductive cooling of the urethra was used, and the prostate was heated with a calculated intra-prostatic temperature of 45.5 degrees C for 55 minutes. No anaesthesia was required for most of the patients. Kawamura et al. [8] summated the results as follows:
- The clinical effects were evaluated at 4 weeks to 6 weeks and 3 months after treatment.
- The symptomatic scores had improved in the majority of patients.
- There was no significant change in the volume of the prostate gland.
- The maximum flow rate and average flow rate were increased at 6 weeks and 3 months, but there was no significant change.
- The only side effects were transient haematuria and short-term obstruction secondary to urethral oedema.
Kawamura et al. [8] concluded that:
- In comparing TUMT with the transurethral resection of prostate (TUR-P), the maximum flow rate after TUMT was lower than that after TUR-P and the improvement of residual urine after TUMT was lower than that after TUR-P.
Djavan et al. [9] evaluated the efficacy and safety of a novel intraurethral prostatic bridge catheter in preventing temporary prostatic obstruction following targeted high energy transurethral microwave thermotherapy in patients with benign prostatic hyperplasia. Djavan et al. [9] a total of total of 54 patients who had benign prostatic hyperplasia and who had undergone high energy transurethral microwave therapy under topical urethral anaesthesia which was followed by placement of a prostatic bridge catheter, which had remained indwelling for as long as 1 month that constituted the prostatic bridge catheter group. The patient evaluation included determination of peak urinary flow rate, International Prostate Symptom Score (I-PSS) and quality of life score at baseline, immediately following transurethral microwave therapy and prostatic bridge catheter placement, and periodically thereafter for 1 month. Djavan et al. [9] retrospectively compared the results with those of 51 patients who had undergone transurethral microwave therapy followed by standard temporary urinary catheterization, typically for 24 hours which constituted the standard catheterization group. Djavan et al. [9] summated the results as follows:
- Immediately pursuant to the trans-urethral microwave therapy and prostatic bridge catheter placement significant improvements (p <0>
- In a retrospective comparison at baseline and 14 days between the prostatic bridge catheter group and standard catheterization group the mean baseline peak flow rate, I-PSS and quality of life score were similar. However, at the 14-day follow-up evaluation in the prostatic bridge catheter group the mean peak flow rate was 101.8% higher, and I-PSS and quality of life score were 47.9 and 51.1% lower, respectively, than the corresponding values in the standard catheterization group (p <0>
- The prostatic bridge catheter was well tolerated and had remained indwelling throughout the entire 1-month follow-up in 48 patients out of 54 patients that amounted to in 88.9% of the patients. Early prostatic bridge catheter removal was required in 3 patients that amounted to in 5.6% of the patients due to urinary retention and in 3 patients which amounted to in 5.6% of the patients due to catheter migration.
Djavan et al. [9] made the ensuing conclusions:
- Prostatic bridge catheter placement does provide an effective and well tolerated option for preventing prostatic obstruction in the acute period after transurethral microwave therapy.
- This approach does tend to avoid the inconvenience and infection risk of standard indwelling catheters or intermittent self-catheterization.
- Prostatic bridge catheter insertion and removal are rapid, facile, non-traumatic procedures.
- Prostatic bridge catheter might potentially be used in an array of minimally invasive procedures involving thermal treatment of the prostate gland.
Djavan et al. [10] evaluated the clinical utility of a novel intraurethral prostatic bridge-catheter (PBC) for prevention of temporary prostate obstruction following targeted high-energy transurethral microwave thermotherapy (TUMT) in patients with benign prostatic hyperplasia (BPH). Djavan et al. [10] reported that high-energy TUMT was administered to 54 BPH patients under topical urethral anaesthesia which was ensued placement of a PBC, which had remained in-dwelling up to 1 month. The patient evaluation had included: determination of peak urinary flow rate (Q-max), International Prostate Symptom Score (IPSS), and quality of life (QOL) score at baseline, immediately following TUMT and PBC placement, and at periodic intervals thereafter up to 1 month. The results were compared retrospectively with those of 51 patients who underwent TUMT followed by standard temporary urinary catheterization, generally for 24 hours. Djavan et al. [10] summated the results as follows:
- Immediately pursuant to TUMT and PBC placement significant improvements (p < 0>
- Further improvements were demonstrable up to 1 month, at which time mean the Q-max, IPSS and QOL score had improved 79.0%, 54.9% and 56.5%, respectively, versus baseline means (p < 0>
- In a retrospective comparison at baseline and 14 days between PBC recipients (PBC group) and a cohort of TUMT patients who had undergone temporary standard catheterization and subsequent catheter removal (standard catheterization group), mean baseline Q-max, IPSS and QOL score were similar between the two groups.
- Nevertheless, at the 14-day follow-up evaluation in the PBC group the mean Q-max was 101.8% higher, and IPSS and QOL score were 47.9% and 51.1% lower, respectively, than the corresponding values in the standard catheterization group (p 0.0005).
- The PBC was well tolerated and remained in situ throughout the entire 1-month follow-up period in 48/54 which amounted to in 88.9% of the patients.
- Early PBC removal was undertaken in 3 out of 54 patients which amounted to in 5.6% of the patients because of urinary retention and in 3 out of 54 patients which amounted to in 5.6% of the patients due to PBC migration.
- During the acute post-TUMT recovery period, PBC recipients had experienced impairment in sexual function which, though statistically significant, was comparatively small in magnitude.
Djavan et al. [10] made the ensuing conclusions:
- PBC does provide an efficacious and well-tolerated option for preventing prostatic obstruction in the acute post-TUMT period.
- This approach avoids the inconvenience and infection risk of standard indwelling catheters or intermittent self-catheterization.
- PBC insertion and removal are rapid, facile and non-traumatic.
- PBC placement might prove useful in improving the early results of TUMT.
Djavan et al. [11] made the ensuing iterations:
- The maximal effect of trans-urethral microwave thermotherapy (TUMT) for lower urinary tract symptoms (LUTS) of benign prostatic hyperplasia (BPH) occurs 3 months to 6 months after treatment.
- In the acute period after TUMT, little change in symptoms, quality of life (QOL), and peak urinary flow rate (Q-max) is observed versus baseline.
- Some men may also develop acute urinary retention secondary to thermally induced oedema.
- Recent reports had indicated that early results of TUMT might be improved with concomitant usage of either a temporary intraurethral prostatic bridge-catheter (PBC) or neoadjuvant and adjuvant alpha-blocker therapy.
- Their report had compared the results of these two adjunctive modalities directly.
Djavan et al. [11] undertook a retrospective non-randomized comparison of results in 186 patients with LUTS of BPH which was based upon findings of three recently reported prospective clinical trials. All patients had undergone targeted high-energy TUMT. Ninety-one patients had received no further treatment (TUMT alone group), 54 an indwelling PBC for up to 1 month (TUMT + PBC group), and 41 neoadjuvant and adjuvant tamsulosin (0.4 mg daily) treatment (TUMT + tamsulosin group). The International Prostate Symptom Score (IPSS), QOL score, and Q-max were determined at baseline and 2 weeks after TUMT. Djavan et al. [11] summated the results as follows:
- All three study groups had experienced statistically significant improvements in mean IPSS and QOL score at 2 weeks versus baseline (P <0>
- Nevertheless, the magnitude of improvement was noted to be greater in the TUMT + PBC group than the other two groups and greater in the TUMT + tamsulosin group than the TUMT alone group.
- A high proportion of the TUMT + PBC group that amounted to 87.8% of the patients had attained a 50% or more IPSS improvement, compared with 4.5% of the TUMT alone group and none of the TUMT + tamsulosin group, and a similar pattern of between-group differences was noted with respect to the proportion of patients having 50% or more improvement in QOL score.
- The TUMT + PBC group was the only group to achieve significant Q-max improvement at 2 weeks compared with baseline.
- In the TUMT alone group, urinary retention 1 week or longer in duration had occurred in 10 (11%) of 91 patients compared with 1 (2.4%) of 41 in the TUMT + tamsulosin group and none in the TUMT + PBC group.
- Early PBC removal was required in 11% of the TUMT + PBC group as a consequence of urinary retention secondary to clot formation or PBC migration.
Djavan et al. [11] made the ensuing conclusions:
- Both PBC placement and neo-adjuvant and adjuvant alpha-blocker treatment are effective for alleviating symptoms and improving QOL during the acute period after TUMT.
- PBC usage also had resulted in substantial early Q-max improvement.
- Either of these adjunctive modalities might be appropriate to consider in the treatment of TUMT patients during the early post-procedure recovery period.
Gravas et al. [12] evaluated evaluated the durability of transurethral microwave therapy (TUMT) Prostasoft 3.5 for the treatment of patients with benign prostatic hyperplasia treated with the 30-minute protocol. Gravas et al. [12] reported a total of 213 patients (45 with urinary retention) who were treated with TUMT Prostasoft 3.5. They assessed International Prostate Symptom Score (IPSS), quality of life (QOL) score, and maximal flow rate (Q-max) were assessed at baseline and at 12, 24, 36, 48, and 60 months of follow-up. Gravas et al. [12] summated the results as follows:
- The overall mean follow-up period was 33.9 months, with a maximum of 65 months.
- Patients without retention had significant improvement (P <0>
- The mean IPSS had decreased significantly from 20.3 to 12.2 at 5 years (P <0>
- Similarly, the mean QOL score had improved significantly during follow-up (P <0>
- In the retention group, analysis had shown that the clinical outcomes in terms of Q-max, IPSS, and QOL score remained stable during the follow-up period.
- Retreatment was needed for 48 patients without urinary retention (28.6%) and 17 patients with retention (37.8%).
- The corresponding Kaplan-Meier cumulative retreatment risk at 5 years was estimated to be 42.3% and 58.8%.
Gravas et al. [12] made the ensuing conclusions:
- Their long-term data had suggested that the IPSS and QOL score had remained improved in responders compared with their pretreatment scores 5 years after the 30-minute TUMT protocol and the Q-max had remained significantly increased for up to 4 years.
- Nevertheless. a significant number of patients had required additional treatment, with those in retention before TUMT at a greater risk.
Wagrell et al. [13] compared the outcome of a microwave thermotherapy feedback system that was based upon intraprostatic temperature measurement during treatment (ProstaLund Feedback Treatment or PLFT) with transurethral resection of the prostate (TURP) for clinical benign prostatic hyperplasia (BPH) in a randomized controlled multicenter study. Wagrell also investigated the safety of the two methods. The study was undertaken at 10 centers in Scandinavia and the United States. A total of 154 patients with clinical BPH were randomized to PLFT or TURP (ratio 2:1); 133 of them had completed the study and they were evaluated at the end of the study 12 months after treatment. The outcome measures of the study included the International Prostate Symptom Score (IPSS), urinary flow, detrusor pressure at maximal urinary flow (Q-max), prostate volume, and adverse events. The patients were seen at 3 months, 6 months, and 12 months. Wagrell et defined the responders according to a combination of IPSS and Q-max: IPSS 7 or less, or a minimal 50% gain, and/or Q-max 15 mL/s or greater or a minimal 50% gain. Wagrell et al. [13] summated the results as follows:
- They did not find any significant differences in outcome at 12 months between PLFT and TURP for IPSS, Q-max, or detrusor pressure.
- The prostate volume which was measured with trans-rectal ultrasonography was reduced by 30?ter PLFT and 51?ter TURP.
- Serious adverse events related to the given treatment were reported in 2?ter PLFT and in 17?ter TURP.
- Mild and moderate adverse events were found to be more common in the PLFT group.
- With the aforementioned criteria, 82% and 86% of the patients were characterized as responders after 12 months in the PLFT and TURP groups, respectively.
- The post-treatment catheter time was 3 days in the TURP group and 14 days in the PLFT group.
Wagrell et al. [13] made the ensuing conclusions:
- The outcome of microwave thermotherapy with intraprostatic temperature monitoring was comparable with that seen after TURP in the study.
- From both a simplicity and safety point of view, PLFT appeared to have an advantage.
- Taken together, their findings had enabled them to conclude that within a 1-year perspective microwave thermotherapy with PLFT is an attractive alternative to TURP in the treatment of BPH.
In 2012, Hoffman et al. [14] made the ensuing iterations:
- Trans-urethral resection of the prostate (TURP) gland had been the gold-standard treatment for the alleviation of lower urinary symptoms and improving urinary flow in men who have symptomatic benign prostatic hyperplasia (BPH).
- Nevertheless, the morbidity of TURP has approached 20%, and less invasive techniques had been developed for the treatment of BPH.
- Preliminary data had indicated that microwave thermotherapy, which delivers microwave energy to produce coagulation necrosis in prostatic tissue, is a safe, effective treatment for BPH.
- They had assessed the therapeutic efficacy and safety of microwave thermotherapy techniques for treating men with symptomatic benign prostatic obstruction.
Hoffman et al. [14] undertook randomized controlled trials which were identified from The Cochrane Library, MEDLINE, EMBASE, bibliographies of retrieved articles, reviews, technical reports, and by contacting relevant expert trialists and microwave manufacturers. Hoffman et al. [14] reported that all randomized controlled trials evaluating transurethral microwave thermotherapy (TUMT) for men with symptomatic BPH were eligible for this review and that the comparison groups could include transurethral resection of the prostate gland, minimally invasive prostatectomy techniques, sham thermotherapy procedures, and medications. Hoffman et al. [14] included the outcome measures as: urinary tract symptoms, urinary function, prostate volume, mortality, morbidity, and retreatment. They pointed out that two review authors had independently identified potentially relevant abstracts and then assessed the full papers for inclusion. Hoffman et al. [14] also stated that two review authors had independently abstracted study design, baseline characteristics, and outcomes data and assessed methodological quality using a standard form. Hoffman et al. [14] attempted to obtain missing data from authors or sponsors, or both. Hoffman et al. [14] summated the results as follows:
- They had identified no new randomized comparisons of TUMT that had provided evaluable effectiveness data.
- Fifteen studies that involved 1585 patients had met their inclusion criteria, including: six comparisons of microwave thermotherapy with TURP, eight comparisons with sham thermotherapy procedures, and one comparison with an alpha-blocker.
- The study durations had ranged from 3 months to 60 months.
- The mean age of participants was 66.8 years and the baseline symptom scores and urinary flow rates, which had not differed across the treatment groups, and had demonstrated moderately severe lower urinary tract symptoms.
- The pooled mean urinary symptom scores had reduced by 65% with TUMT and by 77% with TURP.
- The weighted mean difference (WMD) with 95% confidence interval (CI) for the International Prostate Symptom Score (IPSS) was -1.00 (95% CI -2.03 to -0.03), which had favoured TURP.
- The pooled mean peak urinary flow had increased by 70% with TUMT and by 119% with TURP.
- The WMD for peak urinary flow was 5.08 mL/s (95% CI 3.88 to 6.28 mL/s), which had favoured TURP.
- Compared to TURP, TUMT was found to be associated with decreased risks for the development of retrograde ejaculation, treatment for strictures, visible haematuria, blood transfusions, and the transurethral resection syndrome, but had been associated with increased risks for the development of dysuria, urinary retention, and retreatment for BPH symptoms.
- Microwave thermotherapy had improved the IPSS symptom scores (WMD -5.15, 95% CI -4.26 to -6.04) and peak urinary flow (WMD 2.01 mL/s, 95% CI 0.85 to 3.16) compared with sham procedures.
- Microwave thermotherapy had also improved the IPSS symptom scores (WMD -4.20, 95% CI -3.15 to -5.25) and peak urinary flow (WMD 2.30 mL/s, 95% CI 1.47 to 3.13) in the one comparison with alpha-blockers.
- No studies had assessed the effects of symptom duration, patient characteristics, serum prostate-specific antigen levels, or prostate volume on treatment response.
Hoffman et al. [14] made the ensuing conclusions:
- Microwave thermotherapy techniques are effective alternatives to TURP and alpha-blockers for treating symptomatic BPH in men who don’t have any history of urinary retention or previous prostate procedures and prostate volumes between 30 to 100 ml.
- Nevertheless, TURP had provided greater symptom score and urinary flow improvements as well as reduced the need for subsequent BPH treatments compared to TUMT.
- There were small sample sizes and differences in study design limit comparisons between devices with different designs and energy levels.
- The effects of symptom duration, patient characteristics, or prostate volume on treatment response were not known.
Sherar et al. [15] made the ensuing iterations:
- Thermal therapy is used to kill tumours by heating them to temperatures that are higher than 50°C for an extended period of time.
- Cell death emanates from thermal coagulation.
- The energy sources that are available for this approach include radiofrequency electrodes, microwave antennas, laser fiberoptics, and ultrasound transducers.
- Each of these modalities has the potential to be delivered in a minimally invasive manner, and many theoretical and experimental investigations of these devices had been undertaken.
- Their review article had described the current knowledge of interstitial microwave thermal therapy for prostate cancer. Examples had been provided from an ongoing trial in patients who have recurrent or persistent disease following radiotherapy.
- These techniques have the potential to optimize treatments upon a patient-specific basis and would be instrumental in planned future trials of this treatment option as first line for prostate cancer.
Boku et al. [16] examined the safety and efficacy of microwave tissue coagulation (MTC) for prostate cancer and assessed its utilisation in lesion-targeted focal therapy in a non-clinical study and a clinical phase II trial. Boku et al. [16] reported that in the non-clinical study using Microtaze®-AFM-712 (Alfresa Pharma Corporation, Osaka, Japan) with an MTC needle, MTC was undertaken utilising a trans-perineal approach to targeted canine prostatic tissue under real-time ultrasonography guidance. Utilising various MTC output and irradiation time combinations, the targeted and encompassing tissues which included the rectum, urinary bladder and fat, were examined to confirm the extent of coagulative necrosis or potential cell death, and to compare intra-operative ultrasonography and pathology findings. The exploratory clinical trial was undertaken to examine the safety and efficacy of MTC. Five selected patients had undergone trans-perineal MTC to clinically single lesion magnetic resonance imaging (MRI)-visible lesions with Gleason score 3 + 4 or 4 + 4. Boku et al. [16] compared: Prostate-specific antigen (PSA), MRI and Expanded Prostate Cancer Index Composite questionnaire findings were compared before and 6 months after the surgery. Boku et al. [16] summated the results as follows:
- The region of coagulative necrosis was predictable by monitoring of ultrasonically visible vaporization; hence, by placing the MTC needle at a certain distance, they were able to undertake a safe procedure without adverse events affecting the surrounding organs.
- Based upon the non-clinical study, which had used various combinations of output and irradiation time, MTC with 30-W output for 60-s irradiation was selected for the prostate gland.
- Based upon the predictable necrosis, the therapeutic plan (where to place the MTC needle to achieve complete ablation of the target and how many sessions) was strictly determined per patient.
- There were no serious adverse events in any patient and only temporary urinary symptoms related to MTC therapy were identified.
- In addition, post-treatment satisfaction was very high.
- All of the preoperative MRI-visible lesions had disappeared, and serum PSA level had decreased by 55% 6 months pursuant to the surgery.
Boku et al. [16] concluded that:
- Microwave tissue coagulation might be an option for lesion-targeted focal therapy for prostate cancer.
Sterzer et al. [17] in 2000, iterated that TLDR (Too Long, Didn’t Read) had described three novel microwave techniques which had demonstrated promise for being useful for the treatment of diseases of the prostate gland. They are: microwave urethroplasty for providing immediate symptomatic relief of urinary obstructions that are caused by benign prostatic hypertrophy. They stated that TLDR is a technique which utilises microwave balloon catheters for the production of biological stems within the urethra as well as that the initial results that had been obtained in an Federal Drug Administration approved Phase I clinical trial were highly encouraging, hyperthermia produced within the prostate gland by dual microwave balloon catheters-when combined with external beam radiotherapy or implanted radioactive seeds, this technique had the potential of improving local recurrence rates of prostate cancer over the rates that are obtained when only radiotherapy treatments are given, and microwave poration therapy-a treatment that, when combined with either systemic or locally administered chemotherapy, had been demonstrated to be effective in shrinking implanted prostatic tumours in rats.
Kabiri et al. [18] presented a hyperbolic Pennes bioheat equation in cylindrical coordinate for modelling the Microwave Ablation (MWA) that is applied in prostate cancer. Kabiri et al. [18] made the ensuing iterations:
- Due to recent reports, the number of patients of prostate cancer had been growing by 15 million in the world each year.
- Since, it had been demonstrated that the application of uniform microwave within the prostate area of different patients might produce different temperature, the Pennes bioheat equation is considered to study the effect of perfusion term on produced temperature profiles.
- The solution method is Eigen value method which results in a closed form solution.
- The results demonstrated the importance of tissue perfusion term in the estimation of temperature profiles and had established that the thermal tissue damage is expected to initiate from 1 to 3 mm above the catheter surface and to promote up to 7 mm.
- The solutions could be applied as a verification branch for other numerical works and could be very useful to reduce uncertainty about MWA treatments and improve the reliability of clinical protocols giving insight to the Surgeons.
Wu et al. [19] made the ensuing iterations:
- Microwave ablation (MWA) is a type of hyperthermia therapy to cancer disease area.
- Conventional MWA with electromagnetic frequency as 915MHz and 2450MHz had been widely utilized to clinical surgery.
- Nevertheless, higher frequency sources for Industrial, Scientific and Medical (ISM) bands had been available for tumor detection.
Wu et al. [19] evaluated the effect of high frequency microwave (6GHz and 18GHz) applied to liver cancer treatment against conventional microwave (915MHz, 2450MHz) by a finite element model coupled electromagnetic field and bio-heat transfer equation. Wu et al. [19] analyzed tissue damaged region, temperature rise and distribution characteristics in the biological tissue consists of liver and tumor tissue that may represent a realistic situation of cancer treatment. The results had demonstrated that high frequency MWA could cause less collateral damage, more concentrated ablation region and better material response than conventional MWA. Wu et al. [19] concluded that:
- The investigation had indicated that high frequency microwave could be applied to cancer therapy.
Chung et al. [20] made the ensuing iterations:
- Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) causes pain and urinary symptoms which involve the prostate and/or other parts of the male.
- They had analysed the clinical outcomes of medication and microwave thermotherapy.
Chung et al. [20] assigned a total of 132 patients with CP/CPPS for at least 3 months to one of the three study groups (group A: medication; group B: thermotherapy; group C: combination therapy). The NIH-CPSI was recorded at baseline, and at weeks 2 weeks, 4 weeks, 8 weeks, and 12 weeks post-therapy. EPS was evaluated, and semen analysis was undertaken in order to assess the changes in prostatic inflammation. In addition, patient satisfaction questionnaire was completed. Chung et al. [20] summated the results as follows:
- Comparisons between groups A and B, as well as between groups B and C had demonstrated no significant changes in pain, quality of life, and total scores.
- At week 12, group C, when compared with group A, had a significantly improved voiding score (4.19±3.02 vs. 2.71±2.30, p=0.019) and EPS (12.47±15.91 vs. 3.73±4.82, p=0.003).
- At week 4, the patient satisfaction score in group C was significantly different from that in other groups (p=0.043), but there was no difference at week 12 (p>0.05).
- There was no statistically significant difference in laboratory test results, serum PSA levels, and prostate volume between the three groups at baseline and week 12.
- Complications of thermotherapy had resolved with conservative management.
Chung et al. [20] made the ensuing conclusions:
- Their results had demonstrated that a combination of medication and thermotherapy had improved NIH-CPSI and patient satisfaction in CP/CPPS more than medication alone.
- They had suggested that thermotherapy could be another treatment option for CP/CPPS.
Murat et al. [21] presented the findings of a comprehensive study which had explored the synergistic effects arising from the combination of microwave ablation and pulsed electromagnetic field (PEMF) therapy on prostate cancer cells. The research had encompassed five distinct experimental groups, with continuous electric field measurements conducted during the entire treatment process. Group 1 and Group 2, were subjected to microwave power below 350 W, exhibited specific electric field values of 72,800 V/m and 56,600 V/m, respectively. In contrast, Group 3 and Group 4, were exposed to 80 W microwave power, displayed electric field levels of approximately 1450 V/m, while remaining free from any observable electrical discharges. Murat et al. [21] assessed the migratory and invasive capacities of PC3 cells through a scratch test in all groups. Notably, cells in Group 3 and Group 4, were subjected to the combined treatment of microwave ablation and PEMF, had demonstrated significantly accelerated migration in comparison to those in Groups 1 and 2. In addition, Group 5 cells, receiving PEMF treatment in isolation, had exhibited decreased migratory ability. These results had strongly suggested that the combined approach of microwave ablation and PEMF holds promise as a potential therapeutic intervention for prostate cancer, as it effectively reduced cell viability, induced apoptosis, and impeded migration ability in PC3 cells. Moreover, the isolated use of PEMF had demonstrated potential in limiting migratory capacity, which could hold critical implications in the fight against cancer metastasis.
Murat et al. [21] summated their study and the results of the study as follows:
- In the study, a new approach to treat prostate cancer by combining microwave ablation (MWA) and pulsed electromagnetic field (PEMF) therapy was explored.
- They used specific devices like rectangular waveguides for MWA and circular coils for PEMF.
- The energy sources that were used in the study had comprised a magnetron tube system, similar to the microwave source found in a microwave oven, for generating microwaves, and a signal generator for producing PEMF.
- They used specialized equipment for MWA and PEMF to maintain controlled conditions, ensuring precise and reliable results.
- The research had included testing various groups of prostate cancer cells that were exposed to different intensities of microwave power and magnetic flux density.
- The movement of cancer cells in different groups was examined through a wound healing assay, where cancer cells were placed on a flat surface, and they observed whether they filled the gap created by their movement. Interestingly, cells treated with both MWA and PEMF demonstrated faster movement compared to cells treated with MWA alone or PEMF alone. This combined treatment not only effectively decreased cell movement but also had demonstrated the potential cell death.
- The results had shown that the combination of MWA and PEMF had suggested a promising therapeutic strategy.
- The findings had contributed to the development of precise and effective therapies that could enhance patient outcomes and quality of life.
- Nevertheless, further research and validation are essential before translating these findings into clinical applications.
DeSantis et al. [22] evaluated the use of spherical nanocarbon (Grafex) which was injected into known Human Prostatic carcinoma to increase absorption of microwave energy, specifically into tumor cells. DeSantis et al. [22] selected the study to evaluate if nanocarbon and microwave could be used as primary treatment and selected to study heat sink associated with microwave treatment. This specific nanocarbon had demonstrated a range of energy absorption capabilities superior to other non-metallic materials. With regard to the materials and methods, DeSantis et al. [22] reported that 10 Nude nu/nu mice were injected with DU145 (ATC#HTB-81) 1x 10^7 Human Prostate carcinoma cells introduced into the dermis and allowed to grow to more than 1cm. One control mouse had received no treatment. One control mouse received only an injection of nanocarbon. The remaining 8 mice received treatment with the microwave and the nanocarbon. Medwave and BSD magnetron generators with temperature probes were used. Nanocarbon and a viscous carrier were injected into the neoplasms. Short cycle power using 10 watts at 15 seconds used as baseline settings. Target temperature within the tumor was 60 degrees C. DeSantis et al. [22] summated the results as follows:
- The control non treated mouse was euthanized due to metastatic prostate cancer 3 weeks pursuant to the initial injection.
- Seven of the original treated mice had resolved their prostate tumors with no apparent ill effects from the nanocarbon.
- One mouse had a non-treated skin ulcer from the non-cooled microwave probe during the treatment process and was also euthanized; nevertheless, was responding to treatment.
- The one mouse which had received just the nanocarbon treatment, was alive; however, the tumor growth had not reduced in size or advanced in size.
- All of the mice were kept in isolation and were observed to have no side effects from the nanocarbon.
DeSantis et al. [22] made the ensuing conclusions:
- Nanocarbon assisted microwave therapy maximizes energy transfer.
- Conversion of microwave energy does cause thermal ablation to the cancer cells. This does reduce heat sink effect and encompassing tissue damage by utilizing much shorter treatment times and lower power output wattage. This does suggest that Grafex nanocarbon causes enhancement of the dielectric properties of the tumor causing cytotoxic heating.
- Up to time to the time of publication of their article in 2013, there had not been any observed toxic side effects in mice from this small study.
Tan and Wei Phin. [23] made the ensuing iterations:
- Some authors, [16] undertook an animal model study and a phase 2 clinical trial to evaluate the safety and efficacy of focal therapy using microwave tissue coagulation (MTC) to treat prostate cancer.The results had indicated that focal therapy using microwave ablation is relatively safe and might be an option for lesion-targeted therapy for prostate cancer. In a canine prostate model, the authors [16] demonstrated that the thermos-coagulative effect of MTC could successfully cause coagulative necrosis upon histological evaluation of healthy prostate tissue. This was evaluated by removing the prostate and the encompassing tissue from the animal model a few hours ensuing treatment with MTC. The authors. [16] found that the extent of coagulation necrosis and cell death that was produced by MTC was proportional to both the energy output and irradiation time. The authors [16] then demonstrated that intraoperative ultrasonographic measurements were correlated with pathological measurements of the ablated tissue. Even though this study had demonstrated the potential utility of MTC for the treatment of prostate cancer, the study had some notable limitations.
Tan et al. [23] made the ensuing summating iterations:
- First, microwave ablation causes heating by forcing water molecules within the tissues to oscillate out of phase with the applied fields; hence, it had been stated that some of the electromagnetic energy is absorbed and converted to heat. [24]
- Given that prostate cancer presents with an altered glandular structure upon histopathology examination, and studies had revealed that the perfusion of blood to prostate cancer lesions varies between normal prostate parenchyma and cancer, [24] prostate cancer may have higher energy requirements to obtain a similar ablative temperature. In addition, the kill zone of MTC might be smaller than that of the ablated zone on real-time ultrasonographic findings.
- Secondly, in terms of the clinical study, the authors did not undertake prostate biopsies in 3 of the 5 patients. An obvious concern was that residual cancer had remained within the prostate gland after treatment. Even though some clinicians choose to only perform for-cause biopsies after focal therapy, all patients who were enrolled in this trial should have undergone a scheduled prostate biopsy to determine the oncological effect of MTC.
- Thirdly, a recent consensus statement had suggested undertaking prostate biopsy between 6 months and 12 months after focal therapy, as most experts believe that serum prostate-specific antigen testing and magnetic resonance imaging are not sufficient to determine oncological success after ablation. [25]
- Lastly, most pathologists are not likely to encounter specimens obtained immediately after focal therapy, due to the fact that patients are more likely to undergo needle biopsies 6 months to 12 months ensuing focal ablation.
- It is certainly possible that the extent of the ablation zone and the changes from MTC might not be visualized immediately following the ablation.
- Interestingly, biopsies that are obtained up to 8 months after high-intensity focused ultrasound might reveal changes of coagulative necrosis. [26] This finding might be similar in patients undergoing MTC; therefore, longer-term biopsy data is required to ascertain whether histopathology samples could adequately be characterized after MTC.
- Considering that animal model studies are extremely challenging and expensive to undertake, professor Ukimura and his team should be commended for successfully demonstrating that MTC might be a safe and efficacious treatment for prostate cancer
- However, many questions must be answered for trans-perineal microwave ablation of the prostate to be adopted for mainstream usage in clinical care.
Franco et al. [27] made the ensuing statements:
- Trans-urethral resection of the prostate (TURP) had been the gold‐standard treatment for alleviating urinary symptoms and improving urinary flow in men with symptomatic benign prostatic hyperplasia (BPH).
- Nevertheless, the morbidity of TURP approaches 20%, and less invasive techniques had been developed for treating BPH.
- Transurethral microwave thermotherapy (TUMT) is an alternative, minimally‐invasive treatment which delivers microwave energy to produce coagulation necrosis in prostatic tissue.
- They had provided an update pursuant to a review that was last published in 2012.
Franco et al. [27] assessed the effects of transurethral microwave thermotherapy for the treatment of lower urinary tract symptoms in men with benign prostatic hyperplasia. Franco et al. [27] undertook a comprehensive search using multiple databases (the Cochrane Library, MEDLINE, Embase, Scopus, Web of Science, and LILACS), trials registries, other sources of grey literature, and conference proceedings published up to 31 May 2021, with no restrictions by language or publication status. Franco et al. [27] included parallel‐group randomized controlled trials (RCTs) and cluster‐RCTs of participants with BPH who underwent TUMT. Franco et al. [26] reported that with regard to data collection and analysis, two review authors had independently assessed studies for inclusion at each stage and undertook data extraction and risk of bias and GRADE assessments of the certainty of the evidence (CoE). Franco et al. [27] considered review outcomes that were measured up to 12 months after randomization as short‐term and beyond 12 months as long‐term. The main outcomes of Franco et al. [27] included: urological symptoms scores, quality of life, major adverse events, retreatment, and ejaculatory and erectile function. Franco et al. [27] summated the results as follows:
- With regard to the main results, in their update, they had identified no new RCTs, but they had included data from studies that were excluded in the previous version of this review. They had included 16 trials with 1919 participants, with a median age of 69 and moderate lower urinary tract symptoms. The certainty of the evidence for most comparisons was moderate‐to‐low, due to an overall high risk of bias across studies and imprecision (few participants and events).
- With regard to the TUMT versus TURP, based upon data from four studies with 306 participants, when compared to TURP, TUMT probably had resulted in little to no difference in urological symptom scores measured by the International Prostatic Symptom Score (IPSS) on a scale from 0 to 35, with higher scores indicating worse symptoms at short‐term follow‐up (mean difference (MD) 1.00, 95% confidence interval (CI) −0.03 to 2.03; moderate certainty). There is likely to be little to no difference in the quality of life (MD −0.10, 95% CI −0.67 to 0.47; 1 study, 136 participants, moderate certainty). TUMT likely does result in fewer major adverse events (RR 0.20, 95% CI 0.09 to 0.43; 6 studies, 525 participants, moderate certainty); based on 168 cases per 1000 men in the TURP group, this corresponded to 135 fewer (153 to 96 fewer) per 1000 men in the TUMT group. TUMT; nevertheless, probably does result in a large increase in the need for re-treatment (risk ratio (RR) 7.07, 95% CI 1.94 to 25.82; 5 studies, 337 participants, moderate certainty) (usually by repeated TUMT or TURP); based upon zero cases per 1000 men in the TURP group, this corresponded to 90 more (40 to 150 more) per 1000 men in the TUMT group. There might be little to no difference in erectile function between these interventions (RR 0.63, 95% CI 0.24 to 1.63; 5 studies, 337 participants; low certainty). Nevertheless, TUMT might result in fewer cases of ejaculatory dysfunction compared to TURP (RR 0.36, 95% CI 0.24 to 0.53; 4 studies, 241 participants; low certainty).
- With regard to TUMT versus Sham, based upon data from four studies with 483 participants they had found that, when compared to sham, TUMT probably does reduce urological symptom scores utilising the IPSS at short‐term follow‐up (MD −5.40, 95% CI −6.97 to −3.84; moderate certainty). TUMT might cause little to no difference in the quality of life (MD −0.95, 95% CI −1.14 to −0.77; 2 studies, 347 participants; low certainty) as measured by the IPSS quality‐of‐life question on a scale from 0 to 6, with higher scores indicating a worse quality of life. They were very uncertain about the effects upon major adverse events, since most studies had reported no events or isolated lesions of the urinary tract. TUMT might also reduce the need for re-treatment compared to sham (RR 0.27, 95% CI 0.08 to 0.88; 2 studies, 82 participants, low certainty); based upon 194 retreatments per 1000 men in the sham group, this does correspond to 141 fewer (178 to 23 fewer) per 1000 men in the TUMT group. They were very uncertain of the effects on erectile and ejaculatory function (very low certainty), since they found isolated reports of impotence and ejaculatory disorders (anejaculation and hematospermia).
- There were no data available for the comparisons of TUMT versus convective radiofrequency water vapor therapy, prostatic urethral lift, prostatic arterial embolization or temporary implantable nitinol device.
Franco et al. [27] made the ensuing conclusions:
- TUMT does provide a similar reduction in urinary symptoms compared to the standard treatment (TURP), with fewer major adverse events and fewer cases of ejaculatory dysfunction at short‐term follow‐up.
- Nevertheless, TUMT probably results in a large increase in retreatment rates.
- Study limitations and imprecision had reduced the confidence they could place in these results.
- In addition, most studies were undertaken over 20 years ago.
- Given the emergence of newer minimally‐invasive treatments, high‐quality head‐to‐head trials with longer follow‐up are required to clarify their relative effectiveness.
- Patients' values and preferences, their comorbidities and the effects of other available minimally‐invasive procedures, among other factors, could guide clinicians when choosing the optimal treatment for this condition.
Djavan et al. [28] compared directly the efficacy, safety, and durability of targeted transurethral microwave thermotherapy with that of alpha-blocker treatment for lower urinary tract symptoms of benign prostatic hyperplasia. Djavan et al. [28] reported that: In a randomized, controlled clinical trial, 52 patients with lower urinary tract symptoms due to benign prostatic hyperplasia had received terazosin treatment and 51 had undergone microwave treatment under topical anaesthesia. The patient evaluation included the International Prostate Symptom Score, peak flow rate, and quality-of-life score before microwave treatment or initiation of terazosin treatment and at periodic intervals thereafter up to 18 months. Djavan et al. [28] summated the results as follows:
- The mean International Prostate Symptom Score, peak flow rate, and quality-of-life score had all improved significantly in both groups by 6 months.
- Nevertheless, the magnitude of improvement was found to be significantly greater in the microwave group than in the terazosin group.
- The significant between-group differences that were observed at 6 months in the mean International Prostate Symptom Score, peak flow rate, and quality-of-life score were fully maintained at 18 months, at which time the improvements in these three outcome measures were significantly greater (P <0>
- The actuarial rate of treatment failure at 18 months was significantly greater by sevenfold in the terazosin group.
- Adverse events were noted to be generally infrequent and readily manageable in both groups.
Djavan et al. [28] concluded that:
- Even though the initial onset of terazosin action was more rapid, the longer-term clinical outcomes of targeted microwave treatment were markedly superior.
- The more favourable results in patients who had undergone microwave treatment were maintained for at least 18 months.
Wu et al. [29] made the ensuing iterations:
- Radiotherapy (RT) is the primary treatment for prostate cancer (PCa); nevertheless, the emergence of castration-resistant prostate cancer (CRPC) often leads to treatment failure and cancer-related deaths.
- They had undertaken a study to explore utilization of microwave hyperthermia (MW-HT) to sensitize PCa to RT and to investigate the underlying molecular mechanisms.
Wu et al. [29] developed a dedicated MW-HT heating setup, which was created an in vitro and in vivo MW-HT + RT treatment model for CRPC. Wu et al. [29] evaluated PC3 cell proliferation using CCK-8, colony experiments, DAPI staining, comet assay and ROS detection method. Wu et al. [29] also monitored nude mouse models of PCa during treatment, measured tumour weight, and they calculated the tumour inhibition rate. Western blotting was used to detect DNA damage repair protein expression in PC3 cells and transplanted tumours. Wu et al. [29] summated the results as follows:
- Compared to control, PC3 cell survival and clone formation rates had reduced in the RT + MW-HT group, demonstrating significant increase in apoptosis, ROS levels, and DNA damage.
- Lower tumour volumes and weights were identified within the treatment groups.
- Ki-67 expression level was reduced in all treatment groups, with significant decrease in RT + MW-HT groups.
- The most significant apoptosis induction was confirmed in RT + MW-HT group by TUNEL staining.
- Protein expression levels of DNA-PKcs, ATM, ATR, and P53/P21 signalling pathways had significantly decreased in RT + MW-HT groups.
Wu et al. [29] concluded that:
- MW-HT + RT treatment had significantly inhibited DNA damage repair by downregulating DNA-PKcs, ATM, ATR, and P53/P21 signalling pathways, leading to increased ROS levels, aggravate DNA damage, apoptosis, and necrosis in PC3 cells, a well-established model of CRPC.
Liu et al. [30] made the ensuing iterations:
- Lacking a precise targeting strategy, castration-resistant prostate cancer (CRPC) has still been hard to be treat effectively.
- Exploring treatment options that could accurately target CPRC is an important issue with urgent need.
- In their study, a novel nanotechnology-based strategy had been developed for the precise target treatment of CRPC. By combining microwaves and photothermal therapy (PTT), this nanoplatform, cmHSP70-PL-AuNC-DOX, targets tumour tissues with outstanding precision and achieves better anti-tumour activity by contemporaneously eliciting photothermal and chemotherapeutic effects.
- From nanotechnology, cmHSP70-modified and thermo-sensitive liposome-coated AuNC-DOX were prepared and utilised for CRPC-targeted photothermal ablation and chemotherapy. Doxorubicin (DOX) was selected as the chemotherapeutic agent for cytotoxicity. In terms of the curative scheme, prostate tissues were firstly pre-treated with microwaves to induce the expression of heat shock protein 70 (HSP70) and its migration to the cell membrane, which was then targeted by HSP70 antibody (cmHSP70) coated on the nanoparticles to achieve accurate drug delivery. The nanoplatform then achieved precise ablation and controlled release of DOX under external near-infrared (NIR) irradiation.
- Through the implementation, the targeting, cell killing, and safety of this therapeutical strategy had been verified in vivo and in vitro.
- This work had established an accurate, controllable, efficient, non-invasive, and safe treatment platform for targeting CRPC, has provided a rational design for CRPC’s PTT, and offers new prospects for nanomedicines with great precision.
Heo et al. [31] made the ensuing iterations:
- Magnetic hyperthermia (MHT) has emerged as a promising therapeutic approach in the field of radiation oncology because of its superior precision in controlling temperature and managing the heating area compared to conventional hyperthermia.
- Recent studies had proposed solutions to address clinical safety concerns that tend to be associated with MHT, which arise from utilisation of highly concentrated magnetic nanoparticles and the strong magnetic field needed to induce hyperthermic effects.
- Despite these efforts, challenges had remained in the quantification of the treatment outcomes and in the development oof treatment plan systems for combining MHT with radiation therapy (RT).
Heo et al. [31] undertook a study to quantitatively measure the therapeutic effect, including radiation dose enhancement (RDE) in the magnetic hyperthermia-radiation combined therapy (MHRT), using the equivalent radiation dose (EQD) estimation method. Heo et al. [31] undertook the conduction of EQD estimation for MHRT, and they compared the therapeutic effects between the conventional hyperthermia-radiation combined therapy (HTRT) and MHRT in human prostate cancer cell lines, PC3 and LNCaP. Heo et al. [30] adopted a clonogenic assay to validate RDE and the radio-sensitizing effect induced by MHT. Heo et al. [31] analysed the data on survival fractions were using both the linear-quadradic model and Arrhenius model to estimate the biological parameters describing RDE and radio-sensitizing effect of MHRT for both cell lines through maximum likelihood estimation. Based upon these parameters, a new survival fraction model was suggested for EQD estimation of MHRT. Heo et al. [31] summated the results as follows:
- The newly designed model describing the MHRT effect, effectively captures the variations in thermal and radiation dose for both cell lines (R2 > 0.95), and its suitability was confirmed through the normality test of residuals.
- The model had appropriately described the survival fractions up to 10 Gy for PC3 cells and 8 Gy for LNCaP cells under RT-only conditions.
- In addition, utilising the newly defined parameter r, the RDE effect was calculated as 29% in PC3 cells and 23% in LNCaP cells. EQDMHRT calculated through this model was 9.47 Gy for PC3 and 4.71 Gy for LNCaP when given 2 Gy and MHT for 30 min. Compared to EQDHTRT, EQDMHRT showed a 26% increase for PC3 and a 20% increase for LNCaP.
Heo et al. [31] made the ensuing conclusions:
- The proposed model had effectively described the changes of the survival fraction induced by MHRT in both cell lines and had adequately represented actual data values through residual analysis.
- Newly suggested parameter r for RDE effect had demonstrated the potential for quantitative comparisons between HTRT and MHRT, and optimizing therapeutic outcomes in MHRT for prostate cancer.
Zhao et al. [32] made the ensuing iterations:
- Hyperthermia had long been recognized as a modality in anticancer therapy option.
- In their study, they had provided an update on the recent knowledge about the molecular mechanisms of thermal radio-sensitisation on highly invasive NSCLC cells.
Zhao et al. [32] stated that: In a study, they previously undertaken, they had isolated invasive sub-populations of cancer cells from established human non-small cell lung cancer (NSCLC) H460 cell lines. The subpopulation of highly invasive NSCLC cells (H460-INV) had shown cancer cell stemness, increased DNA damage repair. H460-INV cells were exposed to hyperthermia and irradiation. Cell survival was determined by an in vitro clonogenic assay and growth curve for the cells treated with or without hyperthermia. Immunohistochemical staining assay was performed to detect the expression of Ki67、γH2AX foci. Cell apoptosis was performed by Flow cytometry. Cell-scratches and trans-well invasion chamber experiments were undertaken to detect the ability of cell migration and invasion. Western blot assay was used to detect DNA damage repair related molecular changes. Zhao et al. [32] summated the results as follows:
- Hyperthermia could significantly enhance irradiation-killing cells. SER was 1.823.
- Ki67 immunofluorescence results had suggested that thermo-radiation could significantly inhibit cell proliferation (p < 0>
- Flow cytometry results had shown that the apoptotic cells had increased significantly in heat treatment group (p < 0>
- Compared with the control group, H460-INV cell migration and invasion ability had significantly reduced.
- WB results had suggested that thermal downregulated the expression of E cadherin, upregulated N-cadherin.
- Relative persistence of γ-H2A.X nuclear foci in the H460-INV cells after IR treatment was identified, when compared to the no treat H460-INV cells.
- WB results had suggested that thermal combined with radiation had inhibited the DNA repair by inhibiting expression of Ku70 and Ku80.
Zhao et al. [32] made the ensuing conclusion iterations:
- Microwave thermal therapy could increase the sensitivity of highly invasive NSCLC cells to radiation and its mechanism may be related to inhibition of radiation induced DNA damage repair, promoting tumour cell apoptosis, and thermo- radiotherapy can inhibit tumour cell invasion ability.
- The results of their study had suggested a beneficial clinical impact of microwave thermal therapy as a radio-sensitizer for benefiting highly invasive lung cancer patients.
Kigure et al. [33] made the ensuing iterations:
- For many years, transurethral resection of the prostate (TURP) had been the definitive treatment for benign prostatic hyperplasia (BPH).
- Nevertheless, TURP is regarded to be rather invasive because about 20% of the patients develop significant complications within 10 years.
- With the development of microwave technology, minimally invasive procedures had been introduced in an attempt to decrease the morbidity experienced with TURP.
- Various studies that had been reviewed in their reported article had indicated that the outcome of microwave heat therapy for BPH and prostatic cancer is encouraging even though further research is needed to evaluate the long-term effectiveness and safety of this therapy.
- The authors had concluded that, as microwave technologies improve in the near future, increased clinical utilization of this exciting method would be expected.
Herrman et al. [34] made the ensuing iterations:
- Minimally invasive therapies for the treatment of benign prostatic hyperplasia (BPH) compete with the gold standard transurethral resection of the prostate (TURP).
- Comparisons of efficacy and safety had broadened the knowledge of different treatment modalities.
- Concerns of quality of life such as unaltered sexual function as well as cost considerations drive the market to develop techniques of lower-level invasiveness.
- Among the competitors the office based transurethral microwave thermotherapy (TUMT) has provided the broadest scale of scientific data.
- Many manufacturers sell various modifications of this technology. According to different clinical studies TUMT had been proven to be an effective, safe, and durable therapy for the treatment of lower urinary tract symptoms (LUTS) secondary to BPH.
- Nevertheless, TURP still holds the steadier long-term results and is more effective to reduce obstruction as well as other LUTS.
Türk et al. [35] reported an 84-year-old man who had manifested lower urinary tract symptoms (LUTS) related him having urinary bladder outlet obstruction that was attributed to BPH (see figure 1a, and figure 2a). Preceding his manifestation, he had undergone treatment with α-blockers had proven not to be effective. The patient’s advanced age and extensive arteriosclerosis of the anterior division of the internal iliac artery had resulted in the failure of PE conducted within a different medical facility. He had experienced severe symptoms, as was demonstrated by his international prostate symptom score of 28. In addition, he had exhibited a diminished maximum urinary flow rate of 5.1 mL/sec and incomplete urinary bladder emptying, which was demonstrated by his post-micturition residual urine volume of 350 ml. His prostate volume (PV) assessment demonstrated a significant enlargement of his prostate gland, at 218 ml. Elevated total and free serum prostate-specific antigen (PSA) serum levels were noted (total PSA: 14.9 ng/mL, free PSA: 7.78 ng/mL), with a free-to-total PSA ratio of >0.2. His PSA density (total PSA/PV) was calculated as 0.068, which had fallen below the 0.15 limit.
Given the patient’s advanced age, comorbidities (diabetes mellitus, hypertension, coronary artery disease, atrial fibrillation, cerebrovascular disease), and a poor 10-year prognosis, a decision was made to forego a prostate cancer study. With regard to his management, the patient received a 7-day course of cefixime (400 mg/day), Ibuprofen (2 × 600 mg/day), and gastroprotective therapy. Notably, his ablation treatment had commenced 12 hours preceding his scheduled procedure. He was positioned in the dorsal lithotomy posture. With regard to anaesthesia, lidocaine (10 mL) was administered into his prostate/seminal vesicle angle and the bilateral prostate apex. The coaxial needles and microwave antenna were inserted under the guidance of ultrasound scan (Aplio 500, with a 3.5 MHz Convex ultrasound probe; Toshiba, Japan) and computerized tomography (SOMATOM Scope; Siemens AG, Germany). Three 15-G/13.8 cm coaxial needles (TruGuide; Bard, GA, USA) were strategically placed behind his urethra at the midline, right, and left sides of the hypertrophic transitional zone of the prostate (see figure 1b). The exposure energy and duration were calculated utilising liver data, measuring the targeted ablation area around the microwave antenna. The antenna’s tip was positioned at a distance longer than 1 cm from the capsule and longer than 0.5 cm from the rectal wall and the urethra, ensuring the preservation of the rectal wall and the urethra during thermo-ablation. The microwave ablation device, equipped with a 16-G/20-cm microwave ablation antenna (Canyon; Nanjing, China), operated at 2,450 MHz in continuous mode. The midline of the prostate received an exposure power of 20 W for 2 minutes, and the right and left sides had exposure powers of 40 W for 3 minutes and 2 minutes, respectively. In order to monitor the temperature of the periprostatic tissue encompassing the treatment site, two interstitial thermocouple sensors were inserted bilaterally just outside the prostatic capsule, using two 19-G/20-cm microwave ablation temperature probes (Canyon; Nanjing, China). Pursuant to the treatment, he underwent immediate magnetic resonance imaging, followed by assessments at 1- and 3-month intervals. An 18-F urethral catheter, which was inserted prior to his TPMT procedure, was removed 2 weeks subsequently. The safety and efficacy of the technique were assessed via a series of tests that were undertaken before (within 30 days), as well as 1 month and 3 months ensuing the TPMT. The assessments included blood tests, urine culture, complete urinalysis, uroflowmetry, and chest X-rays, as well as comprehensive abdominal, trans-perineal, and transrectal ultrasound scans. These evaluating assessments were repeated at 1 month and 3 months pursuant to his TPMT in order to monitor any changes or developments. The study had obtained informed consent. Türk et al. [35] summated the results as follows:
- The procedure was undertaken as an outpatient procedure in a day hospital.
- The patient did not develop any abdominal discomfort, anorectal pain, or any changes in defecation rhythm pursuant to his TPMT.
- The only transient issue that was encountered was post-operative haematuria, which was promptly addressed by means of saline irrigation within 6 hours and he did not require a blood transfusion.
- His initial post-voided (PV) urine residual volume of 218.8 mL had reduced to 94.1 ml 1 month ensuing his TPMT and further reduction to 80.8 ml was found 3 months after his TMPT.
- His subsequent haematological assessments which were undertaken after his TPMT had consistently demonstrated normal results, while his functional measures had demonstrated improvement.
- His ejaculatory function was not recorded due to the limited sexual activity that the patient had reported. Meanwhile, a significant reduction in the size of his prostate gland gland size was identified (see figure 1c and figure 1, as well as figures 2b, 2c and 2d).
- The patient experienced approximately 3 weeks of dysuria following his TPMT, which necessitated catheterization for 2 weeks post-procedure.
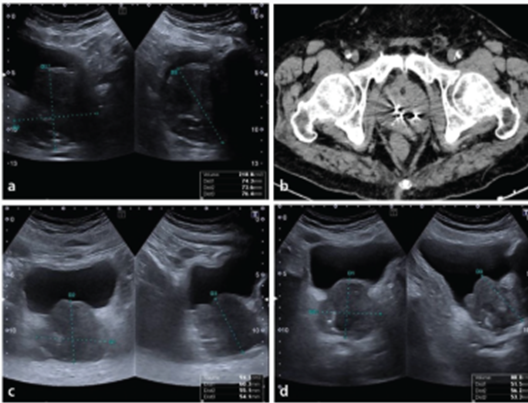
Figure 1. Ultrasound (US) image (a) before Computed Tomography (CT) image (b) during, and US images, (c, d), after interventions. (a) the prostate gland was enlarged as measured on the US image before transperineal prostate microwave thermoablation (TPMT). (b) TPMT was performed under under CT guidance. Three coaxial needles are observable in the image. The prostate gland was reduced in size after (c) 1 month and (d) 3 months post-procedure. Reproduced from [35] under the Creative Commons Attribution License.
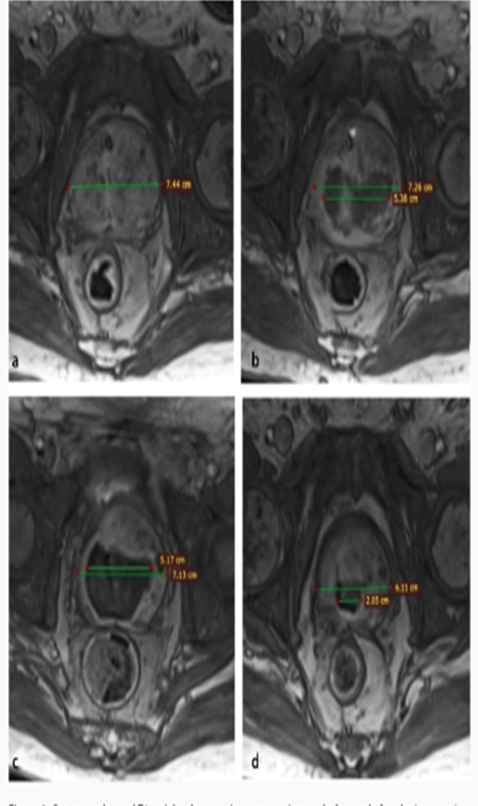
Figure 2. Contrast-enhanced T1-weighted magnetic resonance images before and after intervention. The shrinkage of the prostate gland is observable immediately after transperineal prostate microwave thermoablation (TPMT) (transverse diameter of the prostate and the ablated zone: 7.26 and 5.38 cm), (b), as well as in the follow-up controls 1 month (7.13 and 5.17) (c) and 3 months after TPMT (6.11 and 2.05 cm) (d) in comparison with before
TPMT condition (7.44 and 0.00 cm) (a). Reproduced from [35] under the Creative Commons Attribution License.
Türk et al. [35] made the ensuing conclusions:
- The utilization of interstitial microwave ablation antennas in TPMT appeared to be a promising treatment for LUTS that are caused by BPH.
- However, the need for the undertaking of randomized clinical studies is pivotal to comprehensively assess the effectiveness and practicality of implementing TPMT within clinical settings.
Conclusions And Summations
- Lower urinary tract symptoms (LUTS) are common among men and become more prevalent with the increase of age in men.
- One frequent cause of lower urinary tract obstructing symptoms is benign prostatic obstruction (BPO).
- Patients who have LUTS/BPO could be ameliorated if the obstructive tissue is removed.
- The reference surgical option of treating the obstructed lower urinary tract due to benign prostate hyperplasia is by means of trans-urethral resection of the prostate (TURP) gland, and an outpatient alternative treatment option is to provide transurethral microwave thermotherapy (TUMT).
- Microwave ablation has been reported to have been used in the management of afflictions of the prostate gland including: Benign prostate hyperplasia; localised prostate cancer; and prostatitis. These reported cases are few but generally, most of the procedures had been undertaken under local anaesthesia which means that patients who have co-morbid problems that would prevent them from undergoing general anaesthesia and spinal anaesthesia who need treatment for some of their afflictions of the prostate gland could benefit from undergoing microwave therapy of their prostatic afflictions.
- It does appear that microwave therapy of afflictions of most of the aforementioned afflictions of the prostate does lead to improvement in many of their problems, and the complications of the therapy tend to be less than complications that tend to be associated with prostatectomy; nevertheless, it does appear that the long-term improved results would be inferior to that of prostatectomy and recurrence of the afflictions of the prostate may be more frequent pursuant to microwave ablation of the prostate gland.
- It is pivotal for all clinicians who provide microwave treatment for afflictions of the prostate gland to report the cases they had treated with documentation of long-term follow-up results pursuant to obtaining consent from the patients so that all clinicians throughout the world would update their knowledge about microwave therapy of the prostate gland.
Conflict of interest - none
Acknowledgments
Acknowledgements to:
- Interventional Radiology. Technical Note, and the Turkish Society of Radiology. For granting permission for the reproduction of contents and figures from their journal article under the Creative Commons Attribution License under the ensuing copyright iterations: COPYRIGHT, LICENSE AND OTHER RIGHTS I affirm that this work represents original material, has not been previously published, and is not under consideration for publication elsewhere. By signing this form, authors agree that the article, if accepted for publication by the Journal of Diagnostic and Interventional Radiology, will be licensed under a Creative Commons Attribution-Non-Commercial 4.0 International (CC BY-NC 4.0) which permits third parties to copy, distribute, or reuse the content for non-commercial purposes by giving the appropriate credit to the author and original work. For further details of the license CC BY-NC 4.0, please see https:// creativecommons.org/licenses/by-nc/4.0/. The copyright of the published article belongs to its author under CC BY-NC 4.0 license. The authors agree to transfer the commercial rights to the Turkish Society of Radiology if the article is accepted for publication.
References
- Rubeinstein J N, Kevin T. McVary K T. Transurethral microwave thermotherapy for benign prostatic hyperplasia. Urological Neurology. International Brazilian Journal of Urology. 2003 June; 29(3):
View at Publisher | View at Google Scholar - Yerushalmi A, Servadio C, Leib Z, Fishelovitz Y, Rokowsky E, Stein JA. Local hyperthermia for treatment of carcinoma of the prostate: a preliminary report. Prostate. 1982;3(6):623-30. doi: 10.1002/pros.2990030612. PMID: 7155995.
View at Publisher | View at Google Scholar - Yerushalmi A, Fishelovitz Y, Singer D, Reiner I, Arielly J, Abramovici Y, Catsenelson R, Levy E, Shani A. Localized deep microwave hyperthermia in the treatment of poor operative risk patients with benign prostatic hyperplasia. J Urol. 1985 May;133(5):873-6. doi: 10.1016/s0022-5347(17)49270-6. PMID: 2580997.
View at Publisher | View at Google Scholar - Sapozink MD, Boyd SD, Astrahan MA, Jozsef G, Petrovich Z. Transurethral hyperthermia for benign prostatic hyperplasia: preliminary clinical results. J Urol. 1990 May;143(5):944-9; discussion 949-50. doi: 10.1016/s0022-5347(17)40146-7. PMID: 1691792.
View at Publisher | View at Google Scholar - Brehmer M, Svensson I. Heat-induced apoptosis in human prostatic stromal cells. BJU Int. 2000 Mar;85(4):535-41. doi: 10.1046/j.1464-410x.2000.00473.x. PMID: 10691840.
View at Publisher | View at Google Scholar - Goldfarb B, Bartkiw T, Trachtenberg J. Microwave therapy of benign prostatic hyperplasia. Urol Clin North Am. 1995 May;22(2):431-9. PMID: 7539188.
View at Publisher | View at Google Scholar - Neĭmark AI, Ryzhenkov SV, Sibul' IE. Transuretral'naia mikrovolnovaia termoterapiia dobrokachestvennoĭ giperplazii predstatel'noĭ zhelezy [The transurethral microwave thermotherapy of benign prostatic hyperplasia]. Urol Nefrol (Mosk). 1996 Mar-Apr;2:30-2. Russian. PMID: 8677549.
View at Publisher | View at Google Scholar - Kawamura K, Kikuyama A, Moriyama M, Nakajima C, Shiba N, Kobayashi S, Magome A, Kido C, Miyazawa K, Tanaka T, et al. [Transurethral microwave thermotherapy for benign prostatic hyperplasia]. Hinyokika Kiyo. 1993 Nov;39(11):993-6. Japanese. PMID: 7505524.
View at Publisher | View at Google Scholar - Djavan B, Fakhari M, Shariat S, Ghawidel K, Marberger M. A novel intraurethral prostatic bridge catheter for prevention of temporary prostatic obstruction following high energy transurethral microwave thermotherapy in patients with benign prostatic hyperplasia. J Urol. 1999 Jan;161(1):144-51.
View at Publisher | View at Google Scholar - Djavan B, Seitz C, Fakhari M, Ghawidel K, Marberger M. Prévention de l'obstruction prostatique temporaire après thermothérapie micro-ondes haute énergie par mise en place d'un tuteur prostatique [Prevention of temporary prostatic obstruction after high-energy microwave thermothery by placement of prostatic bridge catheter]. Prog Urol. 1999 Apr;9(2):261-70. French. PMID: 10370950.
View at Publisher | View at Google Scholar - Djavan B, Ghawidel K, Basharkhah A, Hruby S, Bursa B, Marberger M. Temporary intraurethral prostatic bridge-catheter compared with neoadjuvant and adjuvant alpha-blockade to improve early results of high-energy transurethral microwave thermotherapy. Urology. 1999 Jul;54(1):73-80. doi: 10.1016/s0090-4295(99)00029-1. PMID: 10414730.
View at Publisher | View at Google Scholar - Gravas S, Laguna P, Kiemeney LA, de la Rosette JJ. Durability of 30-minute high-energy transurethral microwave therapy for treatment of benign prostatic hyperplasia: a study of 213 patients with and without urinary retention. Urology. 2007 May;69(5):854-8.
View at Publisher | View at Google Scholar - Lennart Wagrell, Sonny Schelin, Jorgen Nordling, Jonas Richthoff, Bo Magnusson, Moddy Schain, Thayne Larson, Emmett Boyle, Jens Duelund, Kurt Kroyer, Håkan Ageheim, Anders Mattiasson. Feedback microwave thermotherapy versus TURP for clinical BPH—a randomized controlled multicenter study. Urology. 2002; 60(2): 292-299. ISSN 0090-4295,
View at Publisher | View at Google Scholar - Hoffman RM, Monga M, Elliott SP, MacDonald R, Langsjoen J, Tacklind J, Wilt TJ. Microwave thermotherapy for benign prostatic hyperplasia. Cochrane Database of Systematic Reviews. 2012(9). Hoffman RM, Monga M, Elliott SP, Macdonald R, Langsjoen J, Tacklind J, Wilt TJ. Microwave thermotherapy for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2012 Sep 12;(9):CD004135. doi: 10.1002/14651858.CD004135.pub3. Update in: Cochrane Database Syst Rev. 2021 Jun 28;6:CD004135.
View at Publisher | View at Google Scholar - Sherar MD, Trachtenberg J, Davidson SR, McCann C, Yue CK, Haider MA, Gertner MR. Interstitial microwave thermal therapy for prostate cancer. Journal of endourology. 2003 Oct 1;17(8):617-25.
View at Publisher | View at Google Scholar - Boku H, Kaneko M, Yamada Y, Morinaga Y, Konishi E, Uno A, Ito‐Ihara T, Yamada A, Horiguchi G, Teramukai S, Fujihara A. Microwave focal therapy of prostate cancer: a non‐clinical study and exploratory clinical trial. BJU international. 2022 Dec;130(6):776-85.
View at Publisher | View at Google Scholar - Sterzer F, Mendecki J, Mawhinney DD, Friedenthal E, Melman A. Microwave treatments for prostate disease. IEEE Transactions on Microwave Theory and Techniques. 2000 Nov;48(11):1885-91.
View at Publisher | View at Google Scholar - Kabiri A, Talaee MR. Theoretical investigation of thermal wave model of microwave ablation applied in prostate Cancer therapy. Heat and Mass Transfer. 2019 Aug 1; 55:2199-208.
View at Publisher | View at Google Scholar - Wu X, Liu B, Xu B. Theoretical evaluation of high frequency microwave ablation applied in cancer therapy, Applied Thermal Engineering. 2016; 107: 501-507. ISSN 1359-4311,
View at Publisher | View at Google Scholar - Chung H, Choi H, Yoo TK, Cho JM, Kim HS. The effects of microwave thermotherapy for chronic prostatitis/chronic pelvic pain syndrome: a prospective, randomized study. Urogenital Tract Infection. 2017 Apr 30;12(1):35-41.
View at Publisher | View at Google Scholar - Murat C, Kaya A, Kaya D, Erdoğan MA. Experimental study for in vitro prostate cancer treatment with microwave ablation and pulsed electromagnetic field. Electromagnetic Biology and Medicine. 2024 May; 20:1-0.
View at Publisher | View at Google Scholar - DeSantis M, Bowne W, Ferretti J A, Dalessandro T, Kumar A, Sclafani S J, Dolan C E. Abstract No. 263 - In situ nanocarbon assisted microwave therapy (NAMT) for application of targeting human prostate tumor cells in nude mice causing cytotoxic thermal ablation using extremely short cycle microwave energy as primary therapy, Journal of Vascular and Interventional Radiology. 2013; 24(4): Supplement, S116-S117, ISSN 1051-0443,
View at Publisher | View at Google Scholar - Tan, Wei Phin. Re: Microwave focal therapy of prostate cancer: A non-clinical study and exploratory clinical trial. Current Urology. September 23; 17(3): 173.
View at Publisher | View at Google Scholar - Esen M, Onur MR, Akpolat N, Orhan I, Kocakoc E. Utility of ADC measurement on diffusion-weighted MRI in differentiation of prostate cancer, normal prostate and prostatitis. Quant Imaging Med Surg. 2013 Aug;3(4):210-6.
View at Publisher | View at Google Scholar - Lebastchi AH, George AK, Polascik TJ, Coleman J, de la Rosette J, Turkbey B, Wood BJ, Gorin MA, Sidana A, Ghai S, Tay KJ. Standardized nomenclature and surveillance methodologies after focal therapy and partial gland ablation for localized prostate cancer: an international multidisciplinary consensus. European urology. 2020 Sep 1;78(3):371-8.
View at Publisher | View at Google Scholar - Evans A J. Treatment effects in prostate cancer. Mod Pathol. 2018 Jan;31(S1):S110-121.
View at Publisher | View at Google Scholar - Franco J V, Garegnani L, Liquitay CM, Borofsky M, Dahm P. Transurethral microwave thermotherapy for the treatment of lower urinary tract symptoms in men with benign prostatic hyperplasia. Cochrane Database of Systematic Reviews. 2021(6).
View at Publisher | View at Google Scholar - Djavan B, Seitz C, Roehrborn CG, Remzi M, Fakhari M, Waldert M, Basharkhah A, Planz B, Harik M, Marberger M. Targeted transurethral microwave thermotherapy versus alpha-blockade in benign prostatic hyperplasia: outcomes at 18 months. Urology. 2001 Jan 1;57(1):66-70.
View at Publisher | View at Google Scholar - Wu Y, Liu P, Chen W, Bai S, Chen S, Chen J, Xu X, Xia J, Wu Y, Lai J, Sun C. Microwave hyperthermia enhances radiosensitization by decreasing DNA repair efficiency and inducing oxidative stress in PC3 prostatic adenocarcinoma cells. International Journal of Hyperthermia. 2024 Dec 31;41(1):2335201.
View at Publisher | View at Google Scholar - Liu P, Wu Y, Xu, X. Fan X, Sun C, Chen X, Xia J, Bai S, Qu L, Lu H, Wu J, Chen J, Pian J-G, Wu Z. Microwave triggered multifunctional nanoplatform for targeted photothermal-chemotherapy in castration-resistant prostate cancer. Nano Res. 2023; 16, 9688–9700.
View at Publisher | View at Google Scholar - Heo D, Lokeshwar B L, Barrett J T, Mostafaei F, Kwon S-H, Huh C. Quantitative analysis of radiosensitizing effect for magnetic hyperthermia-radiation combined therapy on prostate cancer cells. Medical Physics. International Journal of Medical Physics Research and Practice. 2024 October; 51(10): 7606 – 7618. First published: 25 June 2024.
View at Publisher | View at Google Scholar - Zhao Y, Zhang S, Wu Z, Zhang J, Zhu L, Xu Y. Microwave Thermal Therapy Enhances Radiosensitivity of Highly Invasive Human Non-Small Cell Lung. The Journal of Thoracic Oncology. 2017 January; 12(1): Suplement. S1048. P2. 05-029
View at Publisher | View at Google Scholar - Kigure T, Nakata K, Yuri Y, Harada T, Miyagata S, Fujieda N, Koh D, Etori K. Microwave thermal therapy in the treatment of benign prostatic hyperplasia and prostatic cancer. Journal of Microwave Surgery. 2012; 30:239-45.
View at Publisher | View at Google Scholar - Herrman TR, Gross AJ, Schultheiss D, Kaufmann PM, Jonas U, Burchardt M. Transurethral microwave thermotherapy for the treatment of BPH: still a challenger? World journal of urology. 2006 Sep;24: 389-96.
View at Publisher | View at Google Scholar - Türk Y, Devecioğlu I, Çilesiz N S, Çilesiz B. Transperineal microwave thermoablation for benign prostatic hyperplasia-related lower urinary tract symptoms in an elderly patient. Interventional Radiology. Technical Note. 2024 02 10;
View at Publisher | View at Google Scholar
