

Case Report | DOI: https://doi.org/10.31579/2835-8295/159
Measuring and Managing Multifaceted Obesity- A Challenge!
*Corresponding Author: Suresh Kishanrao, Family Physician & Public Health Consultant, Bengaluru.
Citation: Suresh. K, (2026), Measuring and Managing Multifaceted Obesity- A Challenge! International Journal of Clinical Reports and Studies, 5(3); DOI:10.31579/2835-8295/159
Copyright: © 2026, Suresh. K. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 March 2026 | Accepted: 20 April 2026 | Published: 04 May 2026
Keywords: porencephaly; cystic encephalomalacia; arachnoid cyst; cerebral palsy; perinatal brain injury; mri pitfall
Abstract
Obesity is a growing public health problem as it leads to chronic diseases like metabolic syndrome, diabetes mellitus, cardiovascular disease, hypertension, non-alcoholic fatty liver disease, cancers, depression, and stroke. Early diagnosis is crucial to lowering the risk of these complications. Given its multifactorial causes and various measurement tools identifying Obesity in early stages and starting interventions is delayed. Obesity must be treated as a medical condition and professional help sought. Obesity is commonly defined as having too much body fat. Obesity is classified by BMI, fat distribution (apple vs. Pear), based on underlying causes- a) Primary/ Genetic, b) Secondary, c) Sarcopenic (muscle loss), and distribution-based types like Central & Peripheral. The major risk factors responsible for lifestyle diseases are obesity, physical activity, tobacco smoking, alcohol consumption, and mental stress. Recent observations have shown that increased mental stress and activation of the physiologic stress response from chronic exposure to stressors, low socioeconomic status (SES), severe mental health problems, or aggressive behaviour increases the risk of lifestyle diseases.
Materials and Methods: This article is based on 5 anecdote cases managed in different ways both by primary care physician and tertiary care hospitals. Based authors experience and literature search an attempt is made to collate existing guidelines to help family physicians or general practitioners to motivate and mobilize their obese clients for taking the first step toward long term health benefits and life free from all guilt and stigma on 4th March the World Obesity Day 2026.
Outcomes: Non pharmacotherapy (diet, sleep, exercise, stress reducing methods like meditation), Pharmacotherapy (GLP1 and GLP-1RA) and most effective treatment of integrated therapy both allopathic and Ayurvedic systems have shown success, if appropriate individualized treatment plan is made and individual make sustained efforts.
Keywords & Abbreviations: BMI= body mass index, CVD= cardiovascular disease, ICMR= Indian Council of Medical Research, NCDs= non‐communicable diseases, NP‐NCD= National Programme for Prevention and Control of Non‐Communicable Diseases, PCP= primary care physician, T2D= type 2 diabetes, WC= waist circumference, NC= Neck Circumference, HC= Hip circumference, WHR= Waist–hip ratio, BFA= Body fat percentage
Introduction
Obesity is a growing public health problem as it leads to chronic diseases like metabolic syndrome, diabetes mellitus, cardiovascular disease, hypertension, non-alcoholic fatty liver disease, cancers, depression, and stroke. Early diagnosis is crucial to lowering the risk of these complications. Given its multifactorial causes and various measurement tools identifying Obesity in early stages and starting interventions is delayed. Obesity must be treated as a medical condition and professional help sought [1,2]. Obesity is commonly defined as having too much body fat. Obesity is generally classified by BMI into Class lass 1 Obesity = BMI 30 to 35 kg/m2, Class 2 Obesity = BMI 35 to 40 kg/m2 and Class 3 Obesity = BMI 40 kg/m2 and above. Other key types are based i) on fat distribution (central/apple vs. peripheral/pear) ii) based on underlying causes- a) Primary/ Genetic, b) Secondary (due to other conditions), c) Sarcopenic (muscle loss), and iii) distribution-based types like Central (abdominal) & Peripheral (hips/thighs) [3].
Generally, people start blaming the overweight or obese individual for not willing or putting enough efforts to reduce weight. But it is not just a failure of willpower, it is a chronic biological condition shaped by genetics, environmental and behavioural factors. Blaming never helps but understanding always does! Knowing the various causes of obesity and benefits of weight reduction will motivate obese people to make all out efforts. Here is the hint of the weight reduction proportion & accruing benefits: Weight reduction up to 1- 5% improves hypertension and blood sugar levels. A reduction of 5-10% helps prevent T2D, PCOS, reduce dyslipidaemia,10-15% reduction leads to lower the risk of CVD, OSA, and Knee arthritis, and more than 15% weight loss reduces biomarkers like blood sugar levels, Triglycerides, BP and HbA1c to prediabetes levels [4]
Current strategies for management of obesity and lifestyle diseases in India include i) Change the narrative: as obesity is a complex, chronic disease, impacting multiple aspects of daily life to be addressed before complications or comorbidities arise, ii) Move from a disease oriented approach to a health‐focused approach to reduce disparities in prevention & management, iii) Invest in healthcare systems & the capacity to improve management & prevention and iv) Initiate, augment & scale the support by the healthcare system to people living with obesity v) Policy change is needed in India to ensure that obesity is adequately managed, to improve health of the overall population and reduce disease burden and healthcare costs [4,5].
Obesity Day which aims creating an Awareness & Prevention plan. Launched on 11 October 2015, it was moved to March 4 each year in 2020. This article is an attempt to collate existing guidelines to help family physicians or general practitioners to motivate and mobilize their obese clients for taking the first step toward long term health benefits and life free from all guilt and stigma on 4th March 2026 World Obesity Day 2026.
Case Reports:
Case 1. A female bank manager aged 45 years presented with a 5-year history of obesity, Knee joint pian, and hypertension to a public sector Ayurvedic tertiary care hospital in May 2025. She was diagnosed as " Sthoulya (Obese) in Ayurveda. History revealed constant work pressure of accounting, sedentary work involved sitting for hours. She hardly tried to walk or exercise due to dual responsibility of home management, taking care of 2 adolescent children and office work and high-calorie diets. The case was attributed to Ati Ahara Sevana (excess food intake), Avyayama (lack of physical exercise), and Beejadosha (genetics).
Management: The patient underwent a comprehensive treatment plan focusing on reducing fat tissue (Medodhatu), comprising: i) Udwartana: Dry powder massage to reduce cellulite and stimulate fat burning ii) Bashpa Sweda: Therapeutic sweating iii) Sadyo Virechana- Prompt purgation iv) Shamana Aushadhis: Ayurvedic medicine to manage body metabolism v) Lifestyle change Inclusion of yoga and dynamic exercises.
Outcome: Significant reduction in BMI, weight, and improved serum lipid profiles within 20 days. Ayurvedic management, highlights a successful reduction in weight, BMI, and improved lipid profiles over 20 days using Apatarpan chikitsa (Self- commitment- including Udwartana, Bashpa sweda), diet modification, and exercise.
Case 2.A combined non-pharmacotherapy success: A 58-year-old rural woman with chronic obesity and metabolic issues demonstrated successful weight management through a combination of diet, counselling, and increased physical activity, leading to a 7% reduction in body weight in about 6 months
Case 3: Single patient’s obesity pharmacological intervention: An obese male of 56 years old sedentary businessman with a weight of 120 Kg, BMI >40 kg/m² with co-morbidities like hypertension, diabetes, and dyslipidaemia. He was put on a combination of lifestyle counselling for dietary modification by including lots of papaya and other fruits, green leafy vegetables and eggs to the tune of 50% of the volume in each of 3 meals in, exercise in terms brisk walking, weightlifting and yoga asana and pharmacological intervention. Pharmacotherapy included Semaglutides (GLP-1) namely- i) Liraglutide (GLP-1): A 3.0 mg daily dose for 6 months, when resulted in a 7.1% body weight reduction. ii) Orlistat: A 120 mg capsule, 3 times a day with fat-containing meals, to address comorbidities like Type-2 diabetes, another 5% kg adding to a total of 12.5% weight loss in 6 months.
While GLP-1 was Highly efficient in appetite regulation in significant reduction in food intake and Orlistat and GLP-1 analogy, has demonstrated improvements in, or reversal of, metabolic syndrome components prevalent in India, including high blood pressure, abdominal obesity, and insulin resistance. This Success is attributed to Long-term Commitment, with high adherence to both medication and lifestyle changes. The case was regularly monitored for GI side effects, acute hepatotoxicity as they are known adverse effects in some case
Case 4: Beer Belly of 5 Friends: Five young software professionals (aged 28-35, unmarried) approached this author in Mid 2025 with a complaint of a protruding belly, hard, to shed and seeking help as they were finding it difficult to find alliances. A detailed history revealed that they were consuming draft beer almost every day after the end of a hectic day, sometime as late as midnight with some snacks. Their work pressure and late-night hitting bed had restricted their sleep to 6hrs. All other systemic examination revealed no significant clinical findings except their abdominal girth ranges from 100-120 cm. This author counselled them giving the technical details of Beer and snack consumption which is caused an accumulation of fat in the abdominal area. Beer belly is common in men and is characterised by excessive beer consumption; and other factors like diet, lifestyle, hormones, and other alcoholic beverages that are determinants for pot belly formation. As alcohol is notorious for disrupting fat metabolism, especially in the abdominal area. Alcohol contains empty calories that have no nutritional value, which add to the weight gain. Excessive drinking should be avoided, as there is health risks associated with drinking beer. The were explained about an unhealthy diet alongside alcohol contributed significantly to the formation of central beauty or pot belly. Consuming a diet that is excessive in calories can lead to abdominal fat accumulation. Other behaviours like late-night eating can disrupt the digestive system and encourage fat storage. Furthermore, skipping meals was not advised as it causes people to overeat to compensate for the meals they missed. A sedentary lifestyle also contributed to the accumulation of fat in the stomach area, as physical exercises are crucial for burning calories. Therefore, they were advised to avoid spending too much time sitting and not engaging in any physical activities. They were asked to take up physical activities such as jogging, walking, running, and weights or stretch bands to strengthen muscles which encourages reduced calorie expenditure as they help to burn calories all over the body.
Though the appearance of a beer belly was their key cosmetic concern, but it was impressed that is a clear indicator of an increased risk of various health problems like digestive problems, liver diseases, high blood pressure, and so many more. In the last 7 months all of them have reduced about 10-12% of their weight and waist circumference by 5-10 CM.
Case 6 hypothalamic obesity (HO): A 24-year-old male approached the author in January 2025 with the complaints of a significant weight gain of 40 Kg in 6 months after a brain’s surgery. The discharge notes from a private cancer hospital showed the condition as craniopharyngioma, and the surgery was done about 8 months ago, with no post-operative complications. Initial weight gain made the family and the adult happy for first 3 months. But when it started increasing rapidly, they tried limiting foot and proteins prescribed. The case was referred to the same hospital who put him on semaglutide 2.4 mg subcutaneous injection on Weekly. He lost a total weight of >30 kg, with marked improvement in metabolic parameters and reversal of rapid weight gain. Because HO involves damage to the brain's satiety centre in hypothalamus. GLP-1RAs works by acting on alternative satiety-related sites in the hindbrain, such as the nucleus of the solitary tract and area postrema.
Discussions:
Obesity is a chronic and complex disease that can affect our overall health and quality of life. Obesity can lead to serious medical conditions. It can affect your self-esteem and mental health. It’s a common condition especially among urban middle-aged adults especially in well to do families starting as early as childhood.
By 2025, the global overweight and obesity burden is projected to reach approximately 2.7 billion adults affected. Obesity prevalence is expected to reach 18% in men and over 21% in women. Over 1 billion people are now living with obesity, marking a massive surge in prevalence and health-related costs [1]. According to World Obesity Atlas 2026, nearly 14.9 million Indian children aged 5–9 years and over 26.4 million adolescents aged 10–19 was living with overweight or obesity in 2025. India ranks second only to China in total numbers, with 41 million schoolchildren (5–19 years) living with high BMI and 14 million living with obesity alone. According to UNICEF’s Child Nutrition Global Report 2025, obesity (9.4%) has, for the first time, surpassed underweight (9.2%) globally as the most common form of Malnutrition among school-aged children and adolescents. Today, one in ten children worldwide, nearly 188 million, live with obesity [2]. Once considered a condition of affluence, obesity is now spreading rapidly in low and middle-income countries.
WHO defines overweight and obesity as i) For adults: a) overweight is a BMI greater than or equal to 25; and b) obesity is a BMI greater than or equal to 30 ii) For Children: Age needs to be considered when defining overweight and obesity a) Children aged between 5–19 years- overweight is BMI-for-age greater than 1 standard deviation above and obesity is greater than 2 standard deviations above the WHO Growth Reference median. WHO growth reference for children aged between 5–19 years has 2 components- a) Children under 5 years of age b) For children under 5 years of age. Overweight is weight-for-height greater than 2 standard deviations above; and Obesity is weight-for-height greater than 3 standard deviations above the WHO Child Growth Standards median
Everybody knows and most doctors advise diet and exercise for weight loss. But biology often pushes people with obesity back to their starting point. The weight regain cycle will be exhausting. It’s not about weakness, lack of motivation or will-power, but it’s about our own biology fighting against us. Quality of weight loss -more fat loss and not muscle loss matters for lifelong health and obese people need help not blame.
Burden of Obesity in India: Obesity in India has emerged as a critical, rapidly escalating, and often under-recognized public health crisis, with the country ranking third globally in the number of adults living with obesity. Driven by rapid urbanization, sedentary lifestyles, and dietary changes, obesity is increasingly coexisting with undernutrition, a phenomenon known as the "double burden of malnutrition". Research indicates that Indians weight for 2-3 years before seeking medical help. This delay may result in risk of complications like heart & liver diseases, PCOS. In 2025, India faces a severe obesity crisis, with projections indicating over 21 crore men and 23 crore women are overweight or obese, impacting nearly one-third of the population. Sedentary lifestyles and processed foods have driven this surge. In 2021, the ICMR-INDIAB study estimated 254 million people with generalized obesity (BMI 25 kg/m²) and 351 million with abdominal obesity (WC 90 cm in males, 80 cm in females). By 2019-21, 40% of women and 12% of men were found to be abdominally obese. Approximately 32% of Indians exhibit a "thin-fat" phenotype (normal BMI but high visceral fat and high cardiometabolic risk), requiring specific diagnostic approaches beyond standard BMI. Rates are higher in urban areas, but rural areas are "fast catching up". Obesity is more prevalent in women (30-49 age) & in high-income, urban populations. Childhood Obesity: Alarming rise from 0.1%–0.2% in 1990 to 3.1%–3.7% in 2022, with projections indicating 12.5 million children & adolescents will be obese by 2030 [6,7].
Pint to Paunch-An Urban Phenomenon of Craft Beer Culture Fuelling Obesity: Extra pint of craft beer at the end of a long day adds more to the waistline than one realizes. Microbrewery culture has become significant driver of weight gain, when added to a sedentary and high stress urban lifestyle. Its combination of multiple pints, heavy starters, late night disrupting sleep time and very little movements. Many young professionals otherwise looking healthy presenting with increased waist circumference, early fatty liver, borderline blood sugar and hypertension has become a common scene today in cities. Most of them have a clear history of frequent brewery visits [8].
Obesity in Karnataka: Studies in Southern Karnataka indicate a high prevalence of central obesity among women, with a significant portion of the population (nearly one quarter of women, aged 15-49) being overweight or obese. Key contributors in the region include urban living, sedentary occupations (e.g., banking/office work), poor sleep duration, and high-calorie, mixed-diet consumption. Obese patients in the region frequently present with related conditions such as metabolic syndrome, hypertension, and arthritic issues.
A cross-sectional study among 800 adolescents aged 13–17 school-going adolescents from various private schools in Kalaburagi city a backward district of Kalyan Karnataka known for high prevalence of malnutrition. Anthropometric measurements were taken using standardized methods. Overweight/obesity was classified based on the 2015 Indian academy of paediatrics (IAP) growth chart. Statistical analysis was performed using IBM SPSS version 25.0, with the Chi-square test applied for significance (p<0>
The study found that 34.3% of participants were either overweight or obese. A significant association was observed between overweight/obesity and various lifestyle factors like diet, screen time, physical activity, and family history. High intake of calorie-dense, processed, and fast food emerged as a major contributor [9].
Clinical Manifestations and Comorbidities: In Indian populations, metabolic complications often appear at a lower Body Mass Index (BMI 25 kg/m²) compared to Western populations.
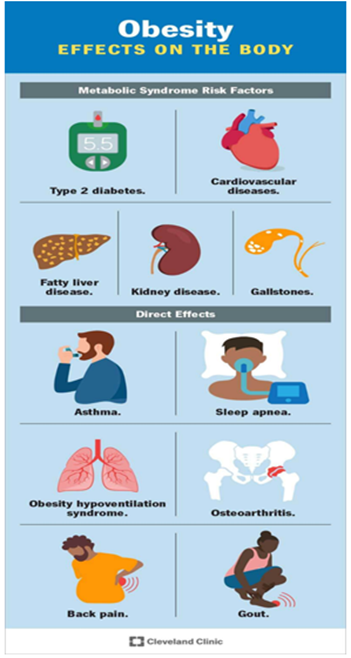
i) Cardiometabolic Syndrome: High prevalence of abdominal (visceral) obesity directly links to hypertension, type 2 diabetes mellitus (T2DM), and dyslipidaemia ii) Metabolic Disorders: 57% of diabetic individuals remain undiagnosed iii) Fatty Liver Disease: High prevalence of Non-alcoholic fatty liver disease (NAFLD), with a 63.4% prevalence among obese children iv) Musculoskeletal Issues: Osteoarthritis (mainly knee joints), chronic back pain, and reduced mobility v) Respiratory Problems: Obstructive sleep apnoea (OSA) and shortness of breath vi) Skin Manifestations: Acanthosis nigricans (velvety, darkened skin patches indicating insulin resistance), skin tags, & intertrigo (infection in skin folds) vii) Reproductive/ Endocrine Issues -Polycystic ovary syndrome (PCOS) in women, infertility, & gestational diabetes viii) Psychosocial Impact: Low self-esteem, depression, and social stigma.
Diagnostic Challenges & Options: Obesity’s assessment requires several clinical indicators, as no single measure can accurately capture all obesity-related risk factors.
- Body mass index (BMI) is an accepted screening tool for identifying overweight and obesity and is calculated using weight and height. A high BMI is linked with increased risk of non-communicable diseases and mortality. However, individuals with the same BMI may differ in body fat distribution and skeletal muscle mass. Overweight >23 kg/m2 and Obesity >30 kg/m2
- Waist circumference (WC) is used to measure central obesity and is strongly associated with metabolic complications. Waist circumference alone (>102 cm for men, >88 cm for women). Waist circumference >90 cm in men or >80 cm in women is considered as central obesity.
- Hip circumference (HC) is measured at the widest part of the hips and is primarily used in combination with waist circumference to assess fat distribution. Hip Measurement measures the distribution of fat, focusing on metabolic risk (visceral fat). A high ratio indicates "android" (apple-shaped) obesity, which is more strongly linked to heart disease, type 2 diabetes, and premature death than "gynoid" (pear-shaped) obesity. While useful, it is often paired with or superseded by WHR.
- Waist–hip ratio (WHR) is a straightforward indicator of central obesity, calculated by dividing WC by HC. Elevated WHR is associated with increased cardiometabolic risk. Abdominal obesity is better determined using the waist-to-hip ratio (WHR), calculated by dividing waist circumference by hip circumference at largest part of buttocks. WHO defines abdominal obesity as a WHR >0.90 for men and >0.85 for women. A ratio >1.0 for either sex signifies a significantly increased risk of health complications.
- Wrist circumference: Wrist circumference (WrC) is a valuable, non-invasive anthropometric tool for assessing nutritional status and body composition, particularly for identifying frame size, obesity, and cardiovascular risk. It is considered a proxy for bone mineral density and peripheral fat distribution, providing a stable measure of skeletal size that is not significantly influenced by weight fluctuations or abdominal distension.
Key Findings on Wrist Circumference and Nutrition:
- Frame Size Definition:
- Small Frame: < 17>
- Medium Frame: 17.5 – 17.8 cm
- Large Frame: > 17.8 cm
Obesity and Cardiometabolic Risk: Higher wrist circumferences are positively associated with high blood pressure, low HDL cholesterol, insulin resistance, & Metabolic Syndrome (MetS). Cut-off Points for Obesity: Males: 16.5 cm to 18 cm & Females: 15.7 cm to 16.3 cm
- Neck circumference (NC): Neck circumference is associated with metabolic syndrome, visceral adiposity, & cardiometabolic risk in adults and children. These measures are low-cost and practical for clinical screening. Neck circumference (NC) is a valid, simple, and low-cost screening tool for estimating upper-body subcutaneous fat and cardiometabolic risk. Generally, obesity is indicated by an NC greater than 35.5 cm in men and 32 cm in women. Some studies suggest higher thresholds of 38.5 cm for men and 34.5 cm for women, depending on the population. NC is a useful, quick alternative to waist circumference for assessing metabolic syndrome. A thicker neck (e.g., >17 inches or 43 cm for men, >15.5 inches or 39 cm for women) can indicate a higher risk for obstructive sleep apnoea.
- Body fat percentage can be assessed using bioelectrical impedance analysis (BIA), which estimates fat mass and fat-free mass and is considered more accurate than BMI for body composition assessment. One can calculate body fat percentage (BF%) using various methods, from simple formulas based on measurements (height, waist, neck, and hips) to more complex ones using BMI, or even high-tech options like DEXA scans or Bod Pods. The US Navy Method (Circumference-Based) is a popular, free, tape-measure method for estimating BF%. A) For Men: Measure Height, Waist (at navel), and Neck (below Adam's apple). B) For Women: Measure Height, Waist (narrowest point), Neck (narrowest point), and Hips (widest point). Calculation: Input these measurements into an online US Navy body fat calculator. But skinfold callipers (pinching skinfolds at specific sites) or online calculators using circumference are popular, accessible ways to track trends, even if they have limitations compared to professional equipment.
- Imaging techniques like magnetic resonance imaging (MRI), computed tomography (CT), and dual-energy X-ray absorptiometry (DEXA) provide precise measurements of total and regional fat mass.
- Comprehensive Approach: The "4 Ms of Obesity" is a framework for comprehensive assessment and treatment, focusing on Meals, Movement, Mind, and Medicine. Metabolic factors (including Mechanical and Monetary aspects), to address the complex, multi-dimensional nature of obesity beyond just weight, looking at lifestyle, mental health, physical function, and medical complications for a personalized plan.
Complications of Obesity:
Obesity, Microbial Changes and Early onset Rectal Cancers (EOCRC):
Obesity has repeatedly been associated with microbial changes that contribute to EOCRC. A study by Xu et al. suggested that EOCRC exhibits reduced faecal alpha diversity in the luminal gut microbiome compared with both LOCRC and healthy controls, with an increase in specific taxa that correlate with obesity and high-fat diet (HFD). Specifically, members of the Firmicutes phylum, including Blautia, Actinomyces, and Clostridia, showed positive correlations with HFD-induced obesity, while beneficial SCFA producing taxa were markedly reduced. The study also suggested that pathobionts relevant to EOCRC are responsive to obesity, such as Fusobacterium nucleatum, enterotoxigenic Bacteroides fragilis, and Escherichia coli, along with cohort signals indicating that Fusobacteria and Bacteroides differentiate EOCRC from LOCRC. Notably, taxa associated with short-chain fatty acids (SCFAs) are diminished, and Mitsuokella multacida was not present in EOCRC samples. Mitsuokella multacida was notably absent from EOCRC samples, further reflecting depletion of protective commensals. Obesity-associated dysbiosis enriches pathobionts that activate Wnt/β-catenin and dampen anti-tumour immunity (Fusobacterium nucleatum), cleave E-cadherin and drive NF-κB/STAT3/IL-17 inflammation (enterotoxigenic Bacteroides fragilis), and deliver colibactin-mediated DNA damage (Escherichia coli pks⁺). These mechanisms provide a biological basis for why obesity may specifically accelerate EOCRC [12].
Lipodystrophy- obesity-related complications: A desperate father walked into our clinic cradling his 14-year-old daughter. The girl was rail thin, weak, and covered with painful lesions. Her triglycerides were off the charts, and her liver was huge. We wondered why someone with so little fat would have some of the worst obesity-related complications. Later we learnt that the culprit was lipodystrophy, a rare disorder in which the body lacks the fat cells needed to make leptin. Most of doctors and general population look at fat as something bad. It is this beautiful tissue that stores energy and sends all kinds of important signals. Without the leptin signal, the brain panics, pausing tasks like reproduction and fighting infection to focus on one mission finding food. Without healthy tissue to store lipids, the body crams them into inopportune places, leading to fatty liver disease and fat-filled skin lesions called xanthomas. Congenital lipodystrophy is an extremely rare genetic disorder in India, typically presenting as Congenital Generalized Lipodystrophy (CGL) or Familial Partial Lipodystrophy (FPLD) with an estimated global prevalence of 1 per 4.7 per million, though often quoted as 1 in 10 million worldwide. The prevalence of FPLD is higher (1 in 7000), and cases in India are frequently underreported, often associated with consanguineous marriages. Until recently, there was no treatment. Since July of 2000, daily leptin injections are given [11].
Obesity Related Hypertension: According to the latest standards of care published by the American Heart Association, beta-blockers, metoprolol, propranolol, and atenolol, must not be used to treat hypertension in patients with obesity owing to their weight-promoting effects. Instead, weight-neutral drugs such as ACE inhibitors, ARBs, calcium channel blockers, and diuretics should be prioritized. For children and adolescents with overweight or obesity, routine evaluation for hypertension and blood pressure monitoring at every clinic visit must start at age 3 yrs. to detect and prevent hypertension-related comorbidities. Obesity and hypertension have a well-studied dose-response relationship, showing that the risk for hypertension increases 20%-30% for every 5% increase in body weight. Lowering a patient's body weight can reverse this effect, and a mean BMI reduction of 2.27 leads to a decrease in systolic and diastolic blood pressure of 5.79 mm Hg and 3.36 mm Hg, respectively, consistent with a 5%-10?crease in weight led to reduction of 3 mm Hg in systolic blood pressure, recently published in JAMA.
A calorie restriction, specifically the DASH diet, is the most effective intervention for lowering blood pressure through weight loss. Aerobic exercise, isometric training, low‐sodium and high‐potassium salt, comprehensive lifestyle modification, salt restriction, breathing‐control, meditation and low‐calorie diet have effects on blood pressure reduction, but low-calorie diets could lower blood pressure more than exercise alone. The DASH diet involves low intakes of fat, sugar, and salt and high consumption of fruits, vegetables, whole grain, and lean protein. It has a greater anti-hypertensive effect than Mediterranean diet.
A recent review of metabolic surgery's effect on hypertension found that Roux-en-Y gastric bypass, which is the most common bariatric surgery performed, had the most significant effect on reducing blood pressure. Although other modalities such as gastric banding, BPD/DS, and DJBL showed effectiveness compared to nonsurgical interventions [14].
Obesity & diabetes: The pathway from obesity to diabetes is rarely straightforward. Chronic stress—measured as allostatic load quietly shapes how prediabetes evolves, particularly in people carrying excess weight. In a cross-sectional study of adults with obesity, researchers compared prediabetes phenotypes defined by a 75-g oral glucose tolerance test: impaired fasting glucose (IFG), impaired glucose tolerance (IGT), and the combined IFG + IGT phenotype. Individuals with both IFG & IGT showed significantly higher allostatic load, greater body weight, and greater insulin resistance than those with either abnormality alone, independent of aerobic fitness. The IFG + IGT group had lower fasting ghrelin levels, a key appetite hormone, while PYY levels were similar across groups. Self-reported hunger and fullness did not vary, yet there was a tendency toward greater preference for fatty foods in the combined phenotype. These findings add nuance to the prediabetes pathway in obesity. Chronic physiological stress appears linked to altered appetite signalling & metabolic strain, especially in those with combined glucose abnormalities. Prediabetes is not a single state—it is a spectrum. Recognizing how stress biology intersects with appetite and insulin resistance will help clinicians intervene earlier, before the pathway progresses to overt diabetes [15].
Asthma and Obesity: Between 2001 and 2025, asthma-related hospitalizations, emergency visits and number of attacks per patient have all declined. Excess weight is a known risk factor in causing asthma, and obesity and overweight prevalence remain problematic. Severe obesity, especially among women continues to rise; the overall rate of obesity in children goes in the same direction. People with obesity and asthma do not respond to typical asthma treatments, like corticosteroids, as well as those who have normal weight. Their disease develops differently than in normal weight individuals. Each 1?c rise is linked to lower forced expiratory volume in 1 second (FEV₁) and more hospitalizations. Poor glucose control worsens asthma, while steroids worsen glucose metabolism. Physicians should track BMI and A1c at every visit. From a medical point, Asthma patients have reduced lung volumes and airway closure. The inflammation is cytokine-driven and steroid-resistant. Comorbidities like obstructive sleep apnoea (OSA-40-90%), gastroesophageal reflux disease (GERD-60-75%) and rhinosinusitis (RS-80%) are found in most patients. Because of this a doctor must expect blunted inhaled corticosteroid effect, and respond by optimizing the device, step up earlier and consider biologics. GPs must liaise with Specialists such as allergists (environment/immune therapies), pulmonologists (lung mechanics/severe asthma), endocrinology, dietitians (weight/metabolism), otorhinolaryngologists and gastroenterologists (airways/GERD). Refer an adult with asthma & obesity to specialists [10]
Obesity-asthma is a distinct phenotype with reduced corticosteroid responsiveness. Collaborative, multidisciplinary care improves outcomes. Refer when asthma remains uncontrolled despite guideline-based therapy and correct inhaler use, when metabolic disease complicates management, or when advanced diagnostics are needed. Specialists to consider with these specific triggers are i) Pulmonology/Allergy: Two or more oral corticosteroids-treated exacerbations per year, daily or nocturnal short-acting beta-agonist use, phenotype refinement, biologics ii) Allergy/Immunology: Environmental evaluation, allergy testing, immune-based therapies (biologics, immunotherapy in selected allergic asthma), co-management after ED/hospital visits iii) Endocrinology: A1c over 7?spite treatment, GLP-1 consideration iv) Otorhinolaryngology: Chronic rhinosinusitis, nasal polyps, airway, v) Gastroenterology for Symptomatic/refractory GERD and vii) a dietitian for nutrition counselling, structured weight programs, tailored activity [9]. Family Physicians must add weight goals to the asthma plan & emphasize weight loss to asthma improvement. For example, losing just 5-10% of our weight improves asthma control, reduce flare-ups, and help our lungs work better. Consult endocrinologists for GLP-1s, review every 3-6 months and document counselling [10].
Obesity & Severe Infection Risk: New research has showed that obese people have a significantly increased risk for hospitalization or death, with the highest level of obesity associated with an approximately threefold higher risk for nonfatal and fatal infections and possibly accounting for 1 in 10 infection-related deaths worldwide, from severe infection spanning a wide range of infections. The risks were consistent across wide-ranging types of infections, including SARS-CoV-2, pneumonia, urinary tract infections, and across nonfatal and fatal, acute and chronic, bacterial and viral, as well as parasitic and fungal infections with the exceptions severe HIV or Tuberculosis. We all have witnessed during the COVID-19 pandemic, people with obesity had a higher risk of being hospitalized or dying of SARS-CoV-2 infection [12].
Hypothalamic obesity (HO): It is a severe, often treatment-resistant metabolic disorder caused by damage to the hypothalamus due mostly from tumours like craniopharyngiomas. surgery, or radiation disrupting satiety and energy regulation. It is characterized by rapid, uncontrollable weight gain, extreme hyperphagia, reduced metabolic rate, and low physical activity.
High BMI Confirmed as a Causal Factor in Diabetic Kidney Disease: Diabetic kidney disease (DKD) is a common complication of type 2 diabetes mellitus (T2DM), affecting approximately 20% to 40% of individuals with diabetes.1 Factors such as hypertension, hyperglycaemia, and hyperlipidaemia contribute to disease progression. High HBMI is a significant risk factor that warrants attention [13]. Mendelian randomization (MR) and Global Burden of Disease (GBD) 2021 data evaluated the role of HBMI in DKD development. The MR analysis, based on 360 genetic variants linked to BMI, demonstrated a causal association between elevated BMI and increased DKD risk (odds ratio: 3.02; 95% CI: 2.28–4.13). Multiple analytical methods confirmed the consistency of this association [16].
Global estimates from the GBD 2021 revealed an increase in DKD burden attributable to HBMI (HBMI-T2DKD) between 1990 and 2021. Mortality rose from approximately 40,000 to 173,000 deaths, while disability-adjusted life years (DALYs) increased from 1.2 million to 4.3 million. Older adults, East Asia, and middle-Socio-Demographic Index (SDI) regions showed the highest burden. Males and individuals aged 65 years and older are expected to be most affected. Small Pacific Island nations currently report the highest age-standardized mortality and DALY rates, influenced by high obesity prevalence and limited healthcare infrastructure. Intervention strategies such as BMI screening, lifestyle modification, and pharmacological treatments, including GLP-1 receptor agonists and SGLT2 inhibitors, are essential. Causal evidence linking elevated BMI to DKD supports the inclusion of weight management as a core component in DKD prevention efforts.
Urbanization & Lifestyle (Rising disposable income & a shift in drinking culture among urban youth especially Draft Beer): Bira 91, launched in 2015 revolutionized the Indian beer market by introducing craft beer on-tap in cities like Delhi, Mumbai, Pune and Bangalore. By targeting urban millennials with flavourful, low-alcohol, imported-from-Belgium, and later locally produced, draught, the brand achieved rapid, viral growth. Launched in 2015 in Hauz Khas Village, Delhi, using on-tap, kegged, and bottled formats to offer "fresh" and "authentic" beer focused on urban millennials and young consumers in metropolitan cities. It shifted consumer preference from strong, mass-produced lagers to milder, flavourful craft options. Consumers viewed on-tap, draught beer as fresher, higher quality, and better value compared to bottled alternatives. A recent study in an International Journal of Obesity reported a clear dose-dependent relationship between alcohol consumption and Visceral Fat Mass (VFM) using a DEXA scan of 5761 adults’ Highest alcohol consumption had over 15% more visceral mass compared to light drinkers independent of total body fat. While bottled Beer has 100-150 calories, Craft beer has 200-300 Calories. If a person takes 5-6 portions he has (1500 calories) from Beer alone. Combine this with fried starters like Cheesy Pizza, burgers, Potato finger chips, meat, and elaborate deserts hitting about 100 calories the persons consume a total of 2000-3000 calories leading to Beer Belly & abnormal liver enzymes, disturbed sleep, acid reflux, gastritis, and high risk of diabetes among regular beer consumers. Every alternate adult in urban settings is overweight or obesity due to these multiple factors [8].
Prevalence of Obesity in India and Its Neurological Implications: Data for 1,00,531 adults from a nationwide randomized cluster sample survey (Niyantrita Madhumeha Bharata 2017, phase 1) determined Obesity using body mass index, and cross-tabulations were calculated across zones, age, gender, education, physical activity, and area. The prevalence of obesity in India was 40.3%. South had highest at 46.51% and east lowest at 32.96%. Obesity was higher among women than men (41.88% vs. 38.67%), urban than rural (44.17% vs. 36.08%), and over 40 than under 40 (45.81% vs. 34.58%). More education implied a higher obesity (44.6% college vs. 38% uneducated), as did lowered physical activity (43.71% inactive vs. 32.56% vigorously active). The odds ratio for physical activity was 3.83, stronger than age (1.58), education (1.4), urban (1.3), and gender (1.2).
Given the new evidence indicative of a three-fold increase in the risk of developing AD among obese populations without type 2 diabetes, and a potential modelling of AD itself as a brain-specific form of diabetes—the so-called type 3 diabetes, this represents a potentially large neurological dimension to the malady of obesity. Type 3 diabetes is a term used to describe the hypothesis that Alzheimer's disease is a form of diabetes caused by insulin resistance and impaired insulin signalling specifically within the brain. It is often referred to as "diabetes of the brain" because, like Types 1 and 2, it involves metabolic dysfunction—specifically, the brain's inability to use glucose properly, leading to neurodegeneration [17].
Obesity Management: As obesity prevalence continues to rise globally, combining these clinical measures is essential to improve risk stratification, personalize treatment, and move obesity care from simple categorization to meaningful clinical management. Lifestyle interventions targeting weight loss of 7–10% over 6 months and a diet hypocaloric by 30% or 500–1000 kcal forms the central pillar in the management [18].
Challenges to Management: i) Obesity is often viewed as a sign of prosperity or merely a cosmetic issue, rather than a chronic disease, leading to low medical seeking behaviour ii) Nearly 35% of individuals with high BMI would have not received a diagnosis from a healthcare professional iii) Lack of Structure: Limited specialized obesity clinics and inconsistent training for healthcare providers.
National academy of medical Sciences (NAMS) task force report on Obesity and lifestyle diseases in India recommends [5]:
- Primordial prevention which is the adaptation of strategies to stop the emergence of the risk factors before they have appeared. The preventive measures comprise the maintenance of normal body weight through the adoption of healthy nutritional habits and physical exercise. The role of health authorities & stakeholders is to manipulate the obesogenic environment in Favor of a healthy lifestyle environment, providing adequate space for physical activity. It is recommended that every adult and child must perform 30 min of daily physical activity for a minimum of 5 days a week. Stress management through recreational activities and mindfulness to be utilized at community levels, in schools and workplaces to prevent lifestyle diseases. Screening for NCDs, including NAFLD must be performed in all individuals >30 years of age.
- Primary prevention: Primary prevention during the stage of early pathogenesis phase of lifestyle diseases is to be promoted. For example, the pre-diabetes phase [impaired fasting glucose (IFG)/impaired glucose tolerance (IGT)] before the development of DM. In India, NCDs like CVD, cancer, chronic respiratory diseases, diabetes are estimated to account for around 60% of all deaths. The GOI has been implementing the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) since 2010 up to the district level under the National Health Mission.
- Secondary prevention: Preventive strategies that are carried out after obesity and lifestyle diseases have been detected to prevent or delay the development of long-term complications of the disease. Early diagnosis and prompt treatment of lifestyle disease, Once the person is diagnosed with obesity and lifestyle diseases, for the prevention of other comorbidities associated with that disease. For example, for diabetes, regular monitoring of blood glucose - Fasting Plasma Glucose (FPG) and 2 hours post prandial plasma glucose (2 h PPPG) at least once a month and more often if values are not in the ideal target range, and HbA1c at least every 6–12 months and more often (every three months) if values are not in the ideal target range, or tight control must be attempted. Tobacco & excessive use of alcohol must be discouraged. Urine glucose monitoring is not recommended, but urine examination for estimation of ketones is mandated if blood glucose is > 400 mg/dl each time
- Pharmacotherapy for Obesity: The weight loss medications are generating significant interest due to their proven ability to help individuals achieve substantial weight loss. For example, Ozempic (semaglutide) has gained widespread attention for its effectiveness in reducing body weight, even in individuals with obesity who do not have diabetes. When used alongside a balanced diet and regular physical activity, semaglutide can lead to a reduction of up to 15% of total body weight within a year, making it one of the most powerful pharmaceutical options for weight management. By targeting the GLP-1 receptor, semaglutide administered once a week, providing convenience, helps control appetite & improve insulin sensitivity, offering notable benefits for non-diabetic patients with obesity. Similarly, liraglutide, GLP-1 RA, requires daily injections, works in much the same way,
- Successful allopathic pharmacotherapy for obesity in India commonly involves using GLP-1 receptor agonists (e.g., Liraglutide, Semaglutide) or Orlistat alongside lifestyle modifications. These medications, such as weekly Semaglutide (up to 15% body weight loss) or daily Liraglutide (approx. 7% loss), effectively reduce weight and improve metabolic co-morbidities like type-2 diabetes in Indian patients.
- Integrated Prompt treatment: Pharmacological and non-pharmacological treatment must be provided to any person with obesity and lifestyle diseases coming to a facility for any illness. Regular health check-ups responding to the development of any co-morbid condition and referral to any other specialist if needed be ensured.
- 5. Tertiary prevention: It is carried out at the stage when complications have already set in, with the aim of preventing the progression of these complications.
- 6. Disability limitation: Tertiary prevention seeks to reduce the impact of obesity and lifestyle diseases by eliminating or reducing disability, minimizing suffering, and maximizing potential years of quality life. In epidemiological terms, tertiary prevention aims to reduce the number and/or impact of complications. This is the task of therapy and rehabilitation.
- 7. Rehabilitation: Follow-up of chronically ill obesity and lifestyle diseases patients to ensure adherence to medication regimen, monitor changes, and assist them in maintaining independence in daily life. Rehabilitation of patients to restore functions, through physiotherapy, and prevent recurrence or further complications through appropriate medication is an essential feature of rehabilitation.
- Strategies for existing health-care delivery system: NAMS recommendations has detailed i) Role of centres of excellence ii) Roles of Primary, Secondary & Tertiary public health facilities, and roles of health functionaries like medical officers, Health Assistant ASHA’s & AWWS [5].
Conclusions:
India and some middle-income countries in recent decades, have been experiencing a rapid epidemiological and economic transition, which has created several implications for the health status of the people. Lifestyle diseases or non-communicable diseases (NCDs) have emerged as the leading cause of morbidity and mortality for adults throughout the world, including developing countries like India. India’s burden of NCDs is escalating & contributes to around 65% of all deaths. NCDs typically present in individuals aged 55 years or older in developed countries, but in India their onset occurs is a decade earlier (≥45 years of age). Given the high cost of obesity in terms of type 2 diabetes, cardiovascular diseases, and Alzheimer s Disease, urgent public health measures are necessary to reduce its impact.
The major risk factors responsible for lifestyle diseases are obesity, physical activity, tobacco smoking, alcohol consumption, and mental stress. Obesity is the single most important risk factor. Several large prospective cohort studies have shown that the most important risk factors are overweight and obesity. The increased distribution of body fat, particularly in the truncal and abdominal region, has been shown to be associated with an increased risk of insulin resistance and diabetes.
There is convincing epidemiologic data to support the role of physical activity in preventing diabetes. Aerobic exercise done by overweight and obese adults results in modest weight loss, which is independent of the effect of caloric reduction through dieting. However, only part of the beneficial effect of physical activity on diabetes is mediated through body weight. Physical activity is clearly associated with increased insulin sensitivity.
Although smoking cessation is associated with a modest increase in weight, it increases insulin sensitivity and improves the lipoprotein profile. Effects of alcohol consumption on the risk of development of lifestyle diseases follow a U-shaped curve. While moderate consumption is shown to be associated with lower incidence, this beneficial effect is reversed with heavy consumption. Recent observations have shown that increased mental stress and activation of the physiologic stress response from chronic exposure to stressors, low socioeconomic status (SES), severe mental health problems, or aggressive behaviour increases the risk of lifestyle diseases. There are certain genes that predispose Indians to diabetes, while other genes that afford protection against diabetes. Lifestyle interventions targeting weight loss of 7–10% over 6 months and a diet hypocaloric by 30% or 500–1000 kcal form the central pillar in the management of lifestyle diseases.
Overall, calorie restriction appears to be more important than the type of diet per se, and patients should be counselled to restrict calories by curtailing carbohydrates and fat. A healthy diet sourced from locally available food products suited to local culinary tastes is more likely to be adhered to in the long term, which is crucial for sustainable benefits.
Suggested exercise usually consists of moderate-intensity aerobic exercises, such as brisk walking, jogging, running, swimming, or cycling for 30–45 min/day at least five days a week. However, resistance training supplements aerobic exercises and may be particularly useful for patients who cannot otherwise do aerobic exercises due to poor cardiorespiratory reserve, joint pains, etc. Importantly, exercise can improve insulin resistance, improve blood flow, decrease atherosclerosis, decrease lipids in blood, and hepatic steatosis even in the absence of weight loss.
In obese patients who are unable to decrease and maintain body weight using lifestyle measures, various options like pharmacotherapy, endoscopic procedures for weight loss, or bariatric surgery may be considered on an individual basis.
Initiating NCD screening at the health and wellness centre-level, incorporating yoga and wellness activities closer to the community, and with integration of Non-Alcoholic Fatty Liver Disease (NAFLD) to National Programme for prevention & Control of Cancer, Diabetes, Cardiovascular Diseases & stroke (NPCDCS) program, the Government of India (GOI) targets control on lifestyle diseases soon.
References
- World Obesity Federation, (2025). The World Obesity Atlas 2025, World Obesity Federation Data Portal.
View at Publisher | View at Google Scholar - UNICEF, (2025). Child Nutrition Global Report 2025, UNICEF Report.
View at Publisher | View at Google Scholar - Types of obesity based on the area of fat distribution, General Source.
View at Publisher | View at Google Scholar - Kalra S et al., (2026). Burden of obesity in India: Need for policy changes, Clinical Obesity, 16(2), e70072.
View at Publisher | View at Google Scholar - Duseja A et al., (2024). NAMS task force report on obesity and lifestyle diseases in India, Annals of National Academy of Medical Sciences, Report.
View at Publisher | View at Google Scholar - Medtalks, (2026). Measuring obesity beyond weight: A comprehensive clinical assessment, Online Clinical Newsletter.
View at Publisher | View at Google Scholar - Sruthi KG et al., (2023). Assessment of obesity in the Indian setting: A clinical review, Clinical Epidemiology and Global Health, 23, 101348.
View at Publisher | View at Google Scholar - The Times of India, (2026). Pint to paunch—An urban phenomenon of craft beer culture fuelling obesity, Newspaper Article.
View at Publisher | View at Google Scholar - Sameer Ahammad S et al., (2025). Study of prevalence of overweight and obesity among school-going adolescents in North Karnataka and its association with lifestyle changes, International Journal of Contemporary Paediatrics, Online Article.
View at Publisher | View at Google Scholar - Bahls C, (2026). Asthma and obesity: Quick reference for primary care, Medscape.
View at Publisher | View at Google Scholar - Akinci B, (Year not available). Lipodystrophy syndromes: Presentation and treatment, NCBI Bookshelf.
View at Publisher | View at Google Scholar - Melville NA, (2026). Obesity linked to increased severe infection risk, Medscape.
View at Publisher | View at Google Scholar - Xu P et al., (2024). Obesity and early-onset colorectal cancer risk: Emerging clinical evidence and biological mechanisms, Frontiers in Oncology, 14, 1366544.
View at Publisher | View at Google Scholar - Ali YS, (2026). Obesity-related hypertension, Medscape.
View at Publisher | View at Google Scholar - Malin SK et al., (2026). Appetite regulation and allostatic load across prediabetes phenotypes, Nutrients, 18(1), 158.
View at Publisher | View at Google Scholar - Jiang W et al., (2020). Establishment and validation of a risk prediction model for early diabetic kidney disease, Diabetes Care, 43(4), 925–933.
View at Publisher | View at Google Scholar - Rao MV et al., (2021). Prevalence of obesity in India and its neurological implications, Annals of Neurosciences, 27(3–4), 153–161.
View at Publisher | View at Google Scholar - Cleveland Clinic, (2024). Weight control and obesity, Cleveland Clinic Health Library.
View at Publisher | View at Google Scholar - Chakrabarti SK et al., (2025). The impact of weight loss drugs on health and society in India, Addiction Research & Behavioural Therapies, 4(1), 1–8.
View at Publisher | View at Google Scholar
