

Research Article | DOI: https://doi.org/10.31579/2835-2971/051
Maternal and Socioeconomic Factors Drive Childhood Anemia in Tajikistan: Examining the Role of Zero Vegetable or Fruit Consumption among under five
1School Of Public Health and Social Work, Queensland University of Technology (QUT), Brisbane, Australia.
2Fatima Memorial Hospital College of Medicine and Dentistry, Lahore, Pakistan.
3Ziauddin Medical College, Ziauddin University, Karachi, Pakistan.
4United Medical and Dental College, Karachi, Pakistan.
5Dow University of Health Sciences, Karachi, Pakistan.
*Corresponding Author: Bushra Ashar, 5Dow University of Health Sciences, Karachi, Pakistan.
Citation: Asif Khaliq, Namra Ijaz, Yusra Rizwan, Sarah Aijaz, Bushra Ashar, (2025), Maternal and Socioeconomic Factors Drive Childhood Anemia in Tajikistan: Examining the Role of Zero Vegetable or Fruit Consumption among under five, Journal of Clinical Pediatrics and Mother Health, 4(1); DOI:10.31579/2835-2971/051
Copyright: © 2025, Bushra Ashar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 February 2025 | Accepted: 17 February 2025 | Published: 26 February 2025
Keywords: anemia; preschool child; socioeconomic factors; maternal nutritional physiological phenomena; diet surveys; tajikistan
Abstract
Objectives: To examine whether complete absence of vegetable and fruit consumption (Zero Vegetable or Fruit - ZVF) independently associates with anemia among children aged 0-59 months in Tajikistan, and to identify key maternal and socioeconomic determinants of childhood anemia.
Design: Cross-sectional analysis using recent 2023, nationally representative Demographic and Health survey data from Tajikistan.
Setting: National population-based study across all regions of Tajikistan (urban and rural areas) using two stage stratified cluster sampling.
Participants: 2,355 children in age group 0-59 months with complete data on hemoglobin levels and dietary intake in the preceding 24 hours residing in households selected from 2023 Tajikistan Demographic and Health Survey were included in this study.
Main Outcome Measures: Primary outcome, childhood anemia status (hemoglobin <10.5g/dl for 6-23 months, <11g/dl for 24-59 months, altitude-adjusted per WHO 2024 criteria).
Results: Among Tajik children under 5 years, 36.1% of children consumed no vegetables or fruits in the preceding 24 hours and the prevalence of anemia was 33.2%. Adjusted odds in our study revealed no association of ZVF consumption with anemia (OR=0.85, 95% CI: 0.63 to 1.14). Significant associations emerged for maternal anemia which increased child anemia odds by 48% (OR=1.48, 95% CI: 1.16 to 1.88), richest index had 60% lower anemia odds compared to the poorest (OR=0.39, 95% CI: 0.27 to 0.56) and low birth size increased anemia risk two fold (OR=1.92, 95% CI: 1.31 to 2.81).Each additional daily meal consumption reduced anemia odds by 14% (OR=0.86, 95% CI: 0.76 to 0.98).
Conclusions: Child anemia in Tajikistan is not primarily driven by specific dietary factors but maternal nutritional status during pregnancy, birth outcomes, and socioeconomic disparities are main drivers. This novel null finding on ZVF intake, underscores that non dietary drivers predominate, informing targeted interventions aligned with SDG2 (Zero hunger). Thus integrated approaches aim to address maternal nutrition, antenatal care, wealth inequalities, and feeding frequency promotion.
What is already known on this topic:
Over 40% of children under five globally are affected by childhood anemia with dietary factors like low fruit and vegetable intake considered important contributors. However, the specific impact of complete absence (zero consumption) of vegetables and fruits on childhood anemia needs to be explored particularly in Central Asian countries like Tajikistan as here the dietary pattern differs from other low- and middle-income settings.
What this study adds:
This first nationally representative Central Asian study showed that downstream factor that’s the zero vegetable or fruit consumption had no association with childhood anemia in Tajikistan. Instead, upstream factors like maternal anemia during pregnancy, household wealth disparities, small birth size, and meal frequency emerged as primary determinants, challenging dietary-centric intervention approaches.
How this study might affect research, practice or policy:
These findings redirect anemia prevention strategies towards integrated interventions addressing maternal nutrition during pregnancy, poverty alleviation, improved antenatal care for fetal growth monitoring, and feeding frequency promotion rather than focusing solely on vegetable or fruit consumption. This evidence informs sustainable development goals (SDG) aligned nutrition policies requiring upstream determinants to be prioritized alongside dietary diversity programs in similar settings
Introduction:
Anemia remains a major public health concern especially for children of age 6-59 months.
According to the estimates of World Health Organization (WHO) 2025 showed over 40% of children under five years of age worldwide to be affected [1]. Especially a concern in rural areas some related factors like limited dietary diversity, food insecurity, seasonal poverty, and inadequate access to nutritious food such as iron-fortified products, fruits, vegetables, and animal proteins, there by prevalence is consistently rising [2. The weaning period is the time of maximum burden which a child under 2 years face in low- and middle-income countries as evidenced by the United Nations Children's Fund (UNICEF) [3] and also reports the intergenerational impacts of child anemia with maternal anemia [4]. During infancy and early childhood, stunted growth, decreased immunity, and poor cognitive and psychomotor development are heavily influenced by anemia [5]. These effects not only are deleterious for child survival but also compromise long-term educational achievement and productivity, leading to vicious cycles of poverty and ill health. Anemia caused ~52 million years lived with disability (YLDs) globally in 2021, with under 5s contributing 20% [6]. While SDG 2.2 anemia target focuses on women, interventions for children under 5 are critical to achieving broader malnutrition goals, as maternal and child anemia are interlinked [3]. The stable 40% prevalence (~269 million children in 2025) from WHO/UNICEF estimates underscores the urgency of scaling up interventions [4] to meet the SDG target 2030. Fruits and vegetables are rich sources of non-heme iron, vitamin C, folate, and antioxidants, all crucial for hemoglobin synthesis and red blood cell production. Although non-heme iron from plant sources is less bioavailable than heme iron from animal foods, vitamin C in fruits and vegetables enhances its absorption by reducing ferric (Fe³⁺) to ferrous (Fe²⁺) iron [7]. The Zero Vegetable or Fruit consumption (ZVF) a new standard variable was introduced in the 2021 update to the Infant and Young Child Feeding (IYCF) guidelines by the WHO & UNICEF, 2021 [8] for household surveys to measure unhealthy eating practices. The target children for this variable are aged 6–23 months who did not consume vegetables or fruits in the previous day or night. This indicator is critical because inadequate vegetable and fruit intake heighten anemia and some studies support stunting risk [9] and in long-term leads to heart disease and type 2 diabetes [8]. Tajikistan representing a LMIC in Central Asia, shows similar burden moreover where rural households often rely on self-grown staples like cereals and potatoes, which are low in bioavailable iron, exacerbating micronutrient deficiencies [10]. While global evidence relates low fruit and vegetable consumption to anemia, research on the impact of entire absence (“zero consumption”) remains limited, and no earlier study has specifically addressed this association in Tajikistan [11,12]. This represents a critical regional gap, as Central Asia specific studies on dietary anemia specifically ZVF context and using DHS data are scarce, leaving policymakers without localized evidence to guide interventions (13). A part from dietary factors socioeconomic and maternal factors further shape child nutritional outcomes. Maternal education improves awareness of proper feeding practices and health-seeking behaviors, while household wealth affects food affordability and dietary diversity [14]. In Tajikistan, rural households sometimes face additional challenges, including poorer maternal education, restricted healthcare access, and inadequate market connectivity [15]. These discrepancies contribute to dietary deficiency and greater anemia prevalence among children in impoverished groups. Understanding how socioeconomic disparities connect with ZVF consumption is therefore crucial for devising effective, equitable nutrition programs. Using data from the 2023 Tajikistan Demographic and Health Survey (TjDHS), this study examines whether complete absence of fruit and vegetable consumption independently associates with anemia among children aged 0-59 months, filling a critical evidence gap in Central Asia. It investigates how this relationship varies by household wealth, maternal factors, and urban-rural residence. Notably, null findings would be equally valuable indicating that dietary interventions alone may be insufficient without addressing upstream determinants such as maternal health status, intrauterine growth, and poverty. The findings are intended to offer evidence-based insights that will direct national nutrition plans and inform specific policies there by targeting SDG 2.2 (ending all forms of malnutrition by 2030) and SDG 3.2 (reducing preventable child deaths).
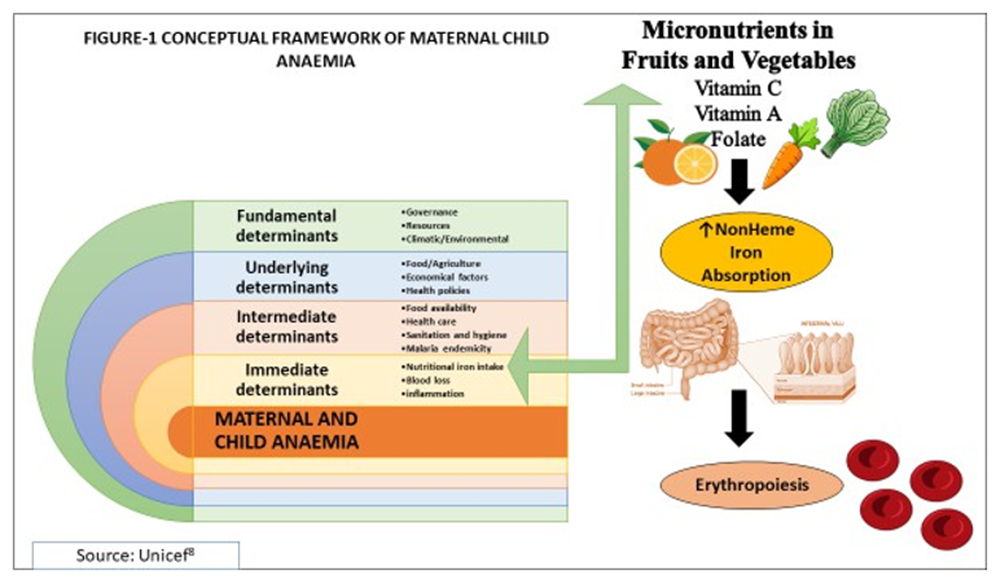
Conceptual Framework:
The conceptual framework for childhood anemia recommended by UNICEF, adapts its broader framework for maternal and child undernutrition. It identifies a hierarchy of causes, including immediate causes like inadequate diet, illness and health care, underlying causes such as household food insecurity and health policies, and basic causes stemming from social, economic, and political factors. UNICEF’s approach emphasizes that interventions must be integrated and addressed at all levels of these determinants [10]. Nutritional iron intake is the most immediate or downstream pathway that is responsible for child’s anemia.
Methodology:
Study Design and Setting:
We conducted a cross-sectional study that utilized secondary data analysis from the DHS 2023 Tajikistan, (TjDHS). Thereby we were interested to investigate the association between ZVF consumption with anemia in children aged 0-59 months in this country. The TjDHS,2023 the third following surveys in 2012 and 2017, took place from August to November 2023 during post-harvest months, potentially underrepresenting food shortages common in off-seasons. Tajikistan’s mountainous landscape, reliance on staple crops like rice and wheat, and climate challenges likely heighten child malnutrition and anemia, an ongoing public health issue. Our study adhered to strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines which emphasized structured overview of design, variables, and analyses enhancing replicability and robust estimates thus minimizing reporting biases [16].
Sampling Methods and Sample Frame:
The TjDHS utilized a two-stage stratified cluster sampling design [17], covering all regions and balancing urban and rural areas to provide a nationally representative profile of child anemia. It involved nine strata (urban/rural across regions). In the first stage, 370 primary sampling units (PSUs) were selected with probability proportional to size, based on the 2020 Tajikistan Population and Housing Census [TPHC] as its sampling frame conducted by the Agency on Statistics under the President of the Republic of Tajikistan (Tajstat). In the second stage, 22 households per PSU were systematically selected from updated household listings, yielding 8,140 households (3,652 urban, 4,488 rural). This design, with no replacements allowed, ensured a representative sample of 10,718 completed interviews with women age 15–49 covering all regions [17,18]. (Figure-2)
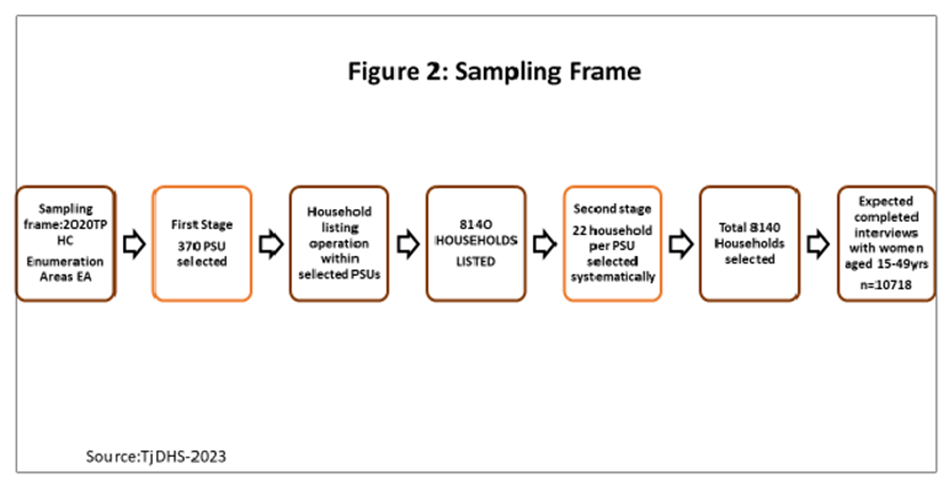
Figure 2: Sampling Frame
Where,
TPHC- Tajikistan Population and Housing Census PSU- Primary Sampling Units
Study Participants and Eligibility:
The target population comprised children with age 0–59 completed months and non-pregnant women 15-49 completed years of age, with no distinction between lactating and non-lactating women residing in households selected for the 2023 DHS survey in Tajikistan. This total reflects all de jure participants. All eligible children in these households were recruited, minimizing selection bias [18]. Inclusion criteria included children with complete data on hemoglobin levels and dietary intake in the preceding 24 hours. Children over 59 months (per WHO anemia guidelines) were excluded. The analytic sample consisted of 2,355 children after exclusions for missing data on specific variables (e.g. child age, anemia, dietary variables) representative of the 2023 Tajikistan DHS, which surveyed 8,035 households with a 99.6% response rate, covering all regions and urban-rural strata. The survey weights minimized non- response bias and ensured representativeness [18].
Data Collection:
Data was collected via standardized DHS questionnaires involving the Woman’s Questionnaire that collected information from all eligible women age 15-49yrs related to health and nutrition, breastfeeding and complementary feeding practices. The Biomarker Questionnaire was used to record the results of anemia testing. The protocol for anemia testing was reviewed and approved by the Institutional Review Board of Ministry of Health and Social Protection of the Population of Tajikistan (MoHSPP) and the ICF, UNICEF and Asian development bank [17]. The DHS surveys use single method, the HemoCue system for hemoglobin measurement.
Quality Assurance:
Hemoglobin measured by trained enumerators following DHS protocols, with quality control Blood specimens for anemia testing were collected from women age 15-49yrs who consented to be tested and from children age 0–59 months whose parents or guardians had given consent to the testing. Capillary blood was drawn from a finger prick (or a heel prick in the case of children age 6–11 months and the third drop of capillary blood was collected in a HemoCue® 201+ microcuvette. Hemoglobin analysis was carried out on-site using a battery-operated portable HemoCue® 201+ device, daily HemoCue device calibration was also checked. Altitude adjustment applied using DHS-provided geospatial data. Hemoglobin levels were measured following established Demographic and Health Surveys (DHS) protocols, utilizing trained enumerators to ensure data consistency and accuracy. To maintain data reliability and validity, a rigorous quality control process was implemented, including duplicate testing on a 5% subsample of measurements. Furthermore, all hemoglobin values were adjusted for altitude using geospatial data provided by DHS, a critical step to account for physiological variations at different elevations. Field supervision by team of supervisors, field coordinators and biomarker specialists observed procedures directly and use checklists ensure accurate measurements, achieving ~95% biomarker coverage [17]. Any necessary data cleaning steps were performed to enhance the integrity of the dataset.
Completeness of Data:
A precise analysis of 2023 data survey of Tajikistan was done by a team of researcher A.K and B.A, in order to validate the completeness of data for children aged 0–59 months. The data showed a total of 5,068 cases with 135 missing data for child’s age. A stepwise approach was done to handle the missing values by listwise deletion from the system. Next the data on child’s anemia was checked for appropriateness. This included 413 "Missing" cases as explicitly and "System" missing (likely due to incomplete or unrecorded hemoglobin measurements). Among the valid cases, 4520 children had complete anemia data. No specific outliers were reported during data cleaning suggesting values were within expected ranges after quality control by trained field staff and biomarker monitors (~95% biomarker coverage). The 413 missing cases were excluded by listwise deletion from data finalizing complete anemia data. Further missing values were similarly handled from various food diversity variables thus ensuring completeness of data of valid 2355 cases.(Figure-3)
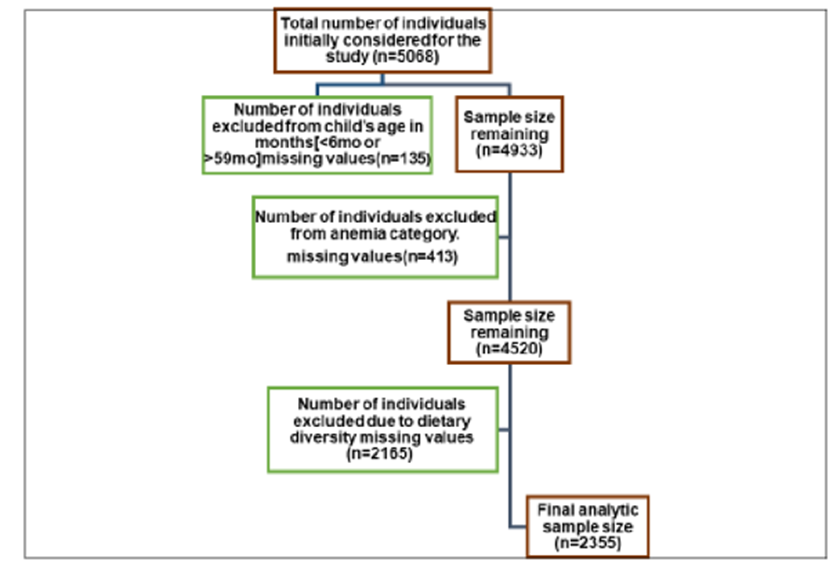
Figure 3: Strobe flow diagram for participants and eligibility criteria for DHS analysis.
Study Variables:
Exposure Variables:
Zero Vegetable or Fruit consumption:[ZVF]
ZVF consumption 0-59 months reflects percentage of children age 0-59 months who were not fed any vegetables or fruits during the previous day. Number of youngest children age 0-59 months living with their mother(8). In the 2023 Tajikistan Demographic and Health Survey (TjDHS), data on vegetable and fruit consumption for children aged 0-59 months were gathered via structured 24-hour dietary recall interviews with mothers or primary caregivers, using a standardized questionnaire. Fieldworkers queried whether children consumed specific items in the past day, including fruit juice (V410), other vegetables (V414A), plantains/potatoes/cassava (V414F), pumpkin/carrots/squash (V414I), dark green leafy vegetables (V414J), mangoes/papayas/vitamin A-rich fruits (V414K), and other fruits (V414L), ensuring consistent and reliable dietary assessment. Responses were recorded as binary (yes/no) for each food item, later combined into a derived variable, ZVF Consumption (ZVF), Children who responded "no" to all seven vegetable and fruit consumption variables were classified as having zero consumption (ZVF=1), while those who consumed at least one item were classified as having consumed vegetables and fruits (ZVF=0), (19) [Supplementary file 1].
Minimal meal frequency: [MMF]
Minimum meal frequency is a proxy for meeting energy requirements. Breastfed children age 6–8 months are considered to be fed with a minimum meal frequency if they receive solid, semisolid, or soft foods at least twice a day. Breastfed children age 9–23 months are considered to be fed with a minimum meal frequency if they receive solid, semisolid, or soft foods at least three times a day. Non breastfed children age 6–23 months are considered to be fed with a minimum meal frequency if they receive solid, semisolid, or soft foods or milk feeds at least four times a day and if at least one of the feeds is a solid, semisolid, or soft food [8].
Outcome Variable:
Child Anemia
The children presented in this study used the new cutoffs to define anemia and have been adjusted for altitude according to the latest WHO guidance. Anemia is defined as hemoglobin <10 severe=1, moderate=2 mild=3 xss=removed>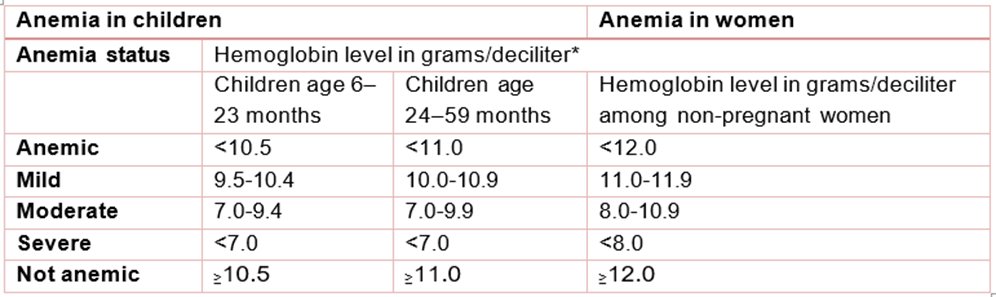
Table 1: Anemia cutoff points in accordance with WHO 2024.
*Hemoglobin levels are adjusted for altitude according to WHO 2024(20).
Covariates:
Covariates were chosen based on prior Demographic and Health Survey research on child anemia, targeting socioeconomic, demographic, and health-related factors linked to nutritional deficiencies in low- and middle-income settings. These included child age (6–23 months for early feeding risks, 24–59 months for high body demands), sex to address potential gender-based feeding variations, urban-rural residence to account for food and healthcare access gaps, maternal education (none, primary, secondary+) as a marker of health knowledge, household wealth index from asset-based analysis to reflect economic limits, birth order for household resource distribution, recent morbidity (diarrhea or fever in past two weeks) affecting nutrient uptake, and minimum meal frequency to control for feeding frequency’s impact on nutrient intake in children aged 6–59 months.
Ethical Considerations:
This secondary analysis used de-identified public data hence no additional ethical approval required. Original DHS adhered to Helsinki Declaration ethical framework for the original survey’s data collection, ensuring informed consent was obtained from the participants of the study.
Statistical Analysis:
Descriptive statistics characterized the study population using weighted frequencies and percentages for categorical variables were utilized. Inferential analyses utilized binomial and multivariable logistic regression, conducted in Jamovi version 2.3 and SPSS version 25 softwares, to estimate unadjusted and adjusted odds ratios (ORs) with 95% confidence intervals for the association between ZVF intake and anemia among children aged 0-59 months. We used binomial logistic regression to examine factors associated with childhood anemia, treating anemia status as a binary outcome (anaemic vs. non-anaemic). The analysis proceeded in two stages. First, we ran separate unadjusted models for each predictor variable to identify their crude associations with anemia. Variables that showed statistical significance (p < 0>
Statistical significance was set at p < 0>
Results:
Sociodemographic and Health Characteristics of the Study Population:
The study included 2,355 children aged 0-59 months, with a nearly equal distribution between males (50.4%) and females (49.6%). The largest proportion of children were in the 12-23 months age group (39.2%), followed by infants aged 0-11 months (21.7%), while children aged 24-35 months, 36-47 months, and 48-59 months constituted 12.2%, 14.6%, and 12.4% of the sample, respectively. The vast majority of children were singleton births (98.3%), with only 1.7?ing twins or triplets. Among those with recorded birth size data (n=1,720), approximately two-thirds (65.7%) were perceived as average size at birth, 23.5% as large, and 10.8% as small. Birth weight information was available for 1,720 children, with 95.1% having normal birth weight and 4.9% classified as low birth weight. Regarding birth order, 63.9% were subsequent children while 36.1% were index children. Recent childhood morbidities showed that 18.0% of children experienced diarrhea in the two weeks preceding the survey, 11.0% had fever, and 4.2% presented with symptoms of acute respiratory infection characterized by short, rapid breaths. Maternal characteristics revealed that over half of the mothers (54.6%) were aged 25-34 years, followed by those aged 15-24 years (35.6%) and 35 years or older (9.7%). Maternal nutritional status showed considerable variation, with 38.0% having normal BMI, 36.0?ing overweight, 20.6% obese, and 5.5% underweight. Maternal anemia was also highly prevalent, affecting 34.6% (n=815) of mothers, while 65.4% (n=1,538) were not anaemic. Educational attainment indicated that three-quarters of mothers (75.1%) had lower education levels, while 24.9% had higher education. At the household level, the majority of families were of medium size with 6- 10 members (59.5%), followed by small households with 0-5 members (21.1%) and large households with more than 10 members (19.4%). The sample was predominantly rural (60.8%) compared to urban (39.2%). Wealth distribution showed relative heterogeneity, with the richest index representing the largest group (29.9%), while the poorest, poorer, middle, and richer indexs accounted for 16.9%, 17.2%, 17.7%, and 18.4% of the sample, respectively. (Table-2)
Variables | Categories | Weighted frequency (N) | Percentage (%) | |||||
Child Factors | ||||||||
Child’s Age | 0-11 | 510 | 21.7% | |||||
| 12-23 | 922 | 39.2% | |||||
| 24-35 | 288 | 12.2% | |||||
| 36-47 | 344 | 14.6% | |||||
| 48-59 | 291 | 12.4% | |||||
Sex | Male | 1188 | 50.4% | |||||
| Female | 1167 | 49.6% | |||||
Birth Type | Singlet | 2314 | 98.3% | |||||
| Twin / triplets | 41 | 1.7% | |||||
Birth Size | Large | 405 | 23.5% | |||||
| Small | 185 | 10.8% | |||||
| Average | 1130 | 65.7% | |||||
Birth Weight | Low birthweight | 84 | 4.9% | |||||
| Normal Birthweight | 1636 | 95.1% | |||||
Birth Order | Index Child Subsequent Child | 850 1505 | 36.1% 63.9% | |||||
Food frequency | None | 217 | 16.4% | |||||
| 1 | 315 | 23.7% | |||||
| 2 | 628 | 47.3% | |||||
| 3 | 121 | 9.1% | |||||
| 4 | 24 | 1.8% | |||||
| 5 | 16 | 1.2% | |||||
| 6 | 5 | 0.4% | |||||
| 7 | 3 | 0.2% | |||||
ZVF consumption | No | 1504 | 63.9% | |||||
| Yes | 851 | 36.1% | |||||
Shortness of breaths | No | 2255 | 95.8% | |||||
| yes | 98 | 4.2% | |||||
Fever | No | 2094 | 88.9% | |||||
| yes | 258 | 11.0% | |||||
Diarrhea | No | 1928 | 81.9% | |||||
| Yes, last two weeks | 425 | 18.0% | |||||
Child Anemia | No Anemia | 1573 | 66.8% | |||||
| Anemia | 782 | 33.2% | |||||
Maternal Factors | ||||||||
Maternal age | 15-24 | 839 | 35.6% | |||||
| 25-34 | 1287 | 54.6% | |||||
| 35- or more | 229 | 9.7% | |||||
Maternal BMI | Normal | 894 | 38.0% | |||||
| Underweight | 129 | 5.5% | |||||
| Overweight | 848 | 36.0% | |||||
| obesity | 484 | 20.6% | |||||
Maternal anemia | Anemia | 815 | 34.6% | |||||
| No anemia | 1538 | 65.4% | |||||
Maternal education | Lower education | 1769 | 75.1% | |||||
| Higher education | 586 | 24.9% | |||||
Household Factors | ||||||||
Family size | Small size (0-5) | 496 | 21.1% | |||||
| Medium size (6-10) | 1401 | 59.5% | |||||
| Large size (10+) | 458 | 19.4% | |||||
Type of place of | Urban | 923 | 39.2% | |||||
residence | Rural | 1432 | 60.8% | |||||
Wealth index | Poorest | 398 | 16.9% | |||||
combined | Poorer | 404 | 17.2% | |||||
| Middle | 417 | 17.7% | |||||
| Richer | 433 | 18.4% | |||||
| Richest | 703 | 29.9% | |||||
Table 2: Demograhic Characteristics of health and Feeding profile of Tajikistan’s infants and young children 0-59mo.
Prevalence of Childhood Anemia , Feeding Frequency and ZVF Consumption:
The overall prevalence of anemia among children under five years in Tajikistan was 33.2% (n=782), indicating that approximately one-third of the study population was anaemic, while 66.8% (n=1,573) were non-anaemic. Analysis of child feeding practices revealed considerable variation in meal frequency among children. Among those for whom feeding data were available (n=1,329), the majority of children consumed solid, semi-solid, or soft foods twice daily (47.3%), followed by once daily (23.7%), while 16.4% reportedly consumed no such foods in the previous 24 hours. Smaller proportions consumed these foods three times (9.1%), four times (1.8%), five times (1.2%), six times (0.4%), or seven times (0.2%) daily, with 1.4% of caregivers unable to recall feeding frequency. Critically, the derived variable for ZVF consumption indicated that 36.1% (n=851) of children consumed no vegetables or fruits whatsoever in the 24 hours preceding the survey, while 63.9% (n=1,504) consumed at least one type of vegetable or fruit. (Figure-4)
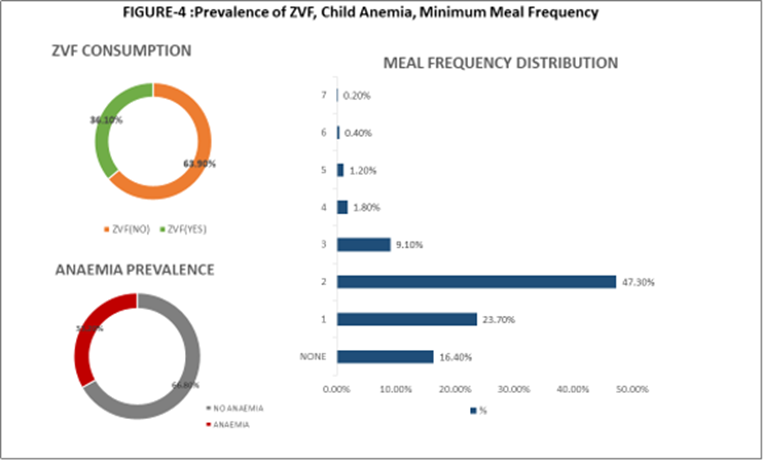
Figure 4: Prevalence OF ZVF, Child anemia, Minimum Meal Frequency.
Where, ZVF=Zero Vegetable or Fruit consumption.
Association Between ZVF Consumption and Childhood Anemia
In the unadjusted binomial logistic regression analysis from our study, ZVF consumption showed no statistically significant association with childhood anemia. However only marginally higher but non- significant odds of anemia were revealed when compared to those who consumed vegetables and fruits (OR = 1.03, 95% CI: 0.86 to 1.24), indicating no crude association between dietary diversity and anemia status. However, when ZVF consumption was examined in the multivariable adjusted model that controlled for months since last birth (M39), wealth index (V190), maternal anemia status (V457A), and perceived birth size (M18), the direction of association reversed, though it remained statistically non- significant that is had lower odds of anemia compared to those who consumed vegetables and fruits (OR = 0.85, 95% CI: 0.63 to 1.14), representing an approximate 15% non-significant reduction in anemia odds. The multivariable model demonstrated good overall fit [(chi square) χ² = 69.7, (degree of freedom) df = 9, p< 0 xss=removed> Variable Child’s Anemia Unadjusted odds (95% C.I) Adjusted odds (95% C.I) Dietary factors Vegetable and fruit consumption Yes No Ref 1.03(0.86 to 1.24) 0.85(0.63 to 1.14) Food frequency 0.88(0.79 to 0.98)* 0.86(0.76 to 0.98)* Child factors Child age 0-11 months 12-23 months 24-35 months 36-47 months 48-59 months Ref 1.29(1.03 to 1.62)* 0.97(0.67 to 1.24) 0.47(0.34 to 0.65)* 0.40(0.28 to 0.57)* Sex Male Female Ref 0.89(0.75 to 1.06) Birth type Singlet Twin/ triplet Ref 1.16(0.61 to 2.21) Birth order Index child Subsequent child Ref 1.12(0.94 to 1.34) Birth size Average Small Large Ref 1.68(1.23 to 2.31)* 1.18(0.94 to 1.50) 1.92(1.31 to 2.81)* 1.10(0.83 to 1.44) Birth weight Low birthweight Normal birthweight Ref 0.86(0.55 to 1.34) Diarrhea No Yes Ref 1.09(0.87 to 1.36) Fever No Yes Ref 1.13(0.86 to 1.48) Shortness of breaths No Yes Ref 1.17(0.77 to 1.79) Maternal factors Maternal age 15-24 years 25-34 years 35 years or more Ref 0.75(0.63 to 0.91)* 1.05(0.77 to 1.41) Maternal education Lower education Higher education Ref 1.05(0.86 to 1.28) Maternal BMI Normal Underweight Overweight Obese Ref 1.55(1.06 to 2.25)* 0.91(0.74 to 1.11) 1.05(0.83 to 1.33) Maternal anemia No anemia Anemia Ref 1.41(1.18 to 1.68)* 1.48(1.16 to 1.88)* Household and community factors Wealth index Poorest Poorer Middle Richer Richest Ref 0.86(0.65 to 1.15) 0.86(0.65 to 1.14) 0.73(0.55 to 0.97)* 0.50(0.38 to 0.65)* 0.72(0.49 to 1.06) 0.84(0.57 to 1.22) 0.53(0.36 to 0.78)* 0.39(0.27 to 0.56)* Family size Small Medium Large Ref 1.03(0.83 to 1.28) 0.84(0.63 to 1.10) Type of place of residence Urban Rural Ref 1.47(1.23 to 1.76)*
Where * means p<0>
Association of Significant Covariates with Childhood Anemia:
Several maternal, socioeconomic, and birth-related factors demonstrated significant associations with childhood anemia in unadjusted analyses, and these relationships persisted with varying magnitudes after adjustment in the multivariable model. Household wealth index exhibited a strong dose-response relationship with childhood anemia in both unadjusted and adjusted analyses. In the crude model, wealth status was highly significant [χ² = 34.6, df = 4, p < 0 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed>
Discussion:
Our study's null finding on the association between ZVF consumption and childhood anemia is novel for Tajikistan and Central Asia, where dietary-anemia links are understudied, with no prior DHS- based analyses focusing on ZVF(13). This result implies that while low vegetable/fruit intake is prevalent (36.1%), anemia in Tajik children is driven more by maternal and socioeconomic factors than this specific dietary element, directing resources toward targeted, non-dietary interventions. There is limited and fragmented studies on the specific association between fruit and vegetable (F&V) intake and anemia in infants and young children, particularly in contexts like rural Tajikistan with ZVF focus. Most available research is cross-sectional from LMICs in Africa (e.g., Uganda, Ethiopia, South Africa) or Asia (e.g., India), with only a handful directly isolating fruits and vegetables (F&V) rather than broader dietary diversity, and even fewer targeting under five years (0-59 months) or rural settings [22]. Non-heme iron in F&V offers low direct bioavailability (2-20?sorption) for infants and young children, contributing minimally to iron needs but crucially enhancing absorption from other plant sources via vitamin C, which can boost uptake by 2-6 times countering inhibitors, phytates in cereal-based diets. Across the studies we reviewed, low F&V consumption is generally associated with higher anemia risk in children, often through reduced vitamin C enhancement of non-heme iron absorption. Studies from Brazil (23) and Uganda (24) link low F&V intake to higher anemia prevalence in children, contrasting our findings of no significant ZVF-anemia association. However, results are mixed, some Ethiopian studies [25] show low or no direct correlation, aligning with our result, suggesting confounding by socioeconomic factors, infections, or staple-heavy diets that overshadow F&V's indirect benefits. In infant/young child contexts, F&V aren't strong direct iron sources but help mitigate Iron deficiency anemia IDA via diversity; protective effects are clearer with vitamin C-rich options,supported by an Indian evidence [26] that emphasized vitamin C-rich F&V's role in enhancing iron absorption, suggesting our Tajik children's traditional staple-heavy diets may dilute ZVF effects unless combined with bioavailable iron sources. South African data [27] ties low F&V nutrient density to anemia with rural-targeted diversity interventions. The null associations as the study’s case highlight the need for broader interventions beyond ZVF alone, such as addressing maternal anemia or rural access barriers. The protective effect of increased food frequency as revealed from our study is consistent with WHOs recommendations [28] on infant and young child feeding practices suggests that increasing the number of feeding opportunities can have a positive impact on nutritional status even in low-diversity diets potentially compensating for low ZVF consumption (28) (Table 3). The lack of ZVF-anemia association in our study may stem from methodological, biological, and cultural factors. Methodologically, we combined the three categories of anemia (mild, moderate, and severe) into a binary outcome (anemia vs. no anemia) for this analysis. One major drawback of this aggregation is that it might have obscured the actual effects of ZVF thus resulting in combining the more common, frequently multifactorial mild cases with the less common, nutrient-sensitive severe cases, as suggested by Shibeshi et al. 2024, [26]. Biologically, anemia’s high prevalence (33.2%) likely reflects iron deficiency from infections (18% diarrhoea, 11?ver) or non-heme iron diets(63.9%) [29]. Culturally, rural Tajik diets rely on high consumption of dairy products and starchy staples and a low intake of meat, eggs, and nutrient-dense foods [30]. Thus, inadequate intake of bioavailable iron (from animal sources) and persistent subclinical infections that prevent iron absorption and utilization may be the main causes of the anemia seen [29] thereby suggesting ZVF alone may not address the dominant iron deficiency drivers in this high-burden setting unless it is combined with greater availability and intake of other bioavailable iron sources. Despite the inconclusive nature of the primary hypothesis in our study, the adjusted model produced a number of extremely significant and robust risk factors for child anemia that are highly consistent with both domestic and international epidemiological research. The most compelling results emphasized the importance of maternal health. Maternal health strongly predicts child anemia in Tajikistan, particularly in rural settings. Children of anaemic mothers (34.6% prevalence; Table 1) faced significantly higher odds of anemia, reflecting intergenerational iron deficiency transmission [31,32]. This link is conciliated by inadequate iron stores passed from mother to fetus [33]. Specifically, the study by Siddiqui et al. (2024) suggested that maternal anemia during pregnancy adversely affects placental function and leads to decreased neonatal iron stores, which are vital for an infant's first 4-6 months of life and directly influence early anemia status [33]. Underweight mothers also increased child anemia risk, indicating chronic maternal nutritional deficiencies (34). Younger maternal age (15-24 years) was a risk factor compared to 25-34 years, possibly due to less experience in diverse feeding practices. Low maternal education (75.1% with lower education; Table 1) may further limit awareness of vegetable/fruit benefits in rural areas, where media exposure and extension services are scarce, though this was not significant in adjusted models [35]. These findings underscore the need for pre- and peri-conceptional maternal nutrition interventions to improve child outcomes in rural Tajikistan [36]. The null ZVF-anemia association of Tajikistan’s dietary context as interpreted above is linked with socioeconomic context, particularly in rural areas where majority of the children resides (60.8%) and face a higher anemia risk due to limited access to diverse foods and markets, especially during winter. Some studies also highlight that rural areas are also disproportionately affected by low maternal education and economic status [37]. This discrepancy is essentially related to access and infrastructure issues. In addition, poor clusters in urban areas also face similar issues with limited access to healthcare, clean water, and sanitation, stressing the point that the problem is systemic and linked to socioeconomic disparities all across Tajikistan [38]. Socioeconomic gradients further amplify this as children in the richest wealth index had significantly two thirds lower anemia odds compared to the poorest, suggesting ZVF may reflect poverty driven dietary constraints rather than directly causing anemia. Analysis of DHS data from several Sub- Saharan African countries, discovered that the household wealth index was repeatedly linked with lower odds of childhood anemia, independent of maternal and child-level factors [39]. Large family sizes (19.4%) of households with 10+ members; Table 2) in rural areas may further strain food resources, diluting access to perishables like fruits and vegetables, though this showed no significant adjusted association (Table 2). Younger children (12-23 months) and those with small birth size are particularly vulnerable during weaning, when ZVF introduction is critical but often inadequate in rural households [40].
Our analysis established that the youngest children (12-23months) are the most vulnerable, with anemia odds declining significantly for children aged 36 months and older. The period of rapid growth and the shift from reliance on maternal iron stores to supplemental feeding are the reasons for this age- related vulnerability, which has been extensively documented [40–42]. Small birth size was also a significant risk factor, which is in line with research showing that low birth weight and poor fetal growth are associated with lower iron endowment and a higher chance of iron deficiency anemia later in infancy [43,44].
Strengths and Limitations:
The main advantage of this study is that it employs the nationally representative DHS dataset, which enables the findings to be generalized to Tajikistan's entire infant and young child population. Additionally, multivariable logistic regression concurrently controls for a myriad of potential confounders. The main limitation is that the cross-sectional nature of the data prevents the inference of causality. As crucially discussed before, the aggregation of all anemia severity levels may have masked the true relationship between specific dietary deficiencies and the more severe forms of the condition thus limiting generalizability. Finally, the dietary data relies on maternal recall, which is subject to recall bias
Conclusions:
This study examined associations between ZVF consumption and anemia among 2,355 children aged 0-59 months in Tajikistan using 2023 Demographic and Health Survey data. The null finding of our study that is no significant ZVF-anemia association despite 36.1% prevalence of children with zero consumption is methodologically robust and regionally novel, representing the first nationally representative examination of this relationship in Central Asia. This challenges dietary centric approaches common in LMIC nutrition programs. Instead, maternal(intergenerational) and socioeconomic factors emerged as primary drivers, maternal anemia increased child anemia odds by 48%, small birth size nearly doubled risk, and wealth disparities showed pronounced gradients with the richest index having 60% lower anemia odds than the poorest. These findings indicate that effective childhood anemia reduction in Tajikistan and potentially across Central Asia requires SDG aligned integrated interventions addressing maternal nutrition during preconception and pregnancy, improved antenatal care to prevent intrauterine growth restriction, poverty alleviation strategies enhancing food security, and promotion of appropriate feeding frequency.
Conclusions:
This study examined associations between ZVF consumption and anemia among 2,355 children aged 0-59 months in Tajikistan using 2023 Demographic and Health Survey data. The null finding of our study that is no significant ZVF-anemia association despite 36.1% prevalence of children with zero consumption is methodologically robust and regionally novel, representing the first nationally representative examination of this relationship in Central Asia. This challenges dietary centric approaches common in LMIC nutrition programs. Instead, maternal(intergenerational) and socioeconomic factors emerged as primary drivers, maternal anemia increased child anemia odds by 48%, small birth size nearly doubled risk, and wealth disparities showed pronounced gradients with the richest index having 60% lower anemia odds than the poorest. These findings indicate that effective childhood anemia reduction in Tajikistan and potentially across Central Asia requires SDG aligned integrated interventions addressing maternal nutrition during preconception and pregnancy, improved antenatal care to prevent intrauterine growth restriction, poverty alleviation strategies enhancing food security, and promotion of appropriate feeding frequency.
Future Research:
Future research should employ longitudinal designs and comprehensive dietary assessments to elucidate complex interactions between dietary quality, infectious diseases, and socioeconomic determinants in childhood anemia etiology.
Policy Implications:
Our findings provide actionable, evidence-based guidance for national nutrition programs working toward SDG targets in Central Asia and similar LMIC contexts. The Immediate Priority Actions must be given to maternal anemia screening and treatment in all antenatal care units, with free iron-folic acid supplementation for pregnant and lactating women there by Contributing to SDG 3.1(maternal health), 3.2(child health). This must be paralled with targeted cash or food vouchers transfer for the poorest wealth index thereby contributing to SDG 1.2(poverty reduction), 2.1 (food security). Optimal feeding frequency promotion must be done by Community health worker particularly in rural areas which contribute to SDG 2.2(malnutrition). In the intermediate term enhanced antenatal care quality with ultrasound access and fetal growth monitoring to identify and manage intrauterine growth restriction may require equipment investments and sonographer training in rural health facilities. This contributes to SDG
3.1 (maternal mortality reduction), 3.8 (universal health coverage). In the long term agricultural diversification policies must be employed beyond staple grains thus contributing to SDG 2.3 (agricultural productivity), 2.4 (sustainable food production). As maternal education and wealth showed protective effects, long-term investment can be done for next-generation outcomes.
Abbreviations
ZVF: ZVF intake
df : Degree of Freedom X2 : Chi square
CI: confidence interval OR: odds ratio
MMF: minimum meal frequency
MRM: Micronutrient Related Malnutrition SDGs: Sustainable Development Goals WHO: World Health Organization
UNICEF: United Nations International Children Emergency Fund NNS: National Nutrition Survey
PSU: Primary Sampling Units EB: Enumeration Blocks
LMICs: Lower- and Middle-Income Countries. CI: Confidence Interval
OR: Odds Ratio
AIC: Akaike Information Criteria BIC: Bayesian Information Criteria VIF: Variance Inflation Factors
Declarations/Statements:
Authors’ contribution: AK: Conceptualization, data management, data analysis, reviewing, editing, and supervision. NI: Introduction writing and helped in reviewing of manuscript. YR: Discussion writing and helped in reviewing of manuscript. SA: Result writing and helped in reviewing and editing. BA: Original draft writing, methodology section, visualization, and formatting of the manuscript also assisted AK in data analysis and in final review of the manuscript.
Ethics approval: In this study, an ethical approval waiver was granted because the data used was de- identified, and the research team had no direct contact with the study population. Consequently, individual participant consent and ethical approval of this study was not required. However, the data in each DHS was collected following ethical principles of Helsinki’s declaration.
Consent to participate: In this study, the research team utilized de-identified data obtained from the DHS repository. This data does not contain any information that could be used to identify or trace individual participants. Consequently, individual participant consent was not required by the primary research team for this study.
Consent for publication: In this research, the DHS data of Tajikistan was used. To access this data, a formal application was submitted, which included our intention to publish the findings. The DHS data archivist provided us with a letter granting permission to publish our research, with the condition that we acknowledge the DHS data repository in the acknowledgments section of the publication
Data Availability: The data that support the findings of this study are openly available in The DHS Program at https://dhsprogram.com/.
Conflict of interest: All authors declare no conflict of interest.
Funding: This research received no specific grant from any funding agency for research publication and dissemination purposes.
Acknowledgement: We would like to acknowledge the data archivist of the Demographic and Health Surveys [DHS] Program, who provided access to the dataset of DHS implemented in Tajikistan for analysis.
Supplementary file: The supplementary file has two tables, which presents the individual variables of fruit and vegetables and derived variable from them. zvf folder\Supplementary file.docx
Supplementary file 1:
Feeding Variables for infants and child(6-59mo) from DHS Tajikistan 2023
Child FeedingVariables | Variables |
Gave child fruitjuice/fruit flavoured drinks | V410 |
Gave child any other vegetables | V414A |
Gave child plantains,potatoes, cassava, or other tubers | V414F |
Gave child pumpkin, carrots, squash (yellow or orangeinside) | V414I |
Gave childany dark greenleafy vegetables | V414J |
Gave child mangoes, papayas, other vitamin A fruits | V414K |
Gave childany other fruits | V414L |
Supplementary file 2:
Derived Feeding Variable for infants and child (6-59mo) from DHS Tajikistan 2023
Derived Feeding Variable | Category | Feeding Variable |
ZVF1 | 0=No consumption 1=Consumed | V410,V414,V414F,V414I,V414J,V414K,V414L |
References
- WHO. Anemia. WHO headquaters Geneva,Switzerland: World Health Organization; 2025 Feb [cited 2025 Oct 11]. Available from: https://www.who.int/news-room/fact-sheets/detail/anemia
View at Publisher | View at Google Scholar - Crivelli M, Wyss K, Grize L, Matthys B, Aebi T, Zemp E. Are overweight and obesity in children risk factors for anemia in early childhood? Results from a national nutrition survey in Tajikistan. Int J Public Health. 2018 May;63(4):491–9.
View at Publisher | View at Google Scholar - UNICEF. Publications Archives. 2025 [cited 2025 Oct 11]. Available from: https://data.unicef.org/resources/resource-type/publications/
View at Publisher | View at Google Scholar - WHO. Anemia in women and children. Geneva,Switzerland: WHO headquaters; 2025ed [cited 2025 Oct 11]. (Global Health Observatory data). Available from: https://www.who.int/data/gho/data/themes/topics/anemia_in_women_and_children
View at Publisher | View at Google Scholar - Chaparro CM, Suchdev PS. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann N Y Acad Sci. 2019 Aug;1450(1):15–31.
View at Publisher | View at Google Scholar - Stevens GA, Beal T, Mbuya MNN, Luo H, Neufeld LM, Global Micronutrient Deficiencies Research Group. Micronutrient deficiencies among preschool-aged children and women of reproductive age worldwide: a pooled analysis of individual-level data from population-representative surveys. Lancet Glob Health. 2022 Nov;10(11):e1590–9.
View at Publisher | View at Google Scholar - Zimmermann MB, Hurrell RF. Nutritional iron deficiency. Lancet Lond Engl. 2007 Aug 11;370(9586):511–20.
View at Publisher | View at Google Scholar - WHO. Indicators for assessing infant and young child feeding practices: definitions and measurement methods . Geneva: World Health Organization and the United Nations Children’s Fund (UNICEF); 2021 [cited 2025 Oct 22]. 122 p. Available from: https://www.who.int/publications/i/item/9789240018389
View at Publisher | View at Google Scholar - Khaliq A, Wraith D, Miller Y, Nambiar S. Association of Infant Feeding Indicators and Infant Feeding Practices with Coexisting Forms of Malnutrition in Children under Six Months of Age. Nutrients. 2022 Oct 12;14(20):4242.
View at Publisher | View at Google Scholar - USAID team. USAID Multi-Sectoral Nutrition Strategy 2014-2025 - World | ReliefWeb . 1300 Pennsylvania Avenue, NW Washington, DC 20523: U.S. Agency for International Development; 2014 May [cited 2025 Oct 12] p. 58. Available from: https://reliefweb.int/report/world/usaid-multi-sectoral- nutrition-strategy-2014-2025
View at Publisher | View at Google Scholar - Park K, Kersey M, Geppert J, Story M, Cutts D, Himes JH. Household food insecurity is a risk factor for iron-deficiency anemia in a multi-ethnic, low-income sample of infants and toddlers. Public Health Nutr. 2009 Nov;12(11):2120–8.
View at Publisher | View at Google Scholar - Allen CK, Assaf S, Namaste S, Benedict RK. Estimates and trends of ZVF consumption among children aged 6-23 months in 64 countries. PLOS Glob Public Health. 2023;3(6):e0001662.
View at Publisher | View at Google Scholar - Barth-Jaeggi T, Zandberg L, Bahruddinov M, Kiefer S, Rahmarulloev S, Wyss K. Nutritional status of Tajik children and women: Transition towards a double burden of malnutrition. Matern Child Nutr. 2019 Nov 8;16(2):e12886.
View at Publisher | View at Google Scholar - Mantadakis E, Chatzimichael E, Zikidou P. Iron Deficiency Anemia in Children Residing in High and Low-Income Countries: Risk Factors, Prevention, Diagnosis and Therapy. Mediterr J Hematol Infect Dis. 2020;12(1):e2020041.
View at Publisher | View at Google Scholar - Rahman MS, Mushfiquee M, Masud MS, Howlader T. Association between malnutrition and anemia in under-five children and women of reproductive age: Evidence from Bangladesh Demographic and Health Survey 2011. PloS One. 2019;14(7):e0219170.
View at Publisher | View at Google Scholar - Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007 Oct 20;335(7624):806–8.
View at Publisher | View at Google Scholar - Tajikistan. Tajikistan Demographic and Health Survey 2023 . 2025 Aug [cited 2025 Oct 11]. Available from: https://dhsprogram.com/publications/publication-FR392-DHS-Final-Reports.cfm
View at Publisher | View at Google Scholar - Analyzing DHS Data . [cited 2025 Oct 11]. Available from: https://dhsprogram.com/data/Guide-to- DHS-Statistics/Analyzing_DHS_Data.htm
View at Publisher | View at Google Scholar - Khaliq A. Determinants and distribution of coexisting forms of malnutrition among neonates, infants and children of Pakistan [QUT Thesis (PhD by Publication)]. Queensland University of Technology; 2023 [cited 2025 Oct 22]. Available from: https://eprints.qut.edu.au/241461/
View at Publisher | View at Google Scholar - WHO. Haemoglobin concentrations for the diagnosis of anemia and assessment of severity . 2011 [cited 2025 Oct 11] p. 7. Report No.: WHO/NMH/NHD/MNM/11.1. Available from: https://www.who.int/publications/i/item/WHO-NMH-NHD-MNM-11.1
View at Publisher | View at Google Scholar - Agency on Statistics under the President of the Republic of Tajikistan, Ministry of Health and Social Protection of the Population of the Republic of Tajikistan, ICF. Tajikistan Demographic and Health Survey 2023 . Dushanbe, Republic of Tajikistan and Rockville, Maryland, USA: Agency on Statistics under the President of the Republic of Tajikistan and ICF; 2025. (FR392). Available from: https://www.dhsprogram.com/pubs/pdf/FR392/FR392.pdf
View at Publisher | View at Google Scholar - Li H, Moosavian SP, Ghanbari N, Mirlohi SH, Rahimlou M. Association of dietary diversity and odds of anemia in children and adolescents: a systematic review and meta-analysis of observational studies. BMC Nutr. 2025 Apr 22;11(1):83.
View at Publisher | View at Google Scholar - Augusto RA, Cobayashi F, Cardoso MA, ACTION Study Team. Associations between low consumption of fruits and vegetables and nutritional deficiencies in Brazilian schoolchildren. Public Health Nutr. 2015 Apr;18(5):927–35.
View at Publisher | View at Google Scholar - Kajoba D, Egesa WI, Muyombya S, Ortiz YA, Nduwimana M, Ndeezi G. Prevalence and Factors Associated with Iron Deficiency Anemia among Children Aged 6-23 Months in Southwestern Uganda. Int J Pediatr. 2024;2024:6663774.
View at Publisher | View at Google Scholar - Gashu D, Stoecker BJ, Bougma K, Adish A, Haki GD, Marquis GS. Stunting, selenium deficiency and anemia are associated with poor cognitive performance in preschool children from rural Ethiopia. Nutr
View at Publisher | View at Google Scholar - J. 2016 Apr 12;15:38.
View at Publisher | View at Google Scholar - Shibeshi AH, Mare KU, Kase BF, Wubshet BZ, Tebeje TM, Asgedom YS, et al. The effect of dietary diversity on anemia levels among children 6-23 months in sub-Saharan Africa: A multilevel ordinal logistic regression model. PloS One. 2024;19(5):e0298647.
View at Publisher | View at Google Scholar - Visser J, McLachlan MH, Maayan N, Garner P. Community-based supplementary feeding for food insecure, vulnerable and malnourished populations - an overview of systematic reviews. Cochrane Database Syst Rev. 2018 Nov 9;11(11):CD010578.
View at Publisher | View at Google Scholar - WHO. Guideline for complementary feeding of infants and young children 6–23 months of age . Geneva: World Health Organization; 2023 [cited 2025 Oct 15]. (WHO Guidelines Approved by the Guidelines Review Committee). Available from: http://www.ncbi.nlm.nih.gov/books/NBK596427/
View at Publisher | View at Google Scholar - Tako E. (PDF) Fe Deficiency, Dietary Bioavailbility and Absorption . secial edition. Basel, Switzerland: MDPI; 2018 [cited 2025 Oct 15]. 216 p. Available from: https://www.researchgate.net/publication/327843408_Fe_Deficiency_Dietary_Bioavailbility_and_Abso rption
View at Publisher | View at Google Scholar - Wood EA, McNamara K, Kowalewska A, Ludgate N. Household decision-making around food in rural Tajikistan: a cross-sectional study to help extension workers in the field. Food Nutr Res . 2018 Mar 15 [cited 2025 Oct 15]; Available from: https://foodandnutritionresearch.net/index.php/fnr/article/view/1330
View at Publisher | View at Google Scholar - Tsamantioti E, Alfvén T, Hossin MZ, Razaz N. Maternal anemia and risk of neonatal and infant mortality in low- and middle-income countries: a secondary analysis of 45 national datasets. BMJ Glob Health. 2025 Mar 3;10(3):e014654.
View at Publisher | View at Google Scholar - Zhao B, Sun M, Wu T, Li J, Shi H, Wei Y. The association between maternal anemia and neonatal anemia: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2024 Oct 18;24(1):677.
View at Publisher | View at Google Scholar - Siddiqui DSA, Begum DL, Bibi DR, Ali DSM, Tagar DMR, Hassan6 DJ. MATERNAL ANEMIA IN PREGNANCY AND ITS EFFECT ON PLACENTAL FUNCTION AND NEONATAL IRON STORES: A CROSS-
View at Publisher | View at Google Scholar - SECTIONAL ANALYSIS. J Popul Ther Clin Pharmacol. 2024 Dec 22;31(11):2071–8.
View at Publisher | View at Google Scholar - Patel A, Prakash AA, Das PK, Gupta S, Pusdekar YV, Hibberd PL. Maternal anemia and underweight as determinants of pregnancy outcomes: cohort study in eastern rural Maharashtra, India. BMJ Open. 2018 Aug 1;8(8):e021623.
View at Publisher | View at Google Scholar - Alem AZ, Efendi F, McKenna L, Felipe-Dimog EB, Chilot D, Tonapa SI, et al. Prevalence and factors associated with anemia in women of reproductive age across low- and middle-income countries based on national data. Sci Rep. 2023 Nov 20;13(1):20335.
View at Publisher | View at Google Scholar - Aweke MN, Yitageasu G, Agimas MC, Yismaw GA, Baffa LD, Alemu GG. Co-occurrence of maternal anemia and child undernutrition in Ethiopia: multilevel analysis of analysis of EDHS data (2005–2016). BMC Public Health. 2025 Aug 11;25(1):2722.
View at Publisher | View at Google Scholar - Osborne A, Adeleye K, Bangura C, Wongnaah FG. Trends and inequalities in anemia prevalence among children aged 6–59 months in Ghana, 2003–2022. Int J Equity Health. 2024 Nov 8;23(1):231.
View at Publisher | View at Google Scholar - Tebeje TM, Aregu MB, Asgedom YS, Gebrekidan AY, Abebe M. From poverty to health: intraurban inequalities in child health indicators in low-income and middle-income countries during the SDG era. BMJ Glob Health. 2025 Aug 14;10(8):e019134.
View at Publisher | View at Google Scholar - Moschovis PP, Wiens MO, Arlington L, Antsygina O, Hayden D, Dzik W, et al. Individual, maternal and household risk factors for anemia among young children in sub-Saharan Africa: a cross-sectional study. BMJ Open. 2018 May 14;8(5):e019654.
View at Publisher | View at Google Scholar - Miniello VL, Verga MC, Miniello A, Di Mauro C, Diaferio L, Francavilla R. Complementary Feeding and Iron Status: “The Unbearable Lightness of Being” Infants. Nutrients. 2021 Nov 23;13(12):4201.
View at Publisher | View at Google Scholar - Qasem W, Fenton T, Friel J. Age of introduction of first complementary feeding for infants: a systematic review. BMC Pediatr. 2015 Sep 2;15:107.
View at Publisher | View at Google Scholar - Dewey KG. The challenge of meeting nutrient needs of infants and young children during the period of complementary feeding: an evolutionary perspective. J Nutr. 2013 Dec;143(12):2050–4.
View at Publisher | View at Google Scholar - Li N, An H, Jin M, Li Z, Zhang Y, Zhang L, et al. Association of Infants Small for Gestational Age with Anemia under Five Years Old in Two Large Longitudinal Chinese Birth Cohorts. Nutrients. 2022 Feb 27;14(5):1006.
View at Publisher | View at Google Scholar - Liu X, Liu X, Yang Z, Li Z, Zhang L, Zhang Y, et al. The Association of Infant Birth Sizes and Anemia under Five Years Old: A Population-Based Prospective Cohort Study in China. Nutrients. 2024 Jun 7;16(12):1796.
View at Publisher | View at Google Scholar
