

Case Report | DOI: https://doi.org/10.31579/2834-8761/038
Managing Hormonal Disruption in Perimenopausal Syndrome
- K. Suresh *
Public Health Consultant and Family Physician Bengaluru and Karnataka State Rural Development and Panchayat Raj University, GADAG, Karnataka, India 582101.
*Corresponding Author: K. Suresh, 70022, Altamura (Bari), Italy; Via Della Conciliazione, 65 Cap 74014 Laterza (Ta) Italy.
Citation: K. Suresh, Bernardino, (2023), Managing Hormonal Disruption in Perimenopausal Syndrome, Clinical Endocrinology and Metabolism,3(1), DOI: 10.31579/2834-8761/038
Copyright: © 2023, K. Suresh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 December 2023 | Accepted: 29 December 2023 | Published: 04 January 2024
Keywords: perimenopausal symptoms; contraceptive use; luteinizing hormone (lh) or follicle stimulating hormone (fsh); anovular menstrual cycles; belly bulging; mood swings
Abstract
Natural menopause is a transition phase from the reproductive to the nonreproductive phase in a woman's life. It occurs with the final menstrual period after 12 months of amenorrhea for which there are no obvious pathological and physiological causes. The menopausal transition is characterized by menstrual cycle variability and fluctuations in reproductive hormone levels, that sets the stage for aging and noncommunicable diseases.
Contraceptive induced perimenopause syndrome is getting attention in recent year, as taking birth control pills can prevent the body from recognizing the natural decline in oestrogen and progesterone that occurs during menopause. After stopping hormonal birth control for a few months, woman can notice symptoms like irregular periods, hot flashes, night sweats and mood changes. Many women do not have periods when using a pill containing oestrogen and progestin until they stop contraception. Experiencing amenorrhea (the absence of menstruation and ovulation) or anovulation (the presence of menstruation but absence of ovulation) is usually due to Low luteinizing hormone (LH) or follicle stimulating hormone (FSH) levels. Ovulation Induction Treatment (OIT) is a fertility reviving process with medications to increase the number of eggs produced or regulate or cause ovulation.
Common physical symptoms of perimenopause include- hot flushes, when the lady has sudden feelings of hot or cold in her face, neck and chest which makes her dizzy, difficulty sleeping, night sweats and make her feel tired and irritable during the day. She may have menstrual periods every two weeks, gaining weight, aversion towards sex etc. Weight gain continues at the rate of 1kg. each year, usually gaining weight around the abdomen (belly bulging), rather than the hips and thighs. The individual response varies due to genetic, cultural, lifestyle, socioeconomic, education, behavioural and dietary factors.
Peri menopausal age group is not covered under any of the national health programmes. There is lack of standard data related to peri menopausal women in India, especially in rural area, where lack of services has been a huge issue and where most of women of this age group reside and are suffering silently!
This article is based on 3 cases of natural cases and one Contraceptive induced Perimenopausal case the author has managed in recent years.
Materials and Methods: This article is based on 2 urban and 2 rural case experiences each one giving different perspective of the condition. The social support in terms of sharing their emotions and household chores become more important. In case of contraceptive induced perimenopause Ovulation Induction Therapy has a role to revie fertility.
Introduction
Natural or spontaneous menopause is a transition phase from the reproductive to the nonreproductive phase in a woman's life. It occurs with the final menstrual period which is known to occur after 12 months of amenorrhea for which there are no obvious pathological and physiological causes. It sets the stage for aging and accelerates the process of noncommunicable diseases. Middle age is one of the most important phases in every one’s life, more so for women to cope up with perimenopausal syndrome.
Peri menopausal age group is not covered under any of the national health programmes. There is lack of standard data related to peri menopausal women in India, especially in rural area, where lack of services has been a huge issue and where most of women of this age group are expected to reside. The symptoms of menopause are reflected not only in the female genital tract but also in the skeletal, cardiovascular, and psychological system. With increasing life expectancy, women are likely to face long periods of menopause accounting to approximately one-third of their age. This has resulted in higher burden of morbidities.
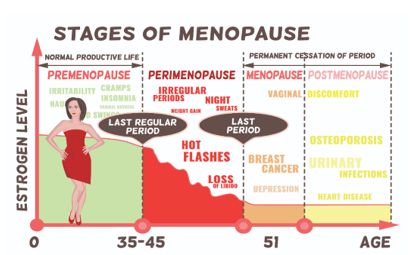
Perimenopause describes the period before menopause, when a woman’s body experiences hormonal changes that finally lead to the end of menstrual cycles. Though it starts a year or two before menopause around early 40’s, but some women notice changes as early as their mid-30s or even earlier. Completing menopause before age 40 is called premature menopause [3]. For most women it lasts four to eight years, for some this phase is for only a few months. Or a year or two. The term perimenopause simply describes the time when woman’s cycles are not predictable. The best predictor of when lady will have her final period will be is the age at which her mother entered menopause. The menopausal transition is characterized by menstrual cycle variability and fluctuations in reproductive hormone levels. The individual response to menopause varies considerably due to genetic, cultural, lifestyle, socioeconomic, education, behavioural and dietary factors [2].
A newer category of perimenopause is being observed among woman who take birth control pills, which can prevent the body from recognizing the natural decline in oestrogen and progesterone that occurs during menopause. As a result, the symptoms that a person typically experiences during perimenopause may not be as apparent. After stopping hormonal birth control for a few months, woman can notice symptoms like irregular periods, hot flashes, night sweats and mood changes. Many women do not have periods when using a pill containing oestrogen and progestin every day until the patent stops contraception.
The prevalence of perimenopausal syndrome in the different age groups (1.79%, 7.98%, 13.33%, and 17.54% in the 40–45, 45–50, 50–55, and 55–60 age groups, respectively) demonstrated a statistically significant difference (P < 0>
Case Reports:
1.A PM woman with no one to share her grief: Mrs Sita 54-year-old urban resident the perimenopausal phase became very difficult because she had no one with whom to share her grief over the death of her husband. She complained of frequent headaches and joint pains, for two years, she suffered from heavy bleeding and painful menstruation. It was difficult, and painful. Her husband died three months back, her son is busy with his own life and daughter-in-law doesn’t care her.
2.Geeta Keeps Fighting & exhausted: Ms. Geeta a 59, rural resident remembers her perimenopause experience and calls it a “suffering.” She mentions her frequent fights with her husband and even her son. She expresses that she suffered a lot, as she had very heavy bleeding which was unmanageable. She tried many home-remedies, but nothing worked. She was unable to sleep, fully exhausted and didn’t want to talk to anyone, became anxious, used to get irritated over small things, had frequent fights with her husband and even with her son. She groused that they don’t understand what a woman is going through, and she could not explain them. It was a difficult time.
3.Enjoying with Daughter-in-laws Support: Another Gita, a 52, rural resident also had heavy bleeding before I stopped menstruating, but felt it is normal! every woman must go through this! She appreciated her daughter-in-law as she managed all the household chores at that time. After menopause daughter in law works and she looks after her grandchildren, and feels she is free and enjoying life.
- Contraceptive Induced Perimenopause: Thirty-year-old young married lady with a daughter of 6 years, had used oral contraceptive for postponing her second pregnancy for about 3 years followed by two shots of injectable contraceptive at 3 months interval, stopped her contraceptive use for more than 18 months, making all efforts hasn’t been able to conceive. Since early 2024 her periods have been irregular, interval between periods increased for 28 days to 30-35 days and every time their scanty white discharge followed by a day’s spotting. Since a year she has put on 10kg of weight, mostly around her waist. Her mother-in-law complains of her mood swings. The coupe is worried and the goal of inducing ovulation is to plan second pregnancy.
Discussions:
The first sign of perimenopause typically is a disruption of menstrual cycle. For many women, if their period starts earlier or later than normal, for example, instead of normal 28 days, her period could come as early as 21 or as late as 35 days. Some women start skipping months entirely and then experience heavier-than-normal periods when they do have them. Mood swings, tiredness, weakness, weight gain, and hot flush may also be experienced. It also effects sexual health leading to vaginal dryness, burning in Vaginal area, decreased libido and failure to climax. It can lead to complications due to a deficiency of Vitamin B12 and other vitamins. Bruning in the vagina may confuse the primary care doctor to consider it as Urinary tract infection and try multiple antibiotics with no benefit.
Common physical symptoms of perimenopause include- hot flushes, when the lady has sudden feelings of hot or cold in her face, neck and chest which makes her dizzy, difficulty sleeping, night sweats and make her feel tired and irritable during the day. She may have menstrual periods every two weeks, gaining weight, aversion towards sex etc. Weight gain continues at the rate of 1kg. each year. The hormonal changes of the perimenopause tend to make women gain weight around the abdomen, rather than the hips and thighs. It is not just hormonal changes alone that cause the weight gain, but also aging, as well as lifestyle and genetic factors.
Most women get overwhelmed as their body is behaving differently, though medical examination or even though biomarkers indicate all is well, and the patient is more confused and anxious and even a general practitioner keeps guessing. Some women who used to do exercises or Gym happily now just don’t find like working out and body is not feeling right. Although it's unlikely, the lady can get pregnant during perimenopause, as she still has periods but notice symptoms such as hot flushes, night sweats and mood swings. Her body will still be releasing eggs ovulating and pregnancy is a possibility.
It is necessary to get blood tests to check hormone and Vitamin levels. The most reliable blood test looks for high levels of follicle-stimulating hormone (FSH), released by the pituitary gland in response to declining oestrogen stores. But if a woman is taking birth-control pills, she must stop for at least 3 menstrual cycles after coming off hormonal contraception before taking a test to get accurate results. Hitting Gym or any other exercise routine like weight training, cardio, kickboxing, or yoga, despite dis-interest will help over time keeping the stress levels in check. People should try to incorporate foods high in fiber and antioxidants in their diet, limit salt, sugar, and processed foods. Experts agree that it's best to get calcium from foods like milk, yogurt, cheese, sardines, salmon, and leafy greens. They will benefit from eating five or six smaller meals each day and reduce weight eating more fruits, vegetables. Systemic estrogenic therapy in the forms of pills, skin patch, spray, gel, or cream remains the most effective option for relieving perimenopausal hot flashes and night sweats. Hormone therapy is used to help with hot flashes that affect quality of life. It also helps redistribute the fat that accumulates around the centre of the abdomen called visceral fat. Hormone therapy also helps the lady manage her weight by improving sleep, more activities and healthier lifestyle changes.
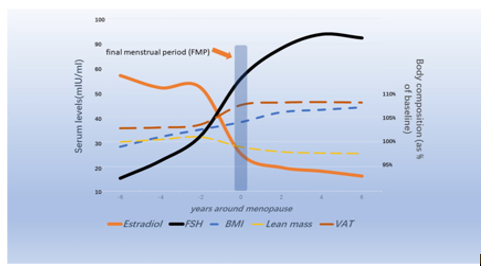
Contraceptives induced Perimenopause: Oestrogen- and progesterone-containing oral contraceptives inhibit the release of luteinizing hormone-releasing hormone, which suppresses levels of follicle stimulating hormone (FSH) and luteinizing hormone (LH), thus preventing follicular development and ovulation. FSH begins to increase 6 years before menopause, and more rapidly increased 2 years before the final menstrual period and stabilized 2 years after menopause. Epidemiological studies have shown that high levels of follicle-stimulating hormone (FSH) in perimenopausal women are closely associated with changes in body composition, central obesity, and cognitive decline. Exogenous FSH causes growth and proliferation of adipose, whereas blockage of the FSH signalling pathway leads to decline in adipose. Mechanistically, FSH, FSH receptor (FSHR), G protein coupling, gene mutation and other pathways are involved in adipogenesis and cognitive impairment. Further understanding of the exact mechanisms of FSH aggravating obesity and cognitive impairment may provide a new perspective for promoting healthy aging in menopausal women. As for cognitive impairment, clinical studies found that high levels of FSH are closely related to brain structural and functional damage. Future research is needed to demonstrate how fat formation caused by high levels of FSH during menopause may directly or indirectly impair cognitive function, such as inflammation, mitochondrial damage, oxidative stress, and autophagy changes. In clinical research, since the efficacy and side effects of hormone replacement therapy are not fully understood, lifestyle management, such as exercise, diet, and mood management, should be an important means to prevent lipo-metabolic disturbance and cognitive impairment in postmenopausal women, as well as some typical menopausal diseases, such as postmenopausal osteoporosis, anxiety, and depression.


Nearly 4% of Indian women experience signs of menopause between 29 and 34 years of age, said a survey conducted by The Institute for Social and Economic Change (ISEC) in 2016. The figure goes up to 8 per cent in the case of women between 35 and 39 years of age.
It is important for women to keep a track of their periods and the symptoms so that they can discuss it with their doctor if there be any aberration from the normal for geographical and familial trends. Basic investigations begin from tests of assessing thyroid condition which causes hormonal imbalance. The next tests are Follicle Stimulating Hormone (FSH), Oestrogen, and Prolactin (PL), Anti Mullerian hormone (AMH) levels. As FSH and PL levels increase, and oestrogen levels and PL decrease signal approaching perimenopause and menopause. Other investigations include scans, to check the thickness of the endometrium. If the woman is not getting periods during perimenopause, the inner lining should not be very thick. If it is thick, they conduct other tests like hysteroscopy and D&C, pap-smear tests to rule out abnormalities like cervical cancer.
A cross-sectional study of 1062 women aged 40 to 60 years of 3 communities of Shanghai in 2016, reported, the prevalence of perimenopausal syndrome (PMS- 10.92%), depression (25.99%), and anxiety (12.62%) respectively. The differences in the prevalence & severity of PMS, in the prevalence of depression, and in the severity of anxiety in different age groups were statistically significant (P < 0.001, P = 0.028, P = 0.003, P = 0.002, respectively). The relationships between perimenopausal syndrome and mood disorders were strong and positive (P < 0.001). Age, employment status, personality characteristics, menstruation, and constipation were risk factors for perimenopausal syndrome, but monthly household income was a protective factor. Disharmonious family relationships, irregular menstruation, the need to conceal delayed menstruation, constipation, and severity of perimenopausal syndrome were harmful to depression. For anxiety, attitudes to children status, caesarean section times, and constipation were risk factors [3].
A community based cross-sectional study of 400 middle aged women from April 2018 to March 2019 by random sampling technique, in Haryana India, using the menopause rating scale reported a Prevalence of menopausal symptoms be 87.7%. Majority of the study subjects had anxiety (80%), followed by physical and mental exhaustion (71.5%), sleep problem (61.2%), irritability (60.7%), Joint and muscular discomfort (56%) and heart problems (54%). The most classical symptom of menopause i.e., hot flushes were reported in 36.7%. The mean age of menopause was 47.53 standard deviation 4.5 years. Statistically significant difference was seen for the mean score of few symptoms i.e., hot flushes, sweating (P < 0>
A community based study of 350 women rural women in Bagalkot district, Karnataka reported 84% of the women in study had poor sleep, 75.4% of women had feeling of panic, feeling of sadness was seen in 38.3%of women, 56.6% of women felt anxious, 57.7% of women had lost interest in everyday things, 70.3% of women felt palpitations, 54.7 said that they did not enjoy everyday things, 16.6% of women felt that life was not worth living, 58.9% of women felt tensed, and 56.7% of women did not have good appetite [5].
Contraceptive Induced Perimenopause: Taking birth control pills can prevent the body from recognizing the natural decline in oestrogen and progesterone that occurs during menopause. After stopping hormonal birth control for a few months, woman can notice symptoms like irregular periods, hot flashes, night sweats and mood changes. Many women do not have periods when using a pill containing oestrogen and progestin every day until the patient stops contraception.
In patients with chronic anovulation, cyclic hormonal contraception can restore menstrual bleeding. Any progestin therapy can reduce the long-term risks of unopposed Oestrogen, and clomiphene citrate can help with ovulation for patients desiring fertility. There are several methods that may help to balance hormones, which in turn help to increase the odds of ovulation, that include getting plenty of sleep, maintaining a healthy diet, exercising regularly, minimizing stress levels, supplements, of folates, omega-3 fatty acids, and iron.
Experiencing amenorrhea (the absence of menstruation and ovulation) or anovulation (the presence of menstruation but absence of ovulation) is usually due to Low luteinizing hormone (LH) or follicle stimulating hormone (FSH) levels. Thyroid disease, Polycystic Ovary Syndrome (PCOS), Hyperprolactinemia, Excessive weight loss/gain and excessive exercising. In Indian women who neither smoke nor engage in regular light physical activity, diets high in fruits and proteins do not play a role. The goal of inducing ovulation is to plan pregnancy.
How to increase (or induce) ovulation naturally:
1.Refine sleep habits:
Getting a good night’s sleep is paramount to balancing hormones and increasing chances of ovulation. One study found that follicle stimulating hormone (FSH) levels were 20% higher in women who slept an average of 7-9 hours each night compared those who slept for less than 7 hours each night. Sleep is essential for stress management and emotional regulation. If a patient is struggling to sleep, consider refine her sleep habits by i) Waking up and going to bed at the same time each day. ii) Avoiding caffeinated beverages after lunchtime. Iii) Making sure that your bedroom is a cool, dark, and quiet place to sleep.
2.Exercise regularly
Another natural method for increasing chances of ovulation is exercise. Regular physical activity not only helps you to maintain a healthy weight, reduce the risk of insulin resistance and type 2 diabetes and reduce feelings of stress and anxiety. Following tips would help: i) Take time to explore different types of activities and find something that you enjoy. ii) Do low/medium intensity exercises and don’t do high-intensity exercises iii) Start with fifteen to twenty minutes each day to exercise, over time you can build up to longer intervals.
3.Maintain a healthy diet:
The foods and drinks that we consume have a major influence on how our hormones work. Diet not only helps to keep body weight regulated, but also ensures that the body gets the nutrients it needs to function properly. Unfortunately, there is not one specific food or food group that you can eat that will magically make you ovulate. However, the key foods in moderation for a healthy diet include Folates – such as leafy green vegetables, beans, and whole grains. Fiber – such as broccoli, avocados, and apples. Iron – such as spinach, quinoa, and turkey. Calcium – such as seeds, yogurt, and lentils. Omega-3 fatty acids – such as flax seeds, walnuts, and salmon. Protein – such as cottage cheese, pumpkin seeds and eggs, chicken breast. Avoiding sugar, alcohol, caffeine, nicotine, and drugs is also important.
4.Supplements when needed:
As humans, it is not realistic to think that we will have the perfect diet all the time. As supplements like folic acid, B-vitamins, vitamin E, vitamin D, zinc, iron, and calcium are essential for balancing hormones, it’s a good idea to take a general multivitamin or prenatal vitamin daily. Better get Blood vitamin levels assessed to guide what vitamin to take.
- Minimize stress:
Keeping your stress levels to a minimum is another natural way to balance your hormones and regulate ovulation. That’s because when stress levels are high, it can cause cortisol levels to spike. When this happens, things like your appetite, metabolism, and ability to maintain a healthy weight are disrupted. Breathing techniques, to lower heart rate and combat stress, anxiety, and insomnia are helpful. Practicing good self-care by setting clear boundaries at work and in personal life, taking time out to relax, and prioritizing activities that help you to de-stress.
What’s going on in the body during ovulation?
At the very beginning of menstrual cycle of any woman (i.e. day one of your period), follicle stimulating hormone (FSH) levels begin to rise. This hormone is responsible for developing an ovarian follicle while also initiating the production of oestrogen. Oestrogen continues to increase during the first half of the cycle. Approximately 24-36 hours before ovulation, luteinizing hormone (LH) rises rapidly, to trigger the body to ovulate. After ovulation, progesterone rises and dominates the second half of the cycle to eventually fall, if no fertilization occurs and initiates next period, and the entire cycle repeats. As the female reproductive process is guided almost entirely by hormones, when a woman’s hormones are in balance, the entire system including ability to ovulate works the way it should.
Ovulation Induction Treatment (OIT)
Ovulation Induction (OI) is a fertility treatment which involves the use of medications to increase the number of eggs produced during a cycle or regulate or cause ovulation. This technique is used so that intercourse, in vitro fertilization (IVF) and intrauterine insemination procedures, can be scheduled at an optimal time and the opportunity for pregnancy can be increased. It helps determine the time in the menstrual cycle when getting pregnant is most likely. The test detects a rise in luteinizing hormone (LH) in the urine.
The Primary process of the OIT:
Step 1 – Stimulation: Ovulation induction medications include clomiphene citrate, gonadotropins, etc. These oral drugs promote the growth of the follicles (fluid-filled sacks) carrying the eggs. These medicines replace FSH (follicle-stimulating hormone), and then the ovaries produce multiple follicles and mature, high-quality eggs. The hormone levels and follicular development are tracked throughout the stimulation cycle and accordingly medication protocol is set for best results.
Step 2- Control: Blood tests and ultrasound are used to monitor the effect of the hormonal medicines introduced. It helps to determine the hormone levels, identify the maturation status of eggs, and assess the size of follicles, known as Follicular Monitoring.
Step 3- Egg Release (Ovulation):
When the follicles are ready, generally between 16 and 20 millimetres in diameter depending on your medication, an injection of is given to prepare you for intrauterine insemination (IUI) or intercourse.
How to monitor ovulation and fertility
Hormone tracking
One of the most accurate ways to monitor ovulation is by measuring and tracking your fertility hormone levels directly. This can be done with a blood test at a laboratory. Alternatively, it can also be done with at-home solutions as explained earlier kit use which can measure oestrogen, progesterone, and LH levels with a simple urine test. E.g. PregatHome Ovulation Testing Kits used in Detecting Luteinizing hormone.
BBT
The “BBT” method stands for the Basal Body Temperature Method. Because the body’s temperature dips right before ovulation and quickly rises after ovulation, this method helps to track that change. To follow this method, take your temperature at the exact time each day using a basal thermometer. Over time, daily BBT measurements can then be used to identify ovulation patterns in subsequent cycles.
Calendar method
The calendar method, also known as the rhythm method, is one of the most basic methods of monitoring ovulation. To follow this method, you must use a calendar to keep track of the first day of each period over the course of six months. Once you have this information, you then follow a formula to calculate your fertile window and estimated day of ovulation. You can do these calculations by hand, or you can let a tool.
Management of Perimenopausal Syndrome:
A combination of Medication, hormone replacement and psychiatric therapies to deal with the symptoms of perimenopause are the best choice if the quality of life or daily life is affected due to severity of symptoms.
Psychiatric help in difficult times with mood swings and irritability.
Maintaining a positive attitude helps in addressing mood swings and mental issues.
For hot flashes, it is recommended that they sleep in a cool and airy place. A change of place during the hot flash may help as will drinking cool water.
It is important to follow a good and nutritious diet and avoid fried food and sweets, vitamins, and supplements for getting the required nutrition. Avoiding or reducing intake of caffeine, alcohol, and smoking as these increase the symptoms.
Women can use lubricants to manage the problems of vaginal dryness.
Exercise is a very important part of managing symptoms.
Micronized Progesterone 300 mg at bedtime is in the offing as best medication.
In a double-blind study in Canada recently 300 mg micronized Progesterone was tried at bedtime for 3 months. It decreased perimenopausal life interference without increasing the depression. Perceived night sweats and sleep quality significantly improved [8].
Conclusion:
Perimenopause is a very natural part of life and much of the symptoms can be handled naturally by just following a good lifestyle rather than depending on medications.
The menopausal transition is characterized by menstrual cycle variability and fluctuations in reproductive hormone levels.
The individual response to menopause varies considerably due to genetic, cultural, lifestyle, socioeconomic, education, behavioural and dietary factors.
A combination of Medication, hormone replacement and psychiatric therapies will deal with the symptoms of perimenopause.
Woman need more of social support, to address the mood swings than medicines.
Contraceptive induced Perimenopausal syndrome can be managed with Ovulation Induction Treatment.
References
- Perimenopause,
View at Publisher | View at Google Scholar - First Signs of Perimenopause, https://www.franciscanhealth.org/ 18 January 2023
View at Publisher | View at Google Scholar - Rui-xia Li, et.al, (2016). Perimenopausal syndrome and mood disorders in perimenopause, Medicine (Baltimore). Online Aug 12.
View at Publisher | View at Google Scholar - Meenakshi Kalhan et.al, (2020). Prevalence of Menopausal Symptoms and its Effect on Quality of Life among Rural Middle-Aged Women of Haryana, India, Int J Appl Basic Med Res. Jul-Sep; 10(3): 183–188.
View at Publisher | View at Google Scholar - Ashok. S. Dorle Prevalence of menopausal symptoms in perimenopausal women in rural part of North Karnataka
View at Publisher | View at Google Scholar - Indian women facing early menopause, A Survey, October 18, 2016
View at Publisher | View at Google Scholar - Natural remedies to perimenopause symptoms, https://www.medicalnewstoday.com/
View at Publisher | View at Google Scholar - Jerilynn C Prior et.al, (2023). Oral Micronized Progesterone for perimenopausal sweats & Hot flushes, , 3 June
View at Publisher | View at Google Scholar
