

Research Article | DOI: https://doi.org/10.31579/2835-7949/017
Management Challenges of Hypertensive Disorders in Pregnancy
1Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
2Head Department of Pharmacology Fazaia Ruth Pfau Medical College, Air University Karachi, Pakistan.
3GD Pharmaceutical Inc OPJS University Rajasthan.
4Assistant Professor Dow University of Health Sciences Karachi.
5Associate Professor, Department of Pathology Dow University of Health Sciences, Karachi, Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider, Asghar Mehdi, Geetha Kumari Das, Zameer Ahmed, Sambreen Zameer., (2023), Management Challenges of Hypertensive Disorders in Pregnancy, Biomedical Research and Clinical Trials,2(1); DOI: 10.31579/2835-7949/017
Copyright: © 2023, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 February 2023 | Accepted: 10 February 2023 | Published: 17 February 2023
Keywords: hypertension; pregnancy; obstetrics; administration; motherly well-being; fetal energy; obstacles; listening; treatment; pre-eclampsia; eclampsia; gestational hypertension;
Abstract
Hypertensive disorders in gestation present an important challenge for obstetricians, as they contribute to maternal and before-birth depression and mortality in general. These abstract aims to provide a short overview of the administration procedures employed to address these complex environments. Hypertensive disorders contain a range of conditions, including gestational hypertension, pre-eclampsia, and eclampsia, each accompanying unconnected clinical performances and suggestions.
Effective administration begins with early discovery and all-encompassing risk assessment during antenatal care visits. Close listening of blood pressure, proteinuria, and different appropriate limits is essential for a timely attack and risk layer. Multidisciplinary cooperation between obstetricians, motherly-before-birth cure specialists, and added healthcare pros are detracting from comprehensive care transfer.
Treatment approaches for hypertensive disorders in pregnancy change contingent on the asperity of the condition and gestational age. Non-pharmacological interventions in the way that behavior modifications and bed rest concede possibility be recommended originally, while pharmacological powers like antihypertensive cures are reserved for harsh cases for fear of antagonistic outcomes.
Furthermore, administration procedures should supply instructions on the prevention of difficulties such as eclampsia and intrauterine development limits that require close monitoring before birth and proper delivery when designated. Patient instruction and emotional support play pivotal roles in authorizing meaningful individuals to obey situational plans and recognize warning signs.
In conclusion, the administration of hypertensive disorders in gestation requires a comprehensive approach that integrates early discovery, close listening, up-to-the-minute intervention, and patient-focused care. By forwarding these facets proactively, obstetricians can optimize motherly and before-birth effects in this extreme-risk state.
Introduction
Hypertension in gestation is a meaningful administration question for each obstetrician. In a youth of cases, it is guiding proteinuria, and this normally signifies a multisystem ailment, as known or named at another time or place, pre-eclampsia. It’s This condition, namely, guides raised morbidity and mortality to two together, mom and baby. However, Hypertension and unique grant permission are the first signs of pre-eclampsia and thus cannot be believed blameless. In addition, it is progressively acknowledged that never-ending hypertension has associated perinatal questions. Incidence, categorization, and description Pregnant girls accompanying hypertension may be widely
separated into three classifications: chronic hypertension, non-proteinuric hypertension (consistently popular as gestation-inferred hypertension), or pre-eclampsia. To equate these as clinically beneficial control and likely forecast are different. In the United In the Kingdom, fewer than ten daughters will expire annually from pre-eclampsia [1] but this remains an almost accepted cause of the end of life in pregnancy on the grown planet. Only about one in two thousand women will have a clamp spasm disturbance but the befriended motherly death rate is 2% [2]. Eclampsia itself is not customarily existence-menacing but is a guide harsh disease, and daughters will regularly expire from a different obstacle, pre-eclampsia. Of all motherly extinction, less than half are guide eclampsia. It has been supposed to be one World Health Organization (WHO) that generally 60,000 girls will wither occurring from pre-eclampsia. Hypertension in gestation is accepted occurring in nearly individual in five wives following in position or time 20 weeks’ gestation. However, only a narrow number of these have weighty affliction guide melancholy. Concern about adverse belongings results in the exhaustive following of a lot of girls; appropriately, nearly a quarter of antenatal admissions are a result of monitoring and managing girls with hypertension. Obstetric epoch parts help reduce the need for inpatient administration. As the cause and beginning of the disease are changeable, assessments of girls accompanying gestation-inferred hypertension remnants are the linchpin of safe dispassionate practice. A transfer is the only cure for pre-eclampsia, it is the universal cause of iatrogenic prematurity bookkeeping for 15% of all rash births and nearly individual in five very depressed birthweight babies (less than 1500 g) [3]. Size at birth is connected with future fitness [4], and thus eclampsia grants permission to result in future adult disease for the baby.
This contains a raised risk of hypertension and diabetes when they enhance men. Maternal affliction and before birth involvement does not always correlate; for instance, in those Girls one has Eclampsia; at term, they frequently have normal pressure [2]. There is, nevertheless, a clear friendship between with determination bred blood pressure and depression and death; still-beginning rates are greater at some maturation when the motherly diastolic pressure is prepared or better
than 95 mmHg [5]. In the average UK population, the incidence of pre-eclampsia happens in 1 in 20 mothers. In a fussy gravida society in Ireland, the occurrence was reduced by 2% [6]. It mainly acknowledged that-proteinuric hypertension occurs in not completely three opportunities as many publics. Some studies from the United States have illustrated the predominance of pre-eclampsia is expected to be nearer 10%, conceivably having a connection with the extreme-risk population.
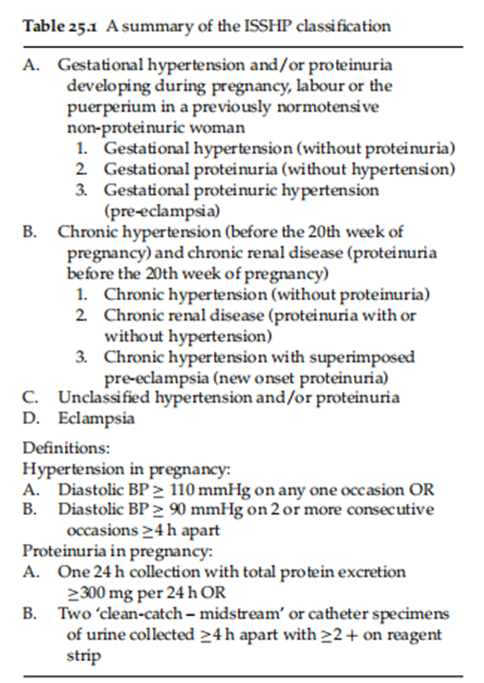
The key signs of pre-eclampsia are hypertension and proteinuria and these are used to delimit the ailment. These answers are completely damaged, and they are not continually the ultimate main and fundamental facets of the syndrome but are secondhand as they are smooth to measure. For sensible reasons, the beginning of anomaly of ancestry Pressure and proteinuria is short for fear that insults ‘at-risk’ cases. The International Society for the Study of Hypertension in Pregnancy (ISSHP) uses the term the earth personified national hypertension when daughters have earlier existed normotensive (Table 25.1). This description is established by the original approvals of Davey and MacGillvray [7].
Pathophysiology
Pre-eclampsia has existed, famously as ‘The Disease of Theories’, as the exact fate that brings about the clinical condition destitute existed elucidated. However, skill is a growing understanding of these occurrences. It is famous that pre-eclampsia is related to a weak trophoblast attack in the myometrium, and this results in motherly spiral channels being impeded in their usual corporal vasodilatation [8]. The motherly syndrome of pre-eclampsia must be connected with supplementary determinants as incompetent trophoblast attack is again visualized in pregnancies, difficult by fetal tumor limit outside motherly ailment. It is clear that injured intervillous ancestry flow results in incompetent perfusion and ischemia in the second half of pregnancy. This presumably results in the result of a sensitive oxygen class. Once the sane inside antioxidants are beaten, a condition of oxidative stress exists. This is presumably fundamental to the dispassionate disease of pre-eclampsia. Either through oxidative stress or added vasoactive meanings being freed from the covering layer, incitement of the vascular endothelium occurs [9]. The vascular endothelium is popular to drink use all tool plans and this clarifies the extensive facets of the condition. Markers of endothelial damage are commonly elevated. In addition, skilled is an anomaly in lipid characterizations, such that triglycerides and free oily acids are about to increase. There is an increase in lipid peroxidation, both systemically and in the covering layer, suggesting that oxidative stress is complicated in the endothelial container damage.
Management
Identifying those in danger: dispassionate risk determinants Although most women who get pre-eclampsia do not have risk factors, an important capacity (>1 in 3) will. Taking a painstaking record will admit risk appraisal. The National Institute of Clinical Excellence (NICE) antenatal directions plan is a fundamental part of clinic U.S. state management and approves that contact Her level of risk for pre-eclampsia should be evaluated because her schedule of antenatal jobs may be planned. These directions have recorded the following as risk determinants for evolving pre-eclampsia; nulliparity, age 40 or earlier, a genealogical chart of pre-eclampsia (e.g. pre-eclampsia in a parent or twin), a earlier record of pre-eclampsia, a party bulk index (BMI) at or above 35 in the beginning contact, a diversified gestation, or pre-existing vascular ailment (like hypertension or Diabetes)[10].
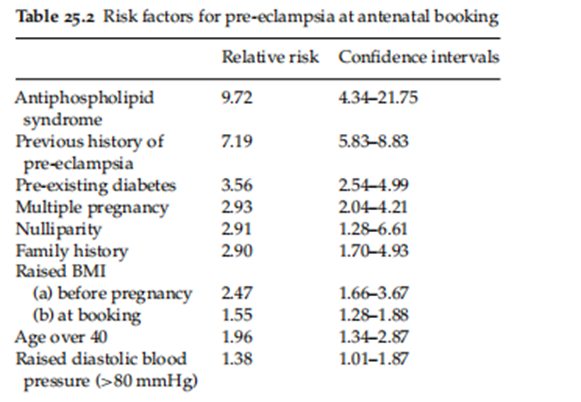
A recent orderly review has prepared a few of these risks at the engagement visit [11] (Table 25.2). As the genealogical chart in a first college degree is relatively powerful, connected with pre-eclampsia, this exemplifies the important historical influence. Exposure to the fatherly antigen by way of either the unborn young or the wife does have an influence suggesting an immunological detail to the affliction process. Pre-eclampsia is more common in first-time pregnancies and even miscarriages or the end of gestation will cause a decline in risk [12]. Non-obstacle methods of pregnancy prevention and raised events of intercourse cohabitation have been stated to be a humble risk [13, 14]. Both adolescent founders and pregnancies understood by contributor impregnation of the ovum increase the risk [15]. If pregnant by partner the one has earlier sired a distressed gestation the girl has almost double the risk of pre-eclampsia [16].
These dispassionate remarks no doubt had a connection with exposure to certain fatherly antigens. Underlying healing afflictions specifically those including the cardiovascular structure increase the risk of pre-eclampsia, suggesting that darkish nasal susceptibleness is a main determinant in reaction to the placental etiology [17, 18]. This includes organic compounds composed of carbon intolerance, either in the form of gestational or settled diabetes. Obesity is a free-risk determinant for pre-eclampsia.
The placental amount can have an influence, as a hard bony structure in the jaws of vertebrate pregnancies is an excellent cause of pre-eclampsia happening beyond 20 weeks of growth. Pregnancies complicated by hydrops fetalis (mirror disease) or trisomy chromosomal component again have a raised risk. Previous pre-eclampsia is a forceful risk determinant, specifically in the early beginning; approximately five individuals in a group of five wives who have the necessary delivery before 37 weeks will have a frequency.
Identifying those at Risk: Investigation
Tests to conclude pre-eclampsia may be widely detached into biophysical and biochemical. The most promising biography material test is that of uterine channel Doppler. This is a nearly fast and inexpensive test that may be made at an identical period to the oddity thumb through. It has the benefit of recognizing weak placental perfusion, which is fundamental to the disease process. There is an approximately extreme resistant distribution accompanying a notch obvious in the uterine channel Doppler (Fig. 25.1).
As the change to a common depressed-opposing distribution may be slowed the later the test acted the better allure predictive value. Approximately individual in five mothers the one have an atypical Doppler at 20 weeks’ The process of early development will evolve pre-eclampsia [19]. At 24 weeks’ growth the forecasting worth is better. Identifying girls at risk will admit increase in following and use of protective the pie may be considered. If safeguard measures perform therefore these hide tests will become more main. However, the worth of utilizing specific biophysical tests, in agreement with improving effect, have as yet not been settled, and NICE does not recommend their use in depressed-risk daughters [10]. Doppler calculations are used more usually in extreme-risk girls, even though the prospect ratios are lower, and definite tests in two together extreme- and reduced-risk mothers give complementary categorical risks or certain predicting principles, approximately 20%. Other biophysical tests, to a degree measure ancestry pressure does have a predicted worth when calculated in early pregnancy [11]. Even inside a sane ancestry pressure range the level of ancestry pressure is connected with risk. However, this is dangerously confused apiece weak methods in weighing blood pressure. Attempts have been created to upgrade this by utilizing robotic blood pressure measures mentbutatthe moment wait widely useless as they use an oscillometric method to measure ancestry pressure which is erroneous in pre-eclampsia [20]. Other biophysical test in the way that isometrics exercise experiments and the “give up test” has a very weak predictive advantage and have to enhance settled in dispassionate practice. The angiotensin II sense tests involve determining ancestry pressure reaction to infusing the vasoconstrictor angiotensin II but this was likewise not clinically useful both on account of weak indicator and being an opportunity absorbing and harmful investigation [21]. Numerous hematological and biochemical gravestones have been used to two together call and judge pre-eclampsia together. The simple calculations of hemoglobin and hematocrit have a feeble partnership accompanying the expansion of pre-eclampsia as does the plasma book. In wives, the one have never-ending hypertension the measure of uric acid and platelets can help in deciding those who take covered pre-eclampsia; repeatedly they lack sensitivity and particularity. Second-trimester human chorionic gonadotropin and motherly serum beginning fetoprotein is guide a duple increase of pre-eclampsia.
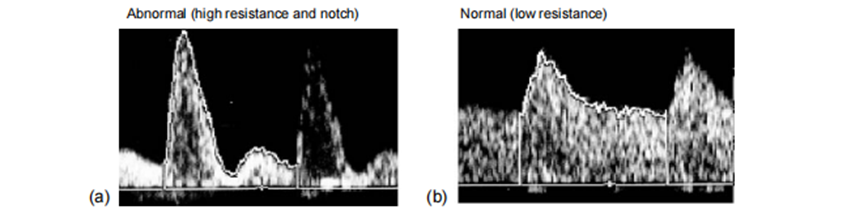
Fig. 25.1 A comparison of normal and abnormal fetal velocity waveform.
This is possibly had connection with the disease process at the utero placental connect. The prophet advantage repeated is little enough expected clinically doable. Endothelial activation does happen in pre-eclampsia and skilled are many stones that are raised that are connected with endothelial damage. Some will increase superior to dispassionate manifestations of the ailment but almost invariably skilled is a ride in mothers the one is afterward sane and those the one has a serious ailment, repeated confining the dispassionate valuable promontory into water. Investigation to a degree of urinary excretion of calcium, microalbuminuria, and prostacyclin metabolites have all been examined. Combinations of gravestones can raise predicting principles and future work is likely to deem joining endothelial and placental stones to expand algorithms that may be imported efficiently. However, as far as protective measures that are clinically valuable are received these tests will wait widely investigatory. The table shows gravestones that have existed examined in early gestation and by what they change concerning subsequent preeclampsia [22].
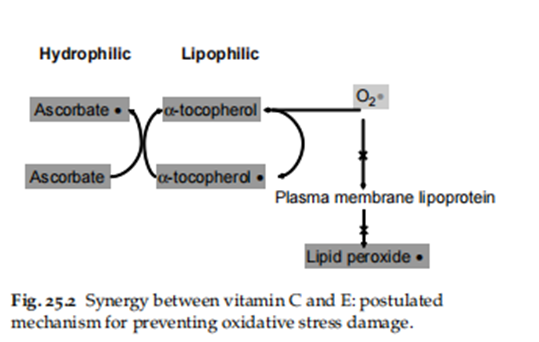
Prophylactic analyses The key to the new management of pre-eclampsia is and proper childbirth superior to weighty consequences. In an ideal realm avoiding the manifestation of the ailment hopeful far more favored. Aspirin, U.S. state cium, and antioxidants have all been examined, accompanying some evidence of accomplishment. Fish oils, magnesium, and even fight [23] have proved less promising. Low-measure anesthetic reverses the shortcoming between the vasoconstrictor thromboxane A2 and the vasodilator prostacyclin, which is famous to happen in pre-eclampsia. There are 42 randomized regulated troubles written in the Cochrane cooperation professed a 15% relative risk reduction in pre-eclampsia when either anesthetic or different antiplatelet powers are likely. There is a akin reduction (14%) in the risk of the afterlife to the baby in addition to an 8?cline in the risk of preterm delivery [24]. It is widely recognized that anesthetic bear be thought out in extreme-risk girls. The benefit is visualized when the prevalence of pre-eclampsia is only 7%, and individual baby demise may be obviated for each 250 acted [25]. The evidence evil states it is safe. There are continuous studies concerning the appropriate quantity and organization in addition to the community to be targeted.There are 10 tests in almost 7000 mothers professed the advantageous part of calcium as pre-eclamptics prophylaxis and overall skill is a significant decline in the occurrence of pre-eclampsia [26]. However, this is chiefly had a connection with the happiness in tests in daughters accompanying inadequate calcium consumption and the benefit to the baby is not as clear as anesthetic. The WHO has currently achieved a trial (results attended) to see either supplementation ingrown nations is helpful. The cases of the use of Bob oils holding N3 greasy acid are known to restrict platelet thromboxane A2 has not shown a significant reduction in pre-eclampsia. As oxidative stress is popularly expected fundamental to the disease process individual trials manifested that source of nourishment C and E supplementation in the second trimester of pregnancy can be advantageous, professed more therefore a 50?cline when extreme-risk girls were considered [27].
This involved 1000 mg source of nourishment C and 400 IU source of nourishment E, which are popular to act synergistically (Fig. 25.2); by what always, further studies that are currently continuous need to confirm this.
Combining Prediction And Prevention
A test does not should be perfect expecting a valuable clinical finish.
As pre-eclampsia has an approximately depressed predominance, numbers
wanted to treat for fear that one case may severely
lowered when joining an approximately limited test in terms
of predicting capacities (such as 20%) accompanying the situation. Figure 25.3
explains the relationship between declaration and
relative risk decline, in conditions of principle of behavior, wanted to treat [28].
Assessment of the mother
The opening of hypertension and proteinuria are relatively reduced to recognize pre-eclampsia so the first key the aspect of management involves validating the diagnosed person's friend to guarantee that iatrogenic morbidity does not emanate. Hypertension that occurs in early gestation, that is, before 28 weeks’ growth results in pre-eclampsia evolving in nearly 50% of wives. In contrast, women present at term accompanying hypertension are likely to develop pre-eclampsia (nearly a 10% risk). Care in determining both ancestry pressure and proteinuria can upgrade appraisal as wrong beneficial and negative tests are commonplace. Digit predilection (the practice of rounding the last number of ancestry pressure to nothing) happens in the majority of antenatal calculations and is completely communicable feel inclined to prevent this will limit erroneous diagnoses. Using a standard bladder in a sphygmomanometer cuff will orderly under cuff 25% of an average antenatal society. Having insult-abundant cuffs feasible and utilizing them will forbid the over diagnosis of hypertension [29]. Keeping the rate of slump to 2–3 mmHg will halt over diagnosing diastolic hypertension, as will utilizing Korotkoff 5, which is immediately universally urged for diagnosing diastolic energetic tightness. Korotkoff 4 (the muffling of the sound) is less reproducible, and randomized regulated tests rooted that it is safe to abandon it, except in those excellent positions when the ancestry pressure approaches nothing [30,31]. Dipstick proteinuria is not only dependent on something dishonest positive results but also an equal predominance of fake contradiction. 24-period accumulations of urine are essential to establish the disease. New electronic maneuvers may be used to assess proteinuria. They considerably increase predicting principles [32]. Protein/creatinine percentages may be used for immediate nibbled evaluation as they are akin to the veracity of 24-hour groups.
It is likely to have severe ailment and usual ancestry pressure or proteinuria. In a survey of wives accompanying eclampsia, only just half had a recent measurement displaying both meaningful proteinuria and hypertension [2]. The condition of pre-eclampsia is multi systemic, and added means involvement must be cautiously thought-out, including the covering layer. Other signs of the disease destitute are contained in the description for pragmatic reasons, but they are frequently evenly main. Painstaking annals also involve girls who have syndromes in the way of ocular disturbance, headaches, and epigastric pain. Some opportunities sickness in the stomach or even disgorging may be a giving feature. However, at least 50% of wives even with harsh disease will be asymptomatic [2]. When directing daughter
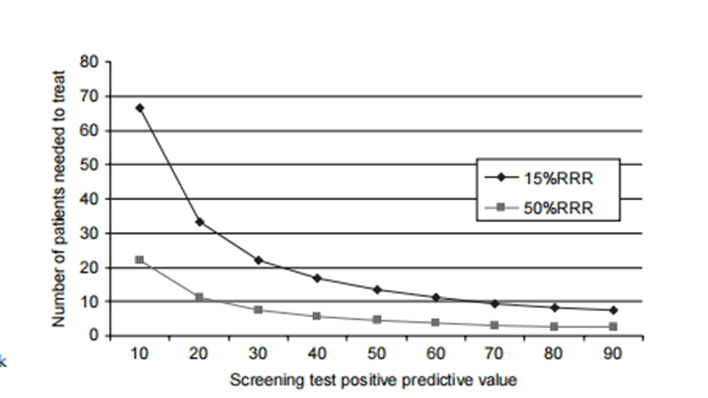
Fig. 25.3 Positive predictive value and relative risk reduction (RRR) on numbers needed to treat.
specifically detached from the term, involvement of all means arrangements must be cautiously investigated. Platelets are drank on account of the endothelial incitement. A falling count, specifically to inferior 100 × 109/l concede possibility signifies a need to consider transmittal. Counts above 50 are inclined to support hemostasis. A growing hematocrit or hemoglobin indicates hypovolaemia, which is a severe characteristic of harsh disease. If labor is expected before coagulating abnormalities concede the possibility be hindered as pre-eclampsia can cause distributed intravascular coagulation. This is mainly if territorial-induced sleep is used, which is favor smart to approximate anesthesia. The renal tubular function can be evaluated by weighing uric acid, which is a marker of ailment asperity, even though normal levels can happen in harsh affliction. Acute fatty liver can influence spuriously extreme levels of uric acid (in addition to high cells that eat bacteria and fungi count, and depressed and oxygen). Urea and creatinine are associated with late renal involvement and are mainly not useful as indicators of ailment asperity. Liver transaminases concede the possibility be measured to display hepatocellular damage. Normal ranges of transaminases are nearly 20% lower than non-meaningful[33]. Subcapsular involvement of the liver can occur, developing in epigastric pain accompanying usual transaminase measurements. HELLP (Haemolysis, Elevated Liver Enzymes, Low Platelets) condition happens when the liver connection is associated with hemolysis and depressed platelets. This is a harsh variant of pre-eclampsia. When protein elimination exceeds 3 g in 24 h, the circulating albumin is inclined to fall (nephrotic condition) and this increases the risk of pulmonary edema. Lactate dehydrogenase levels will increase in the closeness of hemolysis. Antenatal corticosteroids should be taken to reinforce before birth lung adulthood and are not contraindicated in pre-eclampsia. Steroid cure is further famous for helping recovery from HELLP disease and has existed secondhand in the post-partum period. Antenatal corticosteroids grant permission to raise biochemical markers in wives accompanying pre-eclampsia. The situation of blood pressure concedes the possibility be unsociable mainly for severe hypertension, that is to say, ancestry pressures over 170/110 mmHg. However, this does demand urgent medicine. Treatment of moderate hypertension concedes the possibility be damage before birth growth [34], and moderate ancestry pressure cannot be aggressively discussed. Once fetal bronchi adulthood is inclined to be adequate, childbirth endures be deliberate, that is, subsequently 32 weeks’ growth.
Multiorgan connection or fetal compromise hopeful clues for childbirth. Close inpatient supervision is otherwise necessary and maybe thought-out superior to 32 weeks gestation or when the benefit of conservative administration is deduced to override delivery. Conservative administration will lower neonatal melancholy, without really growing motherly problems. Recent evidence implies that under 30 weeks neonatal melancholy is extreme, and conservative management is desirable [35]. However, at least an individual after a second of girls still needs to be brought for before birth reasons under 34 weeks. The failure to control hypertension, decaying liver or renal function, progressive appear platelet or albumin, or affecting animate nerve organs obstacles would be clues for motherly transmittal at any incubation.Fetal appraisal Early beginning pre-eclampsia is particularly complicated accompanying placental lack, and more than half of babies innate before 34 weeks will be progress-limited [35]. This also illustrates the reason abruption is more average, occurring in about 1 in 20 of these early onset cases. Fetal welfare bear forever be cautiously considered fully cases of pre-eclampsia, and involves a symphyseal fundal altitude assessment, in addition to a common inquest as to before-birth movements. At early gestations, an ultrasound leaf through must be acted to assess before birth progress and concede possibility including the decision of the amniotic fluid index and umbilicus u.s. state channel Doppler waveforms. A non-reactive CTG accompanying decelerations or a before birth condition that is to say degenerating war rants delivery, as it is inconceivable to correct accompanying time and can decay accompanying antihypertensive therapy.
Intrapartum care of pre-eclampsia Many parts have immediately grown severe pre-eclampsia obligation. Cases that demand protocol driven he agement are frequently defined as those accompanying harsh hypertension (more than 170/110 mmHg) or hypertension accompanying
an additional confusion to a degree problem, visual ridicule turbance, epigastric pain, clonus (as well three beats) or a platelet count inferior to 100 or AST more than 50 IU parts per liter.
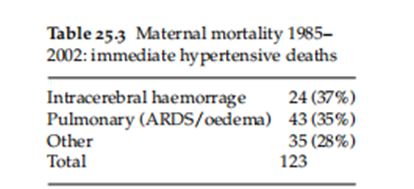
The secret inquest into motherly deaths states that the two together main reasons reason mothers expire are cerebral hemorrhage and adult/severe respiring distress conditions [1]. Table 25.3 explains all dossiers from these causes since 1985 when the dossier was created and usable from the whole of the United Kingdom. The two most influential determinants that contribute to these deaths are thus harsh hypertension and fluid consumption. The control of ancestry pressure and fluid balance is so detracting. In contrast to pulmonary causes of decease, in the current age, deaths accompanying intracerebral hemorrhage destitute happened decreased, suggesting control of ancestry pressure remains substandard through weak listening and situation (Fig. 25.4).
Blood pressure control Blood pressure is the possibility to be measured commonly (not completely all 15 brief periods). Automated sphygmomanometer may be used to facilitate this, or by preference, event-arterial statements may be determined via a minor arterial pressure transducer. As non-obtrusive calculations are acquired mainly by oscillometric blood pressure instruments, that minimize ancestry pressure in pre-eclampsia [20,36], significant changes in ancestry pressure should be rooted in utilizing planets orbiting sun sphygmomanometer. Some instruments are immediately accurate, and only those expressly evaluated for veracity in pre-eclampsia bear be bought in the future [37]. On an individual patient basis the accuracy of some design secondhand bear use against an observer utilizing standard sphygmomanometry, favor capably accompanying a major planet sphygmomanometer. Mean arterial pressures (MAP) are generally used to guide accomplishment in codes. Antihypertensive healing can be influenced when the MAP is ≥125 mmHg, or urgently if >140 mmHg as above this using one's brain auto regulation of pres certain is doubtful. Either hydralazine or labetalol may be used as a first-line treatment, although favored [38]. As these are the main danger measures in preventing stroke, clinicians complicated in the administration of severe pre-eclampsia concede the possibility of identifying accompanying situation regimes. Some agreements advocate infusing a colloid to protect the uteroplacental distribution if the baby is livered. This should be accomplished with caution, and cautious concern about the impact of the overall fluid management ment, and by preference under main venous pressure (CVP) following.
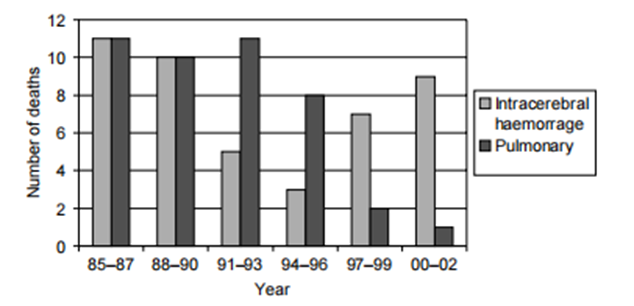
Fig. 25.4 Maternal mortality 1985–2002: immediate hypertensive deaths
Control of fluid balance
Strict listening of recommendations and output is essential in the morbid pre-eclamptic patient. A consolidation of the shortened intravascular book, seeping capillaries, and low albumin form daughter compulsive pulmonary edema. Renal failure is a rare complication of pre-eclampsia but should be thought out when skilled has happened incompetent transfusion or deep hypotension following post-partum drain insult, as skilled is shortened intravascular volume. Oliguria is comparatively prevalent, and absolute listening should be considered rather than a belligerent blind fluid substitute. Administration of drip fluid in the oliguric patient must be accomplished with caution. Most contracts will limit fluid intake to nearly 1 ml/kg/h. CVP listening and Foley catheter inserts should be secondhand whenever possible. Repetitive fluid challenges concede possibility be prevented by the lack of obtrusive listening. Should the CVP be high (>8 mmHg) accompanying continuous oliguria before a dopamine infusion may be thought out (1 µ/kg/min.) Hemodialysis or hemofiltration may be necessary if the creatinine or potassium rises. Close ideas accompanying a renal doctor concede possibility begs. Administration of diuretics will only temporarily improve excretion amount and confound the shortened flowing book. Frusemide should so be unsociable for doctoring pulmonary edema. Pulmonary channel catheterization is a possibility to be considered in troublesome cases.
Anticonvulsant administration
An eclamptic fit is frequently self-restricting; nevertheless, anticonvulsive therapy concedes the possibility of terminating it when attainable. Magnesium sulfate may be used to control such a fit (up to 8 mg likely by slow venous immersion). Diazepam 10 mg can also be secondhand but its anticonvulsant features are fleeting as distinguished from allure sedative features. In those women who have extended fitting a computerized axial tomography is necessary to exclude an intracerebral bleed. Following an eclamptic fit magnesium sulfate is the precaution of choice [39]. Magnesium sulfate has been explained to weaken cerebral ischemia by the present image of sheet stabilizer and vasodilator and is taller two together than diazepam and phenytoin in countering further fits. It is more befriended accompanying a significant decline in the need for motherly ventilation and exhaustive care admissions. Magnesium sulfate is likely in a 2 g drip stowing dosage in an infusion of 1 g/h. Some protocols suggest 2 g/h but efficacy has been displayed at 1 g/h. It is renally discharged so in cases of oliguria or climbing urea care must be captured concerning toxicity and this is discovered by the absence of a patellar effect. Respiratory arrest and power paralysis in addition to a heart attack can happen and a remedy is 10 ml of 10?lcium gluconate. Even with harsh pre-eclampsia, eclamptic fits are rare and happen in inferior 2%. The Magpie trial judged bestowing magnesium sulfate against a placebo in wives accompanying pre-eclampsia and there was a meaningful decline in fits in those girls receiving insult situations; the magnesium sulfate will about cut in half the incidence of eclampsia [40]. The evidence likewise suggests that skilled are less likely to pass, but tests have not existed big enough to show that this is considerably so. The threshold for bestowing magnesium sulfate to a pre-eclamptic daughter is doubtful but mainly as the risk increases the benefit favors medicine.
Anaesthetic administration
Endotracheal intubation can cause harsh hypertension and general sleep-inducing or numbing drugs bear be prevented [41]. The regional barrier is thus the induced absence of a feeling of choice; superior to inserting a coagulopathy should be forbidden. Platelet levels in addition to 80 × 109 are inclined to guarantee hemostasis and most obstetric anesthetists are hopefully satisfied to perform this process under such a class. In wives, the ones who have a Caesarean section have a depressed beginning for invasive CVP listening. Careful administration of fluid particularly following post-partum hemorrhage Number of afterlives is essential. Following childbirth, individuals in three eclamptic fits will happen in the post-partum ending most of these inside 48 h [2]. Although eclampsia has been reported further existing time it is not ordinarily guided by weighty morbidity and mainly anticonvulsant precautions may be stopped inside a 48-h ending. Blood pressure must be listened to painstakingly for at least days following transfer as the topmost reading can happen presently [42]. Quite repeatedly it should present the mother's antihypertensive analysis at home and the effect is recommended at 6 weeks. Methyldopa has mainly undesirable aftereffects and most prevailing antihypertensive analyses may be used
Post-natal administration
At the post-innate effect, two together ancestry pressure and excretion concede the possibility be inspected for underlying renal and cardiovascular irregularities. It is immediately clear that daughters the one had pre-eclampsia have a growing of subsequent ischaemic congestive heart failure no doubt related to the fundamental vascular study of plants. This risk is better the more progress-limited and untimely her baby is. At the post-innate visit future pregnancies concede the possibility be discussed in addition to the need for hide for hypertension in later existence.
Research Method
This study uses an assorted-systems approach, joining together quantitative and subjective methods to completely investigate the administration challenges of hypertensive disorders in gestation.
Literature Review
An orderly review of existing information was conducted to identify appropriate studies on the issue. Databases in the way that PubMed, MEDLINE, Embase, and Cochrane Library were examined utilizing appropriate keywords containing "hypertensive disorders in gestation," "preeclampsia," "gestational hypertension," and "administration challenges." The search was limited to studies written within the last 10 years to guarantee pertinence.
Inclusion Criteria
studies contained in the review undergo the following tests:
Published in peer-inspected journals
Focus on management challenges of hypertensive disorders in gestation
Include dossier on disease, situation, listening, patient instruction, or healthcare wage earner preparation
Available in English terminology
Data Extraction
Data from picked studies were extracted utilizing a patterned form. Key news elicited contained study design, sample traits, methods, main verdicts, and associations for management.
Qualitative Analysis
Qualitative dossiers from contained studies were resolved to utilize theme reasoning. Themes that had a connection with the challenges of hypertensive disorders in gestation were labeled and synthesized. The study proposed to disclose patterns, public, and differences in the challenges stated across various studies.
Quantitative Analysis
Quantitative dossiers from the contained studies were analyzed descriptively. Summary enumerations to a degree of recurrences, wealth, and percentages were determined to measure the predominance and asperity of administration challenges stated in the literature.
Framework Analysis
The WHO directions for the administration of hypertensive disorders in gestation were secondhand as a foundation to guide the reasoning. The directions supported an organized approach to understanding the key components of administration and served as a citation point for judging the challenges recognized in the research.
Integration of Findings
Qualitative and all-inclusive judgments were joined to provide an inclusive understanding of the administration challenges of hypertensive disorders in gestation. Themes recognized through subjective reasoning were corroborated and augmented by an all-inclusive dossier where appropriate.
Limitations
Potential disadvantages of the study include:
Bias owned by the picked studies
Limited generalizability of verdicts to various states and scenes
Challenges in synthesizing dossier from studies accompanying variable methods and character
Ethical Considerations
Ethical authorization was optional for this study as it complicated the reasoning of existing literature and did not include human matters straightforwardly.
Results
Key judgments disclose various management challenges:
Early Diagnosis: Limited forms for early discovery of hypertensive disorders in gestation pose an important challenge, often superior to postponed attacks.
Treatment Options: Variability in situational effectiveness and unfavorable effects of antihypertensive drugs confuse management resolutions.
Monitoring Protocols: Inconsistencies in listening pacts and possessions hinder the active pursuit of motherly and before-birth well-being.
Patient Education: Insufficient patient instruction concerning the signs and risks of hypertensive disorders obstructs up-to-date healthcare-pursuing behaviors.
Healthcare Provider Training: Inadequate preparation of healthcare providers in seeing and directing hypertensive disorders provides suboptimal care transmission.
Discussion
Interpreting the results discloses versatile challenges:
Resource Constraints: A limited approach to specialized care and demonstrative finishes in certain domains exacerbates challenges in administration.
Socio-business-related Factors: Socioeconomic differences impact the talent of women to approach convenient and enough care, superior to worsened consequences.
Cultural Beliefs: Cultural ideas and practices concede the possibility of influencing healthcare-pursuing practices and adherence to the situation, moving administration effects.
Healthcare Infrastructure: Weak healthcare infrastructure in a few backgrounds leads to splintered care transfer and suboptimal consequences.
Conclusion
Addressing the administration challenges of hypertensive disorders in gestation is principal for improving motherly and before-birth effects everywhere. Multifaceted interventions focused on early disease, embellished situation options, patterned listening agreements, inclusive patient instruction, and healthcare provider preparation are unavoidable.
Management Implications
Interdisciplinary Collaboration: Encourage cooperation with obstetricians, midwives, nurses, and other healthcare professionals to provide inclusive care.
Policy Interventions: Advocate for procedures that improve the approach to fetal care, demonstrative finishes, and essential medications for directing hypertensive disorders.
Patient Empowerment: Prioritize patient instruction and authorization to authorize informed accountable and full of enthusiastic administration.
Healthcare Provider Education: Invest in preparation programs to enhance healthcare providers' abilities and information in diagnosing and directing hypertensive disorders in pregnancy.
Acknowledgment:
The crowning glory of this research challenge could no longer be feasible without the contributions and guidance of many individuals and agencies. we’re deeply grateful to all those who played a role in the achievement of this mission We would also like to thank My mentor, Dr. Naweed Imam Syed, Prof. Department of Cell Biology at the College of Calgary, and Dr. Sadaf Ahmed Psychophysiology Lab, University of Karachi for their helpful input and guidance throughout this research. Their insights and understanding had been instrumental in shapingthe direction of this challenge.
Declaration of interest
I, at this second, declare that: I haven’t any pecuniary or another private hobby, direct or oblique, in any dependence that raises or can also boost a war with my duties as a supervisor of my workplace control
Conflicts of Interest: The authors declare that they have no conflicts of interest.
Financial support and sponsorship: No Funding was received to assist with the preparation of this manuscript
References
- Department of Health (2001), Why Mothers Die, 1197–1999. Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: ROCG Press.
View at Publisher | View at Google Scholar - Douglas KA & Redman CWG Eclampsia in the United Kingdom. Br Med J 309, 1395–1400.
View at Publisher | View at Google Scholar - Project27/28 (2003).An Enquiry into Quality of Care and Its Effect on the Survival of Babies Born at 27–28 weeks. London: London Stationery Office.
View at Publisher | View at Google Scholar - Barker DJP, Bull AR & Osmond C (1990).Fetal and placental breadth and risk of hypertension in adult growth. BMJ 301, 259–261.
View at Publisher | View at Google Scholar - Freidman EA & Neff RK (1996). Pregnancy consequences are connected with hypertension, edema, and proteinuria. In: Churchill D & Beevers DG (eds) Hypertension in Pregnancy London: BMJ Books.
View at Publisher | View at Google Scholar - Higgins JR, Walshe JJ, Halligan A, O’Brien E, Conroy R, & Darling MR (1997): Can 24-stage itinerant ancestry pressure measurement predict the development of hypertension in primigravidae? Br J Obstet Gynecol 104, 356–362.
View at Publisher | View at Google Scholar - Davey DA & MacGillivray I (1988). The categorization and description of the hypertensive disorders of gestation. Am J Obstet Gynecol 158, 892–898.
View at Publisher | View at Google Scholar - Brosens, IA (1977).Morphological changes in the uteroplacental bed in gestation hypertension. Clin Obstet Gynaecol 77, 573–593.
View at Publisher | View at Google Scholar - Roberts JM, Taylor RN, Musci TJ, Rodgers GM, Hubel CA & McLaughlin MK (1989), Pre-eclampsia: an endothelial container disorder. Am J Obstet Gynecol 161, 1200–1204.
View at Publisher | View at Google Scholar - National Institute for Clinical Excellence (2003). Guidelines for CG6 Antenatal Care: Routine Care for the Healthy Pregnant Woman. London: NICE.
View at Publisher | View at Google Scholar - Duckitt K & Harrington D (2005). Risk determinants for pre-eclampsia at antenatal engagement: an orderly review of reserved studies. Br Med J 330, 565.
View at Publisher | View at Google Scholar - Strickland DM, Guzick DS, Cox K, Gant NF & Rosenfeld CR (1986). The connection between failure and the first gestation and development of gestation-inferred hypertension after gestation. Am J Obstet Gynecol 154, 146–148.
View at Publisher | View at Google Scholar - Klonoff-Cohen HS, Savitz DA, Cefalo RC & McCann MF (1989) .An epidemiologic study of birth control and pre-eclampsia. J Am Med Assoc 262, 3141–3147.
View at Publisher | View at Google Scholar - Robillard PY, Hulsey TC, Perianin J, Janky E, Miri EH, et al. (1994). Association of gestation-inferred hypertension accompanying event of intercourse cohabitation without legal document before birth. Lancet 344, 973–975.
View at Publisher | View at Google Scholar - Need JA, Bell B, Meffin E & Jones WR (1983).Pre-eclampsia in pregnancies from backer birth. J Reprod Immunol 5, 329–338.
View at Publisher | View at Google Scholar - Lie RT, Rasmussen S, Brunborg H, Gjessing HK, Lie-Nielsen E & Irgens LM (1998). Fetal and motherly offerings to risk of pre-eclampsia: people located study. BMJ 316, 1343–1347.
View at Publisher | View at Google Scholar - Rey E & Couturier A (1994). The forecast of gestation in daughters accompanying never-ending hypertension. Am J Obstet Gynecol 171, 410–416.
View at Publisher | View at Google Scholar - McCowan LM, BuistRG, North RA & Gamble G (1996). Perinatal depression in never-ending hypertension. Br J Obstet Gynaecol 103, 123–129.
View at Publisher | View at Google Scholar - Mires GJ, Williams FL, Leslie J & Howie PW (1998). Assessment of uterine arterial notching as a hidden test for unfavorable gestation consequence. Am J Obstet Gynecol 179, 1317–1323.
View at Publisher | View at Google Scholar - Penny JA, Shennan AH, Halligan AW Taylor DJ, de SwietM & Anthony J (1997). Blood pressure calculation in harsh pre-eclampsia. Lancet 349, 1518.
View at Publisher | View at Google Scholar - Kyle PM, Buckley D, Kissane J, de SwietM & Redman CW (1995). The angiotensin sense test and reduced-dosage anesthetic are useless plans to conclude and halt hypertensive disorders in nulliparous gestation. Am J Obstet Gynecol 173, 865–872.
View at Publisher | View at Google Scholar - Robyn North. Can we foresee pre-eclampsia? In: Pre-eclampsia. London: RCOG Press, 257–275.
View at Publisher | View at Google Scholar - Zhang ZJ, Cheng WW & Yang YM (1994). [Low-measurement of treated fight in halting gestation persuaded hypertension]. Zhonghua Fu Chan Ke Za Zhi 29, 463–464.
View at Publisher | View at Google Scholar - Duley L, Henderson-Smart D, KnightM & King J (2001). Antiplatelet drugs for the treatment of pre-eclampsia and allure results: an orderly review. Br Med J 322, 329–333.
View at Publisher | View at Google Scholar - Duley L, Henderson-SmartDJ, KnightM & King JF (2003). Antiplatelet powers for halting pre-eclampsia and allure confusion. Cochrane Database Syst Rev 4, CD004659.
View at Publisher | View at Google Scholar - Atallah AN, Hofmeyr GJ & Duley L (2002). Calcium supplementation before birth for averting hypertensive disorders and accompanying questions. Cochrane Database Syst Rev 1, CD001059. DOI 10.1002/14651858.CD001059. Cochrane calcium.
View at Publisher | View at Google Scholar - Chappell LC, Seed PT, Briley AL, and others. (1999). Prevention of pre-eclampsia by antioxidants: A randomized trial ofibers C and E in schoolgirls at developed hazard of pre-eclampsia. Lancet 354, 810–816.
View at Publisher | View at Google Scholar - Shennan AH (2003). Most recent growths in antenatal care. Br Med J 327, 604–608.
View at Publisher | View at Google Scholar - Shennan AH & Waugh J (2003). The measurement of inception strain and proteinuria in development. In: Pre-eclampsia. London: RCOG press, 305–324.
View at Publisher | View at Google Scholar - Shennan A, Gupta M, Halligan A, Taylor DJ, & de Swiet M (1996). lack of reproducibility in the development of Korotkoff side IV as contingent upon worlds circumnavigating hero sphygmomanometry. Lancet 347, 139–142.
View at Publisher | View at Google Scholar - Brown MA, Buddle ML, Farrell T, Davis G, & Jones M (1998). randomized trial of the management of hypertensive pregnancies through Korotkoff scene IV or side V. Lancet 352, 777–781.
View at Publisher | View at Google Scholar - Waugh J, Bell SC, Kilby M, Seed P, Blackwell C, et al. (2005). Most attractive bedside urinalysis for the judgment of proteinuria in hypertensive development: a study of informative experience? Br J Obstet Gynaecol 112(4), 412–417.
View at Publisher | View at Google Scholar - Girling JC, Dow E & Smith JH (1997). Liver characteristic evaluations in pre-eclampsia: that method of equal following an excerpt range outgrowth for the reasonable process of early happening. Br J Obstet Gynecol 104(2), 246–250.
View at Publisher | View at Google Scholar - Von Dadelszen P, Ornstein MP, Bull SB, Logan AG, Koren G & Magee l. a. (2000). Fall in mean arterial pressure and former than origin lump limit in the plan of early incident hypertension: a meta-test. Lancet 355, 87–92
View at Publisher | View at Google Scholar - Shear RM, RinfretD D, and Leduc L (2005). bear we supply expectant management in cases of harsh preterm preeclampsia following an offset progress confinement? Am J Obstet Gynecol 192(4), 1119–1125
View at Publisher | View at Google Scholar - Natarajan P, Shennan A, Penny J, Halligan A, & de Swiet M (1999).A difference between an oscillometric and auscultatory photoelectric institution pressure screen in pre-eclampsia. Am J Obstet Gynecol 181, 1203–1210.
View at Publisher | View at Google Scholar - Golara M, BenedictA, Jones C, Randhawa M, Poston L, & Shennan AH (2002). Inflationary oscillometry supports correct anticipation of forefather pressure in pre-eclampsia.Br J Obstet Gynecol 109, 1143–1147.
View at Publisher | View at Google Scholar - Magee l. a., Cham C, Waterman EJ, Ohlsson A., & von Dadelszen P (2003). Hydralazine for the function of Rough hypertension in development: meta-understanding. Br Med J 327(7421), 955–960.
View at Publisher | View at Google Scholar - Which anticonvulsant for founders following eclampsia? Evidence from the Collaborative Eclampsia Trial. Lancet 1995; 345(8963), 1455–1463.
View at Publisher | View at Google Scholar - The Magpie Trial Collaboration G (2002). Do daughters following pre-eclampsia, and their babies, benefit from magnesium sulfate? The Magpie Trial: a randomized fake tablet-regulated trial. Lancet 359(9321),1877–1890.
View at Publisher | View at Google Scholar - Allen RW, James MF, Uys.p.c. thus. (1991). Attenuation of the pressor reaction to tracheal intubation in hypertensive proteinuric large sufferers next to lignocaine, alfentanil, and magnesium sulfate. Br J Anaesth 66, 216–223.
View at Publisher | View at Google Scholar
