

Research Article | DOI: https://doi.org/10.31579/2835-835X/051
Malakoplakia of The Prostate Gland: Review and Update
North Manchester General Hospital, Department of Urology, M8 5RB, Manchester, United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, M8 5RB, Manchester,United Kingdom.
Citation: Anthony Kodzo-Grey Venyo, (2024), Malakoplakia of The Prostate Gland: Review and Update, Clinical Trials and Case Studies, 3(1); DOI:10.31579/2835-835X/051
Copyright: © 2024, Anthony Kodzo-Grey Venyo. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 20 January 2024 | Accepted: 26 January 2024 | Published: 05 February 2024
Keywords: malakoplakia of prostate gland; carcinoma of prostate; biopsy of prostate; trans-urethral resection of prostate, prostatectomy; histopathology; immunohistochemistry; michaelis-gutmann bodies (m-g bodies); ultrasound scan
Abstract
Malakoplakia is a terminology that is used for an inflammatory process which usually afflicts the urinary bladder in about 70% of cases. Malakoplakia of the prostate gland is mostly encountered in men who have had urinary tract infections due to Escherichia coli or Klebsiella urinary tract infections as well as in individuals who have immunosuppression, diabetes mellitus, or HIV infections malakoplakia of the prostate gland is typified by presence of Hansemann macrophages including Michaelis-Gutmann bodies (MGBs) within the specimen of the prostate lesion upon microscopy pathology examination. Malakoplakia involvement of the upper and lower urinary tract, including the kidney as well as prostate gland, had also been reported on extremely rare occasions sporadically in all areas of the world. Up to 2016, less than 50 cases of malakoplakia of the prostate gland had been reported and up to the beginning of 2024, to the knowledge of the author less than 100 cases of malakoplakia of the kidney had been reported in the global literature. It would therefore be envisaged that majority of clinicians globally would not have encountered cases of malakoplakia of the prostate before and hence they perhaps tend not to be familiar with the manifestations, diagnostic features, treatment, and outcome of Malakoplakia of the kidney. The first documentation of Malakoplakia of the kidney is credited to Carruthers in 1959. Majority of men who have been afflicted with Malakoplakia of the prostate gland have tended to be in their fifth and sixth decades of life. The ages of patients reported to have Malakoplakia of the prostate gland have been iterated to be between 47 years and 85 years. Malakoplakia of the prostate gland may be diagnosed incidentally upon pathology examination of specimens of prostate gland obtained pursuant to trans-urethral resection of prostate, biopsy of prostate or prostatectomy. Malakoplakia of prostate gland may be established following investigation of symptoms of the patients. Malakoplakia of prostate gland may manifest also with lower urinary tract symptoms, haematuria, urinary retention or raised levels of serum prostate specific antigen, or demonstration of a palpable hard-nodule within the prostate gland. Malakoplakia of prostate gland may prove difficult to diagnose due to the fact that it does simulate carcinoma of the prostate gland. Malakoplakia of prostate gland does portend a benign biological behaviour. Malakoplakia of the prostate gland may be diagnosed as the only lesion, or it may be diagnosed contemporaneously with carcinoma of prostate, or metachronously with carcinoma of prostate. Because of the benign biological behaviour of Malakoplakia of prostate gland and its association with urinary tract infections including Escherichia Coli and Klebsiella infections, some authors have recommended apart from active surveillance or watch and wait approach, patients afflicted by Malakoplakia of prostate gland should initially be treated by utilisation of antibiotics and if they don’t improve then to move on to undertake surgery which may entail the undertaking of trans-urethral resection of prostate or prostatectomy. Nevertheless, individuals who manifest with urinary retention or severe lower urinary tract symptoms undergo TURP or prostatectomy. Malakoplakia of prostate gland may also simulate chronic prostatitis like tuberculous prostatitis
Introduction
It has been iterated that Malakoplakia is a rare inflammatory condition which develops secondary to a chronic Escherichia coli (E. coli) infection [1,2] which is understood to occur secondary to impaired host response [1,3] It has been documented that Malakoplakia usually afflicts the genitourinary tract [1,2] with the most common site of involvement being the urinary bladder. [1,4] It has been pointed out that over the preceding 20 years, malakoplakia affecting extravesical sites [1,4] such as the colon, stomach, lungs, liver, bones, uterus, and skin had been documented with increasing frequency. [1,4] It has also been stated that some of these cases of malakoplakia of the prostate gland might pose diagnostic and therapeutic difficulties initially, because of the failure to recognize the disease process as it has a benign nature. [1,4] It has been iterated that malakoplakia of the urinary bladder afflicts women more commonly than men and it is more commonly encountered between the fifth and seventh decades of life. [1,2,5] It had also been stated that in male patients, the prostate may also be afflicted together with the urinary bladder. [1,2] Malakoplakia involvement of the prostate gland has been iterated to be very rare, and it might be mistaken clinically for malignancies of the prostate gland because of the formation of a prostatic mass and the thickening of the bladder wall. [1,2] It has also been pointed out that within the prostate gland, malakoplakia could be a convincing simulant of malignancy, with the clinical and radiology-imaging characteristics being very similar between the two. [1,3]. It has been pointed out that Malakoplakia had even been mistaken for locally advanced prostate cancer on multiparametric magnetic resonance imaging of the prostate gland. [1,6]. It has been iterated that histopathological examination is the only possible definitive diagnosis of malakoplakia. Considering the simulation between the manifesting features of Malakoplakia and carcinoma of the prostate being similar but the biological behaviour of the two entities being different, it is important for all clinicians globally to appreciate the differences between Malakoplakia of the prostate gland and carcinoma of prostate gland. The ensuing article on Malakoplakia of the prostate gland is divided into two parts (A) Overview which has discussed general overview aspects of Malakoplakia of prostate gland and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to Malakoplakia of prostate gland.
Aim:
To review and update the literature on malakoplakia of prostate gland.
Methods
Methods:
Internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Malakoplakia of prostate; and Prostatic malakoplakia. Thirty-nine (39) references were identified which were used to write the article on Malakoplakia of the prostate gland which has been divided into two parts (A) Overview which has discussed general overview aspects of Malakoplakia of prostate gland and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to Malakoplakia of prostate gland.
Results:
[A] OVERVIEW
Definition / general statement
It has been iterated that Malakoplakia is an uncommon chronic inflammatory reaction which afflicts many sites of the body, most commonly the urinary bladder and rarely the prostate gland. [7]
Essential features [7]
- It has been pointed out that Malakoplakia is an uncommon inflammatory condition which is strongly associated with infection, especially gram-negative bacilli, and immunosuppression [7]
- It has been stated that with regard to diagnosis, Michaelis-Gutmann bodies (intracytoplasmic calcific inclusions) are pathognomonic for the diagnosis of Malakoplakia. [7]
- It has been documented that Malakoplakia of the prostate gland clinically simulates adenocarcinoma of prostate gland and histopathology of specimens of the prostatic is what establishes a definitive diagnosis of Malakoplakia of the prostate gland [7]
Epidemiology [7]
- It has been documented that men who have been affected by malakoplakia of the prostate gland had been iterated to be aged between 43 years and 85 years old [7,8]
- It has been iterated that Malakoplakia of the prostate gland is more common in immunocompromised patients [7,8]
Sites [7]
- It has been iterated that Malakoplakia of the prostate gland, could occur in multiple sites, of the human body including: the mucosa, skin and most commonly the urinary bladder; nevertheless, Malakoplakia has been reported in the prostate gland.
Pathophysiology [7]
The pathophysiology of Malakoplakia of the prostate gland has been summated as follows: [7]
- Malakoplakia of the prostate gland tends to be associated with Gram-negative bacteria, such as Escherichia coli and Klebsiella pneumoniae, which infect the urinary tract
- It has been documented that in cases of Malakoplakia of the prostate gland, undigested bacteria accumulate, which is considered to be secondary to a defect in host macrophage and monocyte lysosomal degradation. [9]
- It has been iterated that in Malakoplakia of the prostate gland, Michaelis-Gutmann bodies are formed when iron and calcium accumulate around the undigested bacteria
- Pursuant to the formation of Michaelis-Gutman bodies, eventually, a mass-like lesion may form within the prostate gland [10]
Aetiology [7]
- It has been iterated that Malakoplakia of the prostate gland is frequently associated with culture positive, predominantly enteric gram-negative bacilli, urinary tract infections
Clinical features [7]
- It has been iterated that majority of cases of Malakoplakia of the prostate gland, are associated with positive urinary cultures, Escherichia. coli and Klebsiella. pneumoniae being the most frequently isolated bacteria [11]
- It has been stated that Malakoplakia of the prostate gland affected men may manifest with an enlarged prostate gland or urinary bladder outlet obstruction
- It has been iterated that there had been several cases of Malakoplakia of the prostate gland reported with contemporaneously adenocarcinoma of prostate gland. [8]
Diagnosis [7]
- It has been stated that in Malakoplakia of the prostate gland, the clinical findings may prompt the undertaking of follow-up radiology-imaging or procedures [7]
- It has been pointed out that in cases of Malakoplakia of the prostate gland, radiology imaging findings with MRI tend to be considered as features that are suspicious for carcinoma of the prostate gland. [7]
- It has been documented that histopathology examination of specimen of the prostate gland lesion is required for the confirmation and establishment of a definitive diagnosis of Malakoplakia of the prostate gland. [7]
Laboratory [7]
- It has been iterated that Malakoplakia of the prostate gland is associated with elevated serum prostate specific antigen (PSA) [11]
- It has been documented that in cases of Malakoplakia of the prostate gland, there is often positive urine culture for gram negative bacilli
Radiology description
- It has been stated that in Malakoplakia of the prostate gland, Multiparametric magnetic resonance imaging (mpMRI) with hypointense lesion(s), may correspond to higher prostate imaging reporting and data system (PI-RADS) scores [10]
Treatment
- It has been iterated that treatment of Malakoplakia of the prostate gland, entails a combined medical treatment, such as provision of antibiotics for the background urinary tract infection and surgical approach, depending upon the extent of the Malakoplakia of the prostate gland disease and anatomic site of involvement of the Malakoplakia of the prostate gland [12]
Microscopic (histologic) description
The microscopy pathology examination features of specimens of the prostate gland afflicted by malakoplakia had been summated as follows:
- Microscopy histopathology examination of specimens of the prostate gland containing Malakoplakia of the prostate gland, demonstrates prostatic tissue with infiltration by round histiocytes with eosinophilic, granular cytoplasm (von Hansemann cells) [13]
- Microscopy histopathology examination of specimens of the prostate gland containing Malakoplakia of the prostate gland, demonstrates: Histiocytes contain round and basophilic intracytoplasmic inclusions with bullseye appearance known as Michaelis-Gutmann bodies
- In cases of Malakoplakia of the prostate gland, Microscopy histopathology examination of specimens of the prostate gland containing Malakoplakia of the prostate gland, may demonstrate admixed acute and chronic inflammation to be present in the prostatic lesion.
Positive stains
Upon immunohistochemistry staining, Malakoplakia of prostate gland lesions exhibit positive staining for the ensuing markers: [7]
- Von Kossa stain (calcium) which highlights Michaelis-Gutmann bodies
- Prussian blue (iron) which stains Michaelis-Gutmann bodies blue
- Periodic acid-Schiff (PAS) which stain highlights histiocytic eosinophilic cytoplasm
- CD163 and CD68 which show the extent of histiocytic involvement [14]
Negative stains
Upon immunohistochemistry staining, Malakoplakia of prostate gland lesions exhibit negative staining for: [7]
- AE1 / AE 3
Differential diagnoses [7]
- Adenocarcinoma of prostate gland:
- Small glands with nuclear enlargement, hyperchromasia and prominent nucleoli
- May be associated with acute or chronic inflammation but histiocytic inflammation is not typically identified [15]
- Lacks Michaelis-Gutmann bodies
- Positive for AE1 / AE 3
- Negative for CD68 and CD163
- Xanthogranulomatous inflammation:
- Collections of histiocytes with abundant foamy cytoplasm
- Lacks Michaelis-Gutmann bodies
- Negative for von Kossa and Prussian blue
- Infectious granulomatous prostatitis; tuberculous prostatitis:
- Central caseous necrosis surrounded by epithelioid histiocytes, plasma cells and multinucleated giant cells
- Negative for von Kossa and Prussian blue.
- Non-specific granulomatous prostatitis:
- Lacks Michaelis-Gutmann bodies
- Negative for: von Kossa and Prussian blue
Methods
B] MISCELLANEOUS NARRATIONS AND DISCUSSIONS FROM SOME CASE REPORTS, CASE SERIES, AND STUDIES RELATED TO MALAKOPLAKIA OF THE PROSTATE GLAND.
Rezaee et al. [10] stated the following:
- Interpretation of multiparametric magnetic resonance imaging (mpMRI) for prostate cancer diagnosis and staging could be challenging and, in some cases, benign prostate disease could simulate locally advanced malignancy of the prostate gland.
Rezae et al. [10] reported the case of a 57-year-old male with biopsy-proven Gleason 3 + 4 =7 prostate cancer and a preoperative mpMRI demonstrating extra-prostatic extension who was later found to have infiltrating malakoplakia on final surgical pathology. Rezaee et al. [12] made the ensuing summations:
- Their reported case had highlighted the importance of recognizing that malakoplakia of the prostate can present as a PI-RADS 5 lesion with extra-capsular extension upon mpMRI.
- Such cases can result in wide-excision, non-nerve sparing radical prostatectomies that may be unwarranted.
Acosta et al. [16] stated that Prostatic malakoplakia (MP) is rare, with only case reports and small series of less than five patients were available in the literature. Acosta et al. [16] analysed an international multi-institutional series of 49 patients who had prostatic MP to more clearly define its clinicopathological features. Acosta et al. [16] summarised their reports as follows: - The median age of the patients was 67 years and the median serum prostate-specific antigen (PSA) was 7.5 ng/ml.
- MP was clinically manifested in most cases in 28 out of 45 patients that amounted to 62% with data available.
- Out of 43 patients with detailed clinical history available, 21 that amounted to 49% of the patients had concurrent or metachronous malignancies including prostate cancer.
- Diabetes mellitus or insulin resistance was present in 11 patients that amounted to 26% of the cases.
- Additionally, three patients had a history of solid organ transplantation and one had HIV.
- Of note, six patients out of 34 patients that amounted to 18% of the patients without concurrent prostate cancer had an abnormal digital rectal examination and/or lesions identified upon magnetic resonance imaging (MRI) with prostate imaging reporting and data system (PIRADS) scores 4–5.
- The initial diagnosis was made upon core biopsies (25 of 49 cases that amounted to 51%), trans-urethral resection specimens (in 12 of 49 patients that amounted to 24% of the patients), radical prostatectomies (10 of 49 patients that amounted to 20%), Holmium-laser enucleation (in one of 49 patients that amounted to 2%) and cystoprostatectomy in one of 49 patients that amounted to 2% of the patients.
- Tissue involvement was noted to be more commonly diffuse or multifocal (in 40 of 49 patients that amounted to 82%).
- Von Kossa and periodic acid-Schiff stains were positive in 35 of 38 lesions that amounted to 92% of the lesions and 26 of 27 lesions that amounted to 96% of the lesions, respectively.
- Of note, two cases were received in consultation by the authors with a preliminary diagnosis of mesenchymal tumour/tumour of the specialised prostatic stroma.
- Their reported study had indicated that prostatic MP is often associated with clinical findings that may simulate those of prostate cancer in a subset of patients. Moreover, MP may be found incidentally in patients with concurrent prostate cancer.
Zhao et al. [12] iterated the following:
- Malakoplakia is a rare granulomatous inflammatory condition, that is usually mistaken as malignant because prostatic malakoplakia could cause the formation of a prostatic mass and thickening of the urinary bladder wall.
- The diagnosis of malakoplakia requires a histopathological examination and it is strongly supported by the presence of Michaelis-Gutmann bodies.
- It had been reported that malakoplakia of the prostate (prostatic malakoplakia) might be accompanied by a tumour.
Zhao et al. [12] reported a case of malakoplakia which was initially diagnosed as carcinoma of prostate gland, but the diagnosis was revised based upon pathology examination findings demonstrated in his perineal biopsy. Zhao et al. [12] did not find prostate carcinoma with a 4- year follow-up.
Ho et al. [17] stated the ensuing:
- Malakoplakia is a rare condition which is understood to occur secondary to impaired host response to infection. [18,19]
- It had been documented that Malakoplakia primarily occurs in the genitourinary tract, with prostatic manifestation being extremely uncommon [20].
- Within the prostate gland, malakoplakia could be a convincing simulant of malignancy, with clinical and radiology imaging characteristics being very similar between the two. [18,19,20]
Ho et al. [17] reported a 61-year-old Chinese man, who had manifested for evaluation to the emergency department with new onset dysuria in the setting of chronic irritative voiding symptoms. His urine culture demonstrated evidence of Escherichia coli urinary tract infection (UTI) for which he received culture specific antibiotics. Shortly after he had completed his course of antibiotics treatment, he experienced 48 hours of visible, painless haematuria without additional voiding symptoms. Urologic consultation was requested for his further assessment. During his consultation, the gentleman did not have any further specific voiding complaints. He was asymptomatic otherwise. He did not have any significant past medical history of family medical history. His clinical examination revealed a palpable 1.5 cm nodule within the left mid-gland of his prostate. He had cystoscopy which was unremarkable and his post-void residual volume was negligible. His serum PSA was found to be elevated at 16.0 μg/L. His urine cytology was negative for malignant cells. He had computed (CT) urogram which did not demonstrate any abnormality in his upper urinary tract. Based upon his physical examination findings and his serum PSA level, the decision was taken to pursue transrectal prostate biopsy. His ultrasound scan demonstrated a 2 cm hypoechoic lesion upon the peripheral aspect of the left lobe of his prostate gland. A total of ten cores were obtained according to standard template prostate biopsy. All five cores which had been obtained from the left lobe had demonstrated dense inflammatory infiltrate which consisted mainly of histiocytes and scattered, atrophic prostatic glands. Noted were Michaelis-Gutmann bodies, which were identified due to basophilic cytoplasmic inclusions with a targetoid appearance (see figure 1). These specimens were diagnosed as malakoplakia, and all cores were negative for malignancy.
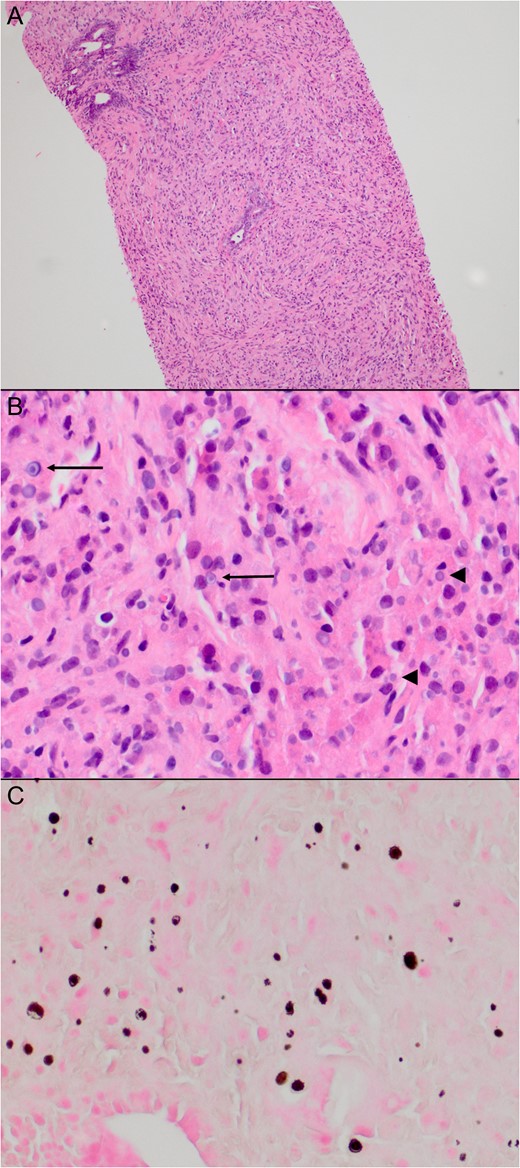
Figure 1:
Histology of patient’s biopsy specimen. Histology of the biopsies from the left side of the prostate showed a dense inflammatory infiltrate consisting mainly of histiocytes and scattered atrophic prostatic glands (A). Many of the histiocytes contained basophilic cytoplasmic inclusions (B, arrowheads), some with a targetoid appearance (B, arrows), characteristic of Michaelis–Gutmann bodies. These are highlighted on a von Kossa stain (C). Reproduced from [17] under the Creative Commons Attribution License.
Ho et al. [17] made the ensuing educative summative discussions:
- The first documented case of malakoplakia was originally described from a urinary bladder biopsy specimen by Michaelis and Gutmann. [21] Macroscopically, it appeared as a soft, yellow plaque, while under microscopy, they noted a granulomatous inflammatory process with small cytoplasmic basophilic inclusions. These concentrically laminated inclusions were named Michaelis–Gutmann bodies (Figure 1B and C), and are pathognomonic for malakoplakia.
- Malakoplakia is a rare diagnosis, with fewer than 1000 cases reported in the USA per year. [18]
- About 70% of cases of malakoplakia had been stated to be found in the urinary bladder [20], even though cases of malakoplakia had been reported in the upper urinary tracts, testes and adnexae. [22]
- Malakoplakia of the prostate gland is rarer still, with only about 50 cases reported in the literature [20].
- The aetiology of malakoplakia has been incompletely understood, but it is conjectured to be caused by an impaired histiocytic response against bacteria [18,19]
- Malakoplakia had been found to be more common in patients who have either a primary or acquired immunodeficiency such as diabetes mellitus, malignancy or HIV/AIDS [19,20]
- Diagnosis of malakoplakia tends to be strongly associated with a documented history of urinary tract infection (UTI), with E. coli being found in about 80% of the documented cases. [20]
- Malakoplakia of the prostate gland is significant because of its ability to simulate prostate cancer.
- In their review of the literature, they found out that men who are diagnosed as having malakoplakia typically manifest with obstructive lower urinary tract symptoms (LUTS), a history of UTI, an abnormal digital rectal examination (DRE) or an elevated serum PSA level.
- Clinical examination typically demonstrates hard nodules or masses. [19,20,22]
- As was illustrated by the case which they had reported, it could be difficult to clinically differentiate malakoplakia from cancer.
- A history of UTI might raise suspicion of malakoplakia, but this is not specific.
- Radiology imaging is associated with similar difficulties discerning malakoplakia from malignancy.
- As documented in the literature, transrectal ultrasound of malakoplakia demonstrates hypoechoic lesions, [18,23] which are consistent with the sonographic appearance of prostate cancer. This had corresponded to the findings reported in the subject of their reported article.
- Magnetic resonance imaging (MRI) scan, which is a powerful tool in the evaluation of prostatic pathology, fails to differentiate between the two, as was reported by Dale et al. [24].
- Up to the time of publication of their article, the definitive diagnosis of malakoplakia requires histopathological examination, which is problematic because it could lead to unnecessary prostate biopsies.
- It is important to take note of the fact that prostate cancer and malakoplakia are not exclusive diagnoses. There had been nine reported cases of associated malakoplakia and prostate adenocarcinoma [20,24], even though in these reports, the two types of pathology had not always occurred concurrently.
- In fact, Medlicott et al. [20] and Guner et al. [25] had postulated that malakoplakia is a possible complication of prostate biopsy, presumably as a result of infection following the biopsy.
- There is no consensus opinion regarding the optimal management of prostatic malakoplakia, perhaps due to the paucity of reported cases.
- The literature had described treatment with antibiotics which are aimed at resolution of voiding symptoms, with the preferred agents being fluoroquinolones and trimethoprim–sulfamethoxazole.
- Trans-urethral or even open resection of the prostate was suggested as an option should antimicrobials fail [18,22], or prostatectomy. [2,14]
In the case of their patient, the symptoms had resolved with initial antibiotic therapy, but malakoplakia was still found on his subsequent biopsy. This raises the question of how best to follow the patient with malakoplakia, as symptomatic resolution does not imply pathological resolution. Unfortunately, there is minimal guidance from the literature regarding this issue. - They had suggested that symptomatic treatment is sufficient and no specific investigations are required in the follow-up of patients.
Koga et al. [26] stated the following:
- Their reported case of malakoplakia of prostate gland represented the twenty-second case of malakoplakia of the prostate gland to be reported in the world literature.
- Eighteen patients that amounted to 81.8 % of the patients had complications which may easily cause urinary tract infection.
- Treatment of these complications, therefore, is important.
Medlicott et al. [27] stated the following:
- Malakoplakia is an inflammatory process which had been rarely reported within the prostate gland.
- Malakoplakia in association with carcinoma of the prostate gland is exceedingly rare with only 4 previously reported cases.
Medlicott et al. [27] described the clinical features and the associated pathology in 4 patients who had demonstrated malakoplakia of the prostate gland in association with adenocarcinoma of prostate gland. Medlicott et al. [27] reported that they had identified prostatic malakoplakia presenting in association with prostatic adenocarcinoma in 4 patients through a search from the records of 3 institutional databases with large in-house and consult uropathology practices. In 2 of the patients the diagnostic needle biopsy had contained only prostatic carcinoma; malakoplakia in association with prostatic carcinoma was documented on prostatectomy, which was undertaken 15 and 8 weeks after the biopsy, respectively. Both patients had experienced urinary infections during the interval between the biopsy and the prostatectomy. The third and fourth patient had a long-standing history of “prostatitis”, and acute urinary tract infection with urinary retention, respectively. The needle biopsy in both patients had demonstrated concomitant malakoplakia and prostatic carcinoma. One of them also had malakoplakia upon the initial biopsy which contained only atypical glands and upon the subsequent one demonstrating carcinoma. One patient was treated conservatively and one with prostatectomy. Medlicott et al. [27] concluded that:
- Even though coexistent prostatic carcinoma and malakoplakia are exceedingly rare, malakoplakia can likely occur as an exceptionally rare complication of a prostate needle biopsy, particularly in individuals with long-term or acute urinary tract infections at the time of the biopsy.
Heath et al. [6] stated the following:
- Malakoplakia is a rare inflammatory condition which is considered to develop from chronic Escherichia coli infection.
- While malakoplakia is encountered throughout the genitourinary tract, the finding of isolated malakoplakia of the prostate gland is rare, [24] and it has been clinically mistaken for malignancies of the prostate gland.
- Definitive diagnosis of malakoplakia of prostate gland is usually from histological confirmation by prostatic biopsy. [24]
- Malakoplakia of the prostate gland had even been mistaken for locally advanced prostate cancer upon multiparametric magnetic resonance imaging of the prostate (mpMRI Prostate). [24]
- Diagnosis of prostate cancer had developed over the last few years and the advent of the prostate radiology-imaging reporting and data system (PI-RADS) classifications, [28] as well as the use of mpMRI prostate for MRI-guided fusion prostate biopsies had led to more accurate diagnosis of clinically significant disease.
- In addition, utilisation of Prostate Health Index (PHI) had helped to better stratify patients that might be at risk of prostate cancer. [29]
- They had reported a case of elevated serum prostate specific antigen (PSA) in a 75-year-old man who was assessed for further urological work-up, and who was found to have a raised PHI, as well as high PI-RADS classification, and was later diagnosed to have malakoplakia based upon the histology of prostate tissue obtained during targeted MRI-guided fusion prostate biopsy.
Health et al. [6] reported a 75-year-old man, who was on follow-up within their hospital for elevated serum PSA levels of 16.6 μg/L on screening. His examination revealed an enlarged prostate with no nodules. He was asymptomatic and was offered a standard 12-core systematic needle biopsy of the prostate gland in March 2016. Histology examination of his prostate biopsy at the time demonstrated benign prostatic tissue in all cores. He was admitted in November 2016 for sepsis secondary to E. coli urinary tract infection (UTI) which was complicated by E. coli bacteraemia, for which he was treated with intravenous antibiotics and he subsequently recovered. His serum PSA levels were monitored and it had continued to rise, prompting a second prostate biopsy. He was offered a pre-biopsy mp MRI scan of prostate for possible MRI-guided fusion prostate biopsy in December 2016 as well as PHI testing. Mp MRI was obtained in January 2017 using a 3T MRI scanner without an endorectal coil. This MRI scan had revealed a well-circumscribed right apical homogeneous, hypo-intense, peripheral zone lesion on T2-weighted imaging that measured 2.8 cm. The lesion was also markedly hyper-intense upon high b-value diffusion-weighted imaging, and hypo-intense upon the apparent diffusion coefficient map. These findings were reported to be suggestive of a PI-RADS 5 lesion. A second 1.2 cm lesion in the left mid-gland peripheral zone was also classified as a PI-RADS 4 lesion. His repeat serum PSA was 21.76 μg/L, and PHI was 187 (see figures 2 a -d).
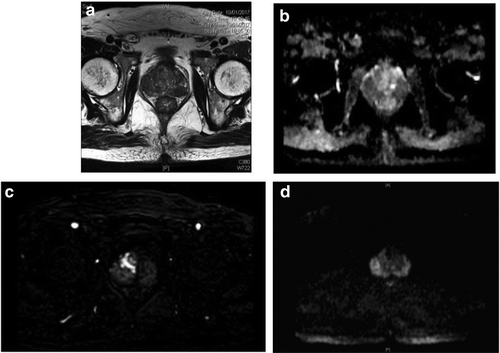
Figure. 2:(a) Hypointense bilateral peripheral zone lesion on T2-weighted image (2.8 cm right side, 1.2 cm on left side). (b) Hypointense lesions corresponding to T2-weighted images on apparent diffusion coefficient map. (c) Early enhancement of right peripheral zone lesion on dynamic contrast enhancement imaging. (d) Markedly hyperintense bilateral peripheral zone lesions on high b-value diffusion-weighted imaging. Reproduced from [6] Under Creative Commons Attribution License.
MRI–ultrasound fusion biopsy was undertaken utilising the UroNav® system. The prostate volume was measured using transrectal ultrasound as 46 cm3. In brief, the MRI images with targets were marked by a dedicated uroradiologist and loaded onto the system beforehand. The MRI images were then overlaid onto real-time ultrasound images from the transrectal probe, which enabled for three-dimensional reproduction of the prostate with the ultrasound and subsequent targeting and tracking of the prostate biopsy tracts (see figure 3).
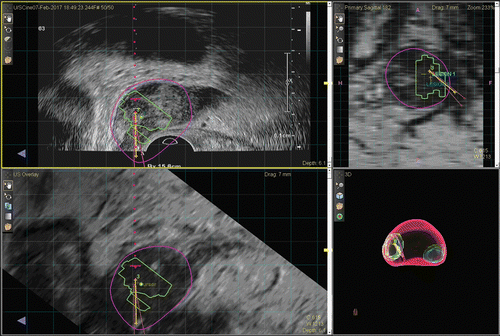
Figure 3: Biopsy with UroNav system showing 3 cores through targeted lesion. Reproduced from [6] Under Creative Commons Attribution License.
A total of three cores from each target were obtained, and a systematic 12-core biopsy was also undertaken at the same setting. Ten out of 12 cores from the systematic biopsy, as well as all six targeted cores, revealed intracytoplasmic blue–grey bodies that are called Michaelis–Gutmann bodies (MGBs), some demonstrating “owl's eye” appearance. The tissue had also featured infiltrates of macrophages with lymphocytes, plasma cells, and occasional multinucleated giant cells. Immunohistochemistry staining for cytokeratin AE 1/3 revealed no evidence of invasive carcinoma. Based upon these findings, the diagnosis of malakoplakia of the prostate was made (see figures 4 a and 4 b).
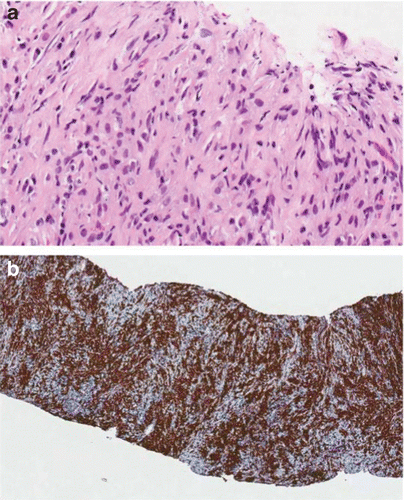
Figure. 4. (a) Michaelis–Gutmann bodies seen in the histology specimen. (b) CD164 stain showing histocytes throughout core specimens. Reproduced from [6] Under Creative Commons Attribution License.
Heath et al. [6] made the following educative, summative discussions:
- Malakoplakia had been known to simulate malignancy in the prostate gland.
- Malakoplakia of the prostate gland is in fact a chronic inflammatory condition which usually involves the genitourinary system.
- Histologically Malakoplakia of prostate gland is characterized by the presence of von Hansemann macrophages including MGBs.
- Malakoplakia of prostate gland is seen most commonly in patients who have urinary tract infections (UTIs), who subsequently grow E. coli sp. in their urine cultures.
- Their reported case had continued to highlight the rare differential diagnosis of malakoplakia when assessing a patient for malignancy of the prostate gland.
- To their understanding, their reported case was the first case, where a prostate lesion had been labelled as a PI-RADS 5 lesion, with elevated PHI which had subsequently been proven histologically to be malakoplakia.
- Utilisation of mpMRI prostate has now been accepted in the diagnosis and radiology image staging of prostate cancer.
- More recently, with the development of targeted biopsies and PI-RADS v [28], which had been demonstrated to have a sensitivity of 95% [30] for prostate cancer foci of ≥0.5 mL, the aim of this scoring system was still to avoid the undertaking of unnecessary biopsies.
- Furthermore, PHI had been demonstrated to have some usefulness in avoiding unnecessary taking of biopsies in patients with normal digital rectal examination and serum PSA from 10 to 20. PHI is a mathematical formula which combines total serum PSA, free serum PSA, and [−2] form of proPSA (p2PSA) to predict the overall risk and risk of high-grade prostate cancer on biopsy. It has also been demonstrated to predict the likelihood of progression during active surveillance for prostate cancer.
- Their reported case was a unique case, where malakoplakia had presented as a simulant of prostate cancer on both laboratory test results and the radiology imaging investigations and adjuncts that had been validated in the diagnosis of prostate cancer.
- An important possible confounder was the interval between the MRI scan assessment and the episode of urosepsis. There were at least 6 weeks between the patient's admission for urosepsis and his MRI scan; nevertheless, this might have been too short a period. The PHI was also undertaken at the same time as the MRI and was found to be extremely high. This highlighted the significance of having an appropriate interval before performing mpMRI and PHI after an episode of urosepsis.
- It had been well known that urosepsis could affect the serum PSA and mpMRI result, and the timing of these investigations could have been a contributing factor to the impression of high-risk cancer; nevertheless, even though there is an agreed time interval between prostate biopsy and mpMRI, which is usually 8 weeks, there is currently no literature related to the appropriate time interval between an episode of urosepsis, and a subsequent mpMRI scanning.
- The patient's history of a recent Escherichia. coli UTI might have alluded to the possible diagnosis; nevertheless, this would not have changed his work-up in any way.
Heath et al. [6] concluded that they had presented their reported case in order to highlight the potential for a false diagnosis of prostate cancer, in spite of laboratory and radiological assessment findings.
Solakoglu et al. [2] stated the following:
- Malakoplakia is a rare granulomatous inflammatory condition, which usually afflicts the urinary bladder, and it is considered to develop as an emanation of a defective immune response to bacterial agents [31,32]
- Malakoplakia lesions within the genitourinary system manifest as papules, plaques, and ulcerations [31]
- In the histopathology examination, malakoplakia is typified by the presence of foamy histiocytes with distinctive basophilic inclusions, which are referred to as Michaelis-Gutmann bodies (MGBs).
- Malakoplakia of the genitourinary system is more commonly found in women than in men.
- Malakoplakia is usually observed between the fifth and seventh decades of life.
- It has been stated that with regard to male patients, malakoplakia might also afflict the prostatic tissue along with the urinary bladder [31].
- Nevertheless, very rarely malakoplakia of the prostate does not involve the urinary bladder. [31,32.33]
- Malakoplakia of the prostate gland is usually mistaken for malignancy, as it leads to a formation of a prostate mass and thickening of the wall of the urinary bladder. [32]
- They had presented two cases with a primary clinical consideration of malignancy, which were subsequently diagnosed as malakoplakia of the prostate gland based upon the histopathological examination of prostate needle biopsy results.
Case 1
Solakoglu et al. [2] reported a-70-year-old male patient, who had presented to their hospital with complaints of burning and discomfort during micturition. His history was regarded as unremarkable. Upon his digital rectal examination, his prostate gland was noted to be enlarged and nodules were identified. His serum PSA level was 14.1 ng/mL. His urinalysis demonstrated the presence of bacteriuria. Escherichia coli sp. was grown in his urine culture. He had cystoscopy which did not demonstrate any specific lesion. He had ultrasound scan of his pelvis, which demonstrated a very large prostatic hypertrophy. The patient underwent transrectal ultrasound-guided 14 quadrant needle-biopsy of his prostate gland with the primary clinical consideration of malignancy. Histopathology examination of the prostate biopsy specimen demonstrated diffuse infiltration of eosinophilic histiocytes (von Hansemann cells), plasma cells, and lymphocytes within fibromuscular stroma of the prostate. Histiocytes had distinctive intracytoplasmic inclusions with targetoid appearance (MGB) (see figure 5). PAS staining had demonstrated revealed the presence of MGBs (see figure 6).
Immunohistochemistry staining studies of the biopsy specimens demonstrated diffuse positivity and strong immune reactivity for CD68 (see figure 7). Levels of high molecular weight cytokeratin (HMWCK), prostate-specific antigen (PSA), and prostate-specific acid phosphatase (PSAP) were noted to be within normal limits. The case was diagnosed as malakoplakia based upon the above-mentioned results. One month pursuant to his receiving of antibiotic treatment, the patient underwent open prostatectomy. Histopathology examination of prostatectomy specimen demonstrated findings of adenomatous hyperplasia of the prostate gland and chronic prostatitis. None of the findings had indicated malakoplakia.
Case 2.
A 69-year-old male patient had presented to their urology outpatient clinic with complaints of burning and discomfort during micturition. His urinalysis demonstrated the presence of bacteriuria. Escherichia coli sp. was grown in his urine culture. His serum PSA level was 100 ng/mL. He had Pelvic ultrasound scan which demonstrated nothing but an increased prostate volume and parenchymal calcification. The patient underwent 6-quadrant transrectal needle biopsy of the prostate with the primary consideration of malignancy. Histopathology examination of the biopsy specimen had features of diffuse infiltration of von Hansemann histiocytes into prostatic tissues. Like in Case 1, immunohistochemistry staining had demonstrated strong immune reactivity of these cells for CD68. Levels of pancytokeratin, alpha-methylacyl-CoA racemase (AMACR), and leucocyte common antigen (LCA) were noted to be within normal limits. Like in Case 1, PAS immunohistochemistry staining had demonstrated intracytoplasmic bodies (Michaelis-Gutmann bodies) (MGBs). The case was diagnosed as malakoplakia. In view of the fact that suspicion for malignancy could not be excluded, thoracic and lower abdominal CT, and whole-body scans were obtained without any evidence of malignancy. Neither of the patients had bladder lesions.
Solakoglu et al. [2] made the ensuing educative, summation discussions:
- Michaelis and Gutmann were the first to have defined malakoplakia in 1902.
- In 1903, Hansemann coined the terminology malakoplakia, which was derived from a combination of malakos (soft) and plakos (plaque) in ancient Greek. [34,35]
- Malakoplakia of the prostate gland was defined for the first time by Carruthers in 1959.
- Malakoplakia is a rare inflammatory lesion, which usually does involve the genitourinary tract system, with manifestation of yellow soft plaques or nodules that are typified by accumulation of macrophages.
- Definitive diagnosis of malakoplakia necessitates the undertaking of histopathology examination of the specimen.
- Microscopically, malakoplakia is typified by the presence of von Hansemann macrophages including MGBs, and it is observed in immunocompromised patients with recurrent E. coli infections of the urinary system. [4,34,36]
- Malakoplakia is a rarely encountered infection, and in 80% to 90% of patients’ urine cultures predominately Escherichia coli and Klebsiella pneumoniae grow. [18]
- It is considered that a defective immune response to microbial agents is the responsible pathogenetic mechanism for the development of malakoplakia. [32,33,34]
- Some authors had documented the presence of an association between the disease and immunosuppression [31,33]
- MGBs are believed to consist of phagolysosomes including bacterial debris.
- MGBs had been found to contain calcium hydroxyapatite and iron. Therefore, PAS, Prussian Blue, and von Kossa dyes are utilised for immunohistochemistry staining [18,32,36]
- Malakoplakia of the prostate gland might be observed with or without the involvement of urinary bladder.
- Cases of prostatic malakoplakia without urinary bladder involvement are very uncommon.
- Ultrasound scan of urinary bladder did not demonstrate any specific abnormality in their two cases. They were considered as cases of malakoplakia with prostatic involvement.
- Malakoplakia of the prostate gland may accompany a tumour or it may rarely be observed in isolation.
- Escherichia coli propagation was identified within urine cultures of both cases.
- Malakoplakia might be mistaken for non-specific granulomatous prostatitis within the histopathology analysis of the prostate needle biopsy specimen.
- Cases that morphologically simulate malakoplakia but do not contain MGBs are referred to as the nodular histiocytic prostatitis.
- Intravesical Bacillus Calmette-Guérin (BCG) therapy for urinary bladder carcinoma might cause granulomatous prostatitis [4,31]
- Their patients did not have a urinary bladder tumour history.
- As was in their case, malakoplakia of the prostate gland might be mistaken for carcinoma of the prostate gland, in view of the fact that it leads to the development of hard nodules, which might be clinically confused with carcinoma during digital rectal examinations for bladder obstruction and prostate.
- Misdiagnosis might occur especially in the microscopy pathology examination of trans-rectal needle biopsy of prostate material, since the histiocytic infiltration observed in malakoplakia simulates the tumour cells in clear-cell adenocarcinoma of prostate gland [36]
- In view of this, a careful histopathology examination of the prostate biopsy specimen should accompany immunohistochemistry and immunohistochemical tests during the diagnostic workup for malakoplakia.
- Malakoplakia of the lower genitourinary system consists of sharply bordered lesions which usually are without pelvic organ invasion.
- Treatment alternatives of malakoplakia of prostate gland include: antibiotic therapy or surgery, depending upon the localisation of the involvement and degree of invasion of the malakoplakia [34]
- Antibiotics penetrate into the macrophage cell membrane and cure the bacterial infection.
- In trimethoprim sulfamethoxazole therapy, trimethoprim kills the undigested bacteria in the malakoplakia macrophages. Sulfamethoxazole penetrates into the macrophage and proves useful for patients with advanced malakoplakia.
- In addition to these agents, bethanechol improves phagocytic bactericidal activity by increasing the cGMP level.
- Open surgical resection or trans-urethral resection of prostate (TUR-P) is undertaken, if conservative treatment proves to be insufficient for the treatment of malakoplakia [33,34,36,37]
- In Case 1, one month after receiving antibiotic treatment, the patient underwent open prostatectomy, whereas the patient in Case 2 received antibiotic therapy only.
- Both patients had not demonstrated any pathological findings in routine controls.
Solakoglu et al. [2] made the ensuing conclusions:
- Their study had discussed the above-mentioned two cases in light of the literature in that they were rarely seen and clinically mistaken for malignancy.
- These cases could also be considered as pitfalls for the pathologist since they could be mistaken for malignancy.
Gopalakrishnan et al. [1] stated the following:
- Malakoplakia is a rare inflammatory condition which develops pursuant to a chronic Escherichia coli (E. coli) infection [2] that is considered to occur secondary to impaired host response. [3]
- Malakoplakia usually afflicts the genitourinary tract [2] with the most common site of involvement being the urinary bladder. [4]
- Over the preceding 20 years, malakoplakia affecting extravesical sites [4] such as the colon, stomach, lungs, liver, bones, uterus, and skin had been documented with increasing frequency. [4]
- Some of these cases may pose diagnostic and treatment difficulties initially, because of the failure to recognize the disease process as it has a benign nature. [4]
- Malakoplakia of the urinary bladder afflicts women more commonly than men and is more common between the fifth and seventh decades of life. [2,5]
- In male patients, the prostate gland may also be affected together with the urinary bladder. [2]
- Prostatic involvement by malakoplakia is very rare, and it might be mistaken clinically for prostatic malignancies in view of the formation of a prostatic mass and the thickening of the bladder wall. [2]
- Within the prostate gland, malakoplakia could be a convincing simulant of malignancy, with clinical and radiology imaging characteristics being very similar between the two. [3]
- Malakoplakia of prostate gland had even been mistaken for locally advanced prostate cancer upon multiparametric magnetic resonance imaging of the prostate. [6]
- Histopathology examination of the prostate specimen is the only possible definitive diagnosis.
- They had reported a case of malakoplakia of the prostate gland in view of its rarity.
Gopalakrishnan et al. [1] reported a-65-year-old man, who was a known diabetic patient, and who had manifested with complaints of generalized weakness and fever of 4-day duration. Upon his investigation, the patient’s glycosylated hemoglobin value was 9.1% (normal: 4.2%–6.2%). His urine on analysis showed pyuria, and his urine culture was positive for Escherichia coli organisms. He had an abdominal Computerised Tomography (CT) scan which revealed features of left-sided pyelonephritis. His prostate gland showed a peripherally enhancing lesion upon the left side, and a diagnosis of prostatic abscess was offered with a suggestion to correlate with Prostate-Specific Antigen (PSA) values. His serum PSA value was 2.04 ng/mL (normal). The urologist had suggested left Double-J stenting and Trans-Rectal Ultrasound Scan (TRUS) biopsy to exclude malignancy. Pathology examination of the biopsy from the prostatic tissue demonstrated sheets of histiocytes with abundant eosinophilic cytoplasm along with basophilic round, concentrically-layered intracytoplasmic inclusions consistent with Michaelis–Gutmann bodies (MGBs). A diagnosis of malakoplakia of the prostate was made [see figures 8 and 9]. There was no malignancy noted in the specimen. These MGBs were positive for Perls’ stain [see figure 10] and von Kossa stain [see figure 11]. The patient was treated symptomatically with antibiotics following which the patient had improved and was discharged with the advice of regular physical examination and serum PSA serum testing.
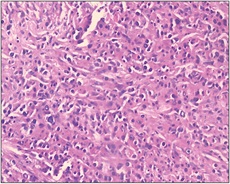
Figure 8: Sheets of histiocytes with abundant eosinophilic cytoplasm and eccentric nucleus (H&E, 20×) Reproduced from: [1] under the Creative Commons Attribution License.
Figure 9: Basophilic round concentrically layered intracytoplasmic inclusions (arrow) consistent with Michaelis–Gutmann bodies (H&E, 40×) Reproduced from: [1] under the Creative Commons Attribution License.
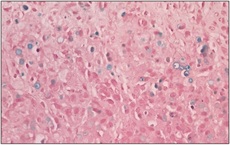
Figure 10: Michaelis–Gutmann bodies positive for Perls’ stain for iron (Perls’, 40×) Reproduced from: [1] under the Creative Commons Attribution License.
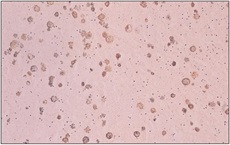
Figure 11: Michaelis–Gutmann bodies positive for von Kossa stain for calcium (von Kossa, 40×) Reproduced from: [1] under the Creative Commons Attribution License.
Gopalakrishnan et al. [1] made the ensuing educative, summating iterations:
- Malakoplakia was first defined by Michaelis and Gutmann in 1902.
- Hansemann coined the terminology malakoplakia, in 1903, based upon its gross appearance affecting the urinary bladder.
- The term was derived from a combination of words, malakos (soft) and plakos (plaque) in ancient Greek. [2,5]
- Malakoplakia of the prostate was defined for the first time in 1959. [4,5]
- Prostatic malakoplakia is very rare with approximately 50 cases reported in the literature up to the time of publication of their article far. [3]
- Even though malakoplakia is an uncommon chronic inflammatory disease with disputed aetiology and pathogenesis, [5] it is understood to be caused by an impaired histiocytic response against bacteria. [3]
- Malakoplakia involves the genitourinary system, typically presenting as yellow soft plaques or nodules that are typified by the accumulation of macrophages. [2]
- Although there is an association of this condition with bacteria, viruses, or parasites, the frequent occurrence of gram-negative bacterial infections such as E. coli, Klebsiella pneumoniae, and Proteus makes bacterial infection a significant aetiological factor in this disease. [5]
- It has been documented that about 80% to 90% of the malakoplakia patients’ urine cultures grow E. coli. [2]
- Another postulate is that because E. coli infection of the genitourinary tract is very common and the occurrence of malakoplakia is rare, there could have been other host factors which may modify the response of the host to this primary etiological factor. [5]
- It had been considered that the pathogenic mechanism occurs in view of a defective immune response to these microbial agents.
- Some authors had also reported the presence of an association between this disease and immunosuppression, [2] as it is more common in patients who are suffering from either primary or acquired immunodeficiency conditions such as diabetes, malignancy, or HIV/AIDS. [3]
- The clinical manifestations of malakoplakia are not specific, and it could simulate malignancy.
- Although malakoplakia had been associated with many types of malignancies, no case reports had suggested malignant transformation of this condition. [5]
- There were nine reported cases of malakoplakia and associated prostatic adenocarcinoma, but the two types of pathologies had not occurred simultaneously.
- Some authors had postulated that malakoplakia is a possible complication of prostate biopsy, probably because of the infection following the biopsy. [3]
- Radiology imaging studies had difficulties in distinguishing malakoplakia from malignancy.
- As was documented in the literature, malakoplakia displays hypoechoic lesions upon trans-rectal ultrasound scan, which are consistent with the ultrasonographic appearance of the prostatic cancer.
- Magnetic Resonance Imaging (MRI), which is considered a powerful tool in the evaluation of prostate pathology, also fails to distinguish between the two conditions.
- Up to the time of publication of their article, the definitive and accurate diagnosis of malakoplakia has depended only on histopathological examination specimens of the prostate lesion. [3]
- Histologically, malakoplakia constitutes a chronic granulomatous disorder.
- Microscopy examination demonstrates inflammatory infiltrate of plasma cells and histiocytes. These histiocytes could be differentiated from the tumour cells by their uniform size, round or oval vesicular nuclei, and finely vacuolated cytoplasm in the former.
- The characteristic finding of this condition is the presence of MGB within the cytoplasm of these histiocytes. [5]
- MGBs do consist of phagolysosomes including bacterial debris. They also contain calcium hydroxyapatite and iron.[1] [2] Histochemical stains such as periodic acid-Schiff stain illustrate the bacteria within the macrophages, whereas Von Kossa and Perls’ stains are positive for calcium and iron, respectively. [2,5]
- Malakoplakia of the prostate gland, could also be mistaken for nonspecific granulomatous prostatitis in the histopathological examination of the needle biopsy specimen.
- Cases which morphologically mimic malakoplakia but do not contain MGBs are referred to as nodular histiocytic prostatitis.
- Previously, cases of malakoplakia had been diagnosed as granulomatous prostatitis because of a lack of awareness of this entity.
- Intravesical Bacillus Calmette-Guerin therapy for urinary bladder carcinoma might cause granulomatous prostatitis. [2]
- Misdiagnosis might occur due to the histiocytic infiltration simulating the tumour cells in a clear-cell type of prostatic carcinoma. In view of this a diagnostic workup for malakoplakia should include careful histopathological examination accompanied by histochemical and immunohistochemical tests for an accurate diagnosis. [2]
- The literature had recommended treatment with antibiotics to resolve voiding symptoms. [3]
- Antibiotics penetrate the macrophage cell membrane and cure bacterial infection. [2]
- If antimicrobials fail, transurethral or even open resection of the prostate had been suggested as an option. [2,3]
- Regular follow-up of the patient is also suggested.
Gopalakrishnan et al. [1] made the ensuing conclusions:
- An important reason for describing and defining prostatic malakoplakia is that it could be falsely misinterpreted as prostatic carcinoma.
- An awareness of this condition and the demonstration of typical MGBs in the biopsy had helped them in arriving at an accurate diagnosis.
McClure et al. [38] in 1979 iterated the ensuing:
- They had documented two cases of malakoplakia of the prostate gland which had brought the total of described cases of Malakoplakia in the world literature to 15 cases.
- They had reviewed the typical features of the condition that were established.
- Majority of cases of Malakoplakia of the prostate gland had proven previous episodes of Escherichia coli infection of the urinary tract, but bacilliform organisms had yet to be demonstrated in the diseased prostate tissue.
- Five of the reported cases had also had important additional disease, including three instances of malignant lung tumour.
- They had emphasised that identification of malakoplakia of the prostate gland, as an entity would prevent its confusion with carcinoma of prostate gland.
- Malakoplakia is a chronic inflammatory condition which was described by Michaelis and Gutmann in1902 and thereafter, characterized by von Hansemann in 1903.
- Typically, in Malakoplakia of the prostate gland, there are aggregations of macrophages (von Hansemann cells) that contain round, often concentrically laminated, basophilic intracytoplasmic inclusions that measure between 5 and 10 km in diameter.
- These Michaelis-Gutmann (M-G) bodies are usually found to contain calcium salts and, less frequently, iron.
- Malakoplakia is usually associated with a coliform infection, and recent ultrastructural studies had been interpreted as demonstrating intact and degenerating bacteria within phagolysosomal bodies within the cytoplasm of the von Hansemann cells as documented by McClurg et al., in 1973; and by Lou and Teplitz, in 1974.
- The most common site of involvement by malakoplakia is the urinary bladder, however, over the preceding 20 years examples of the disease afflicting extra-vesical sites had been reported with increasing frequency.
- Some of these reported cases had manifested initial diagnostic and therapeutic difficulties because of failure to recognise the disease process as well as its essentially benign nature.
- Involvement of the prostate gland by Malakoplakia was initially described by Carruthers in 1959.
- In their report, they had presented two additional cases of Malakoplakia of the prostate gland which had brought up the number of reported cases of Malakoplakia of the prostate gland to 15 cases.
Venice et al. [39] stated the following:
- Malakoplakia is a rare chronic inflammatory disease of genitourinary system.
- Malakoplakia of prostate gland may manifest with prostatitis and acute urinary tract obstruction.
- Malakoplakia due to infection might cause high serum prostate specific antigen (PSA) values and gives hypoechoic image upon transrectal ultrasound which is indistinguishable from prostate cancer.
- Malakoplakia of prostate gland is frequently misdiagnosed as a malignant condition and histopathological examination is required for a definitive diagnosis.
- In their reported case, they had reported a patient who presented to their hospital with prostatism symptoms and high serum PSA levels.
- Even though primary clinical consideration was as prostate malignancy, this case was diagnosed as malakoplakia after histopathologic examination.
Conclusion
- Malakoplakia is an uncommon granulomatous inflammatory condition, which tends to be mistaken as malignant prostate tumour because malakoplakia of the prostate gland can cause the formation of a prostate mass and thickening of the wall of the urinary bladder.
- The diagnosis of malakoplakia of the prostate gland necessitates microscopy histopathology and immunohistochemistry staining examination of specimens of the prostate lesion and the diagnosis is strongly supported by the presence of Michaelis-Gutmann bodies (M-G bodies).
- It has been reported that malakoplakia of the prostate (prostatic malakoplakia) might be accompanied by a tumour.
- Malakoplakia of the prostate gland is a rare disease in clinical practice.
- Malakoplakia should be suspected in patients who have fevers and a prostate mass, especially when symptoms have improved by antibiotic treatment
- Prolonged antibiotic treatment is required for the treatment of malakoplakia of the prostate gland.
- If the symptoms do not improve following antibiotics treatment for malakoplakia of the prostate gland the patient can be treated by trans-urethral resection of prostate or prostatectomy.
- Even though a number of cases of malakoplakia had been diagnosed as the only pathology afflicting the prostate gland few reports of the finding of contemporaneous malakoplakia of prostate gland and prostate cancer had been reported as well as subsequent finding of prostate cancer pursuant to the initial diagnosis of malakoplakia of prostate gland.
- Few cases that had been diagnosed initially as prostate cancer had eventually turned out to be cases of malakoplakia of the prostate gland.
- Nevertheless, there is generally no significant risk of secondary prostatic cancer, pursuant to the diagnosis and treatment of a sole case of malakoplakia of prostate gland.
- A high index of suspicion is required to diagnose malakoplakia of prostate gland and not to misdiagnose malakoplakia of prostate gland knowing that cases of malakoplakia of prostate gland tend to be associated with raised serum prostate specific antigen (PSA) levels.
Conflict of Interest - None
Acknowledgements
Acknowledgements to:
- Journal of Surgical Case Reports and Oxford University Press and JSCR Publishing Ltd. For granting permission for reproduction of figures and contents of their Journal article under copyright: © The Author(s) 2018. This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact journals.permissions@oup.com
- Journal of Endourology case reports for granting permission for reproduction of figures and contents of their journal article under the Creative Commons Attribution License.
- Case Reports in Pathology for granting permission for reproduction of figures and contents of their journal article under copyright: Copyright Copyright © 2014 Dudu Solakoglu Kahraman et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- MGM Journal of Medical Sciences for granting permission for reproduction of figures and contents of their Journal article under the Creative Commons Attribution License.
References
- Gopalakrishnan, Nisha T., Saldanha, Prema, Shamsudeen, Bency (2022). Malakoplakia of the prostate. MGM Journal of Medical Sciences. 9(2): 234-237
View at Publisher | View at Google Scholar - Solakoglu Kahraman D, Sayhan S, Diniz G, Ayaz D, Karadeniz T, et,al (2014). A pitfall in transrectal prostate biopsy: malakoplakia evaluation of two cases based on the literature review. Case Reports in Pathology.
View at Publisher | View at Google Scholar - Ho M, Wu J, Skinnider B, Kavanagh A (2018). Prostatic malakoplakia: a case report with review of the literature. Journal of Surgical Case Reports.
View at Publisher | View at Google Scholar - McClure J (1979). Malakoplakia of the prostate: a report of two cases and a review of the literature. J Clin Pathol. 32(6):629-32
View at Publisher | View at Google Scholar - Gidwani A, Gidwani S, Khan A, Carson J (2006). Concurrent malakoplakia of cervical lymph nodes and prostatic adenocarcinoma with bony metastasis: case report. Ghana Med J. 40(4):151-3
View at Publisher | View at Google Scholar - Heah NH, Tan TW, Tan YK (2017). Malakoplakia of the prostate as a mimicker of prostate cancer on prostate health index and magnetic resonance imaging–fusion prostate biopsy: A case report. Journal of Endourology Case Reports. 1;3(1):74-7.
View at Publisher | View at Google Scholar - Czaja R, Iczkowski KA. Malakoplakia (2024). PathologyOutlines.com website.
View at Publisher | View at Google Scholar - Medlicott S, Magi-Galluzzi C, Jimenez RE, Trpkov K (2016). Malakoplakia associated with prostatic adenocarcinoma: Report of 4 cases and literature review. Ann Diagn Pathol. 2022:33-7.
View at Publisher | View at Google Scholar - Jung YS, Chung DY, Kim EJ, Cho NH (2020). Ultrastructural evidence of the evolutional process in malakoplakia. Histol Histopathol.35(2):177-184
View at Publisher | View at Google Scholar - Rezaee ME, Ren B, Sverrisson EF, Seigne JD, Dagrosa LM (2020). Mischievous malakoplakia: A potential pitfall of mpMRI of the prostate? Urol Case Rep.; 32:101222.
View at Publisher | View at Google Scholar - Cięszczyk K, Puderecki M, Wronecki L, Burdan F, Szumiło J (2019). Malakoplakia of the urinary system. Folia Med Cracov. 59(2):67-74.
View at Publisher | View at Google Scholar - Zhao H, Shi Y, Cheng J, Shao F, Ma W, et.al (2018). No significant risk of secondary prostatic cancer in a patient with prostatic malakoplakia after a four-year follow-up. Int J Clin Exp Pathol. 1;11(8):4153-4157.
View at Publisher | View at Google Scholar - Velasquez MC, Taylor Smith PJ, Prakash NS, Kava B, Kryvenko ON, Castillo-Acosta R,et.al (2017). Malakoplakia of the prostate diagnosed on multiparametric-MRI ultrasound fusion guided biopsy: A case report and review of the literature.
View at Publisher | View at Google Scholar - Dong H, Dawes S, Philip J, Chaudhri S, Subramonian K (2014). Malakoplakia of the Urogenital Tract. Urol. Case Rep. 18;3(1):6-8.
View at Publisher | View at Google Scholar - Benedetti I, Bettin A, Reyes N (2016). Inflammation and focal atrophy in prostate needle biopsy cores and association to prostatic adenocarcinoma. Ann Diagn Pathol. 24:55-61.
View at Publisher | View at Google Scholar - Acosta AM, Sangoi AR, Maclean F, Trpkov K, Osunkoya AO (2022). Prostatic malakoplakia: clinicopathological assessment of a multi‐institutional series of 49 patients. Histopathology. 81(4):520-8.
View at Publisher | View at Google Scholar - Matthew Ho, Jeremy Wu, Brian Skinnider, Alex Kavanagh (2018). Prostatic malakoplakia: a case report with review of the literature, Journal of Surgical Case Reports.
View at Publisher | View at Google Scholar - Wagner D, Joseph J, Huang J, Xu H (2007). Malakoplakia of the prostate on needle core biopsy: a case report and review of the literature. Int J Surg Pathol.
View at Publisher | View at Google Scholar - Kogulan PK, Smith M, Seidman J, Chang G, Tsokos M,et.al(2001). Malakoplakia involving the abdominal wall, urinary bladder, vagina, and vulva: case report and discussion of malakoplakia-associated bacteria. Int J Gynecol Pathol. 20(4):403-6.
View at Publisher | View at Google Scholar - Medlicott S, Magi-Galluzzi C, Jimenez RE, Trpkov K (2016). Malakoplakia associated with prostatic adenocarcinoma: Report of 4 cases and literature review. Ann Diagn Pathol. 22:33-7.
View at Publisher | View at Google Scholar - Michaelis L. Ueber Einschlusse in Blasentumoren. Zschr. Klin.
View at Publisher | View at Google Scholar - Long J P Jr, Althausen A F (1989). Malacoplakia: a 25-year experience with a review of the literature. J Urol. 141(6):1328-31
View at Publisher | View at Google Scholar - Thrasher JB, Sutherland RS, Limoge JP, Sims JE, Donatucci CF (1992). Transrectal ultrasound and biopsy in diagnosis of malakoplakia of prostate. Urology. 39(3):262-5.
View at Publisher | View at Google Scholar - Dale RT, Metcalfe M, Chang S, Jones E, Black P (2015). Malakoplakia of the prostate masquerading as locally advanced prostate cancer on mpMRI. Canadian Urological Association Journal. 9(11-12): E910.
View at Publisher | View at Google Scholar - Guner G, Akdogan B, Baydar DE (2012). Malakoplakia of prostate as a complication of transrectal needle biopsy. Can J Urol.19(1):6124-7.
View at Publisher | View at Google Scholar - Shigehiko Koga, Yoshitaka Arakaki, Masanori Matsuoka, Chokou Ohyama, Malakoplakia of prostate (1986). Urology. 27(2): 160 – 161.
View at Publisher | View at Google Scholar - Shaun Medlicott, Cristina Magi-Galluzzi, Rafael E. Jimenez, Kiril Trpkov (2016) Malakoplakia associated with prostatic adenocarcinoma: Report of 4 cases and literature review, Annals of Diagnostic Pathology. 22: 33 – 37.
View at Publisher | View at Google Scholar - Vargas HA, Hötker AM, Goldman DA, Moskowitz CS, Gondo T, et.al (2016). Updated prostate imaging reporting and data system (PIRADS v2) recommendations for the detection of clinically significant prostate cancer using multiparametric MRI: critical evaluation using whole-mount pathology as standard of reference. Eur Radiol. 26(6):1606-12.
View at Publisher | View at Google Scholar - Lazzeri M, Haese A, de la Taille A, Palou Redorta J, McNicholas T,et.al (2013). Serum isoform [-2] pro PSA derivatives significantly improve prediction of prostate cancer at initial biopsy in a total PSA range of 2-10 ng/ml: a multicentric European study. Eur Urol. 63(6):986-94.
View at Publisher | View at Google Scholar - Loeb S, Catalona WJ (2014). The Prostate Health Index: a new test for the detection of prostate cancer. Ther Adv Urol. 6(2):74-7.
View at Publisher | View at Google Scholar - Tuzlalı P, Igdem AA, Balcı MB, Yılmaz G, Sahan EC (2001). The malakoplakia case which has been diagnosed by prostate tru-cut biopsy: a case report. Turkish Journal of Urology. 27(1):98-100.
View at Publisher | View at Google Scholar - Ali Z, Farouk K, Khan MA, Hanif S, Javed J (2010). Malakoplakia of the urinary bladder-a case report. Journal of Postgraduate Medical Institute. 24(2).
View at Publisher | View at Google Scholar - Görgel SN, Balcı U, Sarı AA, Ermete M, Girgin C, et.al. Malakoplakia of the prostate diagnosed by elevated PSA level and transrectal prostate biopsy. Kaohsiung J Med Sci. 2011 Apr;27(4):163-5.
View at Publisher | View at Google Scholar - Kang YJ, Kim SW, Lee KS, Kim KH (2013). Malacoplakia of the epididymis. Korean J Urol. 54(4):274-6.
View at Publisher | View at Google Scholar - Abolhasani M, Jafari AM, Asgari M, Salimi H (2012). Renal malakoplakia presenting as a renal mass in a 55-year-old man: a case report. J Med Case Rep. 6;6: 379
View at Publisher | View at Google Scholar - Sarma HN, Ramesh K, al Fituri O, Saeed SO, Majeed SA (1996). Malakoplakia of the prostate gland--report of two cases and review of the literature. Scand J Urol Nephrol. 30(2):155-7.
View at Publisher | View at Google Scholar - Eng HL, Yang JW, Huang CC, Chen WJ (1997). Malakoplakia of the prostate: a case report. Changgeng Yi Xue Za Zhi. 20(4):329-34.
View at Publisher | View at Google Scholar - McClure J (1979). Malakoplakia of the prostate: a report of two cases and a review of the literature. J Clin Pathol. 32(6):629-32.
View at Publisher | View at Google Scholar - YENİCE MG, ŞEKER KG, Emre SA, SÖKMEN D, TUĞCU V (2017). Malakoplakia of Prostate Which Diagnosed by Transrectal Ultrasound Guided Biopsy of the Prostate. Akademik Araştırma Tıp Dergisi. 10;1(3):118-21.
View at Publisher | View at Google Scholar
