

Review Article | DOI: https://doi.org/10.31579/2834-796X/059
Low-dose aspirin use to attenuate the risk for cardiac arrest in marathon runners with subclinical coronary atherosclerosis
*Corresponding Author: Arthur J. Siegel, Department of Internal Medicine 2, McLean Hospital, Belmont, MA, Harvard Medical Schoo1 3, Boston, MA, USA.
Citation: Arthur J. Siegel, (2024), Low-dose aspirin use to attenuate the risk for cardiac arrest in marathon runners with subclinical coronary atherosclerosis, International Journal of Cardiovascular Medicine, 3(2); DOI:10.31579/2834-796X/059
Copyright: © 2024, Arthur J. Siegel. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 April 2024 | Accepted: 18 April 2024 | Published: 29 April 2024
Keywords: aspirin; cardiac arrest; marathon; primary cardiovascular prevention
Abstract
While habitual endurance exercise such as training for a marathon is quintessentially cardioprotective, running the race paradoxically increases the risk for cardiac arrest. Male gender and the marathon were identified as significant and independent risk factors for race-associated cardiac arrest in a 10-year registry in United States road races, which events increased significantly in frequency during the study. Fatalities occurred mainly in middle-aged men with coronary atherosclerosis as shown in a concurrent retrospective review. An explanation for this excess race-related cardiac mortality may emerge from observational studies in asymptomatic middle-aged male Boston marathon physician-runners which show post-race elevations in inflammatory biomarkers similar to findings in patients with acute myocardial infarction. Demonstrated as cardioprotective in two randomized controlled clinical trials, low-dose aspirin may attenuate the transiently elevated race-related risk for cardiac arrest in runners with subclinical coronary atherosclerosis. In the absence of contraindications, pre-race low-dose aspirin use is prudent for runners with coronary artery calcium scores greater than 100 Agatston units. This measure attenuates the transiently increased race-related risk for cardiac arrest and sudden death as identified by the presence of significant subclinical coronary atherosclerosis.
The cardiovascular paradox of marathon running:
While habitual endurance exercise such as training for a marathon is strongly cardioprotective, running the race transiently increases the risk for cardiac arrest and sudden cardiac death (1). Confirming this paradox, male gender and the marathon were identified as significant and independent risk factors for cardiac arrest in the 10-year Racer registry beginning in the year 2000 (2). While the low incidence of cardiac arrest (0.5 per 100,000 participants) was characterized as "good news" for marathon runners (3), such events increased in frequency during the latter half of the registry period.
A concurrent retrospective study determined that race-related fatalities occurred mainly in middle-aged men with underlying coronary atherosclerosis (4), providing the focus for an evidence-based strategy to mitigate such excess premature cardiovascular mortality. Low-dose aspirin use is a strong candidate for this purpose, having been demonstrated as cardioprotective in two randomized controlled primary prevention trials (5,6).
Emerging pathophysiological insights:
An explanation for the counterintuitive paradox of marathon running may emerge from observational studies in asymptomatic middle-aged Boston marathon male physician-runners. Post-race inflammatory biomarkers demonstrated the same "cytokine storm" seen in patients during acute myocardial infarction, including a hemostatic imbalance with pro-coagulant effects and in vivo activation of platelets (7,8). Cases of acute coronary thrombosis due to plaque rupture have been reported post-race in Boston marathon runners (9). Inflammation due to exertional rhabdomyolysis after "hitting the wall" during races may trigger acute coronary events, validating the hypothesis in the first study of Boston marathon runners after the inaugural race in 1897 that skeletal muscle injury can damage the heart (10). This pathogenic sequence is similar to the pro-atherogenic inflammatory response reported in human coronary vessels after SARS-CoV-2 infection (11). Aspirin use may thereby be adjunctively beneficial similar to vaccination to mitigate the severe cardiac complications of COVID infection (12).
Attenuating the transiently increased race-related cardiac arrest risk:
Low-dose aspirin use has been proposed to attenuate the increasing frequency of cardiac arrests during marathons, occurring mainly in middle-aged male runners with subclinical coronary atherosclerosis (13-16). Supported by the two randomized controlled primary prevention trials showing significant reductions in major acute cardiac events cited above, low-dose aspirin use for enhanced primary prevention in runners is analogous to this same strategy for patients with elevated lipoprotein a [Lp(a)] (17). Low-dose aspirin use to enhance primary prevention targets excess inflammation analogous to the adding low-dose colchicine for stronger secondary prevention (18).
Coronary artery calcium scoring to assess the benefit of low-dose aspirin use
Based on subclinical coronary atherosclerosis as the main cause of cardiac arrest in middle-aged male marathon runners, coronary artery calcium scoring (CACS) is recommended for participants including novice and experienced runners alike (19). The latter athletes may have elevated coronary artery calcium burden due to habitual endurance exercise, including those in the lowest quartile of risk by traditional calculators (20,21). CACS assess subclinical coronary atherosclerosis, which reliably predicts the risk for major acute cardiovascular events including sudden cardiac death (22,23).
In the absence of clinical contraindications, the anticipated benefit of low-dose aspirin use likely stratifies according to the results of CACS as shown in Table 1 (24). Runners with scores incrementally higher than 100 Agatston units especially benefit, as clear communication of cardiovascular disease risk improves receptivity to preventive measures as shown by meta-analysis (25). While aspirin does not protect against cardiac arrests due to causes other than coronary atherosclerosis, this agent carries a class 1A recommendation for pre-hospital administration in acute coronary syndromes by the American Heart Association and may contribute to favorable outcomes associated with advanced cardiac life support measures.
Discussion:
Some experts might feel that more data is needed before endorsing low-dose aspirin for primary prevention of cardiac arrest in marathon runners. Staunch evidence in two randomized controlled clinical trials demonstrates significant cardioprotective effects in the low-risk individuals and persons at intermediate risk (references # 5,6), while such a ‘gold standard’ trial specifically in runners lacks feasibility due to the infrequency of index events. Decision making on aspirin use guided by coronary artery calcium scoring for enhanced risk stratification is a win-win proposition, the efficacy of which might be assessed prospectively using registry data once this measure were to gain acceptance in the marathon running community.
Beyond its cardioprotective benefit in endurance athletes during marathons and triathlons (26), low-dose aspirin use warrants consideration for attenuating the increasing risk of sports-related sudden cardiac death in elderly persons (27). Enhanced risk stratification with coronary artery calcium scoring in such individuals can assess the benefit of low-dose aspirin for reducing the risk of exertional cardiac arrest including during leisure time exercise. The threshold for aspirin use may likely be higher in the elderly, however, given their greater risk for complications such as gastrointestinal bleeding.
Conclusion:
Low-dose aspirin use is evidence-based to reduce the transiently elevated race-related risk for cardiac arrest in runners with coronary atherosclerosis as assessed by coronary artery calcium scoring.
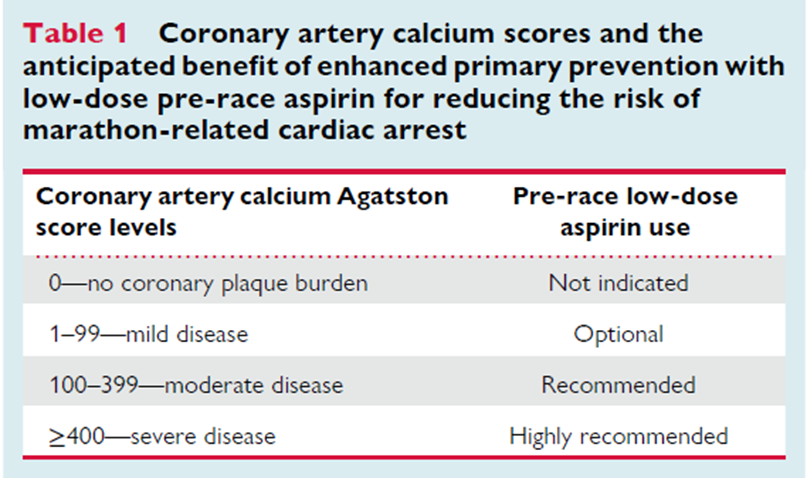
Table taken from reference # 24: Siegel A. Pre-race aspirin to attenuate the risk for marathon-related cardiac arrest: deconstructing the legacy of Pheidippides. Eur Heart J. 2023, ehad641. https://doi.org/10.1093/eurheartj/ehad641 25.
Acknowledgments:
The views herein are solely those of the author and do not reflect endorsement by any group or organization. There are no funding sources or conflicts of interest.
References
- Franklin BA, Thompson PD, Al-Zaiti SS, et al. On behalf of the American Heart Association Physical Activity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Stroke Council. Exercise-related acute cardiovascular events and potential deleterious adaptations following long-term exercise. Downloaded from http://ahajournals.org by on March 3, 2020. Exercise-Related Acute Cardiovascular Events Circulation 2020; 141:00-00.
View at Publisher | View at Google Scholar - Kim JH, Malhotra R, Chiampas G, et al. Cardiac arrest during long-distance running races. N Engl J Med. 2012;366(2):130-40.
View at Publisher | View at Google Scholar - Nearman S. Cardiac deaths in the marathons much lower than previously thought. J Am Med Athletic Assoc. 2012;1:7-8.
View at Publisher | View at Google Scholar - Mathews SC, Narotsky DL, Bernholt DL, et al. Mortality among marathon runners in the United States, 2000-2009. Am J Sports Med. 2012;40(7):1495-500.
View at Publisher | View at Google Scholar - Steering Committee of the Physicians' Health Study Research Group. Final report on the aspirin component of the ongoing Physicians' Health Study; N Engl J Med. 1989;321(3): 129-35.
View at Publisher | View at Google Scholar - TIPS-3 investigators. Polypill plus aspirin reduces incidence of cardiovascular events by 31%: TIPS-3 CardiovascJ Afr. 2021;32(1):32-40.
View at Publisher | View at Google Scholar - Siegel AJ, Stec JJ, Lipinska I, et al. Effect of marathon running on inflammatory and hemostatic markers. Am J Cardiol. 2001;88(8):918-20, A9.
View at Publisher | View at Google Scholar - Kratz A, Wood MJ, Siegel AJ, Hiers JR, VanCott EM. Effects of marathon running on platelet activation markers. direct evidence for in vivo platelet activation. Am J Clin Pathol 2006.125:296-300.
View at Publisher | View at Google Scholar - Albano AJ, Thompson PD, Kapur NK. Acute coronary thrombosis in Boston marathon runners. N Engl J Med. 2012;366(2):185-186.
View at Publisher | View at Google Scholar - Williams H, Aenold H. The effects of violent and prolonged exercise upon the heart. Phila Med J. 189:1233-1235.
View at Publisher | View at Google Scholar - Eberhardt N, Noval MG, Kaur R, et a. SARS-CoV-2 infection triggers pro-atherogenic inflammatory response in human coronary vessels. Nature Cardiovascular Research 2023;2:899-916.
View at Publisher | View at Google Scholar - Siegel AJ. Aspirin use for primary cardiovascular prevention during the COVID-19 pandemic. Am J Med 2020.
View at Publisher | View at Google Scholar - Siegel AJ. Pheidippides Redux: reducing the risk for acute cardiac events during marathon running. Am J Med. 2012;125:630-635.
View at Publisher | View at Google Scholar - Siegel AJ. Pre-race aspirin to protect susceptible runners from cardiac arrest during marathons: is opportunity knocking? Open Heart 2015;2e000102.
View at Publisher | View at Google Scholar - Siegel AJ, Noakes TD. Can prerace aspirin prevent sudden cardiac death during marathons? Br J Sports Med. 2017;51(22):1579-1582.
View at Publisher | View at Google Scholar - Siegel AJ. Pre-race aspirin for enhanced primary prevention of marathon-related cardiac arrest: confronting Pheidippides' legacy. Am J Med. 2023;136 (7):613-615.
View at Publisher | View at Google Scholar - Bhatia HS, Trainor P, Carlisle S, et al. Aspirin and cardiovascular risk in patients with elevated lipoprotein a [Lp(a)]: Multi-Ethnic Study of Atherosclerosis. JAHA. 2024;13:e033562.
View at Publisher | View at Google Scholar - Roubille F, Bouabdallaoui N, Kouz S, et al. Low-Dose Colchicine in Patients with Type 2 Diabetes and Recent Myocardial Infarction in the COLchicine Cardiovascular Outcomes Trial (COLCOT). Diabetes Care. 2024.
View at Publisher | View at Google Scholar - Siegel AJ, Noakes TD. Aspirin to prevent sudden cardiac death in athletes with high coronary artery calcium scores. Am J Med. 2019;132:138-141.
View at Publisher | View at Google Scholar - Aengevaeren VL, Mostard A, Bakker EA, et al. Exercise volume versus intensity and the progression of coronary atherosclerosis in middle-aged men and older athletes: findings from the MARC-2 Study. Circulation. 2023.
View at Publisher | View at Google Scholar - De Bosscher R, Dausin C, Claus P, Bogaert J, Dymarkowski S, Goetschalck K, et al. Lifelong endurance exercise and its relation with coronary atherosclerosis. Eur Heart J. 2023; httpsdl.d2Lu.gl.L0-U93.Leubeutjl.ghadJ52.
View at Publisher | View at Google Scholar - Razavi AC, Uddin SMI, Dardari ZA, et al. Coronary Artery Calcium for Risk Stratification of Sudden Cardiac Death: The Coronary Artery Calcium Consortium. JACC Cardiovasc Imaging. 2022;15(7):1259-1270.
View at Publisher | View at Google Scholar - Fuchs A, Kuhl JT, Sigvardsen PE, et al. Subclinical Coronary Atherosclerosis and Risk for Myocardial Infarction in a Danish Cohort: A Prospective Observational Cohort Study. Ann Intern Med. 2023;176(4):433-442.
View at Publisher | View at Google Scholar - Siegel A. Pre-race aspirin to attenuate the risk for marathon-related cardiac arrest: deconstructing the legacy of Pheidippides. Eur Heart J. 2023, ehad641.
View at Publisher | View at Google Scholar - Bakhit M, Fein S, Abukmail E, et al. cardiovascular disease risk communication and prevention: a meta–analysis. Eur Heart J. 2024; Jan 19.
View at Publisher | View at Google Scholar - Siegel AJ. Aspirin use to reduce the risk of sports-related cardiac arrest and high-risk athletes. Am J Med. 2018.
View at Publisher | View at Google Scholar - Holmstrom L, Chugh HS, Uy-Evanado A, et al. Sports-related sudden cardiac arrest in older individuals JACC: Clinical Electrophysiol 2023;9(7Pt1):893-903.
View at Publisher | View at Google Scholar
