

Case Report | DOI: https://doi.org/10.31579/2834-5029/007
Low Delta Blood Urea Nitrogen and Poor Postnatal Growth in Extremely Low Gestational Age Newborn (ELGAN) Infants
- Shabih Manzar *
* Neonatal Intensive Care Unit, Ochsner LSU Health, Shreveport, LA, USA
*Corresponding Author: Shabih Manzar, Louisiana State University Health Sciences Center, Department of Pediatrics, 1501 Kings Highway, Shreveport, LA 71103, USA
Citation: Manzar S. (2022) Low Delta Blood Urea Nitrogen and Poor Postnatal Growth in Extremely Low Gestational Age Newborn (ELGAN) Infants. International Journal of Biomed Research. 1(2): DOI: 10.31579/2834-5029/007
Copyright: © 2022, Shabih Manzar, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 November 2022 | Accepted: 30 November 2022 | Published: 09 December 2022
Keywords: blood urea nitrogen; gestational age; weight
Abstract
Blood urea nitrogen (BUN) concentrations have shown to be associated with post-natal growth. [1] Protein intake affects the BUN levels in preterm infants. Protein intake affects the BUN levels in preterm infants.
Introduction:
In extremely low gestational age newborns (ELGANs), the higher limit of BUN is 21 mg/dL, and the reference range for these preterm infants is 3-21 mg/dL (1.1–7.5 mmol/L). [3] In a recent study, Thanh et al [4] showed higher BUN as a marker of better postnatal growth. They described significantly higher BUN levels in the high protein formula group than in the control group. To look at the levels of difference in BUN level (delta BUN) and postnatal growth in ELGANs, we performed this study.
We selected four ELGANs ranging from 23-25 weeks of gestation and study their BUN levels with postnatal growth. We calculated the delta BUN (the difference in the BUN level from birth to the day of assessment). The cases are briefly described below. The summary of the findings is displayed n Table 1.

To monitor their growth, we use the formulae as described earlier (Table 2). [5,6]
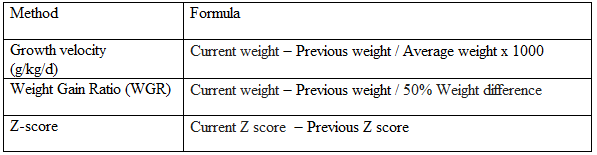
Average weight = Current weight + Previous weight / 2
50% Weight difference = 50% weight at current weight - 50% weight at previous weight
Z-Score: From electronic chart or https://peditools.org/fenton2013/
Table 2: Calculation of GV, WGR and Delta Z [5,6]
Case 1:
Preterm infant, gestational age 25 3/7 weeks. The pregnancy was complicated by no prenatal care, uncontrolled hypertension, and vaginal bleeding. The Apgar score was 3, 6, 7 at 1, 5, and 10 minutes. The infant was intubated in the delivery room. On admission to the NICU, umbilical venous and arterial catheters were inserted. The infant was placed on a high-frequency oscillator ventilator and was started on total parental nutrition. Serum electrolytes were monitored daily while on TPN, and then on enteral feeds as needed. On the day of analysis, the infant was 20 days old.
Case 2:
Preterm infant, gestational age 24 5/7 weeks. The pregnancy was complicated by concern for placental abruption. The infant was intubated in the delivery room. On admission to the NICU, umbilical venous and arterial catheters were inserted. The infant was placed on a high-frequency oscillator ventilator and was started on total parental nutrition. Serum electrolytes were monitored daily while on TPN, and then on enteral feeds as needed. On the day of analysis, the infant was 26 days old.
case 3:
Preterm infant, gestational age 23 1/7 weeks. The mother did not receive any steroids. The Apgar score was 0, 6, 7 at 1, 5, and 10 minutes. The infant was intubated in the delivery room. On admission to the NICU, umbilical venous and arterial catheters were inserted. The infant was placed on a high-frequency oscillator ventilator and was started on total parental nutrition. Serum electrolytes were monitored daily while on TPN, and then on enteral feeds as needed. On the day of analysis, the infant was 32 days old.
Case 4:
Preterm infant, gestational age 24 2/7 weeks. The pregnancy was complicated by premature prolonged rupture of the membrane. The Apgar score was 2, and 7, at 1 and 5 minutes. The infant was intubated in the delivery room. On admission to the NICU, umbilical venous and arterial catheters were inserted. The infant was placed on a high-frequency oscillator ventilator and was started on total parental nutrition. Serum electrolytes were monitored daily while on TPN, and then on enteral feeds as needed. On the day of analysis, the infant was 50 days old.
Discussion
We were able to demonstrate a low delta BUN level in a small group of ELGANs. All infants had poor postnatal growth. The growth velocity rate of less than 10 g/kg/day as observed in all the cases (Table 1) was inadequate. Further, all ELGANs had a low weight gain ratio (WGR). A WGR closer to 1 indicates adequate growth. Similarly, the delta z- score remained negative in all the cases (Table 1). We did not look at the daily protein intake and calories of the individual cases. We are planning a prospective study to look at all the nutritional details in correlation to delta BUN.
Author Contribution:
Conceptualized and wrote the manuscript.
Financial Disclosure Statement:
No funding to disclose.
Competing Interests Statement:
No competing interests to declare.
References
- Roggero P, Giannì ML, Morlacchi L, et al. (2010) Blood urea nitrogen concentrations in low-birth-weight preterm infants during parenteral and enteral nutrition. J Pediatr Gastroenterol Nutr.51(2):213-215.
View at Publisher | View at Google Scholar - Weintraub AS, Blanco V, Barnes M, Green RS. (2015). Impact of renal function and protein intake on blood urea nitrogen in preterm infants in the first 3 weeks of life. J Perinatol.;35(1):52-56.
View at Publisher | View at Google Scholar - Zhang Y, Zeng HH. (2020) Renal Function Profiles in Preterm Neonates With Birth Asphyxia Within the First 24 H of Life. Front Pediatr. 2020;8:583540.
View at Publisher | View at Google Scholar - Thanh LQ, Chen Y, Hartweg M, Thi Nguyen TA. (2022) Effects of higher protein formula with improved fat blend on growth, feeding tolerance and nutritional biomarkers in preterm infants: A double-blind, randomized, controlled clinical trial. Pediatr Neonatol.;63(3):227-238.
View at Publisher | View at Google Scholar - Rochow N, Landau-Crangle E, So HY, et al. (2019) Z-score differences based on cross-sectional growth charts do not reflect the growth rate of very low birth weight infants. PLoS One.14(5).
View at Publisher | View at Google Scholar - Patel AL, Engstrom JL, Meier PP, Jegier BJ, Kimura RE. (2009) Calculating postnatal growth velocity in very low birth weight (VLBW) premature infants. J Perinatol; 29(9): 618-22.
View at Publisher | View at Google Scholar
