

Research Article | DOI: https://doi.org/10.31579/2835-8325/055
Logotherapy and Cognitive Reframing in the Management of Blame Attribution Among Cancer Patients
1,2 Department of Counselling and Human Development Studies, Faculty of Education, University of Ibadan, Nigeria,
3 Faculty of Education, Prince Abubakar Audu University Anyigba, Nigeria
*Corresponding Author: Muraina Kamilu Olanrewaju, Faculty of Education, Prince Abubakar Audu University Anyigba, Nigeria
Citation: Muraina Kamilu Olanrewaju, (2024), Logotherapy and Cognitive Reframing in the Management of Blame Attribution Among Cancer Patients, Clinical Research and Clinical Reports, 5(3); DOI: 10.31579/2835-8325/055
Copyright: © 2023, Edem G.D. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 September 2024 | Accepted: 15 October 2024 | Published: 08 November 2024
Keywords: blame attribution; logotherapy; cognitive reframing; cancer patient; wellbeing
Abstract
This study ascertained how Cognitive Reframing (CR) and Logotherapy (LT) affected how recently diagnosed cancer patients managed their assigning of blame. A quasi-experimental pretest-posttest control group design was used in the study. For screening, the Blame Attribution Questionnaire (α=0.81) was employed. Fifty-four cancer patients were chosen based on their high Blame Attribution Screening score. The subjects were divided into three groups at random: control (15), CR (21), and LT (18). Descriptive statistics, analysis of covariance, and multiple classification analysis post-hoc test at the 0.05 significance level were used to analyze the data. The average age of the participants was 53.85±7.89 years, with 88.9% being female. Breast cancer (53.7%), cervical cancer (33.3%), prostate cancer (9.3%), and skin cancer (3.7%) are the cancer types that participants suffer from. The participants' attribution of blame was significantly affected by the treatment (F(2;42) = 16.03; partial = 0.43). More people benefited from the CR (x ̅ = 42.91) than from the LT (x ̅ = 63.56) or the control (x ̅ = 66.87) groups. In newly diagnosed cancer patients, blame attribution was effectively managed with the help of logotherapy and cognitive reframing. These therapies should be used by clinical psychologists and counselors to manage blame attribution in newly diagnosed cancer patients.
Introduction
The first question asked by patients receiving a cancer diagnosis is typically "Why?" In order to understand what they may have done or not done that may have contributed to the diagnosis, and patients may feel guilty about themselves. Sometimes, patients believe that their lifestyle choices could have influenced their diagnosis. The patient's belief that the condition is hereditary may be influenced by genetic factors. Spiritual or mental issues could be the subject of the "Why?" question. The knowledge that they have a potentially fatal illness such as cancer causes them to react in different ways in patients. When a patient receives a cancer diagnosis, almost all of them typically go through various phases. Feelings of shock, disbelief, anxiety, fear, despair, anger, guilt, and depression are among them (Kantor, 2016). Receiving a cancer diagnosis presents many difficulties that could negatively affect a patient's mental health, causing them to experience depression, unstable emotions, denial of the diagnosis, and rage (Iddrisu, Aziato, and Dedey, 2020). After receiving a cancer diagnosis, most people experience shock and denial initially. This is usually followed by a period of distress marked by a mix of anxiety, anger, and occasionally depression. Withdrawal, avoidance, blame, loss of control, loneliness, loss of dignity, despair, meaninglessness, low mood, and physical manifestations are some other typical feelings that may be experienced (National Cancer Institute, 2018).
However, Humans are prone to placing blame for a negative experience on somebody or something, which serves as a defense for their behaviors and affairs (Banerjee, Gidwani, and Sathyanarayana, 2020). Receiving a cancer diagnosis, no matter what kind, can be frightening and cause a person to experience a wide range of challenging emotions that can have a detrimental impact on many aspects of their life. In clinical settings, it is not uncommon to witness recently diagnosed cancer patients blaming other people or even non-medical factors for their illness. Some patients may even go so far as to refer to the condition as something other than cancer simply because they disagree with the health-related community's diagnosis. These ideas significantly impact the patients because they may seek a cure through alternative means rather than accepting conventional medicine. This would mean a great deal of effort, money, and time would be squandered, and by the time the patient chooses to get medical care, the illness may have advanced to a point where treatment cannot advance, and the prognosis becomes more hazardous (Iddrisu, Aziato and Dedey, 2020; Afolashade et al., 2023). This is a primary cause of the symptoms that some cancer patients experience when the disease is far advanced. Sometimes, a patient goes to a hospital for treatment, but because of their beliefs regarding their illness, they don't follow their treatment plans.
The assignment of blame is a long-standing human construct. According to Hochlaf, Quilter-Pinner, and Kibasi (2019), the disposition of blame in a given situation significantly impacts the subsequent reaction of the parties involved, as demonstrated by their actions. Certain patients might attribute their cancer to their surroundings, influential people in their lives, or themselves and the activities they had previously engaged in. Anxiety, depression, and distress are possible reactions for cancer patients to this. In addition, it might result in isolation, and patients might start blaming objects and people in their efforts to find the illness's source. This typically obstructs the patient's ability to manage their condition appropriately and delays treatment (Asuzu and Akin- Odanye, 2015; Fagbule et al., 2021). Several cancer patients may see traditional doctors both before and after visiting orthodox medical facilities, particularly when accepting undesirable treatment options and a troubling cancer diagnosis, as a result of blame attribution. Until things get terrible, some people don't mind visiting the hospital (Asuzu et al., 2015). Some patients focused on mystical, natural, and otherworldly causes. These always influence the selection of particular healthcare services and frequently impact people's attitudes and beliefs about specific healthcare outcomes (Adewuyi, 2021).
Placing blame could have a detrimental effect on a cancer patient's thoughts, feelings, behavior, and the way they adhere to their treatment plan. Patients may become more susceptible to other serious illnesses as a result, and the course of treatment and appropriate disease management may even be hampered. Gómez-de-Regil (2014) asserts that a growing body of research has highlighted the ways in which people's beliefs about wellness and disease can affect their behavior. Examining how patients view their condition is a crucial part of clinical practice since it influences how likely a patient is to seek and adhere to medical intervention. As a result, how people attribute blame affects how they handle physical symptoms and illnesses (Zhang et al., 2018). Even with earlier studies on the subject, blame attribution remains a prevalent issue for patients who have just received a cancer diagnosis. Thus, this study aimed to examine how Cognitive Reframing (CR) and Logotherapy (LT) affect how newly diagnosed cancer patients assign blame.
One of the most well-known existential therapies is logotherapy, which was created in the 1940s by Austrian Holocaust survivor and neurologist Viktor Frankl. Greek for "meaning," "logo" is the word itself. This therapy is predicated on the idea that humans have an innate need to find purpose in life. Expanding upon Freudian theory of psychopathology, logotherapy has significant therapeutic consequences. Considering these implications, Frankl believes that disorders are frequently caused by a problem of conscience manifesting as an ethical conflict or existential crisis, in addition to physical or psychological illnesses. According to Hoffman et al. (2013), such neuroses are categorized as "noogenic" and are situated next to somatogenic and psychogenic neuroses.
It has been noted that blame-attribution patients have trouble explaining their illness, leading them to believe that other people, circumstances, and the environment are the root of their cancer (Mohabbat-Bahar et al., 2014). LT may redirect their perspective if they can better understand the meaning and purpose of life and events. By giving patients' lives greater purpose and meaning, LT treatment can lessen their tendency to assign blame. This makes people feel happier and less lost in life rather than hopeless or unsatisfied. Based on empirical research, LT has been shown to improve people's quality of life, refuting the blame attribution perspective. Patients have reported being able to respond to their suffering more meaningfully, realize their full potential, and deal with challenges more skillfully (Rahgozar and Giménez-Llort, 2020).
In addition to being a valuable tool for treating somatogenic and psychogenic diseases, logotherapy is the specific treatment of noogenic neuroses. It symbolizes the attempt at psychological treatment from a "spiritual" perspective. It highlights the strength of individual autonomy and each person's accountability for their own life. According to Frankl (2006), finding meaning in life is crucial, and the best ways to see it are through other people's experiences, good deeds or labor, or the mindset one chooses to have during difficult times. According to Jafari- Ko.ula.e.e et al. (2018), LT has been shown to be a successful treatment that supports patients in finding purpose in life, coping with health issues, and becoming more involved in leading fulfilling lives in all health situations.
Another therapeutic package the researchers employ is cognitive reframing, or CR, because of its success in helping psychologists solve issues. A fundamental part of cognitive-behavioral therapy, cognitive reframing describes any shifts in an individual's mental perspective, including a general change in mentality (Beck, 1997). Cognitive restructuring (CR) involves recognizing and challenging illogical or maladaptive beliefs and visualizing and analyzing living situations, ideologies, feelings, and concepts to find more viable solutions. Negative thoughts have the potential to produce illogical beliefs like assigning blame. Therefore, CR could alter their perspective and generate more optimistic ideas to lessen or eradicate irrational beliefs. Turning negative thoughts into positive ones is the ultimate aim of cognitive restructuring. Empirical research has demonstrated the effectiveness of cognitive reframing, a method of therapy that employs various techniques to assist the client in realizing the irrationality of their thought patterns. Consequently, the client would act more appropriately in future situations by learning to devise irrational alternatives to such irrational thought patterns (Sylvester et al., 2023; Nathan and Gorman, 2002).
Cognitive reframing is primarily associated with cognitive behavioral therapies, which aim to lessen psychological distress by changing people's thoughts and how they understand and process events or circumstances (Beck et al., 1979). By assisting the client in changing the verbal or social context, cognitive reframing serves as an intervention tool to expand behavior by lowering the degree to which these cognitions control behavior. Additionally, CR assists clients in viewing their thoughts as theories to be verified by logic and empirical data rather than as indisputable facts. This helps to establish a boundary between the thinker and the ideas they contain and encourages the client to engage with the experiences they are having right now. Changing people's interpretations and assessments of the emotionally significant situations can be utilized to step in early in the emotion-generating process (Wolgast, Lundh, and Viborg, 2013; Omoponle & Veronica, 2023).
In this case, it is reasonable to assume that assigning blame results from pessimistic thinking. From Beck's point of view, the notion that cancer is connected to witchcraft or evil arrows is illogical (2005). Therefore, through constructive confrontation and self-talk, exposure to CR will lessen irrational thoughts associated with assigning blame for cancer to objects or people. To help the clients feel better about life and their current circumstances, the therapist in this scenario will actively engage the clients by teaching them how to replace negative thoughts with positive ones. Cancer patients can begin viewing their illness as a temporary state of life through CR (Kendra, 2016).
Research Hypotheses
This study's main goal was to determine how LT and CR affected newly diagnosed cancer patients' perceptions of blame. At significance levels of 0.05, the following research hypotheses were specifically tested:
H01: There is no significant main effect of Logotherapy (LT) and Cognitive Reframing (CR) in the management of blame attribution among newly diagnosed cancer patients;
H02: There is no significant difference in the effectiveness of Logotherapy (LT) and Cognitive Reframing (CR) in the management of blame attribution among newly diagnosed cancer patients.
Methodology
Design
The study adopted a pretest-posttest, control group, quasi-experimental design.
Population
All newly diagnosed cancer patients receiving treatment in cancer centers throughout Southwest Nigeria made up the study's population. This population is justified by the fact that cancer patients in this category are more likely to be experiencing psychosocial problems related to their recent cancer diagnosis, particularly concerning assigning blame. The six states of Lagos, Oyo, Ondo, Ekiti, Osun, and Ogun make up the southwest region of Nigeria.
Sample size and sample

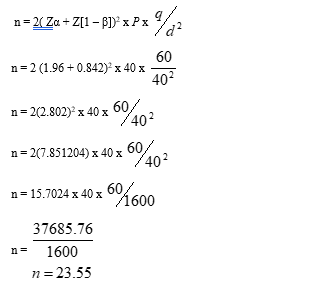
Which is approximately 24 per group
Bearing in mind the likelihood of attrition among this study population based on the nature of their illness, the following formula was employed to make up for attrition:
N1=n/(1-d)
So:
N1=additional sample size
n=calculated minimum sample size
d= drop out rate set at 10%
Then:
24/(1-10%)=24/0.9=26.66 which is 27 per study group
However, only 63 participants were initially enrolled in the study due to its sensitivity, and only 54 finished the program. Inferentially, the attrition rate was 14.2%, meaning that nine (9) individuals dropped out of the program.
The individuals who participated in the present research were chosen through a multistage sampling technique:
Stage I: Of the six states in southwest Nigeria that have cancer treatment facilities, three states—Oyo, Lagos, and Ogun—were chosen at random.
Stage II: Only hospitals in the three states offering comprehensive cancer care were chosen using the purposeful sampling technique. The hospitals in these states were specifically selected because they serve as major tertiary referral centers for other hospitals that handle most cancer cases in southwestern Nigeria and are comprehensive cancer treatment providers. These hospitals are, in order of designation, Lagos University Teaching Hospital (LUTH), Federal Medical Center, Abeokuta (FMC), and University College Hospital, Ibadan (UCH).
Stage III: Among the other patients in the study, newly diagnosed cancer patients were also chosen using the purposeful sampling technique. Sixty-three (63) recently diagnosed cancer patients from three different hospitals—University College Hospital, Ibadan (22), Lagos University Teaching Hospital, Lagos (18), and Federal Medical Center, Abeokuta (23), respectively—were deemed to have high rates of blame attribution when their scores on the Blame Attribution Questionnaire exceeded the 45-point cutoff. The patients in this category made up the study's participants. Nevertheless, only recently diagnosed cancer patients who satisfied the inclusion criteria were considered qualified to participate in the study in any of the chosen hospitals. A ballot system was used to randomly assign patients to groups: 18 in the LT group, 21 in the CR group, and 15 in the control group. These patients underwent treatment and training. This quasi-experimental design of the study aims to evaluate the efficacy of LT and CR among recently detected cancer sufferers, which is why two intervention groups were chosen. There were 54 participants in total—6 men and 48 women—who successfully finished the treatment modules.
Inclusion Criteria
The study's participants were chosen based on the following criteria:
- Patients with just-discovered cancer who registered at treatment facilities rather than upon admission
- Patients who were at least 18 years old, both male and female
- Individuals who completed the screening tool with a score higher than 45;
- Cancer patients who expressed interest in taking part in the treatment regimen
Instrumentation `
Standardized instruments were used to collect data for the study. The tools had been translated to Yoruba by a language expert and consultant to ensure consistency with the original intent and to enable efficient communication between investigators and some individuals who might not understand the English language:
Blame Attribution Questionnaire
The participants' rate of assigning blame after receiving a cancer diagnosis was evaluated using the scale as a screening tool. The Gudjonnson Blame Attribution Inventory-Revised (GBAI-R), designed by Gudjonnson and Singh (1989), served as the model for the scale. The scale measured the three subscales of blame attribution—mental element attribution, external attribution, and guilt feeling attribution. To better serve the study's goals, it was changed to 20 items. After undergoing pilot testing, the scale's Cronbach alpha coefficient of. Eighty-one indicated that it was deemed reliable for use in the study.
Modified Attributions for Serious Illness Scale
Mantler, Schellenberg, and Page's original Attributions for Serious Illness Scale served as the model for the scale's adaptation (2003). The dependent variable (blame attribution) was measured using the scale in the study's post-test phases. To better fit the study's objectives, the items were reduced to 25. The controllability, responsibility, and blame subscales on the scale assessed attribution. It was used to gauge the degree to which patients placed the blame for their health condition on themselves, their surroundings, the government, their genetics, or supernatural forces. To verify the validity and reliability of the instrument, pilot testing was conducted in comparable oncology settings outside of the study group. There was a reported overall Cronbach alpha coefficient of.85.
Procedure for Data Collection
This study was carried out in compliance with accepted ethical standards. Each study site's institutional review board and ethics committee reviewed the study protocol and proposal. The researcher followed the recommendations. ADM/DCST/HREC/APP/2637 is the assigned number for the LUTH Health Research Committee, and the UI/UCH Ethics Committee is assigned the UI/EC/18/0534. The Health Research Ethics Committee at the Federal Medical Centre Abeokuta gave the study its protocol lots FMCA/243/HREC/03/2018/19.
Because of the sensitive nature of the study and concerns about confidentiality, the participants' informed consent was requested. For efficient communication, this was translated back into Yoruba. Before starting the study, the researcher visited the chosen centers to familiarize herself with the patients and the hospital setting. The study was carried out in four phases: pre-sessional activities, pretest, treatment, and posttest. During the pre-session, the centers were randomly assigned to two experimental and control groups, participants were screened using the Blame Attribution Questionnaire, and participants were made aware of the value and advantages of the training and therapies. Additionally, during the familiarization, the researcher and participants decided on a convenient time and location for the activity. The first experimental group's participants consented to meet at the Alaanu House UCH with permission from the supervising hospital staff, and the researcher and the participants were allowed to meet for the duration of the study in a portion of the reception areas of the oncology units at LUTH and FMC, respectively.
Data Analysis
The primary statistical methods used in the investigation were ANCOVA and simple percentages. The demographics of those who participated were analyzed using simple percentages, and the initial variations between the experimental and control groups were established using ANCOVA. The study employed Scheffe's post-hoc analysis to ascertain the differences and current significance patterns.
Results
Results
| Age | Frequency | Percentage |
21-30 years 31-40 years 41-50 years 51-60 years 61-70 years 70 years and above | 1 3 17 25 7 1 | 1.9% 5.5% 31.5% 46.3% 12.9% 1.9% |
| Gender | Frequency | Percentage % |
Male Female | 6 48 | 11.1% 88.9% |
| Educational Qualification | Frequency | Percentage % |
None Primary Secondary Tertiary | 5 12 17 20 | 9.3% 22.2% 31.5% 37% |
| Cancer Type | Frequency | Percentage % |
Breast Cervical Prostate Skin | 29 18 5 2 | 53.7% 33.3% 9.3% 3.7% |
| Stage of Cancer | Frequency | Percentage |
| Stage One | 10 | 18.5 |
| Stage Two | 28 | 51.9 |
| Stage Three | 4 | 7.4 |
| Unknown | 12 | 22.2 |
Table 1: Participants' Demographics
The average age of the participants was 53.85±7.89 years, according to Table 1. This suggests that most individuals were in the 51–60 age range. The study's participant demographic was primarily female (88.9%) instead of male (11.1%), suggesting that more women than men participated in the research. In addition, 9.3% of participants had never attended any formal education, followed by 22.2% with only an elementary education, 31.5% with a secondary education, and 37% with a postsecondary education (OND, NCE, HND, BSc, and its equivalents). In addition, among the participants,
53.7% had breast cancer, while a noteworthy proportion (33.3%) had cervical cancer, 9.3% had prostate cancer, and 3.7% had skin cancer. In addition, the majority of participants (51.9%) had the disease in stage 2, 18.5% had stage 1, 7.4% had stage 3, and 22.2% had no idea what stage their cancer was.
Hypothesis One: There is no significant main effect of Logotherapy (LT) and Cognitive Reframing (CR) in the management of blame attribution among newly diagnosed cancer patients. Dependent Variable: Postest
| Source | Type III Sum of Squares | Df | Mean Square | F | Sig. | Partial Eta Squared |
| Corrected Model | 20171.803a | 11 | 1833.800 | 9.183 | .000 | .706 |
| Intercept | 3531.613 | 1 | 3531.613 | 17.684 | .000 | .296 |
| Pretest | 592.317 | 1 | 592.317 | 2.966 | .092 | .066 |
| Treatment | 6401.614 | 2 | 3200.807 | 16.028 | .000* | .433 |
| Errors | 8387.530 | 42 | 199.703 | |||
| Total. | 200602.000 | 54 | ||||
| Corected Total | 28559.333 | 53 | ||||
Table 2: An overview of the Analysis of Covariance (ANCOVA) demonstrating how treatment groups primarily influence blame attribution in patients with recently diagnosed cancer a. R Squared = .706 (Adjusted R Squared = .629)
*Denotes significant difference at 0.05 level of significance
Within newly diagnosed cancer patients, Table 2 above demonstrates a significant main effect of treatment in managing blame attribution (F2;42 = 16.03; P < 0>
Hypothesis Two
There is no significant difference in the effectiveness of Logotherapy (LT) and Cognitive Reframing (CR) in the management of blame attribution among newly diagnosed cancer patients.
Variable + Category
| N | Unadjusted Mean | Adjusted Mean | Unadjusted Deviation | Eta | Adjusted Deviation | Beta |
Treatment: CR LT Control
|
21 18 15
|
42.905 63.556 66.867 |
44.550 63.356 64.803
|
-13.539 7.111 10.422
|
.473
|
-11.894 6.911 8.359
|
413 |
Multiple R Squared Multiple R | .612 .782 | ||||||
Table 3: The pattern of differences in managing blame attribution among newly diagnosed cancer patients between the treatment and control groups is demonstrated by Multiple Classification Analysis (MCA).
Grand Mean = 56.4444
To obtain additional information regarding the participants' management of blame attribution across the three groups (logotherapy, cognitive reframing, and control), as well as the direction and magnitude of the differences in mean scores between each treatment group and the control group, a Multiple Classification analysis was conducted. The results are displayed in Table 3, indicating that the CR therapy was the most successful in managing blame attribution among participants recently diagnosed with cancer, compared to the LT and control groups, respectively.
There was a statistically significant difference in the mean scores of the post-hoc test for managing blame attribution between the CR and LT groups of newly diagnosed cancer patients. More people benefited from the CR (

=42.91) than from the LT (

=63.56). The post-hoc test mean scores for controlling blame attribution differed significantly between recently diagnosed cancer patients' control and CR groups. Compared to those in the control group (

=66.87), participants in the CR (

=42.91) demonstrated a significantly higher ability to manage blame attribution.
Additionally, among recently diagnosed cancer patients exposed to LT, there was a significant difference in the mean scores of the post-hoc tests for managing blame attribution compared to the control group. Compared to the control group (

=66.87), the LT participants (

=63.56) demonstrated a significantly higher ability to manage blame attribution. This suggests that in terms of controlling blame attribution for newly diagnosed cancer patients, the CR group received the lowest adjusted post-test mean score (

= 42.91). LT (

= 63.56) came in second, and the Control group (

= 66.87) scored the highest. This suggests that CR therapy, as opposed to LT and control groups, was more successful in helping participants manage the attribution of blame for newly diagnosed cancer patients.
Also,between newly diagnosed cancer patients exposed to LT and control groups, there was a significant difference in the post-hoc test mean scores for managing blame attribution. Compared to those in the control group (Mean=66.87), participants in the LT (Mean=63.56) demonstrated a significantly higher ability to manage blame attribution. This suggests that when controlling blame attribution of newly diagnosed cancer patients, the CR group received the lowest adjusted posttest mean score (x ̅ = 42.91). LT came in second (x ̅ = 63.56), and the Control group scored highest (x ̅ = 66.87). This suggests that compared to the LT and control groups, CR therapy was more successful in helping participants manage the attribution of blame for newly diagnosed cancer patients.
Discussion of Findings
This study looked into how newly diagnosed cancer patients were assigned blame and how logotherapy (LT) and cognitive reframing (CR) affected that process. Based on gender, the participants' demographic characteristics show that 88.9% of the participants were female and 11.1% were male. This suggests that a higher proportion of women than men took part in the research. 53.85±7.89 years was the average age of the participants. This makes it abundantly evident that most participants were aged 51 to 60. This is consistent with research from both domestic and foreign sources that shows age to be a risk factor for cancer diagnosis. Based on their educational backgrounds, participants were distributed as follows: the largest group (37%) had a postsecondary education, followed by those with a secondary education (31.5%). 53.7% of participants had breast cancer, according to the distribution of cancer types among participants. This suggests that among the participants, breast cancer was the most common type of cancer. Additionally, the majority of participants (51.9%) had the disease at stage 2.
Furthermore, among newly diagnosed cancer patients who took part in the program, the results showed that logotherapy and cognitive reframing were helpful in managing blame attribution. Determining the level of significance across the three groups—control, cognitive reframing, and logotherapy—is crucial in an effort to provide more details on the participants' management of blame attribution. When the post hoc Analysis was used, it became clear that the participants in the three groups' management of blame attribution significantly differed from one another in terms of the post-hoc test mean scores. Compared to the LT and control groups, the CR therapy was more successful in helping the participants manage their assigning of blame. This suggests that participants in the LT group outperformed those in the control group, and those in the CR therapy group gained more from the training than those in the LT group. This suggests that CR outperforms LT in reducing blame attribution. The effectiveness of the various interventions and their corresponding delivery strategies can be used to explain these discrepancies. This outcome may be explained by the fact that cognitive-reframing therapy (CR) focuses on how participants attribute blame to their thoughts, beliefs, and attitudes, which in turn influence their emotions and actions. The participants in CR were able to gain skills that would enable them to manage their health condition effectively and reject illogical ideas about what caused their illness.
The results of this investigation are consistent with those of Lepore and Helgeson (2012), who found that cognitive reframing was a fundamental strategy that assisted men with prostate cancer in turning horrific events into believable circumstances and encouraging faulty aspects of their experience into a fair mental state while they were being harassed. The findings of (Pandey and Vajpeyi, 2020; Kanmodi et al., 2020) are consistent with this finding. They reported that after participating in a 10-week cognitive therapy psychological intervention, newly diagnosed cancer patients' coping mechanisms, quality of life, and life orientation significantly improved. There was also a decrease in the intensity of negative feelings. Similarly, Ofole and Omole (2017) found that cognitive reframing-exposed participants with developed helplessness had an increased posttest mean rating than the control and self-acceptance therapy groups. Furthermore, cognitive reframing increased participants' optimism more effectively than self-acceptance therapy (Adewuyi, 2021).
Moses (2021) reported that cognitive reframing therapy significantly reduces social disconnectedness among widows. The study's widows exhibited less socially disconnected behavior as a result of this technique. Similarly, after exposing teenagers to cognitive reframing, Rosenberg, Jankowski, Fortuna, and Rosenberg (2011) found statistically significant improvements in depression and PTSD. The benefits of cognitive reframing in lowering the degree of depression in female cancer patients through intervention were also documented by Asuzu et al. (2015). Compared to their baseline scores prior to the intervention, the individuals who received cognitive reframing training reported lower levels of depression. In a similar vein, Sulaiman and Uhuegbu (2021) endorsed cognitive reframing as an effective tactic for lowering truancy among secondary school pupils.
This finding strengthens the case that cognitive-based therapies have clinical evidence to treat a variety of psychological issues, as demonstrated by the results of the following earlier research. Several studies have been conducted on this topic: Tang, Chen, and Cheng (2013); Mardanivalendani and Ghafari (2015); Bhaskaran (2014); Ezegbe et al. (2018); Hajibabaei et al. ( 2020). Since the mediation process produced comparable results, the findings' consistency is crucial. The participants were assisted in altering their cognitive biases through the use of the cognitive reframing technique. Additionally, cognitive reframing helped them see life more clearly, deal with difficult circumstances more effectively, and find fulfillment in life. Furthermore, Linley and Joseph (2004) reasoned that between 30 and 70 percent of people who overcome various dreadful conditions typically exhibit cognitive change. Additionally, Pandey and Vajpeyi (2020) demonstrated differences in the quality of life, life orientation, and coping mechanisms of recently diagnosed cancer patients before and after testing. They also established a decrease in the intensity of negative emotions following a 10-week cognitive therapy-based psychological intervention.
Furthermore, this discovery supports the research conducted by Jafari-Koulaee et al. (2018), which found that logotherapy significantly lowers depression levels in cancer patients. The results of Southwick, Lowthert, and Graber's (2016) study also demonstrated the value and effectiveness of logotherapy in boosting stress and trauma resilience and its capacity to help individuals confronted with adversities. Similarly, Shahabi (2016) confirmed that group logotherapy was highly influential in enhancing the positive outlook on life and the emotional regulation of cancer patients. Furthermore, Ramesh et al. (2014) found that logotherapy is extremely beneficial because it effectively reduces the distress that comes with colorectal cancer and increases hope in those who are affected. This is consistent with a study by Ebrahimi, Bahari, and Zare-Bahramabadi (2014), which found that logotherapy could give leukemia patients more hope. As a result, a connection between logotherapy and blame attribution is made, and the effectiveness of logotherapy is reinforced as it can effectively handle accusations and blame attribution while positively impacting patients' overall feelings of worthlessness and distress.
Similarly, Nader, Ghanbari, Tajabadipour, Gholipour, and Esmaeilzadeh's (2019) research findings corroborated the effectiveness of group logotherapy in improving the resilience and life expectancy of breast cancer patients. It can assist these patients in finding purpose in their lives, getting support from others, learning to live with their illnesses, and changing their perspective on challenges and issues. The study by Sun et al. (2019), which found that logotherapy was beneficial in lowering patients' feelings of depression and demoralization related to breast cancer and gynecological cancer, is consistent with this conclusion. This demonstrates how participants in logotherapy treatment cohorts were pulled from a negative life trajectory and placed in a positive one following the treatment period.
Conclusion
The effectiveness of cognitive reframing (CR) and logotherapy (LT) in managing blame attribution in newly diagnosed cancer patients was investigated in this study. The therapeutic packages were used to train the participants, and data was gathered and examined. The study discovered that among newly diagnosed cancer patients, managing blame attribution was significantly impacted by treatment. This suggests that both LT and CR were successful in addressing the attribution of blame among cancer patients. The findings demonstrated that CR therapy outperformed LT in controlling participants' assigning of blame. According to the study's findings.
The study concludes that in order for patients to effectively manage their cancer and lead well-adjusted lives, it is critical that they complete their treatment plan after receiving a cancer diagnosis. This might not be possible if the patients in question flee or refuse to seek medical attention after receiving such a diagnosis. As a result, the two treatments employed in the study have proven to be robust and successful in reducing the tendency for recently diagnosed cancer patients to assign blame, highlighting the importance of completely integrating psychosocial support into oncology settings.
Recommendations
The following suggestions are underlined for your consideration in light of the study's findings:
- More education, awareness, and sensitization about the value of cancer screening and testing are required. In order to help patients make an informed choice and prevent incorrect attribution, this will increase awareness of the advantages of cancer testing.
- LT and CR can be helpful interventions for managing blame attribution in cancer patients. They can be employed by counselors, clinical psychologists, and other related professionals.
- Many cancer patients have placed blame on other factors as the reason behind their illness. Emotional difficulties have increased as a result, and health is declining. Therefore, participants should lessen the emotional issues that arise from assigning blame.
References
- Adewuyi, H. O. (2021). Mode deactivation, coherence therapies and self-acceptance among in-school adolescents with negative body image in Osun State, Nigeria (Doctoral dissertation).
View at Publisher | View at Google Scholar - Afolashade, I. Jimoh, A. Raji, N, Fowowe-Ogunmilugba, B. Oduola. O, & Ade, H. (2023). Emotional Intelligence, Job Satisfaction, Reward System and Organizational Commitment among Workers. ASEAN Journal of Economic and Economic Education, 3(1).
View at Publisher | View at Google Scholar - Asuzu, C. C. and Akin-Odanye, E. O. (2015). The Delivery of Psychosocial Services in an Oncology Setting: The Ibadan Experience. Journal of Clinical Trials 5:228.
View at Publisher | View at Google Scholar - Asuzu, C.C. and Asuzu, M.C. (2007). Knowledge, Attitude, and Practice of Self Breast Examination among the Female Students of the University of Ibadan, Nigeria. Pakistan Journal of Social Science, 4(3):400-402.
View at Publisher | View at Google Scholar - Asuzu, C.C, Akin-Odanye, E.O and Philip, E.J. (2015). The Effect of Pilot Cognitive Restructuring Therapy Intervention on Depression in Female Cancer Patients. Journal of Psycho-Oncology, wileyonlinelibrary.com
View at Publisher | View at Google Scholar - Asuzu, C.C, Elumelu-Kupoluyi, T., Asuzu, M.C, et al. (2017). A Pilot Study of Cancer Patients' Use of Traditional Healers in the Radiotherapy Department, University College Hospital, Ibadan, Nigeria. Journal of Psycho-Oncology 26:369-376.
View at Publisher | View at Google Scholar - Ayanwale, M.A, Habee, O.A & Olakunle, W. A. (2023). Learning through radio and television during COVID-19: perspectives of K-12 stakeholders. EUREKA: Social and Humanities 2: 61-72.
View at Publisher | View at Google Scholar - Banerjee D, Gidwani C. and Sathyanarayana Rao, T S. (2020). The role of
View at Publisher | View at Google Scholar - Beck, A. T, Rush, A. J, Shaw. B. F, and Emery, G. (1979). Cognitive Therapy of Depression. New York: Guilford Press.
View at Publisher | View at Google Scholar - Beck, A.T. (1997). The Past and the Future of Cognitive Therapy. Journal of Psychotherapy, Practice and Research, 6:276-284.
View at Publisher | View at Google Scholar - Beckham, J.C, Rice, J.R, Talton, S.L, Helms. M.J. and Young, L.D. (1994). Relationship of Cognitive Constructs to Adjustment in Rheumatoid Arthritis Patients. Cognitive Therapy and Research, 18:479-496.
View at Publisher | View at Google Scholar - Bhaskaran, K. (2014). Body Mass Index and Risk of 22 Specific Cancers. Lancet 384 (9945):755-765.
View at Publisher | View at Google Scholar - Ebrahimi, N, Bahari, F. and Zare-Bahramabadi, M. (2014). The Effectiveness of Group Logotherapy on the Hope among the Leukemic Patients. Iranian Journal of Cancer Prevention 7(1): 9-16.
View at Publisher | View at Google Scholar - Ezegbe, B.N, Ede, M. Eseadi, C, Nwaubani, O.O, et al. (2018). Effect of Music Therapy Combined with Cognitive Restructuring Therapy on Emotional Distress in a Sample of Nigerian Married Couples. Journal of Medicine, 97:(34).
View at Publisher | View at Google Scholar - Fagbule, O. F, Kanmodi, K. K, Samuel, V. O, Isola, T. O, Aliemeke, E. O, Ogbeide, M. E, & Ibiyemi, O. (2021). Prevalence And Predictors Of Cigarette Smoking And Alcohol Use Among Secondary School Students In Nigeria. Annals of Ibadan Postgraduate Medicine, 19(2):112.
View at Publisher | View at Google Scholar - Frankl, V. (2006). Man's Search for Meaning. An Introduction to Logotherapy. Boston, MA: Beacon Press.
View at Publisher | View at Google Scholar - Gómez-de-Regil, L. (2014). Causal Attribution and Illness Perception: A Cross-Sectional Study in Mexican Patients with Psychosis; The Scientific World Journal, 969867.
View at Publisher | View at Google Scholar - Gudjonsson, G.H. and Singh, K.K. (1989). The Revised Gudjonsson Blame Attribution Inventory, Journal of Personality and Individual Differences 10(1):67-70.
View at Publisher | View at Google Scholar - Hajibabaei, M. Kajbaf, M.B. Esmaeili, M, Harirchian, M.H. and Montazeri, A. (2020). Impact of an Existential-Spiritual Intervention Compared with a Cognitive-Behavioural Therapy on Quality of Life and Meaning in Life among Women with Multiple Sclerosis. Iranian Journal of Psychiatry, 15(4):322-330.
View at Publisher | View at Google Scholar - Hochlaf, D, Quilter-Pinner, H. and Kibasi, T. (2019). Ending the Blame Game. The Case for a New Approach to Public Health and Prevention. Institute for Public Policy Research.
View at Publisher | View at Google Scholar - Hoffman, A. J, Brintnall, B. A, Brown, J. K, Ige, A, Jones, L. W, et al. (2013). Too Sick not to Exercise: Using a 6 Week, Home-Based Exercise Intervention for Cancer-related Fatigue, Self-management for Post-surgical Small Cell Lung Cancer Patients. Journal of Cancer Nursing 36(3):175-188.
View at Publisher | View at Google Scholar - Hosseinigolafshani, S.Z. Taheri, S, Mafi. M, Mafi. M.H, Kasirlou, L. (2020). The Effect of Group Logotherapy on the Burden of Hemodialysis Patients' Caregivers. Journal of Renal Injury Prevention 9(4):33.
View at Publisher | View at Google Scholar - Iddrisu, M, Aziato, L. and Dedey, F. (2020). Psychological and Physical Effects of Breast Cancer Diagnosis and Treatment on Young Ghanaian Women: A Qualitative Study. Journal of Psychiatry 20:353.
View at Publisher | View at Google Scholar - Jafari- Koulaee, A, Khenarinezhad, F., Abutalebi, M. and Bagheri-Nesami, M. (2018). The Effect of Logotherapy on Depression in Cancer Patients: A Systematic Review Study. World Cancer Research Journal 5(3):23-29.
View at Publisher | View at Google Scholar - Kang, K. Shim, J. Jeon, D, and Koh, M. (2019). The Effects of Logotherapy on Meaning in Life and Quality of Life of Late Adolescents with Terminal Cancer. Journal of Korean Academy in Nursing 39(6):759-768.
View at Publisher | View at Google Scholar - Kantor, D. (2016). Psychological Distress. In Kantor, D. and Suzan, Z, Issues of Cancer Survivorship: An Interdisciplinary Team Approach to Care. Philadelphia, PA: Wolters Kluwer: 47-63.
View at Publisher | View at Google Scholar - Kendra, C. (2016). Attribution and Social Psychology. verywellmind.com. Retrieved 10th March, 2018.
View at Publisher | View at Google Scholar - Lepore, S. J. and Helgeson, V. S. (2012). Social Constraints, Intrusive Thoughts and Mental Health after Prostate Cancer. Journal of Social and Clinical Psychology 17(1):89-106
View at Publisher | View at Google Scholar - Linley, P.A. and Joseph, S. (2004). Positive Change Processes Following Trauma and Adversity: A Review. Journal of Traumatic Stress, 17:11-22.
View at Publisher | View at Google Scholar - Mantler, J, Schellenberg, E.G, and Page, J.S. (2003). Attributions for Serious Illness: Are Controllability, Responsibility, and Blame Different Constructs? Cancer Journal in Behavioural Science, 35(2):142-152.
View at Publisher | View at Google Scholar - Mardanivalendani, M. and Ghafari, Z. (2015). The Effectiveness of Logotherapy on Quality of Life among Multiple Sclerosis Patients in Shahrekord. Journal of Ilam University of Medical Sciences, 23(5):47-56.
View at Publisher | View at Google Scholar - Mohabbat-Bahar, S. Golzari, M. Moradi-Joo, M. and Akbari, M.E. (2014). Efficacy of Group Logotherapy on Decreasing Anxiety in Women with Breast Cancer. Iranian Journal of Cancer Prevention 7(3):165-170.
View at Publisher | View at Google Scholar - Moses, V. (2021). A Non-randomized Study Investigating the Effectiveness of Cognitive Reframing in Socially Disconnected Widows. European Research Journal 7(1):1-11.
View at Publisher | View at Google Scholar - Nader, M. Ghanbari, N, Tajabadi-pour, S. Gholipour, S. Esmaeilzadeh, N. (2019). Effectiveness of Short-term Group Logo-therapy on Life Expectancy and Resilience of Women With Breast Cancer. Archives of Breast Cancer, 6(4):168-173.
View at Publisher | View at Google Scholar - Nathan, P. E. and Gorman, J. M. (2002). A Guide to Treatments that Work (2nd ed.). New York, NY, US: Oxford University Press.
View at Publisher | View at Google Scholar - Ofole, M. and Omole, O. (2017). Remedial Effect of Cognitive Reframing and Self-Acceptance Therapy on Enhancement of Optimism among Students Diagnosed with Learned Helplessness in Ibadan Metropolis. ResearchGate
View at Publisher | View at Google Scholar - Omoponle, A. H, & Veronica, D. (2023). Risky sexual behavior and associated factors among in-school adolescents: a school-based, cross-sectional study. EUREKA: Social and Humanities.
View at Publisher | View at Google Scholar - Pandey, S. and Vajpeyi, L. (2020). Clinical Interview: Improving Quality of Life in Cancer Patients. UGC Care Journal 31(4):681-701.
View at Publisher | View at Google Scholar - Rahgozar, S. and Giménez-Llort, L. (2020). Foundations and Applications of Logotherapy to Improve Mental Health of Immigrant Populations in the Third Millennium. Frontiers in Psychiatry 11:451.
View at Publisher | View at Google Scholar - Ramesh, H.K, Mehrak, R, Mohammad-Ebrahim, S, Kamran, B.L, Hassan J. et al. (2014). Evaluating the Effect of Logotherapy Group on Mental Health and Hope to Life of Patients with Colorectal Cancer receiving Chemotherapy. Bulletin of Environment, Pharmacology and Life Sciences, 3(5):164-169.
View at Publisher | View at Google Scholar - Rosenberg, H, Jankowski, M.K, Fortuna, L.R, Rosenberg, S.D. and Mueser, K. (2011). A Pilot Study of a Cognitive Restructuring Program for Treating Posttraumatic Disorders in Adolescents. Psychological Trauma: Theory, Research, Practice and Policy 3(1):94-99.
View at Publisher | View at Google Scholar - Shahabi, S. 2016. The Effect of Logotherapy on Life Orientation of Cancer Patients. International Journal of Medical Research and Health Sciences 5(9):240-243.
View at Publisher | View at Google Scholar - Southwick, S.M, Lowthert, B.T, and Graber, A.V. (2016). Relevance and Application of Logotherapy to Enhance Resilience to Stress and Trauma. In book: Logotherapy and Existential Analysis, 131-149.
View at Publisher | View at Google Scholar - Sulaiman, A. and Uhuegbu, S. (2021). Impact of Cognitive Restructuring and Token Economy Techniques on Truancy Reduction among Secondary School Students in Lagos State, Nigeria. Islamic Guidance and Counseling Journal, 4(1):21-32.
View at Publisher | View at Google Scholar - Sun, F.K, Hung, C.M, Yao, Y, Fu, C.F, Tsai, P.J. et al. (2019). The Effects of Logotherapy on Distress, Depression, and Demoralization in Breast Cancer and Gynecological Cancer Patients: A Preliminary Study. Journal of Cancer and Nursing, 44(1):53-61.
View at Publisher | View at Google Scholar - Sylvester, E. U, Adewuyi H. O, Falaye A. O, Adegoke S. A and Raji N. A. (2023). Sexual promiscuity among students in tertiary institutions: Interrogating the roles of peer influence, parenting processes, social, economic status, and social media. World Journal of Advanced Research and Reviews, 20(02), 132-143.
View at Publisher | View at Google Scholar - Tang, P.L, Chen, W.L and Cheng, S.F. (2013). Using Logotherapy to Relieve Death Anxiety in a Patient with Recurrent Cancer: A Nursing Experience. Hu Li Za Zhi 60(4):105-110.
View at Publisher | View at Google Scholar - Wolgast, M, Lundh, L and Viborg, G. (2013). Cognitive Restructuring and Acceptance: An Empirically Grounded Conceptual Analysis. Journal of Cognitive Therapy and Research, 37:2.
View at Publisher | View at Google Scholar - Zhang, L, Schwarz, J, Kleinstäuber, M, Fritzsche, K, Hannig, W. et al. (2018). Confirmatory Factor Analysis of the Causal Illness Attribution Scale in Chinese Patients with Multiple Somatic Symptoms. Journal of Psychology, Health and Medicine 23(1):1318-1313.
View at Publisher | View at Google Scholar
