

Research Article | DOI: https://doi.org/10.31579/2834-5118/030
Lip Reduction Surgery (Cheiloplasty) For Lower Lip
*Corresponding Author: Noury Adel, Oral and Maxillofacial Surgery Specialist, Cairo, Egypt
Citation: Noury Adel. (2023). Lip Reduction Surgery (Cheiloplasty) for lower lip. International Journal of Clinical Surgery 2(4); DOI: 10.31579/2834-5118/030
Copyright: ┬® 2023, Noury Adel. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 August 2023 | Accepted: 17 August 2023 | Published: 26 August 2023
Keywords: lip reduction; hypertrophic lips; reduction cheiloplasty; lip surgeries; lips
Abstract
Aim: The present study was performed to evaluate the stability of the lip reduction surgery in reducing the over-sized ŌĆ£hypertrophic ŌĆ£lower lip.
Methods: Ten female patients were included in the study who was unpleased from their enlarged lower lip which was not proportionate to their upper lip, patients were selected according to a specific inclusion and exclusion criteria, pre-operative photographic pictures were taken for planning and records. Preoperative measurement included measuring the vermilion height of the lower lip. Reduction cheiloplasty was performed under local anaesthesia for all patients by removing a strap of epithelium through a curved ellipse outline followed by key sutures evenly distributed and primary closure of the wound by interrupted 0- 5 resorbable sutures. All patients were followed up at 3 weeks, 3 months and 6 months, postoperative measurements were done by measuring the vermilion height changes.
Results: Post-operative measurements at 3 weeks follow up, showed marked decrease in the vermilion height of the lower lip where the lip looked much more smaller. This remained stable up to 3 month, however at six month follow up a slight increase occurred at the vermilion height of the lower lip but never returned to baseline value.
Conclusion: Lip reduction surgery is an effective technique in addressing hypertrophic lip but its long term stability remains questionable where further studies is needed with long term follow up in addition to modifications to the original technique and evaluating the effect of the excision of a wedge shape tissue from the deeper sub mucosal layer.
Introduction
The lips are considered to be one of the most illustrious facial features and play a great role in facial expression thatŌĆÖs why recently a lot of people have grown attention to the size of their lips. A patient self-image of his or her lips, like other body parts, is relative. Some people may prefer large lips while other people even in the same culture may prefer smaller lips, the perception of beauty will always differ among people in same or different cultures [1]. An over- sized lip which is scientifically called ŌĆ£MacrocheiliaŌĆØ which is more encountered in black and Asian patients represents a great challenge in aesthetic surgery [2], however such a condition is caused by several etiologies either; racial, hereditary, dentofacial abnormalities (pseudomacro- cheilia), lymphatic disorder , haemangioma, orbicularis oris dysfunction and medical causes ( Melkersson-Rosenthal syndrome & Ascher syndrome) [3,4].
In the Caucasian patient the upper lip constitutes about 1/3 of the total lip volume on the other hand the lower lip constitutes about 2/3 of the total lip volume giving a ratio of about 1:1.6 [5,6]. Those dimensions are generally larger in African people, the vermillion height norms vary in different ethnicities as well [7,8]. Lip reduction surgery is performed either as an aesthetic surgery for beauty enhancement or for therapeutic goals such as in cases of difficulty in speaking , eating due to very large lips , or drooling as in the case of abnormal orbicularis oris muscle tone [9].
A recent study have been reported in the literature by Jittilaongwong based on his experience of 9000 cases treated with lip reduction surgery [10], furthermore he also evaluated the results of lip reduction surgery on another 7145 patients using the ŌĆ£Seagull wing incisionŌĆØ where the author reported a high satisfaction rate with the surgical outcome [11]. Some techniques aimed at addressing the size of the lips only or focused on the reconstructive side [12,13], where others aimed at achieving smaller lips but putting into consideration the relative proportion of the upper lip and lower lips in order to provide an aesthetic harmony of the labial unit, those of which have advocated some modifications to the outline of the incision such as the Bikini shaped incision [1,14]. Up to our knowledge, none of the previously mentioned studies have reported the long term stability of the results of the surgery neither the amount of the relapse that occurs except for some studies that aimed to address hypertrophic lips due to cheilitis granulomatousm [15,16], it is worth mentioning that there are not enough studies conducted on lip reduction surgery and from where comes the necessity of our study.
Materials and methods
Ten female patients ranging in age from 22 to 33 years who werenŌĆÖt pleased with the appearance of their lower lips due to its large size were included in the study. PatientŌĆÖs medical history was reviewed. Extra oral examination was performed to assess any facial asymmetry and to examine the lip architecture, followed by intraoral examination for the lower anterior teeth, associated periodontium and the mucosa. Digital photographic pictures were taken for recording and planning, in addition to lateral cephalometric to rule out any dentofacial deformities.
Inclusion criteria:-
-┬Ā Female patients.
-┬Ā Over-sized lips due to racial or hereditary causes.
Exclusion criteria:-
-┬Ā Patients with large interlabial distance at rest ( more than 3 mm ).
-┬Ā Dentofacial abnormalities and deformities.
-┬Ā Microgenia
-┬Ā Smokers
-┬Ā Patients with systemic diseases.
The vermillion height were measured by recording the vertical distance from the stomion inferior to┬Ā ┬Āthe┬Ā ┬Āmost┬Ā inferior┬Ā ┬Āpoint┬Ā ┬Āat┬Ā the ┬Ā vermilion┬Ā ┬Āborder┬Ā of┬Ā ┬Āthe┬Ā ┬Ālower┬Ā lip. After proper diagnosis and assessment, lip reduction surgery was explained to the patient with all the possible complications and outcomes; this was preceded by signing all the written forms and consents. The study was conducted ethically in accordance with the Declaration of Helsinki.
Surgical procedure
Patient preparation:-
Marking the lips to detect the amount of excess tissue to be removed is more art than science. First the lips were dried then wiped with alcohol to allow better ink marking, where it have been kept dry after marking by placement of a cotton pellet or a piece of gauze in-between the lips and the lower anterior teeth to avoid dilution of the markings by the saliva, loss of the markings may jeopardize the results, markings were placed before local anaesthesia injection with the patient in an up-right position.
Markings were placed at or posterior to the wet/dry border of the lips to avoid scar visibility and excessive removal of the vermillion zone; on the other hand we avoided placing the marking too far posteriorly because this would have a little effect in drawing the lip backward.
All patients was asked to relax their lips and first markings are made on the neutral place of meeting of the upper and lower lip then the patients were asked to pull their lips toward their teeth imitating the desired shape of her lips, second markings were made as well. All patients were given a mirror and repeated this manoeuvre to a point where they would optimally prefer the amount of vermillion show and posture. The first and second markings were connected to each other on either side of the commissure giving an overall curved ellipse outline which is larger in the centre and tapers toward the commissure where we avoided going into the corner of the mouth in order not to cause a deformity, the distance between the two lines were recorded as it would affect the amount of tissue to be excised (the amount of tissue excised was 2 to 2.5 times the measured distance). Finally the lip mid-line was also marked to aid in proper symmetry during wound closure.
Anaesthesia:-
Infiltration anaesthesia (long acting anaesthesia with epinephrine) in the labial vestibule was given to all the patients for the purpose of pain control followed by infiltration into the substance of the lower lip for purpose of hydro dissection and hemostasis.
Surgical steps:-
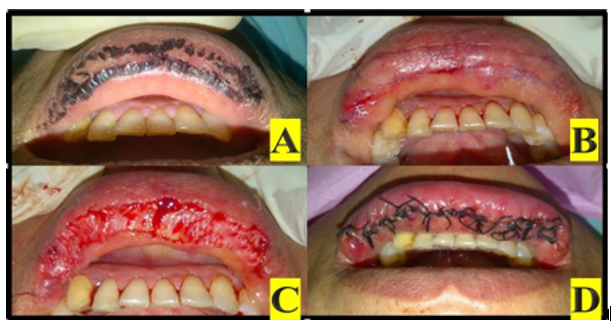
No.15 blade was used for incision through the previously marked lines, followed by sharp dissection for excision of the mucosa from the sub mucosal structures, extreme care was taken not to dissect deep to the sub mucosal layer in order not to disrupt the orbicularis oris muscle which would have a negative impact on its function. Series of key sutures were placed using Silk suture, first suture placed at the midline followed by placing another suture one-half the distance to the end of the incision until 5 to 6 sutures are placed. Finally additional interrupted sutures were used to close the remaining tissue (Figure 1, 2).
Post-operative instructions:-
All patients were instructed to apply ice immediately after the procedure and to use it for 2 to 3 days, sleep with their head elevated, following a soft regime for the first 72 hours, avoiding excessive smiling or stretching the lips, refrain from drinking with a straw. Postoperative medications includes; analgesics (Brufen 600 mg) were prescribed for 3 days, anti- inflammatory (Alphinterin) were prescribed 3 times a day for 1 week and antibiotics (Augmentin 1gm tab) were prescribed 12 hourly for 5 days , antibtioc ointment. Sutures were removed after 3 weeks postoperatively. All patients were followed up at the following intervals; three weeks, three months and six months┬Ā
Results
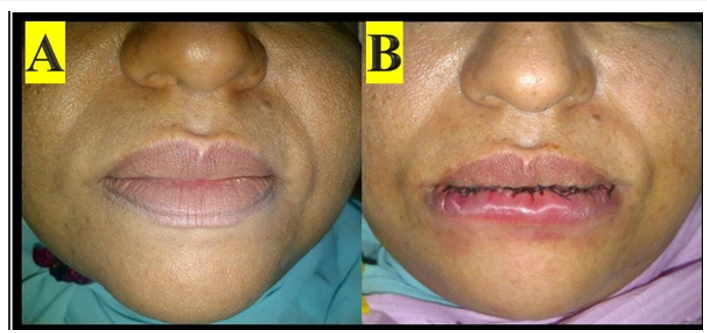
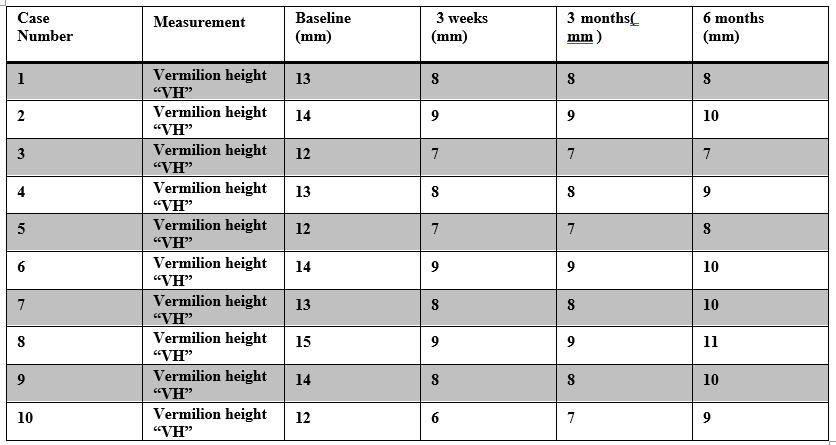
All patients reported edema that subsided within 1 week in addition to tolerable pain that was successfully controlled with the proper analgesic, other complications included tension at the lower lip which subsided within 1 month. At 3 weeks follow up there was a marked reduction in vermillion height of the lower lip and the patients were highly satisfied with the shape of their lip, this decrease in vermilion height remained stable up to 3 month follow. However at six month follow up a minute increase at the vermilion height was reported. (Figure 3&4) (Table 1)


Discussion
The goals of reduction cheiloplasty are to achieve a harmonious relationship between both upper and lower lips that is in perfect balance with the whole face and also to provide a normal lip competence. Lip reduction surgery is either performed as a classical technique or as a modified technique focusing on the resultant contour of the lip and the volume relationship between the upper and lower lip, there are few studies that discuss techniques for lip reduction [17,20].
In our study we excluded patients with large interlabial distance at rest or dentofacial deformities because if lip reduction was performed in those patients it will worsen the cosmetic deformity by overly reducing the lip size and revealing the dentofacial deformity, microgenia was also excluded because the lack of chin prominence can make the lower lip appear larger ŌĆ£PseudoŌĆØ [9]where those patients may benefit from chin augmentation procedures to obtain a balance between the chin and the lips. Furthermore smokers and patients with systemic diseases were not included in our study since those patients are not good candidate for any surgery due to retarded healing and high risk of infection [21,22].
Marked decrease in the lower lip size was attained after 3 weeks of the surgery and remained stable up to 3 month , however at six month minute increase was noticed this may be due to the fact that in our technique we just removed the epithelium which would regenerate all-over again not to mention that those tissue are stretchable and elastic, thatŌĆÖs why further studies may be needed to evaluate the effect of removing a deeper layer of the sub mucosa , different suturing technique and modifying in the original technique in order to contribute to a long lasting results.
Conclusion
Lip reduction surgery is an effective, simple technique for addressing hypertrophic lip but its stability remains questionable, further studies is needed with modifications in the original technique, increasing sample size and longer follow up periods.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
References
- Sforza M, Andjelkov K, Zaccheddu R, Jovanovic M, Colic M. (2012). The ŌĆ£BrazilianŌĆØ bikini-shaped lip-reduction technique: new developments in cheiloplasty. Aesthetic Plastic Surgery. 36(4):827-831.
View at Publisher | View at Google Scholar - Larn SM. (2005). Aesthetic facial surgery for the Asian male. Facial Plast Surg. 21:317-323.
View at Publisher | View at Google Scholar - El-Hakim M, Chauvin P. (2004). Orofacial granulomatosis pre-senting as persistent lip swelling: review of 6 new cases. J Oral Maxillofac Surg. 62(9):1114-1117.
View at Publisher | View at Google Scholar - Ali K. Ascher syndrome: a case report and review of the literature. Oral Surg Oral Med Oral Pathol. 2007;103:26-28.
View at Publisher | View at Google Scholar - Niamtu J. (2006). The use of restylane in cosmetic facial surgery. J Oral Maxillofac Surg. 64:317-25.
View at Publisher | View at Google Scholar - Nimatu J, editor. (2005). New lip and wrinkle fillers. In: Minimally invasive cosmetic surgery oral and maxillofacial surgery clinics of North America, vol. 17. Philadelphia: Saunders; P. 17-27,1.
View at Publisher | View at Google Scholar - Dev VR, Wang P. (2009). Lip reduction.
View at Publisher | View at Google Scholar - Farkas LG. (1981). Anthropometry of the head and face in medicine. New York: Elsevier Science;
View at Publisher | View at Google Scholar - Niamtu J 3rd. (2010). Lip reduction surgery (reduction cheiloplasty). Facial Plast Surg Clin North Am. 18(1):79-97.
View at Publisher | View at Google Scholar - Jittilaongwong P. (2018). Experience of 9000 cases on lip reduction surgery in Thailand. Plast Reconstr Surg Glob Open. 6(9):107-107.
View at Publisher | View at Google Scholar - Jittilaongwong P. (2018). Experience of 7145 cases on lip reduction surgery in Thailand. J Regen Med.
View at Publisher | View at Google Scholar - Rees TD, Horowita SL, Coburn RJ. (1973). Mentoplasty, prognathism and cheiloplasty. In: Rees TD, Wood-Smith, editors. Cosmetic Facial Surgery. Philadelphia: WB Saunders; Pp. 494- 553.
View at Publisher | View at Google Scholar - Hauben DJ. (1988). Reduction cheiloplasty for upper lip hemangioma. Plast Reconstr Surg. 82:694-697.
View at Publisher | View at Google Scholar - Fanous N, Brousseau VJ, Yoskovitch A. (2007). The ŌĆśbikini lip reductionŌĆÖ: a detailed approach to hypertrophic lips. Can J Plast Surg. 15(4):205-210.
View at Publisher | View at Google Scholar - Oliver DW, Scott MJ. (2002). Lip reduction cheiloplasty for MiescherŌĆÖs granulomatous macrocheilitis (Cheilitis granulomatosa) in childhood. Clin Exp Dermatol. 27(2):129-131.
View at Publisher | View at Google Scholar - Kruse-Losler B, Presser D, Metze D, Joos U. (2005). Surgical treatment of persistent macrocheilia in patients with Melkersson-Rosenthal syndrome and cheilitis granulomatosa. Arch Dermatol. (9):1085-1091.
View at Publisher | View at Google Scholar - Stucker FJ. (1988). An adjunctive procedure in the black rhinoplasty patient. Arch Otolaryngol Head Neck Surg. 114:779-780.
View at Publisher | View at Google Scholar - Pierce HE. (1976). Chelioplasty for redundant lips. J Natl Med Assoc. 68:211-212.
View at Publisher | View at Google Scholar - Field LM. (1992). Macrocheiloplasty. Principles and techniques. J Dermatol Surg Oncol. 18:503-507.
View at Publisher | View at Google Scholar - Botti G, Botti C, Cella A. (2002). A simple surgical remedy for iatrogenic excessively thick lips. Plast Reconstr Surg. 110:1335-1116.
View at Publisher | View at Google Scholar - Sorensen LT. (2015). Wound healing and infection in surgery: the pathophysiological impact of smoking, smoking cessation and nicotine replacement therapy: a systematic review. Ann Surg.;225:1069-1079.
View at Publisher | View at Google Scholar - Politis C, Schoenaers J, Jacobs R, Agbaje JO. (2016). Wound healing problems in the mouth. Front Physiol. 7:507.
View at Publisher | View at Google Scholar
