

Case Report | DOI: https://doi.org/10.31579/ 2834-8788/002
Left Main Coronary Stenting in A 83-Year-Old Patient Without Final Kissing-Dilation
1 Kazakh Research Institute of Cardiology and Internal Diseases, Khazkastan
2 The Al-Farabi Kazakh National University, Khazkastan
*Corresponding Author: Kolesnikov A.E, Kazakh Research Institute of Cardiology and Internal Diseases, Khazkastan
Citation: Kolesnikov A.E., Kuzhukeyev A.M, Abzaliev K.B. (2022). Left Main Coronary Stenting In A 83-Year Old Patient Without Final Kissing-Dilation. Journal of Heart and Vasculature.1(1); 10.31579/ 2834-8788/002
Copyright: © 2022 Mamedov M.N, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 September 2022 | Accepted: 15 September 2022 | Published: 28 September 2022
Keywords: left main disease; trifurcation lesion; provisional stenting; pci; FKBT; kissing dilatation
Abstract
Currently, the left main lesions remain a very challenging and life-threatening condition, with still controversial treatment modalities. Although many technical methods of stenting and alternate methods for assessment of the coronary flow have been developed, the left main stenting has not yet become a routine procedure that ensures a hundred per cent positive outcome. It is argued that the kissing balloon technique should routinely be used in bifurcation lesions, with FFR, IVUS and OCT used in every single case.
We present, for broader discussion, our own solution to the LM lesion. This is the case report of our patient with LM and LAD lesions and mild aortic stenosis who was successfully treated with PCI. An 83-year-old male was admitted to our hospital due to exertional dyspnea and worsening of angina pectoris
Introduction
Based on data derived from The National Cardiovascular Data Registry (NCDR®), Valle JA et al [4] reported the final cohort of 3,342,162 patients who underwent PCI from 2009 to 2016, of which number, 33,128 (1.0%) underwent unprotected left main PCI. Of these 33,128 patients who underwent unprotected left main PCI, 24,520 (74.0%) had left main coronary artery lesions rated class C, with 14,947 lesions (45.1%) involving the bifurcation. Of these bifurcation lesions, 6053 (40.5%) were treated with a 2-stent strategy. Multivessel PCI was performed in 15,635 unprotected left main interventions (47.2%) as opposed to 727,907 (22.0%) of all other PCIs.
There are multiple ways to tackle the left main trifurcation lesions, including the preplanned stenting technique (a 2-stent strategy or provisional), robust algorithm in case of complications, 3 coronary wires, guiding catheter (7Fr) with side holes and cardiac surgeons alerted in advance. Our case illustrates the stenting of LM trifurcation without “debulking” or “kissing” balloon inflation at the end of the procedure.
Case report
n admission, the patient complained of chest discomfort, intermittent non-radiating precordial pains, bating on their own, dyspnea on exertion. No subjective feelings were reported relative to BP elevations.
Precordial pain appeared in the summer of 2021. The patient has been hypertensive since last several years, up to 160/90 mm Hg, the highest. His condition deteriorated since late October 2021, when precordial pain appeared, along with unstable BP and reduced tolerance of exercise.
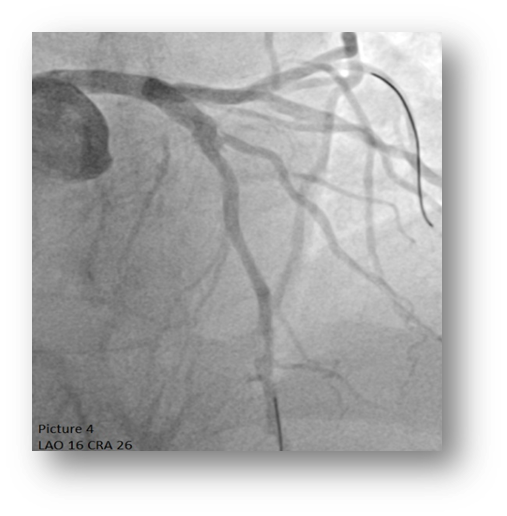
This 83-year-old Caucasian male was diagnosed with multi-vessel coronary artery disease at the private hospital, where coronary angiography was performed. Figure.1 and 2 show 60% distal atherosclerotic calcified plaque left main stenosis with chronic dissection of type A, 90% of proximal left anterior descending artery stenosis at the level of bifurcation with diagonal branch (Medina 1,1,1), Fig. 3 80% at mid-portion of LAD and 50% of proximal intermediate, left circumflex and right coronary arteries. The patient refused to get coronary artery bypass grafting CABG, and was taken to our hospital with moderately reduced ejection fraction (51% Simpson) for percutaneous coronary intervention.


Figure 1 and 2: 60% distal atherosclerotic calcified plaque left main stenosis with chronic dissection, type A

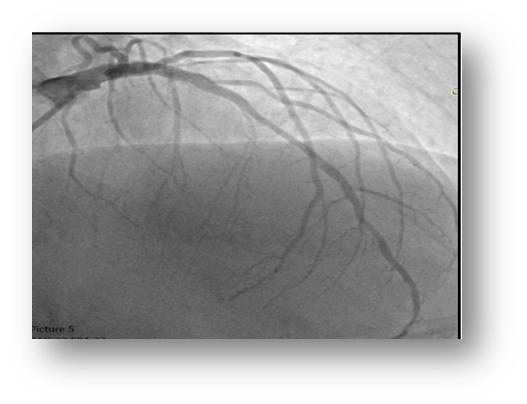
Right radial approach with 6-French Extra Back Up (XB) 3.5 guide-catheter (Cordis) was chosen to engage the left coronary artery. LAD, diagonal branch and LCX were wired with workhorse 0.014-inch silicone/hydrophilic coated wires (Sion blue, Asahi). The LM lesion was pre-dilated with a 2.75 mm x 20 mm compliant balloon at 20 atm. Contrast injection revealed a type B dissection for the distal LM extending into the proximal LAD. A 3.5 mm X 30 mm Resolute Onyx (Medtronic, Minneapolis, MN) drug-eluting stent was deployed at 18 atm. from the LMCA ostium to the proximal LAD. Proximal optimization technique with a 4.0 mm x 15 mm non-compliant balloon was performed. Unfortunately, the dissection propagated further down to the distal edge of the stent Figure.4. We were able to fully seal the dissection using a 2.75 mm x 9 mm Coroflex ISAR Neo (B. Braun, Melsungen) drug-eluting stent. Kissing balloon technique was performed in view of compromised flow in the diagonal branch. The mid-portion was stented with 2.5 mm x 12 mm Coroflex ISAR Neo (B|Braun, Melsungen) drug-eluting stent. The procedure was culminated by final POT with a 4.5 mm x 12 mm non-compliant balloon. Control coronary angiography demonstrated a fully satisfactory result without any flow-limitation in left circumflex and intermediate arteries Figure 5 and 6.

Discussion
It remains to be seen if it is mandatory to employ the final kissing balloon technique after each and every case of left main coronary stenting with obstructing the left circumflex ostium.
In his paper ‘Assessing Optimal Percutaneous Coronary Intervention’ for LMCA (AOI-LMCA) registry, a 6-center retrospective registry which enrolled 1809 consecutive patients who were given FKBT for LMCA Nishida K, et al,[1] inferred that after crossover stenting for the left main coronary artery (LMCA) FKBT after a 1-stent strategy for LMCA crossover stenting, did not affect TLR (target lesion revascularization) and other clinical outcomes during 5-year follow-up. Also, COBIS II registry (3), which included LMCA lesions in 26% of cases, demonstrated that a 1-stent technique with FKBT for any bifurcation lesion was associated with favorable long-term clinical outcomes, whereas a 1-stent strategy with FKBT for LMCA was not associated with better MACE outcomes compared with a 1-stent strategy without FKBT.
Notably, FKBT does lengthen the procedure time because of the necessity to ‘rewire’ and thrusting balloons through the stent cells to a side branch. Furthermore, FKBT is associated with the risk of dissection of the side branch ostium, which in turn, may require additional stenting. In our case, the side branch stenting would entail possible compromise of blood flow through the median artery. In such case, we would have to change it to 7 Fr guiding catheter, perform ‘rewiring’ and FKBT not only in circumflex and median artery, but also in the left main coronary artery, with the perspective of a triple simultaneous inflation of the balloons. It should be noted that additional amounts of contrast needed, could have deleterious effect on renal function, given the advanced age of our patient.
Three days after, the patient was discharged with no angina and overall improvement of physical condition. Two months later the patient underwent elective right coronary artery stenting (Figure 7 and 8). Left main and all its branches had perfect blood flow without any deterioration.
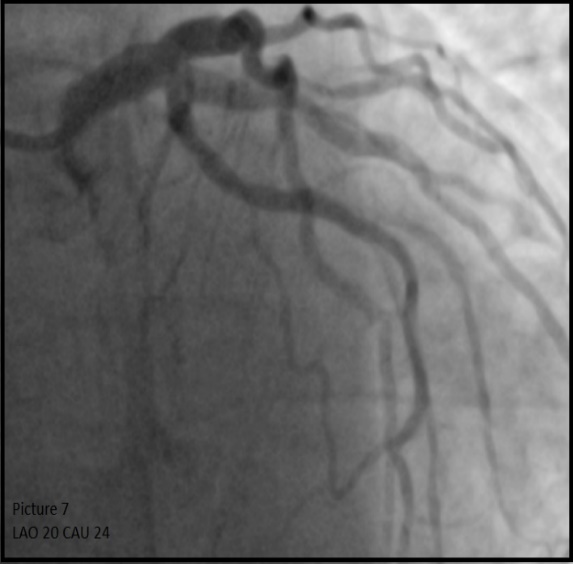

Figure 7 and 8: 2 months follow up
Conclusion
PCI of LM shall be considered as an alternative to CABG even in the elderly patients older than 80 years of age, given high potential surgical risk and complications. “Simple” provisional stenting without FKBT could be a safe and promising tool in interventional cardiologist’s toolbox.
Abbreviations: LM - left main, FKBT - final kissing balloon technique, LAD - left anterior descending artery, LCX - left circumflex artery, IA - intermediate artery, PCI - percutaneous coronary intervention, CABG - coronary artery bypass grafting, MACE - Major Adverse Cardiac Events, POT - proximal optimization technique, BP – blood pressure
References
- Nishida K, Toyofuku M, Morimoto T, Ohya M, Fuku Y et al. (2018) AOI LMCA Stenting Registry Investigators. Prognostic impact of final kissing balloon technique after crossover stenting for the left main coronary artery: from the AOI-LMCA registry. Cardiovasc Interv Ther. 2019 Jul;34(3):197-206. Epub
View at Publisher | View at Google Scholar - Niemelä, M., Kervinen, K., Erglis, A., Holm, N. R., Maeng, M., et al. for the Nordic-Baltic PCI Study Group (2010). Randomized Comparison of Final Kissing Balloon Dilatation Versus No Final Kissing Balloon Dilatation in Patients With Coronary Bifurcation Lesions Treated With Main Vessel Stenting: The Nordic-Baltic Bifurcation Study III. Circulation, 123(1), 79-86.
View at Publisher | View at Google Scholar - Yu CW, Yang JH, Song YB, Hahn JY, Choi SH, et al. (2015). Long-Term Clinical Outcomes of Final Kissing Ballooning in Coronary Bifurcation Lesions Treated With the 1-Stent Technique: Results From the COBIS II Registry (Korean Coronary Bifurcation Stenting Registry). JACC Cardiovasc Interv. 24;8(10):1297-1307.
View at Publisher | View at Google Scholar - Valle JA, Tamez H, Abbott JD, Moussa ID, Messenger JC, et al. (2019) Contemporary Use and Trends in Unprotected Left Main Coronary Artery Percutaneous Coronary Intervention in the United States: An Analysis of the National Cardiovascular Data Registry Research to Practice Initiative. JAMA Cardiol. 2019 Feb 1;4(2):100-109.
View at Publisher | View at Google Scholar
