

Research Article | DOI: https://doi.org/10.31579/2835-8465/011
Late Presentation and Early Treatment Outcome Among Subjects in a New Clubfoot Program of a Nigerian Hospital
- Dim, E.M 1*
- Edagha, I.A 2
- Peter, A.I 2
- Nottidge, T.E 1
- Ubaha, A 1
- Essien, U 1
- Amaraegbulam, P 3
- Oforjigha-Dim, C.W. BMLS 4
- Dim, U.M.E 5
1 Department of Orthopaedics and Traumatology, Faculty of Clinical Sciences, University of Uyo, Nigeria.
2 Department of Human Anatomy, Faculty of Basic Medical Sciences, University of Uyo, Nigeria.
3 Department of Orthopaedics, Federal Medical Centre, Umuahia, Nigeria.
4 Department of Medical Laboratory Services (Haematology and Blood Transfusion Services), Federal Medical Centre, Ebute -Metta, Lagos, Nigeria.
5 Nursing Services Division, National Orthopaedic Hospital, Igbobi, Lagos, Nigeria.
*Corresponding Author: Dim, E.M
Citation: Dim, E.M., Edagha, I.A., Peter, A.I, Nottidge, T.E., Ubaha, A., Essien, et al., (2024), Late Presentation and Early Treatment Outcome Among Subjects In A New Clubfoot Program Of A Nigerian Hospital. Orthopaedics Case Reports.3(1); DOI:10.31579/2835-8465/011
Copyright: © 2024 E. M. Dim, This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 January 2024 | Accepted: 16 January 2024 | Published: 26 January 2024
Keywords: congenital clubfoot; late presentation; pirani score
Abstract
Background: Congenital talipes equinovarus imposes some functional compromise on the foot, resulting in structural adaptation or modification of the local anatomy in conformity with the direction of the structural stress that subserves the abnormal function. The success or otherwise of treatment is a measure of the degree of reversal of these structural adaptations and functional deficits. The aim of this study was to evaluate the early treatment outcome in the background of late presentation among subjects in a new clubfoot program of a Nigerian university teaching hospital.
Methodology: A 6-month prospective, descriptive and health facility-based cross-sectional study of early treatment outcome of congenital talipes equinovarus among children in a Nigerian university teaching hospital is presented.
Results: Sixty-seven children met the inclusion criteria and were recruited for this study. There was a slight preponderance of males over the females, with a male to female ratio of 1.6: 1. The mean age of the study population was 31.6 ± 23.64 months. In 45 (67.2%) children, the clubfoot was bilateral and unilateral in 22 (32.8%). Idiopathic clubfoot was the commonest variant at the rate of 70.1%. Thirty-nine (58.2%) had percutaneous tenotomy (Achilles tendon tenotomy), while 28 (41.8%) did not. The mean of the total initial Pirani score (4.61±1.18) was higher than that of the total final Pirani score (0.81 ± 0.49), with p < 0.001. The mean Pirani score of the left foot (4.78 ± 1.08) in the subjects who had percutaneous tenotomy was higher than that of subjects (3.83 ± 1.88) who did not have percutaneous tenotomy (p = 0.03). The odd of subjects with callosity to achieve correction at 10 or more cast was 11.8 times that of the subjects without callosity. On a logistic regression model, total initial Pirani score and callosity were independently significant (p < 0.05) in being associated with ≥10 castings for correction. For a unit increase in total initial Pirani score, the relative risk ratio of requiring ≥10 cast was 3.49 when the other variables are held constant in the logistic regression model. The relative risk ratio of requiring ≥10 cast for correction increased by 1.03 for a unit monthly increase in the age of the subject.
Conclusion: Late presentation of clubfoot for treatment was common in this study. The Pirani score remained a reliable tool for assessing severity and monitoring treatment of clubfoot, and was valid across all age groups of clubfoot subjects seen in this study. In this study, it predicted the need or otherwise for percutaneous tenotomy, and correlated positively with the number of casting sessions required for correction.
Introduction
Congenital talipes equinovarus (CTEV, congenital clubfoot) is one of the most common structural congenital abnormalities affecting the lower limb, with a generally accepted incidence of one to two per 1000 live births [1, 2]. However, the incidence of CTEV has been reported to vary across the regions of the world from 0.6/1,000 individuals in Asia, 0.9/1,000 individuals in Australia to 6.9/1,000 individuals in Hawaii, Polynesia and Maori [3, 4]. Evidence suggests that 80% of infants with congenital clubfoot live in developing countries [5, 6, 7]. where many of them are deemed unable to receive the expected optimal treatment. It is said to be the commonest congenital musculoskeletal deformity in Nigeria, accounting for 52.8% of all malformations with live births incidence of 3.4/1000 [8-12]. The incidence in males is reportedly higher than in females, with a male to female ratio of 4:1.3 From a global perspective, it has been reported that approximately 100,000 children are born world-wide each year with clubfoot. When neglected, CTEV becomes a serious reason for physical, social, and psychological disability among the affected subjects [13].
The anatomic deformity of congenital clubfoot is characterized by four constant features, namely, equinus, mid-foot cavus, forefoot adduction and hind-foot varus. The deformity is both cosmetic and functional, with associated hypoplasia of skin, muscles, bones, tendons, ligaments and neurovascular bundle on the medial side of the foot. The affected foot is smaller than the normal foot [2, 14]. The functional adaptation occasioned by these deformities in an untreated clubfoot result in additional local anatomical changes such as callosity of the lateral border of the foot due to weight bearing on this part, increasing deformation of the tarsal bones of the foot, skin and bone infections, stiffness of the foot, limitation in mobility, and inability to wear standard shoes. [2].
The severity of clubfoot and its response to treatment is objectively assessed using the instrument of the Pirani score [15]. This is a valid and reliable method originally designed to clinically assess the amount of deformity present in an unoperated congenital clubfoot less than two years.4 In the present study, however, varying number of subjects older than two years were encountered, and were assessed and treated with the same principles as were already propounded for the non-operative treatment of congenital clubfoot [4].
The restoration of a functional, painless, plantigrade foot with good mobility is the aim and hallmark of successful treatment of congenital clubfoot. This study was done to evaluate the early treatment outcome in the background of late presentation among subjects in a new clubfoot program of a Nigerian university teaching hospital.
Methodology
Study area: This study was done at the clubfoot clinic of the Department of Orthopaedics and Traumatology, in a Nigerian university teaching hospital.
Study Design: This was a 6-month prospective health facility based cross-sectional study of subjects with congenital clubfoot seen at the clubfoot clinic from June to November, 2021.
Sample Size Determination: The Cochrane formula [16]. for sample size calculation for a population more than 10,000 was used. Estimation of sample size was based on the formula N = Z2pq/d2, where Z = a constant, 1.96 (Standard normal deviation usually set at 1.96); p = proportion or prevalence rate of disease in decimal and refers to the number of cases which are present within the population at a particular point in time. The pooled estimate for clubfoot birth prevalence for Africa is 0.96, according to Smythe et al., [17]. For the purpose of sample size calculation in this study, the prevalence rate of 0.96 was used; q = 1-p = 0.04; and d = degree of accuracy desired set at 0.05 (95 percentaccuracy was desired).
Therefore, N = 1.962 (0.96 x 0.04) 0.052
N = 59
From the above formula, a minimum sample size of 59 was calculated for this study. However, the actual sample population recruited into this study was 67.
Sampling Technique: Convenience sampling technique was employed among clubfoot subjects seen at the clubfoot clinic.
Data Collection: Data was collected using pre-tested researcher-based proforma. This proforma was completed at the point of enrolment of the subjects into the clubfoot clinic and at weekly follow-up.
Ethical Clearance: Ethical approval for the study, with ethical approval reference AD/S/96/VOL.XXI/574, was obtained from the Ethical Review Board of the university teaching hospital. Ethical procedures in the study were approved by this institutional commission of ethics in research, and all parents gave informed consent before children participation. All information was explained to participants and their parents or guardians before evaluation.
Inclusion/Exclusion criteria: The following were the inclusion criteria for the study: Subjects with congenital clubfoot; subjects 18 years or less in age; must be enrolled at the Orthopaedic/clubfoot clinic; and guardian must be willing to give informed consent. The exclusion criteria were subjects above 18 years; presence of secondary clubfoot (e.g., post-traumatic clubfoot, post poliomyelitis related clubfoot, or clubfoot associated with cerebral palsy); and subjects that were not enrolled in the clinic.
Research Protocol: Consecutive cases of researcher-diagnosed clubfoot subjects enrolled into the clubfoot clinic, and who met the inclusion criteria were selected. The need for the author to see and reassess the subjects on weekly basis to update the facts of the study was explained to the guardians. Pre-tested researcher-based proforma was used as data collecting tool. The demographic information of the subjects and their clinical history relevant to the clubfeet were extracted and documented by the author or, in some instances, by an Orthopaedic surgical trainee appointed by the researcher for this purpose at the onset of the study. All subjects were treated according to the Ponseti method [18, 19].
Initial physical examination and assessment of the subjects’ feet were done by the researcher at first presentation, noting and documenting the specific deformities of clubfoot that were present in the subjects. Each of the clubfoot was subjected to mid and hind-foot contracture scoring, and the total Pirani score calculated for each foot by the researcher or his unit partner, who is a qualified Orthopaedic Surgeon, using the Pirani score template [15]. This information was also entered into the research proforma. After calculating the Pirani scores, each subject had corrective manipulations of the clubfoot by the researcher or his unit partner, usually without requiring anaesthesia. But older or uncooperative subjects sometimes had their deformity manipulation under conscious sedation. Then, corrective manipulation was followed by application of an above the knee Gypsona plaster of Paris cast by a qualified plaster cast technician, while the Surgeon held the foot in the desired corrected position, until cast application was completed. For the older children, the Gypsona plaster casts were reinforced with a layer of Scotch cast material to avoid weakening of the Gypsona and loss of corrected positions of the deformity.
On weekly basis, after the initial manipulation and casting, the subjects were reviewed in the clubfoot clinic by the researcher or his unit partner. The previous plaster of Paris casts was removed by the plaster cast technicians, and the subjects’ feet were reassessed by the researcher and fresh Pirani scores calculated and recorded for each foot. The entire procedure of deformity manipulation and plaster cast application was repeated at weekly intervals, after reassessment and Pirani scoring of the clubfoot. The Pirani scores at each weekly follow up visit were calculated and recorded in the research proforma. Subjects whose Pirani scores dropped to one, or 0.5 with unrelenting stiffness of the Achilles tendon were made to have percutaneous tenotomy. The procedure of percutaneous Achilles tenotomy was a sterile minor clinic procedure carried out by the researcher or his unit partner, under cover of a local anaesthetic agent. Following percutaneous tenotomy, the Pirani scores often dropped to zero. The subjects were considered to have achieved correction when the Pirani scores in the feet dropped to zero, and all deformities of clubfoot were no more present. This often coincided with the timing of percutaneous tenotomy. The final Pirani scores, number of weekly plaster casting sessions required to achieve correction and the need or otherwise for percutaneous tenotomy were noted and documented in the research proforma.
Following percutaneous tenotomy, or after achieving a Pirani score of zero or 0.5, the feet were put in retention below the knee Gypsona plaster of Paris casts for three weeks. At the end of three weeks in retention cast, the feet were managed in foot abduction splints to be worn for 23 hours a day until three months in the first instance [18-20]. None of the subjects had surgery to achieve correction of the clubfoot. The procedures itemized above were performed by the author or his unit partner, with assistance from a clubfoot nurse, orthopaedic surgical trainees and trained orthopaedic plaster technicians. At every stage, data generated was entered into proforma sheets opened for individual subjects.
Data Analysis
Statistical analysis was performed using the statistical package for social science (IBM SPSS for windows version 20). Mean differences comparison were done using independent sample t-test and one way analysis of variance (ANOVA), where applicable. Association between categorical variables was analyzed using Chi-square. The association between continuous variable was done using Pearson product correlation. Tables were expressed in numbers of observation (frequency) with prevalence in percentages, and showing mean and standard deviation. Statistically significant associations and mean differences were considered at p-value less than less than 0.05 (p < 0>
Results
a. Demographic Characteristics of the Children with Clubfoot
A total of one hundred and twelve feet in 67 children with congenital talipes equinovarus (congenital clubfoot) deformities who met the inclusion criteria were seen and recruited into the study. There was a slight preponderance of males over the females, with a male to female ratio of 1.6: 1. There were 41 (61.2 %) males and 26 (38.8%) females. The mean age of the children was 31.6 ± 23.64 months. Seventeen (25.4%) of the children with clubfoot deformities were brought for treatment within the first year of life (0 - 12months). Thirty-seven (55.3%) were brought for treatment in the second and third years of life (13 - 36months), while 13 (19.4%) came for treatment after the age of three years. The highest prevalence (46.3%) of the clubfoot was seen in the firstborn children. Prevalence in subsequent births was lower, dropping to 5 (7.5%) in the fourth births and above. The mean birth weight of the children with clubfoot in this study was 3.14 ± 0.65 Kg (Table 1)
| Variables | Groups | Frequency | Percentage |
| Gender | Female | 26 | 38.8 |
| Male | 41 | 61.2 | |
| Total | 67 | 100 | |
| Age group (month) | 0-12 | 17 | 25.4 |
| 13-24 | 19 | 28.4 | |
| 25-36 | 18 | 26.9 | |
| >37 | 13 | 19.4 | |
| Total | 67 | 100 | |
Position in the Family
| 1st | 31 | 46.3 |
| 2nd | 11 | 16.4 | |
| 3rd | 20 | 29.9 | |
| ≥4th | 5 | 7.5 | |
| Total | 67 | 100 |
Table 1: Demographic characteristics of the children with clubfoot
b. Patho-anatomic Profile of Children with Clubfoot (Classification/subtypes of Clubfoot seen in the Sample Population)
Forty-five (67.2%) children had bilateral clubfoot, while 22 (32.8%) had unilateral clubfoot. In the unilateral affectation, there was equal involvement of the right and left sides. Intrinsic clubfoot was found in 39 (58.2%), while extrinsic clubfoot occurred in 28 (41.8%) of the cases. Based on the clinical subtype, there were 47 (70.1%) idiopathic, 12 (17.9%) syndromic, 7 (10.4%) recurrent and 1 (1.5%) neuropathic case among the sample population. Thirty-nine (58.2%) cases required percutaneous tenotomy (Achilles tendon tenotomy), while 28 (41.8%) did not require tenotomy in the course of treatment (Table 2).
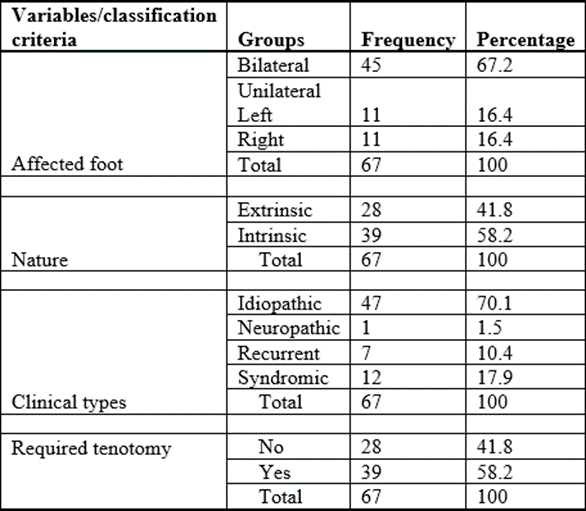
Table 2: Classification/subtypes of clubfoot seen in the sample population
c. The Comparison of Means between Left and Right Pirani Score Parameters
The measures of foot parameters by instrument of the Pirani scores were expressed in mean and standard deviation (SD). The mean of the right mid-foot and Hind-foot scores was 2.42 ± 0.61 and 2.39 ± 0.79 respectively. The mean of the left mid-foot and Hind-foot scores was 2.18 ± 0.82 and 2.21 ± 0.89 respectively. The comparison of means by independent sample t-test showed that there was no statistically significant difference (p > 0.05) between the right and left values of the Pirani scores (Table 3). The comparison of means of the initial and final Pirani scores of the right and left feet in the sample population did not show statistically significant difference (p > 0.05). The initial Pirani score refers to the score before commencement of serial manipulation and casting of the foot. The final Pirani score refers to the score at correction of deformity following serial manipulation and casting. The mean of the total initial Pirani score (4.61 ± 1.18) was higher than the total final Pirani score (0.81 ± 0.49). The analysis of the mean difference between the initial and final Pirani scores showed statistically significant difference (p < 0>
| Variable | Category | Number | Mean ± SD | t-value | p-value |
| Mid-foot score | Right | 56 | 2.42 ± 0.61 | 1.83 | 0.07 |
| Left | 60 | 2.18 ± 0.82 | |||
| Hind-foot score | Right | 58 | 2.39 ± 0.79 | 1.09 | 0.28 |
| Left | 60 | 2.21 ± 0.89 | |||
| Initial Pirani Score | Right | 58 | 4.69 ± 1.37 | 1.23 | 0.22 |
| Left | 60 | 4.36 ± 1.54 | |||
| Final Pirani Score | Right | 56 | 0.84 ± 0.51 | 0.36 | 0.72 |
| Left | 60 | 0.81 ± 0.48 | |||
| Total Pirani Score | Initial | 67 | 4.61 ± 1.18 | 24.33 | <0> |
| Final | 67 | 0.81 ± 0.49 |
Table 3: Comparison of means between left and right Pirani score parameters
The Comparison of Mean Pirani Scores and Number of Casts to Achieve Correction in Relation to Severity Levels of the Clubfoot in the Sample Population
This statistic examined the number of casts to achieve correction and the mean Pirani scores among the sample population as possible predictors of severity of clubfoot (Table 4).
| Variables | Severity | Number | Mean ± SD | 95% CI | F-value | P-value |
| Right Pirani Score | Mild | 4(6.9%) | 3.36 ± 1.84 | 0.44 - 6.31 | 2.62 | 0.08 |
| Moderate | 29(50.0%) | 4.62 ± 1.29 | 4.13 - 5.11 | |||
| Severe | 25(43.1%) | 5.0 ± 1.32 | 4.45 - 5.55 | |||
| Left Pirani Score | Mild | 5(8.3%) | 2.3 ± 1.72a | 0.17 – 443 | 10.64 | <0> |
| Moderate | 31(51.7%) | 4.1 ± 1.55b | 3.53 - 4.66 | |||
| Severe | 24(40.0%) | 5.15 ± 0.9c | 4.76 - 5.52 | |||
| Number of Cast | Mild | 5 | 3.6 ± 0.55a | 2.92 - 4.28 | 8.63 | <0> |
| Moderate | 35 | 6.46 ± 2.45b | 5.61 - 7.30 | |||
| Severe | 27 | 7.78 ± 1.91b | 7.02 - 8.53 |
NB: Values with the same alphabet superscripts (a, b, c) in the different variable groups were not statistically significantly different.
Table 4: Pirani scores and number of casts to achieve correction as predictors of severity of clubfoot
In the right foot category, the mean Pirani scores for mild, moderate and severe clubfoot deformities were 3.36 ± 1.84, 4.62 ± 1.29, and 5 ± 1.32 respectively. The comparison of means in this category showed a p-value of 0.08 (p > 0.05), suggesting that there was no statistically significant difference in the Pirani scores across the groups. In the left foot category, the mean Pirani scores for mild, moderate and severe clubfoot deformities were 2.3 ± 1.72, 4.1 ± 1.55, and 5.15 ± 0.9 respectively. Unlike the right foot category, the comparison of means by one-way ANOVA in the left foot category showed that the differences in the mean Pirani scores across the severity groups were statistically significant at p < 0>
The average number of casts to achieve correction of clubfoot in moderate and severe conditions were significantly higher than in the mild conditions (Table 4). The post-hoc analysis expressed in superscript alphabets showed that the difference in the average number of casts to achieve correction for moderate and severe clubfoot was not statistically significant. However, the difference in the average number of casts to achieve correction for mild clubfoot on the one hand, and for moderate and severe clubfoot on the other, is statistically significant.
- The comparison of mean Pirani Scores and Number of Casting between Non-Tenotomy (no) and Tenotomy (yes) Subjects
Table 5 examines the relationship of mean Pirani scores and number of castings for correction to the need or otherwise of percutaneous tenotomy in the management of clubfoot in the sample population. The result showed that the mean Pirani score of the left foot (4.78 ± 1.08) in the subjects who had percutaneous tenotomy was higher than that of subjects (3.83 ± 1.88) who did not have percutaneous tenotomy. This difference was found statistically significant at p = 0.03 (less than 0.05). On the right foot category, the mean Pirani score of subjects who had percutaneous tenotomy was 4.77 ± 1.48, while that of subjects who did not have percutaneous tenotomy was 4.59 ± 1.24. However, this difference was not found statistically significant at p = 0.62. In table 4 above, it was noted that the differences in the mean Pirani scores across the severity groups were not statistically significant in the right foot category; the same pattern is repeated here in the right foot category in Table 5.
| Variable | Tenotomy | Number | Mean ± SD | t-value | p-value |
| Right Pirani Score | No | 23 | 4.59 ± 1.24 | 0.49 | 0.62 |
| Yes | 35 | 4.77 ± 1.48 | |||
| Left Pirani Score | No | 34 | 3.83 ± 1.88 | 2.31 | 0.03 |
| Yes | 26 | 4.78 ± 1.08 | |||
| Total Initial Pirani | No | 28 | 4.27 ± 1.28 | 2.04 | 0.05 |
| Yes | 39 | 4.85 ± 1.05 | |||
| Total Final Pirani | No | 28 | 0.76 ± 0.52 | 0.66 | 0.51 |
| Yes | 39 | 0.84 ± 047 | |||
Number of Casting for correction
| No | 28 | 6.89 ± 2.53 | 0.33 | 0.74 |
| Yes | 39 | 6.69 ± 2.34 |
Table 5: The comparison of mean Pirani scores and number of casting between non- Tenotomy (no) and Tenotomy (yes) subjects
The mean of total initial Pirani scores in the tenotomy and non-tenotomy groups was 4.85 ± 1.05 and 4.27 ± 1.28, respectively, with p = 0.05. This was not significant. After treatment with serial manipulation and casting, the mean of total final Pirani scores for the tenotomy and non-tenotomy groups was 0.84 ± 0.47 and 0.76 ± 0.52 respectively, and this difference was not found statistically significant at p = 0.51. This suggests that percutaneous tenotomy had no effect on the outcome with respect to Pirani scoring. Also, the relationship between the number of castings required for correction against total initial Pirani score and total final Pirani score in the tenotomy and non-tenotomy groups was not statistically significant (Table 5).
- The Association Between Number of Casting, Age of Subjects (months) and Pirani Score Parameters
The association between the number of casting to achieve correction, Pirani score parameters and age of the subjects in months was assessed by Pearson correlation (Table 6) [21]. The result (R = 0.42) showed a moderate positive correlation with age (in months) of the subjects. All the Pirani score parameters showed low positive correlation and the association was statistically significant (p < 0>
| Variables | Mean | SD | R |
| i. No of Cast | 6.78 | 2.41 | 1 |
| ii. Age(Months) | 31.6 | 23.64 | 0.42** |
| iii. Right Midfoot score | 2.42 | 0.61 | 0.19 |
| iv. Left Midfoot score | 2.18 | 0.82 | 0.30 |
| v. Right Hindfoot score | 2.39 | 0.79 | 0.26 |
| vi. Left Hindfoot score | 2.22 | 0.89 | 0.22 |
| vii. Right Initial Pirani Score | 4.7 | 1.38 | 0.28* |
| viii. Right Final Pirani Score | 0.84 | 0.51 | 0.13 |
| ix. Left Initial Pirani Score | 4.37 | 1.54 | 0.28* |
| x. Left Final Pirani Score | 0.81 | 0.49 | 0.21 |
| xi. Total Initial Pirani | 4.61 | 1.18 | 0.33** |
| xii. Total Final Pirani | 0.81 | 0.49 | 0.15 |
** Statistically significantly correlated at less than 0.001
*Statistically significantly correlated at less than 0.05
Table 6: Pearson correlation assessing the association in relation to number of casting, age of subjects (months) and Pirani score parameter
- Factors Associated with Ten or More (≥10) Castings to Achieve Correction
The number of casting sessions to achieve correction was categorized into less than ten (<10>
| Variables | Categories | Number | <10>%) | ≥10 cast (%) | Odd Ratio | 95%CI |
| Gender | Female | 26 | 21 (80.8) | 5 (19.2) | Ref | |
| Male | 41 | 34 (82.9) | 7 (17.1) | 0.86 | 0.24 - 3.08 | |
| Pregnancy duration | Full term | 52 | 43 (82.7) | 9 (17.3) | 1 | |
| CS | 8 | 6 (75.0) | 2 (25.0) | 1.59 | 0.27 - 9.20 | |
| Post term | 7 | 6 (85.7) | 1 (14.3) | 0.76 | 0.09 - 7.45 | |
| Nature of clubfoot | Extrinsic | 28 | 16 (57.1) | 12 (42.9) | 1 | - |
| Intrinsic | 39 | 39 (100) | 0 | 0 | - | |
| Clinical type | Idiopathic | 47 | 42 (89.4) | 5 (10.6) | 1 | |
| Recurrent | 7 | 4 (57.1) | 3 (42.9) | 6.3 | 1.08 - 36. 65 | |
| Syndromic | 12 | 1 (100) | 4 (33.3) | 4.2 | 0.92 - 19.14 | |
| Neuropathic | 1 | 0 | ||||
| Varus | No | 4 | 4 (100) | 0 (0) | - | - |
| Yes | 63 | 51 (81.0) | 12 (19.0) | - | - | |
| Equinus | No | 3 | 2 (66.7) | 1 (33.3) | 1 | |
| Yes | 64 | 53 (82.8) | 11 (17.2) | 0.42 | 0.04 - 4.99 | |
| Cavus | No | 8 | 7 (87.5) | 1 (12.5) | 1 | |
| Yes | 59 | 48 (81.4) | 11 (18.6) | 1.6 | 0.18 - 14.41 | |
| Callosity | No | 40 | 38 (95.0) | 2 (5.0) | 1 | |
| Yes | 27 | 17 (63.0) | 10 (37.0) | 11.18* | 2.21 - 56.61 | |
| Tibia Torsion | No | 67 | 55 (82.1) | 12 (17.9) | - | - |
| Yes | 0 | 0 | 0 | - | - | |
| Palpable Head of Talus | No | 2 | 2 (100) | 0 (0.0) | - | - |
| Yes | 65 | 53 (81.5) | 1 (18.5) | - | - | |
| Spindle Leg | No | 53 | 46 (86.8) | 7 (13.2) | 1 | |
| Yes | 14 | 9 (64.3) | 5 (35.7) | 3.65 | 0.95 - 14.11 | |
| Tenotomy | No | 28 | 22 (78.6) | 6 (21.4) | 1 | |
| Yes | 39 | 33 (84.6) | 6 (15.4) | 0.67 | 0.19 - 2.33 | |
Severity
| Mild | 5 | 5 (100) | 0 (0) | - | - |
| moderate | 35 | 29 (82.9) | 6 (17.1) | 1 | ||
| Severe | 27 | 21 (77.8) | 6 (22.2) | 0.724 | 0.21 - 2.56 |
NB: *Variable that is significantly associated with the outcome
Table 7: Factors associated with ten or more (≥10) castings to achieve correction
- Multivariate Analysis of the Number of Castings Required to Achieve Correction in Relation to Mentioned Variables
Further evaluation of the number of casting sessions required for correction with respect to Pirani score, age and gender of the subjects, as well as presence of callosity, was done using multivariate analysis (Table 8).
| Variables | Group | Odd Ratio | 95%CI for B |
| Total Initial Pirani scores | 3.49 | (1.11 - 11.02) * | |
| Age (months) | 1.03 | (0.99 - 1.07) | |
| Gender | Female | Ref. | |
| Male | 0.40 | (0.08 - 2.10) | |
| No | Ref. | ||
| Callosity | Yes | 8.87 | (1.08 - 73.20) * |
NB: *Variables that are significantly associated with the outcome
Table 8: Multivariate analysis of the number of castings required to achieve correction in relation to mentioned variables
To adjust for multiple covariates, logistics regression model was performed with number of casts (<10 xss=removed>22 With other variables held constant, total initial Pirani score and callosity were independently significant (p < 0 xss=removed>
- Relationship between Pirani Scores and the Number of Casts to Achieve Correction
The relationship between initial Pirani scores and the number of casts to achieve correction for the left, right and bilateral clubfoot categories in the sample population is presented in correlation charts or scatter graphs (Figures 1, 2 and 3). The mean Pirani scores are plotted on the vertical axes, and the number of casts on the horizontal axes in Figures 1 and 2. In Figure 3, the number of casts to achieve correction is plotted on the vertical axis, while the total mean of Pirani scores in bilateral clubfoot is plotted on the horizontal axis. In all categories, the higher the Pirani scores, the higher the number of casting required for correction.
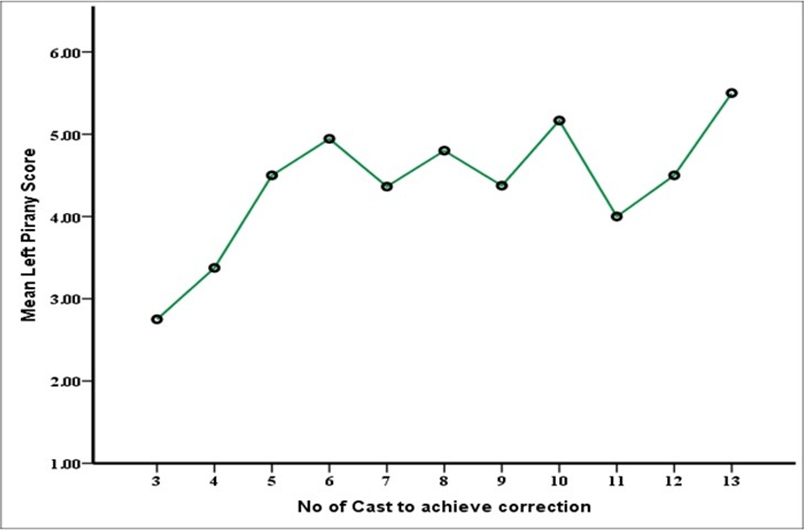
Figure 1: Correlation chart showing the relationship between Pirani score and number of casting to achieve correction in left-sided clubfoot.
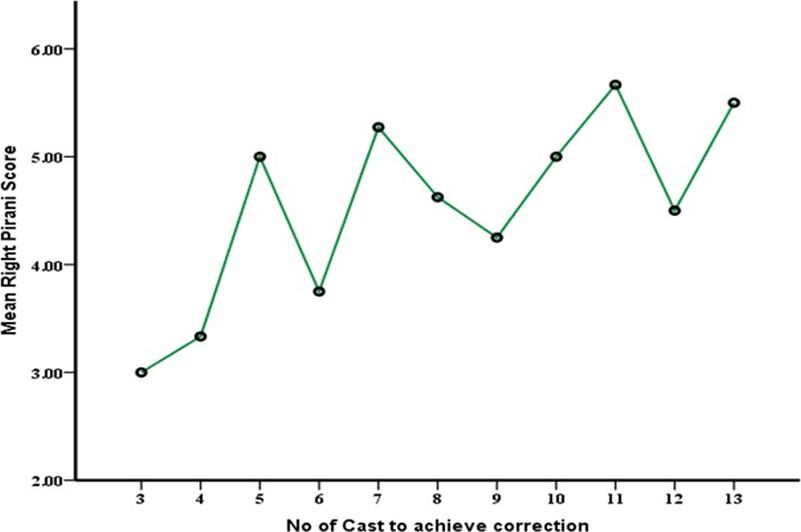
Figure 2: Correlation chart showing the relationship between Pirani score and number of casting to achieve correction in right-sided clubfoot
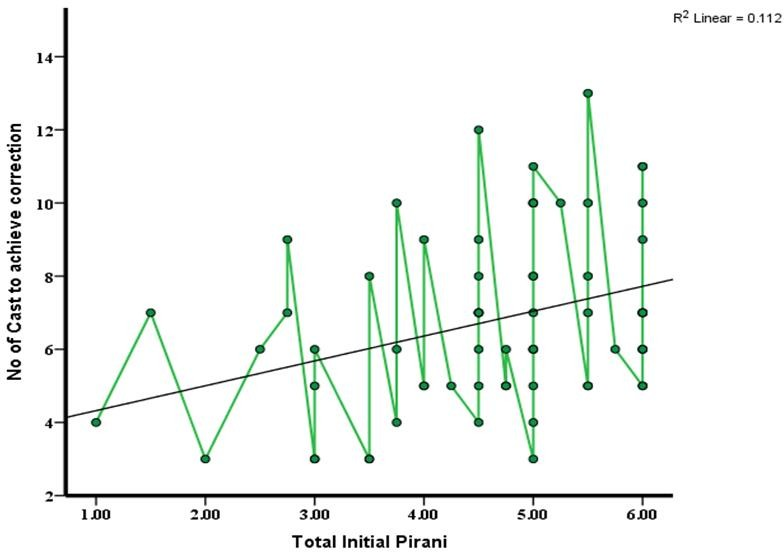
Figure 3: Correlation chart showing the relationship between Pirani score and number of casting to achieve correction in bilateral clubfoot
Discussion
This is a prospective study aimed at evaluating the early treatment outcome, in the background of late presentation among subjects, in a new clubfoot program of a Nigerian university teaching hospital. Notably, congenital talipes equinovarus (CTEV), also commonly known as congenital clubfoot, is reportedly the commonest congenital musculoskeletal deformity in Nigeria, and a leading cause of disability world over, with over 80% of cases believed to be domiciled in developing countries, where clubfoot is adjudged a major disease burden in low-resource settings [5, 7-9, 11, 12, 23-25]. In the course of this study, the overall burden of CTEV relative to other paediatric disorders in the study centre was estimated at 3.04%. If left untreated, CTEV can become a severe disability and deformity that remains with the child into adulthood.26-27 The basic pathological anatomy of clubfoot, as manifested at birth, shows that the foot is turned downwards and rotated internally at the ankle, in varying degrees of severity. There is a twisting of the foot out of shape on account of a co-existing shortening of the Achilles tendon as well as other contiguous soft tissue compromise, giving rise to a club-shaped foot. Such a deformed foot is incapable of normal functions, including weight-bearing, ambulation and wearing of normal shoes [6, 12].
The average age of the children encountered in this study was 31.6 ± 23.64 months. This is very different from the findings by some authors in different locations in Nigeria [11, 12]. About 17 (25.4%) children in this study were within the age of one year, while 37 (55.3%) of these children were brought for treatment in the second and third years of life (13 - 36months). The sample populations studied by Mejabi et al., and Ugorji et al., were much younger than the sample population of this study [11,12]. This is probably because clubfoot clinic service is relatively young in the study centre. The initial clubfoot subjects seen in the study centre comprised neglected and abandoned cases living with the deformity within the various communities across the catchment area of the study centre. These cases came to the study centre as a result of community awareness and sensitization programmes by the clubfoot team of the hospital, following an organized treatment programme, facilitated by the author, with the support of the Miracle Feet Foundation (United States of America), in conjunction with the Straight Child Foundation (Umuahia, Nigeria). Therefore, it is not surprising that the initial cases managed under the programme comprised a lot of older children, who hitherto lived with the deformity in the communities. It is expected that, by the time the older children population with clubfoot is mopped up by the on-going treatment programme, a younger children population in their infancy and neonatal period will become more prevalent, as is the situation elsewhere, 11, 12 with much older clubfoot treatment programmes than that of the present study centre. The activities of unorthodox practitioners such as traditional bone setters (TBS) and even spiritual houses may have contributed in diverting the attention of some parents of children in this study from seeking proper care of the clubfoot at early stages. Asuquo et al., have reported cases as old as nine years at first presentation to the hospital [28]. To the best of our knowledge, this work is the first scientific documentation of clubfoot emanating from the study centre.
The Pirani score, developed by Pirani et al., is one of the numerous classification systems of clubfoot, and is a useful tool for the initial and follow up assessments of the disease [11, 15, 29-32]. The Pirani system had been validated and proven reliable to accurately quantify the severity of a clubfoot deformity, and is now routinely used in describing the outcomes of treatment [11, 33]. Using the Pirani score as a measure of severity of the disease, a score of five or more is classified as very severe and a score of less than five is classified as less severe by some authorities [34, 35]. Unlike Gray et al., and Agarwal et al., Mejabi et al., classified clubfoot, based on Pirani scores, into mild (Pirani score less than or equal to three), moderate (Pirani score more than three, but not up to five) and severe (Pirani score of five and above) [11, 34, 35]. In addition to the Pirani scoring, the severity of clubfoot is also determined based on the number of casting sessions required to overcome the soft tissue stiffness in the foot, and on the need for subcutaneous or percutaneous tenotomy of the Achilles tendon. Based on the number of casting sessions and the need for tenotomy, clubfoot has been classified into mild, moderate and severe [11, 18]. Mild cases require five casting sessions or less without tenotomy; moderate cases require more than five casting sessions without tenotomy, or five casting sessions or less with tenotomy; while severe cases require more than five casting sessions with tenotomy [11]. Other classification or scoring systems have been developed by scholars working independently [29, 36, 37]. Of all these scoring or classification systems, the one proposed by Pirani et al., is the most famous, objective and versatile system, and had been validated and proven reliable to accurately quantify the severity of a clubfoot deformity, and it is now routinely used by clinicians in describing the outcomes of treatment [11,15, 33]. The present study was based on the Pirani scoring system.
In this study, the comparison of means between the left and right foot Pirani score parameters is presented in Table 3. The measures of foot parameters by instrument of the Pirani scores were expressed in mean and standard deviation (SD). The mean of the right mid-foot and hind-foot scores was 2.42 ± 0.61 and 2.39 ± 0.79, respectively. The mean of the left mid-foot and hind-foot scores was 2.18 ± 0.82 and 2.21 ± 0.89, respectively. The comparison of means by independent sample t-test showed that there was no statistically significant difference (p > 0.05) between the right and left values of the Pirani scores. The comparison of means of the initial and final Pirani scores of the right and left feet in the sample population did not show statistically significant difference (p > 0.05). The initial Pirani score refers to the score before commencement of serial manipulation and casting of the foot. The final Pirani score refers to the score after correction of deformity by serial manipulation and casting. The mean of the total initial Pirani score (4.61 ± 1.18) was higher than that of the total final Pirani score (0.81 ± 0.49). The analysis of the mean difference between the initial and final Pirani scores showed statistically significant difference (p < 0>et al., in Ile Ife, Nigeria, and by Iltar et al., in Turkey [11, 38]. As stated by these authors, it means that the progress of treatment of clubfoot, even in our environment, can be assessed using the Pirani scoring system [11]. In this study, the average age of the sample population was higher than that of the population in the study by Mejabi et al., and Iltar et al., [11,44]. This notwithstanding, the Pirani system still proved useful in the assessment in the different populations. From this finding, it may well be stated that the Pirani score system is valid across all age groups afflicted by clubfoot. This finding gives credence to the universal applicability of the Pirani scoring system in assessment of clubfoot.
This study found it convenient, on account of sharing similar geographic space, to segregate its sample population into severity levels in line with the model of Mejabi et al., in Ile Ife, Nigeria, using the Pirani score system [11]. In the right foot category, this study recorded 4 (6.9%) mild, 29 (50.0%) moderate and 25 (43.1%) severe cases. In the left foot category, it recorded 5 (8.3%) mild, 31 (51.7%) moderate and 24 (40%) severe cases (Table 4). Unlike the right foot category, the comparison of means by one-way ANOVA in the left foot category showed that the differences in the mean Pirani scores across the severity groups were statistically significant at p < 0> 0.05), and this may well be a chance occurrence. This study showed more severe cases of clubfoot than the ones reviewed by Mejabi et al., and Itlar et al., [11, 38]. This may be as a result of the higher age of patients in our sample population compared with the patients reviewed by these authors, whose patients were mainly in the neonatal period or in the infancy period within the first year of life. Unlike the report by these authors, the average age of patients in the present study was 31 months, by which time these patients were already walking on the deformed feet. Walking on a clubfoot causes secondary bony and soft tissue changes which render the clubfoot more resistant, thereby increasing the Pirani score and severity of the clubfoot. This study believes that walking on the foot, therefore, can convert an initial mild clubfoot to a moderate or severe clubfoot. This is probably the explanation for the higher number of moderate and severe cases in the present study.
The average number of cast to achieve correction of clubfoot in moderate and severe conditions were significantly higher than in the mild conditions (Table 4). The post-hoc analysis expressed in superscript alphabets showed that the difference in the average number of casts to achieve correction for moderate and severe clubfoot was not statistically significant. However, the difference in the average number of casts to achieve correction for mild clubfoot on the one hand, and for moderate and severe clubfoot on the other, was statistically significant. This can also be explained by the phenomenon of increased soft tissue resistance occasioned by walking on the clubfoot as recorded in this study. It follows, therefore, that the older the patients, the more likely the Pirani scores would be increased due to age-related soft tissue changes, and the more casting sessions that would be required to overcome this soft tissue stiffness.
In this study, the need or otherwise for percutaneous tenotomy in the management of clubfoot in the sample population was compared with the mean Pirani scores and number of castings for correction (Table 5). It was found that the mean Pirani score of the left foot (4.78 ± 1.08) in the subjects who had tenotomy was higher than that of subjects (3.83 ± 1.88) who did not have tenotomy. This difference was found statistically significant at p = 0.03 (less than 0.05). On the right foot category, the mean Pirani score of subjects who had tenotomy was 4.77 ± 1.48, while that of subjects who did not have tenotomy was 4.59 ± 1.24. However, this difference was not found statistically significant at p = 0.62. It has already been noted that the differences in the mean Pirani scores across the severity groups were not statistically significant in the right foot category, and the same pattern is repeated here in the right foot category with respect to the need or otherwise for tenotomy. The mean of total initial Pirani scores in the tenotomy and non-tenotomy groups was 4.85 ± 1.05 and 4.27 ± 1.28, respectively (p = 0.05). This was not statistically significant.
After treatment with serial manipulation and casting, the mean of total final Pirani scores for the tenotomy and non-tenotomy groups was 0.84 ± 047 and 0.76 ± 0.52, respectively, and this difference was not found statistically significant at p = 0.51. This suggests that tenotomy had no effect on the outcome with respect to Pirani scoring. Also, the relationship between the number of castings required for correction against total initial Pirani score and total final Pirani score in the tenotomy and non-tenotomy groups was not statistically significant (Table 5). This may be due to the sample size in this study, as evidence from large cohorts of other authors showed that the Pirani score may determine the number of casting sessions for correction.39 In this study, Pirani scores dropped to zero or less than one in 28 (41.8%) subjects with tenotomy and in 39 (58.2%) subjects without tenotomy after serial manipulations and sessions of casting. These findings appear to suggest that there is no relationship between Pirani scores and the number of castings needed for correction, and that Pirani scores may not always be predictive of the need for tenotomy. They also suggest that tenotomy may be superfluous sometimes, and unnecessary in some clubfoot management, perhaps especially in the idiopathic forms. By this finding, this study suggests that tenotomy may not be made compulsory in the management of clubfoot, but rather, patients may be approached based on their individual merits. Although this opinion may seem to negate an established principle of mandatory percutaneous tenotomy in the routine management of clubfoot as enunciated by Ponseti, there is a reason to suggest that it may be valid and worthy of further investigation [18, 39-41]. In managing these late cases of clubfoot in this study, the author incorporated the scotch cast to reinforce the Gypsona plaster of Paris cast routinely applied to uncomplicated clubfoot according to the Ponseti method (Figure 4).

Figure 4: Scotch cast reinforcement of the Gypsona cast in the older child
The idea of the scotch cast was to strengthen the Gypsona plaster of Paris to hold the deformities in the manipulated position to avoid loss of correction achieved by the manipulation until patient is seen on next appointment. This technique was applied on those subjects, considered as complicated, and who were already walking before presentation to the facility.
Also, according to Pearson correlation analysis (Table 6), Pirani scores did not determine the number of castings to achieve correction in this study, but showed that the higher the age of the subjects at presentation in this study, the higher the number of castings required to achieve correction. The average age of the subjects in this study was 31months, clearly indicating late presentation. However, this relationship between the number of castings and the Pirani scores according to Pearson correlation analysis is different when subjected to a multivariate analysis as presented in Table 8.
The presence of callosity was the only variable significantly associated with ten or more casting sessions to achieve correction in this study, according to univariate analysis. The odd of subject with callosity to achieve correction with ten or more casting sessions was 11.8 times that of the subjects without callosity. The number of castings to achieve correction was not found to be significantly affected by other variables subjected to univariate analysis in this study (Table 7). Callosity is a feature of a complicated, untreated and neglected clubfoot. When clubfoot is untreated or partially treated, the child with the clubfoot walks on the side or top of the foot because the bones and joints of the foot become fixed in the deformed position [6, 7, 40]. As the child continues to walk on the sides of the foot, secondary bony and soft tissue changes are accentuated in the foot. The skin and underlying soft tissue of the lateral border of the foot is subjected to repetitive cycles of tissue breakdown and healing by fibrosis and hyperkeratinisation, resulting in callosity (callus formation), decreased mobility and pain in the foot [6, 7, 40, 42-45]. Callosity is also a trademark of late presentation, of which several factors have been blamed. Poverty, ignorance, lack of access to trained manpower, and need to travel several kilometres to access treatment have been mentioned [7, 11]. Callosities may be predictive of difficult treatment in the younger child, and is an indicator of a need for surgical intervention in the older child [43, 44]. Surgical treatment was not part of the plan in this study, and none of the cases was subjected to any surgical treatment, apart from the percutaneous Achilles tenotomy, which is considered as part of the non-operative management of clubfoot [18, 40, 41, 39].
To further evaluate (as different from the univariate analysis mentioned above) the requirement for casting sessions needed for correction with respect to Pirani score, age and gender of the subjects, as well as presence of callosity, a multivariate analysis was performed (Table 8). To adjust for multiple covariates, logistics regression model was performed with number of casts (<10 xss=removed>et al., [39]. It is, therefore, evident from all analysis in this study that, the number of casting sessions required to correct a clubfoot depended on the age of the subject, the intial Pirani score and the presence of callosities.
The relative risk ratio of requiring ≥10 cast for correction increased by 1.03 for a unit monthly increase in the age of the subject. From the multivariate analysis using the female gender as reference, the male gender had 0.4 times less odd of needing ≥10 castings for correction compared to the female gender, with other variables held constant at 95% confidence interval (Table 8). Using the male gender as reference, the odd of female subjects requiring ≥10 cast for correction was 2.68 times that of male subjects. Therefore, this study found female gender as requiring more number of casts, unlike the study by Smythe et al, in which male gender was associated with increased clubfoot severity and, therefore, higher number of required casting sessions than in the female gender [39]. In other words, this study showed that the age of the patient, female gender, the initial Pirani score and the presence of callosities were predictive of severity in clubfoot disorders in the study cohort. Similar findings have been documented by other scholars [11, 46, 39, 47].
The average number of casting sessions required for correction in this study was 3.6 ± 0.55 for mild clubfoot, 6.46 ± 2.45 for moderate cases and 7.78 ± 1.91 for severe cases. The average number of casting sessions required to achieve correction represented the duration of treatment in weeks, since the casting sessions were done on weekly basis. Although the subjects in this study were much older than those in other study centres, their mean requirements for casting sessions was comparable to those of their younger counterparts in other studies [11, 46, 48, 49]. According to Mejabi et al., the implication of this may be the fact that outcome of clubfoot treatment may not be significantly affected by age at presentation as long as the subject is an infant [11]. But from this study, the finding even calls for more attention since 17 (25.4%) of the children with clubfoot deformities were brought for treatment within the first year of life (0-12months), and 37 (55.3%) were brought for treatment in the second and third years of life. As suggested by Mejabi et al., this may need further research.
Subjects in this study sample were at different stages of follow up programmes, and such short-term outcome parameters as painless and plantigrade feet, and ability to wear shoes were satisfactorily established in the affected subjects as at the time of preparing this manuscript. Long-term follow up of treated cases is important to detect recurrences or relapses. At one year after initial correction, 15 (22.4%) of the 67 subjects in this study had shown some recurrence of varying degrees. Recurrence (or relapse) is defined as the development of one or more of the original deformities (equinus, varus, adductus and cavus) after initial full correction of all deformities of both the hind-foot and the fore-foot [13, 18, 41]. The cause of recurrence is unknown, but it is logically the same mechanism that initially caused the deformities to develop and it is related to rapid growth of the foot. Recurrence is rare after the age of 4 – 5 years and almost never occurs after 7 years of age [13]. This data, as presented by Wallander, may hold for subjects that were seen early in the neonatal or infancy period [13]. Since more subjects in this study came in their second and third years of life, it will be interesting to compare this statement on outcome by Wallander with data from long-term follow-up of subjects in this present study. One key essence of treatment is to improve the quality of life of the affected children, but the concept of quality of life in this instance should be measured from the patient’s perspective. In a study by Wallander [13] on 170 subjects (252 clubfeet) with an average follow-up of 16 years, female patients were found to be less satisfied and more concerned about the shape of their feet and legs compared with their male counterparts, even without demonstrable difference in physical function [13]. One possible explanation could be that women are more cosmetically conscious than men. In the long run, more than 80% of the feet yield good functional long-term results [13].
Conclusion
This study showed that late presentation of clubfoot for treatment was common. The Pirani score was a reliable tool for severity assessment and monitoring of treatment, and was valid across all age groups affected by clubfoot. The Pirani score positively correlated with the need or otherwise for percutaneous tenotomy, as well as the requirement of casts for correction. The number of casting session to achieve correction depended on the severity of the clubfoot, the age and gender of the subjects, and the presence or of callosity. The Pirani score, female gender, age of patient and presence of callosity were independent risk factors for severity in the study. There was no evidence that percutaneous tenotomy enhanced the outcome with respect to Pirani scoring in idiopathic clubfoot. These findings appear to suggest that there is no relationship between Pirani scores and the number of castings needed for correction, and that Pirani scores may not always be predictive of the need for tenotomy. The use of scotch cast reinforcement over the Gypsona plaster of Paris cast may reduce the need for percutaneous tenotomy.
Disclosures
- Treatment sponsorship for congenital talipes equinovarus deformities in the study centre was provided by the Miracle Feet Foundation, United States of America, in conjunction with the Straight Child Foundation, Umuahia, Nigeria;
- This manuscript was adapted from a dissertation submitted by the first author to the postgraduate school of the University of Uyo, Nigeria, in December 2021, in partial fulfilment of the requirements for the award of the Master of Science degree (MSc) in Anatomy.
- This work and other parts of the entire work was presented orally at the Annual General Meeting of the Nigeria Orthopaedic Association held in Calabar in November 2021.
- The literature review portion of the entire MSc work has been published as a review article (Congenital talipes equinovarus: A review. Journal of Orthopedic Surgery and Techniques. 5(2): 474 – 486. ISSN: 2578-7187. Doi: 10.36959/453/595).
Conflict of interests
The authors have no conflict of interests to declare.
References
- Maranho DA, Volpon JB. (2011). Congenital clubfoot. Acta Ortopedica Brasileira. 19(3): 163-169.
View at Publisher | View at Google Scholar - Manisha R, Priyanka K. (2017). Congenital clubfoot: A comprehensive review. Orthopaedics & Rheumatology Open Acces. 8(1):555-728.
View at Publisher | View at Google Scholar - Ricco A, Richards B, Herring J. In: Herring, J. (Ed.) (2014). Tachdjian’s Paediatric Orthopaedics 5th ed. Philadelpia. Elsevier. 785-818.
View at Publisher | View at Google Scholar - Martanto TW, Dominica H, Irianto KA, Bayusentono S, Utomo DN. (2020). The Pirani score evaluation on patients with clubfoot treated with the Ponseti method in public hospital. Eurasian Journal of Biosciences. 14:3419-3422.
View at Publisher | View at Google Scholar - Saltzman HM. (2009). Foot focus: International initiative to eradicate clubfeet using the Ponseti method. Foot & Ankle International. 30(5): 468-471.
View at Publisher | View at Google Scholar - Smythe T H. (2018). Evidence to improve clubfoot services in Africa with Zimbabwe as a case study. PhD (research paper style) thesis, London School of Hygiene and Tropical Medicine.
View at Publisher | View at Google Scholar - Hegazy MA, Khairy HM. Hegazy AA, El-Aidy SM. (2021). Clubfoot in children: An overview. The Foot and Ankle Online Journal. 13(4):10.
View at Publisher | View at Google Scholar - Omololu B, Ogunlade SO, Alonge TO. (2005). Pattern of congenital orthopaedic malformations in an African teaching hospital. West African Journal of Medicine. 24(2): 92-95.
View at Publisher | View at Google Scholar - Adewole OA, Giwa SO, Kayode MO, Shoga MO Balogun RA. (2009). Congenital clubfoot in a teaching hospital in Lagos, Nigeria. African Journal of Medicine and Medical Sciences. 38(2): 203-206.
View at Publisher | View at Google Scholar - Ukoha U, Okafor A, Ogugua I, Udemezue P, Olisah O, Anyabolu, R. (2011). Incidence of congenital talipes equinovarus among children in SouthEast Nigeria. International Journal of Biological & Medical Research. 2:712-715.
View at Publisher | View at Google Scholar - Mejabi JO, Esan IO, Adegbehingbe OO, Orimolade EA, Asuquo J, Badmus HD, Anipole AO. (2016). The Pirani scoring system is effective in assessing severity and monitoring treatment of clubfeet in children. British Journal of Medicine and Medical Research. 17(4):1-9.
View at Publisher | View at Google Scholar - Ugorji TN, Nwakamma JI, Anoliefo KT, Worgu FC. (2020). Epidemiology and pattern of clubfoot in Enugu, South-East Nigeria. American Journal of Biomedical Science and Research. 11(2): 190-193.
View at Publisher | View at Google Scholar - Wallander HM. (2010). Congenital clubfoot. Acta Orthopaedica. 81:1-25.
View at Publisher | View at Google Scholar - Strach EH. (1986). Clubfoot through the Centuries. Progress in Pediatric Surgery, Springer-Verlag. 20:215-237.
View at Publisher | View at Google Scholar - Pirani S, Hodges D, Sekeramayi F. (2008). A reliable and valid method of assessing the amount of deformity in the congenital clubfoot deformity. In: Orthopaedic Proceedings. The British Editorial Society of Bone & Joint Surgery. 90(I):53-53.
View at Publisher | View at Google Scholar - Cochran WG. (1963). Sampling techniques. Wiley. New York.
View at Publisher | View at Google Scholar - Smythe T, Kuper H, Macleod D, Foster A, Lavy C. (2017). Birth prevalence of congenital talipes equinovarus in low- and middle-income countries: a systematic review and meta-analysis. Tropical Medicine and International Health. 22(3): 269-285.
View at Publisher | View at Google Scholar - Ponseti IV. (2000). Clubfoot management. Journal of Paediatric Orthopedics. 20(6): 699-700.
View at Publisher | View at Google Scholar - Ponseti IV, Smoley EN. (2009). The classic congenital club foot: The results of treatment. Clinical Orthopaedics and Related Research. 467(5): 1133-1145.
View at Publisher | View at Google Scholar - Ponseti IV. (1996). Congenital clubfoot: fundamentals of treatment. Oxford: Oxford University Press. Pp. 1-140.
View at Publisher | View at Google Scholar - Cohen J. (1992). A power primer. Psychological Bulletin, 112: 155-159.
View at Publisher | View at Google Scholar - Nagelkerke NJD. (1991). A note on the general definition of the coefficient of determination. Biometrika. 78(3): 691-692.
View at Publisher | View at Google Scholar - Palma M, Cook T, Segura J, Pecho A, Jose A, Morcuende JA. (2013). Descriptive epidemiology of clubfoot in Peru: a clinic-based study. The Iowa Orthopaedic Journal. 33: 167-171.
View at Publisher | View at Google Scholar - Barker S, Chesney D, Miedzybrodzka Z, Maffulli N. (2003). Genetics and epidemiology of idiopathic congenital talipes equinovarus. Journal of Paediatric Orthopaedic. 23:265- 272.
View at Publisher | View at Google Scholar - Morcuende AJ. (2006). Congenital idiopathic clubfoot: prevention of late deformity and disability by conservative treatment with the Ponseti technique. Paediatric Annals. 35(2): 128-136.
View at Publisher | View at Google Scholar - O’Shea RM, Sabatini CS. (2016). What is new in idiopathic clubfoot? Current Reviews in Musculoskeletal Medicine. 9(4): 470-477.
View at Publisher | View at Google Scholar - Sadler B, Gurnett CA, Dobbs MB. (2019). The genetics of isolated and syndromic clubfoot. Journal of Children Orthopaedics. 13:238-244. DOI: 10.1302/1863-2548.13.190063
View at Publisher | View at Google Scholar - Asuquo JE, Abang IE, Anisi C, Urom S, Agweye P, Ngim NE, Okeke EN. (2016). Descriptive epidemiology and predisposing factors to idiopathic talipes equinovarus in south south Nigeria. Journal of Public Health and Epidemiology. 8(8): 147-151.
View at Publisher | View at Google Scholar - Dimeglio A, Bensahel H, Souchet P, Mazeau P, Bonnet F. (1995). Classification of clubfoot. Journal of Paediatric Orthopedics. 4(2): 129-136.
View at Publisher | View at Google Scholar - Harrold AJ, Walker CJ. (1983). Treatment and prognosis in congenital club foot. The Journal of Bone and Joint Surgery. 65(1): 8-11.
View at Publisher | View at Google Scholar - Celebi L, Muratli HH, Aksahin E, Yagmurlu MF, Bicimoglu AB. (2006). International Clubfoot Study Group evaluation of treated clubfoot: Assessment of interobserver and intraobserver reliability. Journal of Pediatric Orthopaedics. 15(1): 34-36.
View at Publisher | View at Google Scholar - Chu A, Labar AS, Sala DA, van Bosse HJ, Lehman WB. (2010). Clubfoot classification: Correlation with Ponseti cast treatment. Journal of Pediatric Orthopedics. 30(7):695-699.
View at Publisher | View at Google Scholar - Scher DM, Feldman DS, van Bosse HJ, Sala DA, Lehman WB. (2004). Predicting the need for tenotomy in the Ponseti method for correction of clubfeet. Journal of Pediatric Orthopedics. 24(4):349-352.
View at Publisher | View at Google Scholar - Gray K, Barnes E, Gibbons P, Little D, Burns J. (2014). Unilateral versus bilateral clubfoot: ananalysis of severity and correlation. Journal of Pediatric Orthopaedics. 23(5): 397-399.
View at Publisher | View at Google Scholar - Agarwal A, Agrawal N, Barik S, Gupta N. (2018). Are bilateral idiopathic clubfeet more severe than unilateral feet? A severity and treatment analysis. Journal of Orthopaedic Surgery. 26(2): 1-2.
View at Publisher | View at Google Scholar - Nordin S, Aidura M, Razak S, Faisham WI. (2002). Controversies in congenital clubfoot: literature review. Malaysian Journal of Medical Sciences. 9(1): 34- 40.
View at Publisher | View at Google Scholar - Cummings RJ, Lovell AW. (1998). Current concept review: Operative treatment of congenital idiopathic club foot. Journal of Bone and Joint Surgery. 70:1108-1112.
View at Publisher | View at Google Scholar - Iltar S, Uysal M, Alemdaroglu KB, Aydogan NH, Talip Kara T, Dogan Atlihan D. (2010). Treatment of clubfoot with the Ponseti method: Should we begin casting in the newborn period or later? The Journal of Foot and Ankle Surgery. 49: 426-431.
View at Publisher | View at Google Scholar - Smythe T, Chandramohan D, Bruce J, Kuper H., Lavy C, Foster A. (2016). Results of clubfoot treatment after manipulation and casting using the Ponseti method: experience in Harare, Zimbabwe. Tropical Medicine and International Health. 21(10):1311-1318.
View at Publisher | View at Google Scholar - Lavy C. (2017). Africa Clubfoot Training: Basic & Advanced Clubfoot Treatment Provider Courses Participant Manual, University of Oxford. 15- 27.
View at Publisher | View at Google Scholar - Ponseti IV, (1963). Smoley EN Congenital Club Foot: The Results of Treatment. The Journal of Bone and Joint Surgery. 45(2):261-344.
View at Publisher | View at Google Scholar - Dobbs MB, Gurnett CA. (2009). Update on clubfoot: etiology and treatment. Clinical Orthopaedics and Related Research. 467:1146-1153.
View at Publisher | View at Google Scholar - Sobel E, Giorgini R, Velez Z. (1996). Surgical correction of adult neglected clubfoot: Three case histories. Journal of Foot Ankle Surgery. 35: 27-38.
View at Publisher | View at Google Scholar - Mirzaya, R, Early SD, Matthys GA, Thordarson DB. (2001). Single-stage talectomy and tibiocalcaneal arthrodesis as a salvage of severe, rigid equinovarus deformity. Foot and Ankle International. 22: 209-213.
View at Publisher | View at Google Scholar - Penny JN. (2005). The Neglected Clubfoot. Techniques in Orthopaedic Surgery in the Developing World. 20(2):153-166.
View at Publisher | View at Google Scholar - Awang M, Sulaiman AR, Munajat I, Fazliq ME. (2014). Influence of age, weight, and pirani score on the number of castings in the early phase of clubfoot treatment using ponseti method. The Malaysian Journal of Medical Sciences. 21(2):40-43
View at Publisher | View at Google Scholar - Agarwal A. Gupta N. (2014). Does initial Pirani score and age influence number of Ponseti casts in children? International Orthopaedics. 38(3): 569-572.
View at Publisher | View at Google Scholar - Laaveg SJ, Ponseti IV. (1980). Long-term results of treatment of congenital club foot. The Journal of Bone and Joint Surgery. 62(1): 23 - 31.
View at Publisher | View at Google Scholar - Pulak S, Swamy M. (2012). Treatment of idiopathic clubfoot by Ponseti technique of manipulation and serial plaster casting and its critical evaluation. Ethiopian Journal of Health Sciences. 22(2):77-84
View at Publisher | View at Google Scholar
