

Research Article | DOI: https://doi.org/10.31579/2834-8664/008
knowledge of the doctors in attention primary on Sexual and Reproductive Health in teenagers and young
1First degree specialist in Obstetrics and Gynaecology. Second grade specialist in Comprehensive General Medicine. Master in Comprehensive Care for Women . Assistant Professor. Luis Augusto Turcios Lima Polyclinic. Mayabeque. Cuba.
2Second Degree Specialist in School Hygiene. Master in Epidemiology. Researcher and Assistant Professor. National Institute of Hygiene, Epidemiology and Microbiology. Havana. Cuba.
*Corresponding Author: Alba Cortes Alfaro, Second Degree Specialist in School Hygiene. Master in Epidemiology. Researcher and Assistant Professor . National Institute of Hygiene, Epidemiology and Microbiology. Havana. Cuba.
Citation: Alba Cortes Alfaro, (2022) Knowledge of the doctors in attention primary on Sexual and Reproductive Health in adolescents and young people. International Journal of Clinical and Medical Case Reports, 1(2); Doi: 10.31579/2834-8664/008
Copyright: © 2022 Alba Cortés Alfaro, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 September 2022 | Accepted: 19 October 2022 | Published: 25 November 2022
Keywords: adolescents/youth; knowledge; sexual and reproductive health
Abstract
Introduction: the problem of sexual and reproductive health during youth is linked to risky sexual practices. It is up to primary care to carry out promotional actions. The Ministries of Public Health and Education have created methodological guidelines for comprehensive sex education, so the basic health team must be prepared to carry them out.
Objective: to identify the knowledge that family doctors who provide services in primary care have on sexual and reproductive health in adolescents/youth.
Method: descriptive, longitudinal and retrospective study with a quantitative- qualitative approach developed at the Luis Augusto Turcios Lima Polyclinic , San José de las Lajas municipality. Mayabeque, during March - May 2018. With a sample of 14 young doctors who carry out care work in family medical offices. Primary source of data collection: survey.
Results: 86% Doctors with stable partners (92%), between 24-26 years of age (57%) with inadequate knowledge about the ages of youth (79%), with wrong concepts and opinions about them (79 and 71% respectively), with inadequate responses about the factors that contribute to the increase in maternity and sexually transmitted infections (86%) and those that cause problems in sexual and reproductive health as well as strategies to reduce them (86 and 57%), the level obtained was low: 79%.
Conclusions: Primary care physicians require interdisciplinary preparation with a social, pedagogical, philosophical and psychological approach that equips them with skills to work on sexuality in adolescents and young people.
Introduction
Adolescence and youth have traditionally been defined as transition ages between childhood and adulthood. Adolescence in particular has been called the period of puberty, which refers to the age at which male or pubic hair appears. This denomination emphasizes what distinguishes adolescence as a stage of the life cycle, a set of biological changes that prepare the subject for procreation. Currently there is consensus in considering adolescence and youth as key moments in the individual's socialization process [1,2].
Adolescence and youth, like the other stages of the life cycle of human development, constitute above all "psychological ages", since we start by considering development as a process that does not occur automatically or fatally determined by the maturation of the child. organism, but above all it has a socio-historical determination, according to the position of LS Vygotsky [ 3-5].
In the STI-HIV/AIDS prevention work, adolescents are considered a vulnerable population, since they are in a stage of their life of discovery and activation of sexual exchange. If you are not educated to assume a responsible sexuality, you can engage in sexual behaviors that damage your health, among which we can mention: starting an early sexual life, having many sexual partners or having a sexual partner who has many sexual partners, having occasional sexual relations with unknown partners, not using a condom or condom during sex, continuing to have sex despite having STI symptoms and not telling sexual partners, and both needing treatment [6].
From this approach, it is considered that as knowledge about risk factors advances, which allows defining preventive actions, damage to health will occur less frequently, guaranteeing the well-being of society in the future [7].
Educational guidance presents different modalities, and although there is no single consent in relation to their content, the following are proposed in the specialized literature: Personal Guidance, School Guidance and Professional Guidance [7].
In the stage of adolescence, there is an expansion of the activity and communication systems that determines the emergence of a set of psychological peculiarities characteristic of this period [8].
As fundamental achievements of personality development, the emergence of theoretical thinking and a more active cognitive attitude towards knowledge of reality can be pointed out , which together with the development of complex motivational formations such as self-worth, ideals and professional motivation , leads to a more conscious and effective regulation of behavior. Special progress occurs in the moral sphere, even without the presence of a conception of the world, a typical formation of youth [9].
Within the national health system (SNS) in the decade of the 80s of the 20th century, a new type of specialist in Comprehensive General Medicine (MGI) emerged in Cuba, inserted in primary health care and within the work functions is promoting health in the community, family, and people it serves. In the improvement of primary health care, the prioritized program of maternal and child care arises, and in the year 2000 the national program of Comprehensive health care in adolescence was approved and implemented [10].
The family doctor and nurse with the basic work group must be in charge of carrying out the activities included in the program. Its fundamental purpose is aimed at training increasingly healthy people, who assume positive behaviors with foresight, discipline and responsibility towards health and its care [10-12].
If the potentialities of the SNS are considered at the present time and the need to approach health problems from an epidemiological-preventive and social perspective that breaks the circle of approaching health from its curative-assistance paradigm in the care of the adolescent population , it is essential to promote promotional work with this group in the prevention of STIs-HIV/AIDS [13-16].
This research was carried out with the aim of Identify the knowledge that family doctors who provide services in primary care have on sexual and reproductive health in adolescents/youth.
A descriptive, longitudinal and retrospective observational study was carried out with a quantitative-qualitative study, developed at the Luis Augusto Turcios Lima Polyclinic, San José de las Lajas municipality. Mayabeque, during March - May 2018. Universe made up of 15 young doctors who carry out care work in family medical offices and with a sample of 14.
Inclusion criteria:
- All general practitioners and MGI specialists who provide assistance in the family medical offices of the Luis Augusto Turcios Lima Polyclinic aged up to 30 years.
- Willingness to participate in the study.
Exclusion criteria.
• MGI who work in administrative positions.
• Express desire to refuse to participate in the study.
• MGI that are not providing assistance at the time of applying the questionnaire.
The distribution was as follows:
- Comprehensive general medicine specialist: 4
- 2nd year resident: 1
- 1st year resident: 9
About obtaining the information:
As the quantitative approach is involved, a structured research design is carried out, with the nature of numerical data, which was collected through an instrument: a questionnaire created for this purpose and statistical analysis.
Each correct answer was given 2 points and the level obtained was finally declared according to the following range:
High: Yes answers 10-8 questions adequately: 20-16 points.
Medium: Yes answers 7-5 questions adequately: 14-10 points.
Low: Yes answers 4 or fewer questions adequately: 8 or fewer points.
The qualitative approach was based on describing, understanding and interpreting the phenomena, through the perceptions and meanings produced by the experiences of the participants.
Techniques such as observation (with the use of an observation guide) and semi- structured interviews (with opinion questions and about knowledge) were fundamentally used, since it was considered a tool that retrieves information in a context of closeness and intimacy with the informants (Annex 2). The registration process to preserve the information offered was carried out through notes and recordings.
This union of both approaches allowed to delve into the investigated topic 17
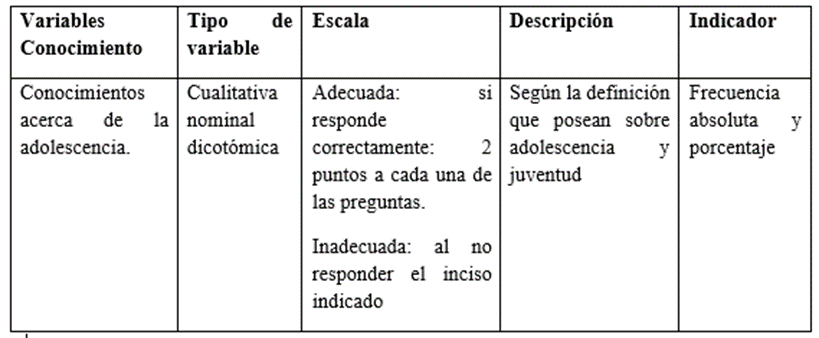
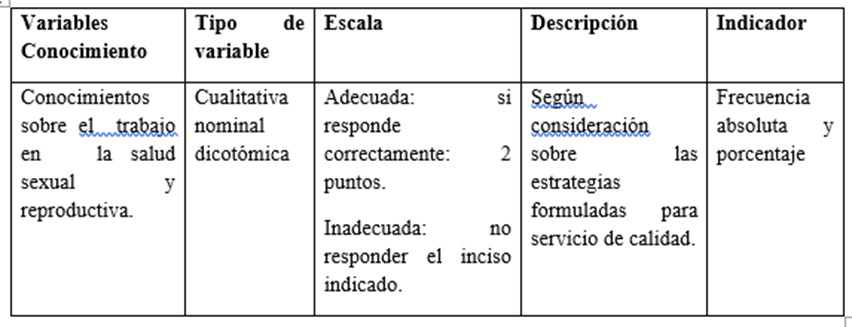
Operationalization of Variables
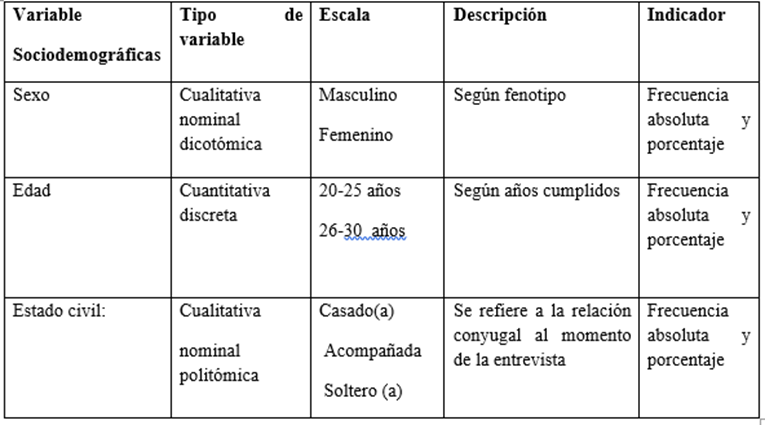
Ethical aspects: communication to the scientific council of the institution. Non-disclosure and confidentiality of the names of the physicians involved in the study. The data is used for scientific purposes, presentation at events and publication.
Data processing and statistics: Use of Microsoft Excel Office 2007 database. Use of descriptive statistics elements: calculation of absolute frequency (AF) and relative ( %) and inferential statistics: Chi Square through the use of the program for epidemiological data analysis. tabulated, version 3.1 (EPIDAT). The results are expressed in tables.
Results
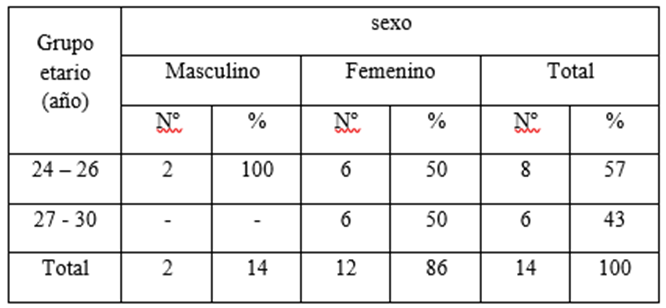
It is observed that 86
Discussion
Discussion of the results.
Analyzing the sociodemographic characteristics of the universe studied, it can be seen that they correspond to the current definition given by the Center for Youth Studies, which defines that: "From the Cuban perspective, youth is a historical category produced socially, it designates the human group in training and development with common sociodemographic traits, which is defined according to their belonging to the social structure. It includes people between 15 and 30 years of age, the time of life in which socio-psychological maturation occurs. It stands out for establishing its own social relationships that configure the youth condition in correspondence with the specific qualities of the stage, forming the recognized youth identity, both by those involved, and by society” [18,19].
We appreciate that the strategy of the Cuban State aimed at promoting their social insertion through work activity is fulfilled; seen not only as a means and guarantee of individual life, but as a real possibility of economic participation and, in a general sense, in the process of building a socialist society [20].
It correlates with studies that report that the country's occupational and category structure corresponds to female youth [21,22].
The high presence of the female sex in the health sector responds to the multidimensionality of the gender approach, considering this as a category that encompasses, in addition to the biological, the socio-psycho- economy - political -cultural category . However, it is shown how Cuba maintains compliance with the United Nations Millennium Goals, in terms of access to education and gender equality [22-25].
When questioning young doctors about the ages framed, youth is not defined, responding fundamentally between 18-24 years of age. This is not the case when asking about the ages at which adolescence is found, since it is well established. During the interview (79 %) adolescents are framed according to biological and psychological changes, considering this stage as a period of crisis.
The opinion about this stage of life is wrongly conceived and distorted, which in turn transforms the possible actions or points of view when working with them.
They do not know that adolescence and youth are considered as "psychological ages", that they have a historical-social determination, according to LS Vygotski, creator of the Historical-Cultural Approach and that according to this approach I. to take into account in the characterization of these stages the "natural line of development", referring fundamentally to the processes of physical maturity and the "social line of development", which includes the peculiarities of the socialization process, including the "position social” that adolescents and young people occupy as evolutionary groups [4,5].
This alternative allows us to evaluate the internal and external conditions of human psychological development, in their dialectical interrelation, and not conceive it as a result of biological maturation or as a linear product of the individual's socialization process. Psychological development goes through regularities in each period that are typical of it, but it is expressed, in a unique and unrepeatable way, in each particular subject. Psychological development is a process that occurs in leaps, and is directed towards new levels of self-determination of the subject, but contains its historicity [4].
During the interview, it was appreciated that 100% see adolescents as a vulnerable risk group where complicated pregnancies, delinquency, drug addiction, school dropouts and dangerous gangs occur, that is, a generalized perception occurs from these symptomatic and problematic poles with an approach based on disease and specific problems. Yes, she is very clear about the repercussions of STIs and early pregnancy in a high percentage .
Similarly, in 92%, they have adequate knowledge about concepts of interpersonal communication, gender and self-esteem but recognize that this is not all to educate and carry out promotion, they confess few skills and attitudes to carry them out.
They recognize that they do not have the tools to carry out educational-preventive work in this population, and even less so within the framework of the socializing space of the school, so they do not feel suitable [24-26].
I agree that it corresponds to not knowing social communication in health or participatory techniques specifically in adolescents [27,28].
Although they know the definition of gender and autonomy, they do not know how to work with a gender approach and sexual rights in adolescence, they maintain the survival of theories and social practices that, supported by medicine, among others, promote adultcentrism [30].
The analysis of knowledge about SRH in adolescents and young people in primary care physicians who are in charge of educational intervention projects, reflects the difficulty in social insertion [31].
This difficulty encompasses both pre-employment socialization and organizational socialization. The first prepares them for incorporation into the life of society through work and participation in community affairs and in organizational socialization that manages the learning of the contents and processes that a person requires to adjust to a role. specific to the organization, implies appropriating the specific requirements of the job and the culture [23].
When faced with concerns that an adolescent might present, they are referred to a psychologist, gynecologist or other specialist, they do not have adolescent circles configured and promotion would be left on another plane.
In a high percentage (80%) they present a broad concept of work because they feel that it encompasses dimensions beyond instrumental rationality, they do not see it only as an instrumental production of use values, but as a means of social solidarity and personal self-realization.
Conclusions
- The majority of women provide services in the Family Physicians' Offices, with a stable union and ages between 24-26 years.
- Misconceptions and opinions about adolescents, strategies to reduce sexual and reproductive health problems and the essential points to be observed when working with them.
- Low perception of being able to work with them in a socialization space such as school.
- The level of knowledge about sexual and reproductive health in adolescents and young people was low.
Recommendation
Primary care physicians are expected to carry out educational intervention activities in adolescents in their different socialization spaces, so they should be provided with theoretical and methodological tools, both in undergraduate and postgraduate courses, contributing to favor the process of labor socialization.
References
- Cruz Sánchez F, Rodríguez Alonso B, Alonso Uría RU Childcare in adolescence. Havana: Ministry of Public Health; 2014; p. 15,16. ISBN:978-959-283-108-7
View at Publisher | View at Google Scholar - Mota J. Bringers of fire. Rev ADOLECA. 2017: 13-18. ISBN: 978-959-7005-97-1
View at Publisher | View at Google Scholar - Vigostki l S. Imagination in children and adolescents in imagination and creation in childhood. 2nd ed: Editorial people and education, p. 27-34; 1999.ISBN 959-13-0710-1
View at Publisher | View at Google Scholar - Domínguez L. Developmental psychology, Adolescence and youth, Reading Selection. Havana, Cuba: Ecimed ; 2006.
View at Publisher | View at Google Scholar - Kon I. Psychology of the Juvenile Age. Havana: People and Education; 1990.
View at Publisher | View at Google Scholar - Santillano Cárdenas I. Comprehensive education of sexuality in childhood, adolescence and youth. conceptual approach. In Guerrero Borrego N. Reflections and views on sexuality in childhood, adolescence and youth. Havana: CENESEX; 2016. p 45. ISBN: 978-959-7187-86-8
View at Publisher | View at Google Scholar - Cruz Sánchez F., et al. Adolescence. Pediatrics, Havana: Medical Sciences; 2011; T.VII
View at Publisher | View at Google Scholar - Álvarez Mesa MI, Domínguez Gómez J, Torre Navarro LM Factors related to the spread of sexually transmitted infections in adolescence. Rev they had science medical [Internet]. 2014 Apr [cited 2017 Jul 5]; 13(2).
View at Publisher | View at Google Scholar - Borrás T. Adolescence: definition, vulnerability and opportunity [online]. Havana; June 11, 2014 [Accessed: July 7, 2017].
View at Publisher | View at Google Scholar - Family doctor and nurse program. Ministry of Public Health. Medical Sciences. Havana; 2011
View at Publisher | View at Google Scholar - National Program for Maternal and Child Care. Ministry of Public Health. Cuban Health Portal; 1999
View at Publisher | View at Google Scholar - Public Health Functions
View at Publisher | View at Google Scholar - Cruz Sánchez F, Rodríguez Alonso B, Alonso Urìa RU Childcare in adolescence. Havana: Ministry of Public Health; 2014; p. 15,16. ISBN:978-959-283
View at Publisher | View at Google Scholar - Rodríguez Alonso B, Solernau Mesa IA, Hernández Salas G, Martínez Ramos M, Ravlo Elvirez M. Health promotion and self-care. In: Childcare in adolescence. Ministry of Public Health. Havana; 2014; p.152-153. ISBN: 978-959-283-108-7
View at Publisher | View at Google Scholar - Ministry of Public Health. National Program. Methodological Manual. STD/HIV/AIDS Prevention Work. Havana: National Center for the Prevention of STIs/HIV/AIDS. MINSAP; 2009.
View at Publisher | View at Google Scholar - Chacón O'farrill D, Cortés Alfaro A, Álvarez García AG, Sotonavarro Gómez Y. Pregnancy in adolescence, its impact on family and society. Rev Cuban obstetric Ginecol [Internet magazine]. 2015 [cited 2017 Nov 6]; 41(1): 50-58.
View at Publisher | View at Google Scholar - Hernández Sampieri R, Fernández-Collado C, Baptita Lucio P. Research methodology. 6th edition. Mexico: Editorial McGraw-Hill Inter-American; 2014
View at Publisher | View at Google Scholar - Bonvillani A. Some clues to think about youth as an analytical category in investigative processes. Rev. Study. 2016: 21. ISSN: 1684 6842
View at Publisher | View at Google Scholar - Domínguez García L. Future projects in young Cubans. a look from the cultural historical approach. Rev. ADOLECA. 2017: 120–131. ISBN: 978-959-7005-97-1
View at Publisher | View at Google Scholar - Castro Espin M, Rivero Pino R. Government responsibility and comprehensive sexuality education in Cuba. Havana: CENESEX, 2015.ISBN:978-959-7187-72-1
View at Publisher | View at Google Scholar - Health Statistical Yearbook 2012. Republic of Cuba. National Directorate of Medical Records and Health Statistics. [Internet]. April 2012. MINSAP. Havana. (ISSN: 1561-4425). [ cited 2017 Jul 2].
View at Publisher | View at Google Scholar - Moreno Fernández YL, Vidal Valdez JR, Nápoles Fernández M L: Rebel Youth: towards journalistic content management with greater emphasis on adolescents and young people. Rev. Study 2016:21. ISSN: 1684 6842
View at Publisher | View at Google Scholar - Weekt Trutie R, Pulgaron Garzòn Y. Adolescents and youth: Challenges and possibilities in the global development agenda. Proceedings of the international congress of researchers on youth. Rev. Non-special Study ISSN 1684-6842, 2016
View at Publisher | View at Google Scholar - Dominguez Garcia MI. Youth and education in Cuba: Strategy for female social inclusion. Cuban Studies. 2011;42(1 ): [ approx. 19 p.].
View at Publisher | View at Google Scholar - González Y, Morejón O, Morejón Y, Sevilla G. The school: a link in health promotion on the HIV epidemic. Conrado [online] July 2015 [Accessed: July 08, 2017]; 11 (48).
View at Publisher | View at Google Scholar - Ortiz N, Rodríguez D, Vázquez M, Álvarez M, Sánchez L. Educational intervention on sexually transmitted infections in adolescents. 2015 [Accessed: August 12, 2017].
View at Publisher | View at Google Scholar - Benavides K, Alfaro DP Didactic mediation strategies for education on sexually transmitted infections in adolescents. Rev. Current Nursing in Costa Rica. [Internet] 2016. [cited 2017 Jul 3]
View at Publisher | View at Google Scholar - Fonseca Robles N, Mujica Utrera E, Álvarez Martínez J. Participatory techniques for work on HIV/AIDS. Havana, 2009
View at Publisher | View at Google Scholar - Bermúdez Gonzales Ma. M, Chalgub Moreno A. Ma., Sala Adam Ma. R, Cruz Sánchez F, Reyea Pairol R S. Social communication tools in sexual and reproductive health for working with adolescents. Cuba: Editorial Molinos Trades S.A; 2011
View at Publisher | View at Google Scholar - Torres Cueto, MA et al. Sexuality education and prevention of STDs and HIV/AIDS from gender, rights and sociocultural approaches. Secondary basic, pre-university, vocational and adult secondary education. Havana: Ministry of Education. [Internet] 2011. [cited 2017 Jul 17].
View at Publisher | View at Google Scholar - Luis Luis M J. Analysis of the labor disengagement of young people in Cuba during the period from 2000 to 2008. Master's thesis. 2009. CESJ Diploma CD. 4th-5th edition ISBN 978-959-311-134-8
View at Publisher | View at Google Scholar
