

Case Report | DOI: https://doi.org/10.31579/2835-2882/046
Intraoperative Findings Heterotopic Ossification of the Mesentery. Case Report and Literature Review
- Vélez-Cuorvo Luis Fernando 1
- Ruíz-Pineda Juan Pablo 2
- Díaz-Castillo José Alejandro 3*
- Solano-Perdomo Francisco 3
- Morales-Espinoza Fabio Andrés 4
1 Physician, General Surgeon, Specialist in University Teaching; Associate Instructor Faculty of Medicine. Sanitas University Foundation. Bogotá DC Colombia.
2 Physician, General Surgeon, Master in University Teaching; Associate Instructor Faculty of Medicine. Sanitas University Foundation. Bogotá DC Colombia.
3 Physician, General Surgery Resident. Sanitas University Foundation. Bogotá DC Colombia
4 General practitioner. Reina Sofia Clinic General Surgery Service. Bogotá DC Colombia.
*Corresponding Author: Díaz-Castillo José Alejandro, Physician, General Surgery Resident. Sanitas University Foundation. Bogotá DC Colombia.
Citation: Luis Fernando VC, Juan Pablo RP, Díaz-Castillo José Alejandro CE, Solano P. Francisco, Fabio Andrés ME., (2024), Intraoperative Findings. Heterotopic Ossification of the Mesentery. Case Report and Literature Review, Clinical Research and Studies, 3(3); DOI:10.31579/2835-2882/046
Copyright: © 2024, Díaz-Castillo José Alejandro. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 March 2024 | Accepted: 18 March 2024 | Published: 14 June 2024
Keywords: general surgery; heterotopic ossification; tissue bone; mesentery; osteoblasts
Abstract
Introduction: Heterotopic ossification of the mesentery is a rare condition in which there is bone formation in tissues that normally do not ossify. In the field of general surgery, it is common to encounter this intraoperative finding incidentally. The etiological and pathophysiological mechanism that leads to overstimulation of osteoblastic activity has not yet been established.
Clinical Case: We present a case of a 41-year-old patient with a surgical history of perforated appendicitis one year ago, who required right hemicolectomy + colostomy, was admitted for colostomy closure with intraoperative findings of multisegmental bony mass.
Discussion: According to the literature, the incidence of heterotopic ossification of the mesentery is unknown and it is associated with a wide age range. Despite its association with surgical history, which generally induces a proinflammatory state in the mesentery, leading to the formation of ectopic bone tissue, the surgical indications are currently mainly secondary causes such as peritonitis, and therefore, these findings are usually incidental intraoperative discoveries, as in the presented case report.
Conclusion: heterotopic ossification of the mesentery is a rare condition that involves an inflammatory process where the presence of osteoblasts is described by theories. It often poses a challenge for the surgeon, considering that it is associated with an incidental intraoperative finding.
Introduction
Tumors of the mesentery are subdivided into 2: primary tumors, which are derived from the mesenchyme and usually present a benign behavior, and secondary tumors that usually originate as an extension of another neoplastic process, either due to contiguity or hematogenous/lymphatic dissemination. Among the primary lesions, extragastrointestinal stromal tumors (EGIST), desmoid tumors, mesenteric lymphoma, mesenteric calcifications, mucinous neoplasms, among others, are described. (1,2)
Heterotopic ossification of the mesentery, also known as myositis ossificans, is a rare and benign pathology in which there is bone formation in tissues that do not normally ossify, generally soft tissues (3) . It has an unknown incidence. The cause of ossification is not yet completely established, but it has been associated with trauma, ischemia and intra-abdominal surgeries which are causes of inflammation (4,5) . It is usually an incidental finding in the surgical approach of patients with abdominal pain; The image of choice is total abdominal computed tomography, which is the imaging modality for the evaluation of mesenteric masses (1) . The clinical case of a patient with heterotopic ossification of the mesentery as an incidental surgical finding is described, with the aim of expanding the understanding of this rare pathology.
Clinical case
A 41-year-old male patient with no associated comorbidities, a history of hospitalization 1 year ago in the context of acute perforated appendicitis, who was taken to exploratory laparotomy, intraoperative findings of an appendicular plastron for which he required right hemicolectomy + colostomy. He was admitted with a plan for colostomy closure, for which contrast-enhanced computed tomography of the abdomen was performed as surgical planning in which there was evidence of a hyperdense image in the mesentery (figure 1) for which he was taken to a surgical procedure with intraoperative findings of foreign body extraction. retroperitoneal + severe adhesion process + multisegmental bone mass adherent to the mesentery (figure 2) without perforation of intestinal loops. Bone mass is removed and taken to pathology.

Figure 1: Contrast-enhanced computed tomography of the abdomen with evidence of hyperdense tissue suggestive of bone in the mesentery: On the left (coronal section) the arrow points to a hyperdense image in the root of the mesentery suggestive of bone formation. On the right (axial section) the arrow points to evidence of a hyperdense foreign body suggestive of bone. Source: Images captured by the authors.
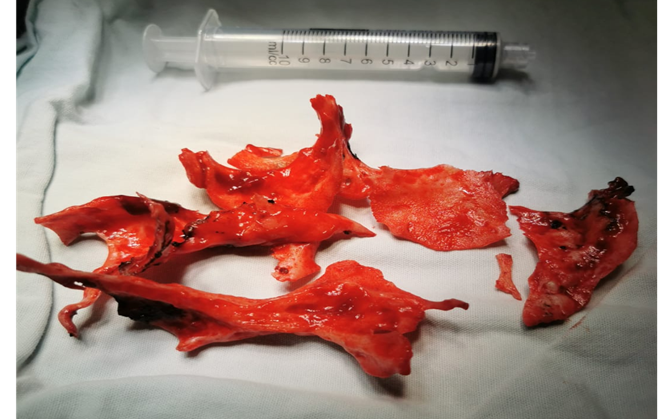
Figure 2: Surgical specimen: Intraoperative findings sent to pathology, multisegmental bone mass. Source: Photograph taken by the authors.
Discussion
Heterotopic ossification of the mesentery was described for the first time in 1883 by Ridel as a complication of a patient with spinal cord trauma (3) ; The first article published on mesenteric ossifying myositis in 1901, which was related to soldiers who presented spinal cord trauma as a result of participating in the First World War (6) . Throughout history, this pathology has received a variety of names such as intra-abdominal myositis ossificans, ossifying mesenteritis, among others (6,7) , but Wilson was the one who named this condition as heterotopic ossification of the mesentery in 1999 (3)
Despite being a rare condition in which its incidence is unknown, the literature describes a wide range of ages at presentation, ranging from 22 to 80 years with the main association between men between 40 and 80 years of age (4,8)., different from the etiology of the calcifying fibrous tumor which is usually more common in women from 4 to 20 years of age (9). It is usually associated with previous traumatic injuries, a history of intra-abdominal surgeries (4,10); By 2020, 73 cases of heterotopic ossification of the mesentery had been described (4).
Clinically, heterotopic ossification of the mesentery can occur in the context of abdominal pain; however, cases of patients with intestinal obstruction or enterocutaneous fistula have been described (4). Usually, the time elapsed between the abdominal trauma and the surgical procedure is usually between 2 to 4 weeks, extending up to 7 years, which is why it is usually an incidental finding in an abdominal surgical procedure (4,11).
Heterotopic ossification has histologically referred to calcium deposits composed of osteoblasts and covered with layers of structured bone (3,12); Macroscopically, it has been described as a white, rubbery grayish-whitish lesion (13). The main theory consists of the formation of reactive bone in mesenteric adipose tissue due to multiple stimuli such as ischemia, edema, trauma associated with inflammation (11) as a common condition which stimulates morphogenic bone proteins which are related to multifunctional cytokines that stimulate stimulating growth factor β and thus overstimulate osteoblast activity through the RANK pathway and its ligand RANKL (4,14).
According to the literature, there are 4 factors that have a significant influence on the pathogenesis of ectopic bone formation in the mesentery (3); First, a trigger that causes inflammation, second, cellular signaling at the site of injury through proinflammatory cytokines, third, the presence of mesenchymal cells with the potential for cell differentiation into chondroblasts and osteoblasts, and finally, an environment and context that allows bone formation. ectopic (3,7,14). As described by McCarthy, ossification can occur in 5 clinical contexts, which are: genetic predisposition, after trauma, neurogenic, post-surgical, and as a consequence of reactive joint injuries (15)
It is worth mentioning that heterotopic ossification of the mesentery has not been associated with metabolic alterations such as calcium, phosphorus or magnesium disorders (15).
After clinical suspicion, triphasic bone scintigraphy with radionuclides was determined as the image of choice in an early phase; however, computed tomography of the abdomen is considered the image of choice for the evaluation of mesenteric masses and their origin (1) in order to to evaluate the origin and its relationships (16) , where in the context of heterotopic intestinal ossification they can report dense and irregular calcified shadows, diffuse focal fatty opacification of the mesentery with evidence of calcified densities, among others (4) , however the radiological differentiation between bone neoplasms, contrast leak, foreign material, osteosarcoma can be difficult to interpret on tomography (4,10) .
The literature describes that in asymptomatic patients’ observation and follow-up with contrasted images can be considered given that when surgically intervening, heterotopic ossification can recur and require multiple surgeries (10).
The indication for surgery is usually a secondary cause such as generalized peritonitis, acute abdomen, intestinal obstruction in a symptomatic patient (3,10).
Prophylactic management with non-steroidal anti-inflammatory drugs, bisphosphonates and even radiotherapy after the surgical procedure has been described in order to prevent the recurrence of ossification; however, there are still no statistically significant studies that verify their use (3,8).
The prognosis is favorable so far with no evidence of malignant potential (3).
In the case presented, the history of previous surgical pathology associated with the inflammatory process of the mesentery and subsequent incidental intraoperative findings consisting of bone mass which had no relationship with the intestine is related.
Conclusion
Heterotopic ossification of the mesentery is the generally benign neoformation of bone tissue in tissues that do not normally ossify; As it is a rare pathology, its incidence is not described and is related to a wide age range; It is associated with a history of intra-abdominal surgery, which conditions an inflammatory process where theories describe the presence of osteoblasts and their activity through the RANK - RANKL pathway. Currently, surgical indications are usually secondary causes such as peritonitis, which is why they are generally incidental intraoperative findings, which generates a challenge for the general surgeon, as we describe in the case report presented.
Ethical considerations:
Informed consent: This article has the informed consent of the patient for the review of their clinical history and the use of their diagnostic images, always protecting their identity and adhering to resolution 008430 of 1993 of the Ministry of Health of Colombia.
Conflict of interest:
The authors declared that they have no conflicts of interest.
Funding sources:
No funding was obtained to carry out this study.
Use of information and communications technologies:
The Paperpile application was used as ICT to involve Vancouver-style bibliographies references.
Authors' contribution
Conception and design of the study: Vélez-Cuorvo Luis Fernando, Ruíz-Pineda Juan Pablo
Acquisition of data: Diaz-Castillo Jose Alexander, Solano-Perdomo Francisco Data analysis and interpretation: Velez-Cuorvo Luis Fernando, Diaz-Castillo Jose Alexander, Solano-Perdomo Francis
Drafting of the manuscript: Diaz-Castillo Jose Alexander, Solano-Perdomo Francis, Morales-Spinoza Fabio Andrew
Critical review: Velez-Cuorvo Luis Fernando, Ruiz-Pineda John Paul
References
- Riquelme F, Vega L, O'Brien A. (2009). Mesenteric masses: evaluation by computed tomography. Chilean magazine of radiology [Internet]. 15(4):165–173.
View at Publisher | View at Google Scholar - Facundo H, Rodríguez C. (2014). Mucinous cystic neoplasia of the mesentery: case presentation and review of the literature. Colombian Journal of Cancerology 1;18(4):197–201.
View at Publisher | View at Google Scholar - Ferreira C, Gomes C, Melo A, Tenreiro N, Pinto B, et al. (2017). Heterotopic mesenteric and abdominal wall ossification - Two case reports in one institution. Int J Surg Case Rep 837:22–25.
View at Publisher | View at Google Scholar - Althaqafi RMM, Assiri SA, Aloufi RA, Althobaiti F, Althobaiti B, et al. (2021). A case report and literature review of heterotopic mesenteric ossification. Int J Surg Case Rep 82:105905.
View at Publisher | View at Google Scholar - Rodríguez Zarco E, Vallejo Benítez A, de Soto Cardenal B, Mora Cabezas M, Pereira Gallardo S. (2016). [Calcifying fibrous tumor of the small bowel]. Cir Esp 94(4):245–247.
View at Publisher | View at Google Scholar - González Q, Bahena-Aponte J, Lezama de Luna J, Ramírez-Avilés E. (2011). Dystrophic bone metaplasia in the mesentery of the small intestine in a patient with multiple abdominal surgeries. Report of a case. Rev Gastroenterol Mex. 76(03):251–254.
View at Publisher | View at Google Scholar - Zhou J, Zhou L, Wu S, Li R, Yang X, et al. (2019). Clinicopathologic Study of Calcifying Fibrous Tumor Emphasizing Different Anatomical Distribution and Favorable Prognosis. Biomed Res Int 5026860.
View at Publisher | View at Google Scholar - Herrera-Toro N, Mejía-Sarasti FJ. (2016). Heterotopic mesenteric ossification in a child: case report. Iatreia
View at Publisher | View at Google Scholar - Chorti A, Papavramidis TS, Michalopoulos A. (2016). Calcifying Fibrous Tumor: Review of 157 Patients Reported in International Literature. Medicine 95(20)
View at Publisher | View at Google Scholar - Hicks CW, Velopulos CG, Sacks JM. (2014). Mesenteric calcification following abdominal stab wound. Int J Surg Case Rep 11;5(8):476–479.
View at Publisher | View at Google Scholar - Zamolyi RQ, Souza P, Nascimento AG, Unni KK. (2006). Intraabdominal myositis ossificans: a report of 9 new cases. Int J Surg Pathol 14(1):37–41.
View at Publisher | View at Google Scholar - Myers MA, Minton JP. (1989). Heterotopic ossification within the small-bowel mesentery. Arch Surg 124(8):982–983.
View at Publisher | View at Google Scholar - Correa S, Gómez PC, Mugnier J, Salamanca E, Sebá JE. (2019). Calcified fibrous pseudotumor of the mesentery: an unusual case in a 9-year-old girl. Cir pediatric 154–157.
View at Publisher | View at Google Scholar - Cooper GM, Hausman RE. (2014). The cell [Internet]. Madrid: Marban
View at Publisher | View at Google Scholar - McCarthy EF, Sundaram M. (2005). Heterotopic ossification: a review. Skeletal Radiol 34(10):609–619.
View at Publisher | View at Google Scholar - Muñoz-Pérez DF, Rodríguez-Flórez RJ. (2022). Giant mesenteric cyst as a simulator of ascites: case report and review of the literature. Rev Colomb Cir. 37:689-694.
View at Publisher | View at Google Scholar
