

Case Report | DOI: https://doi.org/10.31579/2834-796X/015
Intracranial Vascular Abnormalities in Myxoma: Regarding a Case, and a Literature Review
- L. Bencherif *
- C. Guidoux
- M.C. Henry Feugeas
Stroke Center, Bichat-Claude-Bernard Hospital, Paris France.
*Corresponding Author: L. Bencherif, Stroke Center, Bichat-Claude-Bernard Hospital, Paris France.
Citation: L. Bencherif, C. Guidoux, M.C. Henry Feugeas (2023), Intracranial Vascular Abnormalities in Myxoma: Regarding a Case, and a Literature Review. International Journal of Cardiovascular Medicine, 2(1); DOI:10.31579/2834-796X/015
Copyright: © 2023, L. Bencherif. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 February 2023 | Accepted: 24 February 2023 | Published: 28 February 2023
Keywords: myxoma; microbleeds; cerebral microanevrysms
Abstract
Myxoma is an intracardiac tumor that can lead to neurological complications, especially intracranial artery abnormalities. We report a patient's case, and we discuss the main neurological complications of myxoma.
We report the case of a 52-year-old patient who suddenly exhibited dysarthria and regressive left lower limb paresis within a few hours. A brain MRI revealed multiple bithalamic and left frontal subcortical ischemic strokes (IS) visible in diffusion and flair (Figure 1). Time-of-flight MRA did not reveal any noticeable abnormalities of the intracranial arteries.
Myxoma can be complicated by IS, related to emboli of tumor fragments. Secondary cerebral aneurysms secondary to myxoma are rarer. They can occur post-surgery. Such aneurysms are generally multiple and fusiform in 91% of cases, and more rarely saccular.
Introduction:
Myxoma is an intracardiac tumor that can lead to neurological complications, especially intracranial artery abnormalities. We report a patient's case, and we discuss the main neurological complications of myxoma.
Method:
We report the case of a 52-year-old patient who suddenly exhibited dysarthria and regressive left lower limb paresis within a few hours. A brain MRI revealed multiple bithalamic and left frontal subcortical ischemic strokes (IS) visible in diffusion and flair (Figure 1).
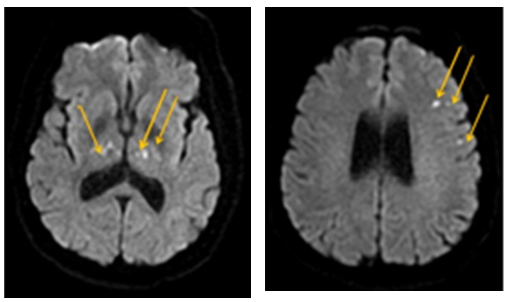
Time-of-flight MRA did not reveal any noticeable abnormalities of the intracranial arteries.
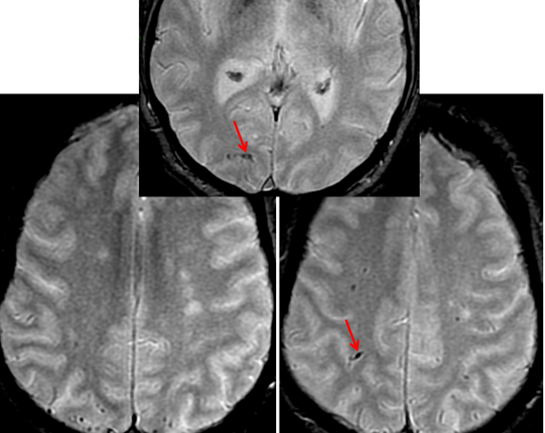
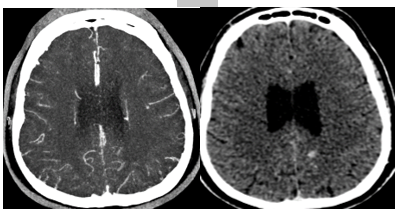
The T2* sequence revealed numerous small spots in hyposignal, of the microbleeds type, but atypical by their location mainly in the posterior subarachnoid spaces (Figure 2), suggesting the presence of distal cerebral microaneurysms. Cerebral angiography revealed a small distal aneurysm of the left anterior cerebral artery associated with contrast imaging late after injection (Figure 3).
Cardiac ultrasound (transthoracic and transesophageal) revealed a voluminous left intra-auricular myxoma that was very mobile and prolapsing through the mitral valve without mitral leakage. Surgical treatment was carried out, consisting of removal of the myxoma and repair of the wall of the left atrium and the mitral ring. The postoperative follow-up was straightforward and favorable.
Discussion:
Myxoma can be complicated by IS, related to emboli of tumor fragments. Secondary cerebral aneurysms secondary to myxoma are rarer. They can occur post-surgery [1]. Such aneurysms are generally multiple and fusiform in 91% of cases, and more rarely saccular. [2]
They can be very small, as seen on T2*, thus requiring use of cerebral arteriography, which remains the reference examination for their identification. Their pathophysiology is debatable and is most often attributed to metastases of fragments of myxoma resulting in weakening of the vessel walls. This leads to impairment of the elasticity and then dilation of the vessel giving rise to the aneurysm presentation. Therapeutic management consists mainly of resection of cardiac myxoma [3]. Coil embolization of fusiform myxoma aneurysms rarely leads to a satisfactory result [4].
Conclusion:
Identification of a cardiac myxoma involves performing both parenchymal and vascular brain imaging to search for aneurysmal complications. In this pathology, as in endocarditis (Klein 2007), T2* imaging appears to hold promise for detecting patients at risk of brain bleeding or tumor aneurysm (Klein 2007, Sato 2016).
References
- Qingsheng Xu, Xiaobing Zhang, Pan Wu, Ming Wang, Yongqing Zhou, Yiping Feng, Multiple intracranial aneurysms followed left atrial myxoma: case report and literature review. Department of Neurosurgery Thorac Dis. 2013;5(6):E227-E231.
View at Publisher | View at Google Scholar - Sabolek M, Bachus-Banaschak K, Bachus R, et al. Cerebral multiple. Aneurysms as delayed complication of left cardiac myxoma: a case report and review. Acta Neurol Scand 2005;111:345-350
View at Publisher | View at Google Scholar - Roeltgen DP, Weimer GR, Patterson LF. Delayed Neurologic complications of left atrial myxoma. Neurology 1981;31:8-13
View at Publisher | View at Google Scholar - Yilmaz MB, Akin Y, Güray U, et al. Late recurrence of left atrial myxoma with multiple intracranial aneurysms. Int J Cardiol 2003;87:303-305
View at Publisher | View at Google Scholar
