

Research Article | DOI: https://doi.org/10.31579/2834-8664/066
"Intra-abdominal abscess, a simulating tumour"
1st and 2nd Degree Specialist in Internal Medicine 2nd Degree Specialist in Natural and Traditional Medicine Master's Degree in Natural Medicine and Bioenergetics Master's Degree in Hyperbaric and Underwater Medicine, Assistant Professor, Assistant Researcher, Hospital Docent Clinic Quarrion ̈Dr. Salvador Allende, Calzada del Cerro No. 1551. Havana, Cuba.
Hospital Docente Clínico Quirúrgico ̈Dr. Salvador Allende ̈ Calzada del Cerro No. 1551. Havana, Cuba. 6th year medical student.
*Corresponding Author: Dr Rodolfo Suárez Iznaga, 1st and 2nd Degree Specialist in Internal Medicine 2nd Degree Specialist in Natural and Traditional Medicine Master's Degree in Natural Medicine and Bioenergetics Master's Degree in Hyperbaric and Underwater Medicine, Assistant P
Citation: Dr Rodolfo Suárez Iznaga., Piquet Cancio World., (2024). "Intra-abdominal abscess, a simulating tumour", International Journal of clinical and Medical Case Reports.3(6); Doi:10.31579/2834-8664/066.
Copyright: © 2024, Dr Rodolfo Suárez Iznaga, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 November 2024 | Accepted: 19 November 2024 | Published: 29 November 2024
Keywords: intra-abdominal abscess
Abstract
An intra-abdominal abscess is a collection of pus in the abdomen that is surrounded by inflamed, encapsulated tissue. Intra-abdominal abscesses have a mortality rate of 10 to 40%. A 68-year-old patient presented to the clinic with marked decay, afternoon fever, weight loss, pain in the left iliac fossa with irradiation to the left hemiabdomen and urinary symptoms of 5 months of evolution. During the investigations, moderate anemia, tumor image in the area of projection of the left iliac fossa and urinary infection were detected. By means of the contrasted abdominal CT scan, the presence of a benign tumor is defined without affecting: the wall abdominal, nor the descending colon and sigmoid. During the surgical act, the following was diagnosed: paracolic intra-abdominal abscess in the left iliac fossa. The patient was treated with broad-spectrum antibiotics. The patient's evolution was satisfactory. Intra-abdominal abscess is an entity that must be diagnosed early to avoid severe complications.
Introduction
An intra-abdominal abscess is a localized collection of pus inside the abdomen, which is surrounded by a fibrous wall or capsule of granulation tissue. Due to their origin, two large groups are recognized: those obtained the community and the postoperative periods. Depending on their location, they can be intraperitoneal, visceral and retroperitoneal and it begins in out-of-hospital and in-hospital settings. Likewise, this entity can be uncomplicated (limited to one organ) and complicated (diffuse to the entire peritoneum or located in a certain site such as the intra-abdominal abscess). The most frequent abscesses are: subphrenic abscesses, subhepatic abscesses, middle abdominal abscesses (antherse, right iliac fossa, left iliac fossa), pelvic abscesses.Verses 1-7This infection can originate in any abdominal organ, such as: the appendix, colon, liver, pancreas, ovaries, kidneys, spleen or uterus. The most common causes of intra-abdominal abscesses include: perforated appendicitis , colon diverticulitis, biliary infection, pancreatitis, intestinal perforation, abdominal trauma, previous abdominal surgery, and gynecologic infections, such as pelvic inflammatory disease or postpartum complications.1,5,8-10In some cases, intra-abdominal abscesses can be caused by bacteria that spread from other parts of the body, such as a skin or urinary tract infection. There are also certain risk factors that can increase the likelihood of developing an intra-abdominal abscess, such as: being over 50 years old, a weakened immune system, diabetes mellitus, Crohn's disease, ulcerative colitis, and cancer.7,8,10The symptoms and signs that make an abscess suspect are fever, usually in the evening, leukocytosis, anorexia and weight loss. Physical examination helps pinpoint the painful area of the abdomen and/or a palpable mass. This, due to its location, makes the anatomical sector affected suspicious.2-5.10Intra-abdominal infection is a common and serious health problem, which requires complex and multidisciplinary treatment. Its morbidity and mortality remain high despite the scientific and technical advances obtained by society. 7
Clinical case:
Reason for admission: decay.
A 68-year-old female patient, a smoker for 20 years, quit smoking at age 50. She has a personal pathological history of: hypothyroidism, high blood pressure, diabetes mellitus, glaucoma, herniated disc in the L5-S1 intervertebral space, repeated trauma to the lumbo-sacral spine associated with falls of the patient, left polycystic kidney with recurrent urinary sepsis, achalasia. He comes because in the last 10 months he had lost 60 pounds. The patient had been presenting periods of constipation of up to 12 days for 6 months, although her feces remained molded. He reported that along with these periods of constipation, pain was manifested in the left lumbar fossa with irradiation to the left hemiabdomen. For 5 months she has been presenting marked decay, dizziness and repeated urinary sepsis, which has limited her usual activities. In addition, since 1 month before the consultation, she has been presenting fetid and cloudy urine intermittently. The patient reported that she had been suffering from afternoon fever for 8 days, which subsided with the administration of antipyretic.
Positive physical examination:
- Skin: persistent skinfold and pale.
- Mucosa: slightly moist and pale.
- Abdomen: globulous, depressible, painful in the left abdomen. On palpation, a tumor mass was defined as covering the flank and left iliac fossa of ± 8cmx10cm, slightly movable, painful on palpation.
- Genitourinary system: positive anterior, superior and middle pyelorenoureteral points. Positive left costo-vertebral and costo-muscular points. Positive left fist-percussion maneuver.
- Rest unaltered.
On-call studies on admission:
- Blood count with differential:Hemoglobin (7.0 g/L),Hematocrit (0.21 u/L),Lekogram(16.1x109/L),Lymphocyte(8.5%),Monocyte(5.8%),Granulocyte ( 85.7%)
- Partial Urine:
Cyturia: Leukocytes-15,000, Cylinders-0 and Red Blood Cells-0
- Chest X-ray: no alterations
- X-ray of the abdomen plain: no alterations
It was decided to admit the patient to the Internal Medicine ward with the following diagnostic impressions:
- Acute pyelonephritis complicated by possible renal lithiasis in polycystic left kidney
- Possible severe anemia associated with left colon cancer.
Treatment is started with: Sulfaprim (480mg) 2 ampoules diluted in 100ml of 0.9% NaCl, EV c/12h for 10 days to pass in 1 hour.
Indoor studies:
- Blood Studies:
Hemoglobin was maintained between 4g/L and 5g/L. It was only possible to improve hemoglobin values with multiple blood transfusions. Granulocyte-predominant leukocytosis was persistent. Erythrocyte sedimentation was always higher than 100mm/h. Blood haemochemistry studies remained within the range of reference values during hospital admission. Samples were taken for 6 serial blood cultures, which were negative.
- Urine culture: No bacterial growth
- Abdominal ultrasound:
-Complex image in the left iliac fossa with a tumorous appearance.
-Polycystic left kidney.
-Colonoscopy is suggested.
- Rectosigmoidoscopy: no alteration. It is suggested to continue studies by colonoscopy.
- TAC simple de abdomen
-Liver, spleen and pancreas of preserved structure are observed. No focal lesions, no visceromegaly.
-Left kidney with multiple hypodense images, liquid densities (50 UH), rounded and polycystic in appearance: the largest measures 31x29 mm, no lithiasis. Renal parenchyma is not visualized.
-Right kidney normal structure. no dilation of excretory tracts, nor lithiasis.
-in projection of the left flank and left iliac fossa, a hypodense image with solid densities (32-40 UH) is observed, measuring 51x62com that extends from the descending colon to sigmoids of tumorous appearance. The lesion is impressive to occlude almost completely the intestinal lumen. Its center is 128 mm from the anal edge. Rest unaltered.
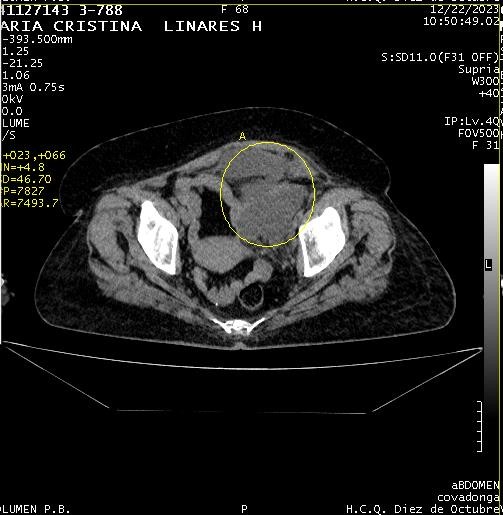 |
Image 1. CT scan photo of the simple abdomen showing a tumor mass in the left flank and left iliac fossa.
The study concludes:a-Tumor-like lesion in the descending colon and sigmoid. b-Colonoscopy is suggested.
- Colonoscopy: The mucosa of the cecum fundus, the ileocecal valve, and the appendicular os, which have normal characteristics, are visualized. At 45cm from the margins of the anus, stenosis is observed, which due to its characteristics is extrinsic. In this section, the passage of the team is difficult, although it is possible to win. The mucosa is observed, in some areas, with loss of the vascular pattern from which a sample is taken from this area for biopsy.
Conclusions:
- Nonspecific colitis.
- Colon stenosis due to extrinsic compression.
The case is discussed together with specialists from: Internal Medicine, Gastroenterology and Surgery. It is possible that the patient is a carrier of a tumor of extrinsic origin to the colon. The tumor may be causing a stenosis of the left colon. A contrasted CT scan of the abdomen should be performed. It was found in the hospitalization room that the patient again had a decrease in her hemoglobin to 4 g/L. There is no evidence of signs of digestive bleeding. Several red blood cell transfusions are indicated to the patient.
- Ct scan of the abdomen contrasted with iodine:
The lesion described in the CT study of the abdomen is well defined in this study. In the arterial and venous phases their densities are similar, there is no contrast uptake. Presence of image projection of the left flank and left iliac fossa with low densities (20-30 UH), well-defined regular contours. In addition, it can be seen that the image described presents a hyperdense halo that limits the lesion with respect to the abdominal wall and colon (descending and sigmoid). The lesion is lengthened with measurements of 54 x 60 mm, forming an interface and occupying an anterior plane. The lesion does not infiltrate neighboring structures.
No peri-aortic or retroperitoneal adenomegaly. Left kidney hydronephrosis is maintained. Due to the characteristics of the lesion described, a benign-looking intra-abdominal tumor is impressive.
Discussion
In paracolic abscesses, one of the most frequent causes is those originating in colonic perforations due to acute diverticulitis together with those originating in acute perforated appendicitis. When it is an abscess, that is, the process is localized and blocked, percutaneous drainage is the indication. In conventional surgery, a medium incision is made and it is only indicated when it is diffuse peritonitis or in those cases where percutaneous drainage was insufficient.9The multidisciplinary group that treated this patient considered that the most likely causes of the intra-abdominal abscess would be: multiple traumas to the lumbar fossa and lumbosacral spine due to the patient's falls and/or recurrent urinary sepsis associated with the polycystic kidneys. Among the risk factors for developing intra-abdominal abscesses, the patient has a history of diabetes mellitus and is over 50 years old. These are causes and risk factors collected in the international literature.2,3,8The first step in treatment is stabilization of the patient (administration of fluids, nasogastric catheterization) and intravenous antibiotic therapy. Effective management depends on: the exact location of the abscess, discrimination between single or multiple abscesses, early and adequate drainage. After treatment, the abscess is considered to be resolved when there is no longer clinical or radiological evidence of infection, and the associated symptoms (pain, inflammation or fever) have disappeared 4,9,10.Plain abdominal and chest x-rays are of interest in the patient's evaluation. They can induce diagnosis, but they do not replace computed tomography with intravenous and oral contrast, which is the method of choice10. In this patient, radiographic studies did not contribute to defining diagnosis or behavior. The contrasted CT scan proved to be a defining study.Intravenous and oral contrast computed tomography is the method of choice for diagnosis. Abscesses are manifested by a hypodense image and in some cases with hydro-aerial levels; it allows them to be located and to see the relationships with other viscera in order to define the most convenient route to carry out the drainage. The sensitivity of computed tomography in the diagnosis of abdominal collections is around 90%. It should not be forgotten that the definitive diagnosis of abscess is clinical and certainty is given by obtaining purulent fluid when puncturing a cavity.6The interesting thing in the case presented is that at the beginning the diagnostic possibilities were considered: complicated acute pyelonephritis and/or cancer of the left colon. At the end of the investigations, through the study of the contrasted abdominal CT scan, the possibility of a benign tumor begins to be assessed. Due to the patient's evolution and the studies obtained, the diagnosis of intra-abdominal abscess in the paracolic left iliac fossa was never considered. This was a finding during the surgical act.Complications of an intra-abdominal abscess can range from mild and transient to severe and life-threatening. They can affect the patient's recovery and outcome. The recurrence of the abscess after it has been treated and apparently resolved, may occur due to: the persistence of the original infection, the presence of a persistent source of infection, or the formation of a new related abscess. In the context of the treatment of intra-abdominal abscesses, mortality may occur due to: serious complications, uncontrolled infections, organ failure, or other underlying medical conditions5,8,9,10. In this patient, despite the long time of evolution, there were no complications, something uncommon.Intra-abdominal abscesses have a mortality rate of 10 to 40%. The course depends mainly on the primary disease or injury of the patient and their general medical condition, rather than the specific location and character of the abscess.8,9,10The intraadominal abscess of the paracolic left iliac fossa, in this patient, simulated a colon tumor due to its symptoms and evolution. Its effective treatment included: surgery and antibiotic therapy. The study patient, despite having several comorbidities and a long time of evolution, did not have postoperative complications. This result was achieved because the patient received care from a multidisciplinary group of surgeons, internists, imaging and gastroenterologists.
References
- Guerra Macías I. (2014). Classification of intra-abdominal abscesses. Letter to the editor. [Cited 20 June 2024]. MEDISAN vol.18 no.7 Santiago de Cuba Jun.-Jul.On-line version ISSN 1029-3019.
View at Publisher | View at Google Scholar - González Rodríguez FG. (2020). Protocol for the diagnosis and treatment of intra-abdominal abscesses. [Cited 10 June 2024]. Medicine - Accredited Continuing Medical Education Program. Volume 13, Number 10, Pages 587-
View at Publisher | View at Google Scholar - 589. Disponible: https://doi.org/10.1016/j.med.2020.06.008
View at Publisher | View at Google Scholar - M. Umar.(2024). Intraabdominal Abscesses [Citado 6 de junio 2024]. Abscess Types,Causes and Treatment. IntechOpen. Disponible en:http://dx.doi.org/10.5772/intechopen.1002902
View at Publisher | View at Google Scholar - Mehta NY, Lotfollahzadeh S, Copelin EL II. (2023). Abdominal abscess. [Citado el 15 de junio del 2024]. In:StatPearls (Internet). Treasure Island (FL):StatPearls Publishing; 3 June. Disponible en: https://www.ncbi.nlm.nih.gov/books/NBK519573/
View at Publisher | View at Google Scholar - Ansari P. (2023) Intra-abdominal abscesses [Cited 2024 Aug 13]. In: Rahway
View at Publisher | View at Google Scholar - Sartelli M, Chichom-Mefire A, Labricciosa FM, Hardcastle T, Abu-Zidan FM,Adesunkanmi AK, et al.(2017). The management of intra-abdominal infections from a global perspective: 2017 WSES guidelines for management of intra-abdominal infections. World J Emerg Surg; 12(1):29.
View at Publisher | View at Google Scholar - Zeynep Akcam F, Ceylan T,Kaya O, Ceylan E, Ridvan Tarhan O.(2020). Etiology, treatment options and prognosis of abdominal abscesses: A tertiary hospital experience. J Infect Dev Ctries; 14(1):59-65. doi:10.3855/jidc.11277
View at Publisher | View at Google Scholar - Fortea-Sanchis C, Forcadell-Comes E, Escrig Sos J. (2019) Risk factors for the appearance of intra-abdominal abscesses after appendectomy. Rev Cubana Cir vol.58 no.3 Ciudad de la Habana jul.-set. 2019 Epub 01-Sep. Print version ISSN 0034-7493. On-line version ISSN 1561-2945
View at Publisher | View at Google Scholar - Méchaï F, Kolakowska A, Carbonnelle E, Bouchaud O, Tresallet C, Jaureguy F. (2023).
View at Publisher | View at Google Scholar - . Intra-abdominal abscesses: Microbiological epidemiology and empirical antibiotherapy. Infectious Diseases Now 53 104604. Disponible en: https://doi.org/10.1016/j.idnow.2022.08.005
View at Publisher | View at Google Scholar - Lian L, Zhao Q, Shan Ma S, Xue B. (2024). Letter to the Editor Rare Causes of Retroperitoneal Abscess: A Case Report . Asian Journal of Surgery. Volume 47, Number 1, January 2024, Pages 691-692. Available at: https://doi.org/10.1016/j.asjsur.2023.09.176.
View at Publisher | View at Google Scholar
