

Research Article | DOI: https://doi.org/10.31579/2835-8465/003
Influence of Variation in Bony Entry Point on Outcome of Intertrochanteric Femur Fractures Treated with PFNA-2
1 Senior Resident, Department of Orthopaedics, Krishna Institute of Medical Sciences Karad, India.
2 Professor, Department of Orthopaedics, Krishna Institute of Medical Sciences Karad, India.
*Corresponding Author: Priyambada Kumar, KS Hegde Medical Academy, P.O. Nityanandanagar, Deralakatte, Mangaluru, Karnataka 575018, India.
Citation: Priyambada Kumar, Nitin S. Patil, Reddy Alladu. (2022), Influence of Variation in Bony Entry Point on Outcome of Intertrochanteric Femur Fractures Treated with PFNA-2, Orthopaedics Case Reports, 1(2), DOI:10.31579/2835-8465/003.
Copyright: © 2022 Priyambada Kumar, This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 October 2022 | Accepted: 18 November 2022 | Published: 09 December 2022
Keywords: bony entry point; low-energy trauma; elderly patients; similar fracture patterns; hip fractures; intertrochanteric femur fractures; PFNA-2; IM; EM
Abstract
Intertrochanteric femoral fractures are a topic of great interest around the world. They are the most commonly operated fracture type, and the high cost of care required after injury has made them a serious health resource issue. Though it is most commonly associated with low-energy trauma in elderly patients, high-energy trauma in young patients can result in similar fracture patterns. Females have a higher risk of sustaining an intertrochanteric femur fracture than males due to greater prevalence of osteoporosis. Low-energy falls from a standing height account for roughly 90% of hip fractures in patients over the age of 50, with a higher share of the female population.
Introduction
Intertrochanteric femoral fractures are a topic of great interest around the world. They are the most commonly operated fracture type, and the high cost of care required after injury has made them a serious health resource issue [1]. Though it is most commonly associated with low-energy trauma in elderly patients, high-energy trauma in young patients can result in similar fracture patterns. Females have a higher risk of sustaining an intertrochanteric femur fracture than males due to greater prevalence of osteoporosis [2]. Low-energy falls from a standing height account for roughly 90% of hip fractures in patients over the age of 50, with a higher share of the female population [3]. High-energy hip fractures are relatively infrequent and more common in men under the age of 40 [4].
Intertrochanteric and subtrochanteric femoral fractures present a challenge for the treating surgeon because the deforming forces on both the proximal and distal segments are difficult to control, especially given the proximal segment's inherent short length. The proximal segment is flexed, abducted, and externally rotated as a result of the pull of the iliopsoas, gluteus medius, and short external rotators, respectively. The unopposed pull of the adductor magnus and longus shortens and adducts the distal segment.
Aside from the difficulties in obtaining an anatomic reduction, the surgeon must ensure that the reduction is maintained throughout the process of healing. The implanted hardware is subjected to significant strain as the subtrochanteric region of the femur is subjected to mechanical forces several multiples of the patient's own weight. To accomplish this goal, various fixation options, including intramedullary (IM) and extramedullary (EM) devices, have been made available [5-7].
The strength of the fracture fragment-implant assembly is determined by several factors, namely (Kueffer et al) [8]:
a) bone quality
b) fragment geometry
c) reduction
d) implant design
e) implant placement.
Among the said factors, the surgeon can only control the quality of the reduction, the choice of implant, and its placement.
Proximal femur nail antirotaion – II, also known as PFNA-II, is a novel technology in orthopaedics. Instead of having separate derotation and compression screws, PFNA-II has a single helical blade and is suitable for patients with short stature, such as our Indian population. When the blade is driven inside the femoral head, it compacts the cancellous bone, increasing femoral head strength and stability in the cervico-cephalic direction [9].
A growing number of studies have recently shown that a poor introduction technique leads to a poor outcome [10-12]. One of the most important factor determining the success of the introduction technique is the entry point. The entry portal is crucial to determine the location of the PFNA-II after implantation and fracture reduction [13–18]. An optimal entry point serves to maintain reduction at fracture site, and also avoid implant-related complications. The objective of this study was to assess the optimal greater trochanter entry portal in patients with intertrochanteric femur fractures treated with PFNA-II implant.
Materials and Methods
The Study was conducted in the department of orthopaedics, from June 2019 to June 2021. The ethics committee clearance was given by Institutional Department of Ethics. 60 patients with intertrochanteric femur fracture, who were fitting the inclusion and exclusion criteria, were enrolled in the study after taking informed and written consent in the prescribed format.
This was a prospective comparative study done to evaluate the functional outcome of intertrochanteric femur fractures operated with Proximal femur nail antirotaion – II (PFNA II) with two different insertion points for the implant – (i) the tip of the greater trochanter and (ii) a point approximately 5mm medial to the tip of greater trochanter.
The fractures were classified pre – operatively according to the AO classification system after taking plain radiographs of :
(i) Pelvis with both hips in anteroposterior view (in 15 degrees internal rotation)
(ii) Lateral view of affected hip
Inclusion criteria:
a. All patients above 18 years of age.
b. Patients able to walk with or without aid prior to their injury.
c. Patients having stable/unstable intertrochanteric femur fracture.
Exclusion criteria:
a. Pathological fracture.
b. Patients who were not ambulatory prior to injury.
Surgical technique:
For both groups, the patient was placed on a fracture table with a perineal post after giving spinal anaesthesia. Reduction at the fracture site was achieved with traction, adduction and internal rotation.
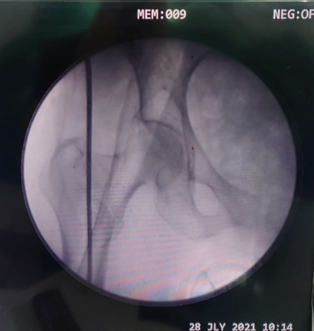
Once the fracture had been provisionally reduced, fluoroscopy views were obtained in the sagittal and coronal planes with the help of image intensifier(C-Arm). The main difference between the protocols for the two groups was the guide pin entry point at the great trochanter. In group A, the trochanteric entry point, was through the tip of the apex of the greater trochanter in the coronal plane and at the midpoint of the antero-posterior junction of the apex of the greater trochanter in the sagittal plane. (Figure 1).

In group B, we used an entry point that was approximately 5mm medial to the trochanteric apex along the medial edge of the greater trochanter in the coronal plane and in the centre in sagittal plane (Figure 2).
A guide wire was passed distally along the femoral shaft and a crusher was used to enlarge the bony entry portal in the proximal shaft. An appropriately sized intramedullary nail was then assembled with its corresponding intramedullary angle guide attachment and inserted through the widened bony entry portal. The nail was positioned to allow proper positing of helical blade in the femoral neck and head. Next, the PFNA-II helical blade and distal screw were inserted according to the manufacturer’s recommendations.
Operative time (from skin incision to skin closure) in minutes and amount of intra-operative blood loss were estimated and noted for both groups. Radiographic assessment was done for all patients post-operatively, and the positioning of the blade in the femoral canal was evaluated as described by Cleveland Index [19].
Follow up was done at 6 weeks, and thereafter monthly upto 6 months. The functional outcome was assessed using the Harris Hip Score [20] at 6 weeks, 3 months and 6 months post-operatively. Evidence of union was analysed from radiographs of the pelvis with both hips in AP view and that of the operated hip in lateral view using RUSH score [21] at each follow-up.
Date analysis: There was no bias of sex, age, mechanism of injury while choosing the samples. All data was entered the Microsoft Excel spreadsheet and variables were analysed using SPSS software. Continuous data with a normal distribution were expressed as mean ± standard deviation. Intergroup comparisons were made using the unpaired student’s t-test for normally distributed variable. All hypothesis tests were two-tailed. A value of p<0>
Observations and Results
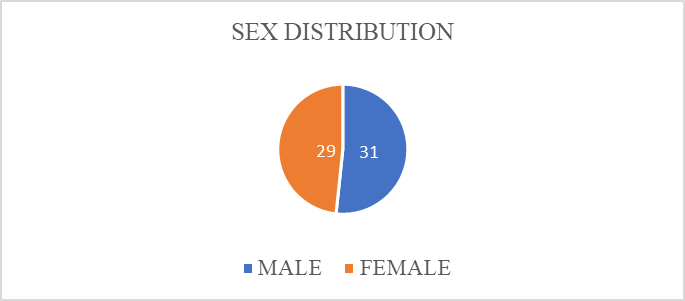
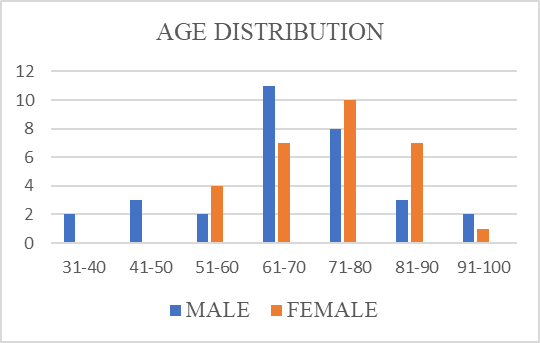
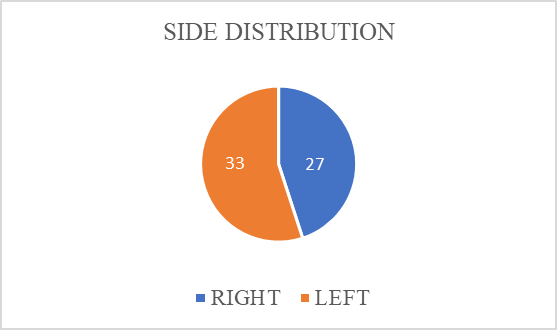
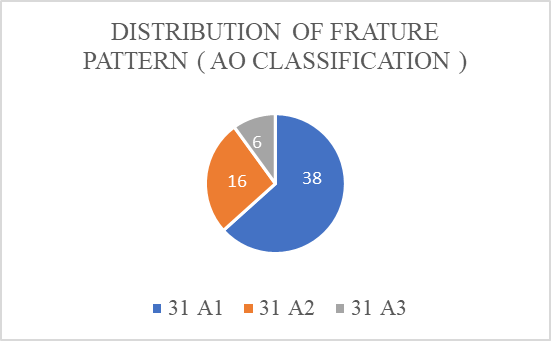
The baseline demographic data did not vary significantly in the two groups (Table 1). There were 31 males and 29 females included in our Study (Figure 3). Age groups of patients varied from 45 years to 85 years (Figure 4). Right side was involved in 27 cases and Left side was involved in 33 patients (Figure 5). The fractures were classified according to the AO classification system preoperatively (Figure 6) after taking plain radiographs of:
(i) Pelvis with both hips in antero-posterior view (in 15 degrees internal rotation)
(ii) Lateral view of affected hip
| GROUP A (n=30) Entry portal from tip of greater trochanter | GROUP B (n=30) Entry portal approx. 5 mm medial to tip of greater trochanter | P value |
Average Age (IN YEARS) | 69.24 +/- 3.2 | 71.18 +/- 2.8 | 0.58 |
Sex Distribution | Males - 16 Females - 14 | Males – 15 Females - 15 | 0.78 0.72 |
Side Distribution | Right - 12 Left - 18 | Right – 15 Left - 15 | 0.64 0.69 |
Table 1: Depiction of baseline demographic data in the two groups
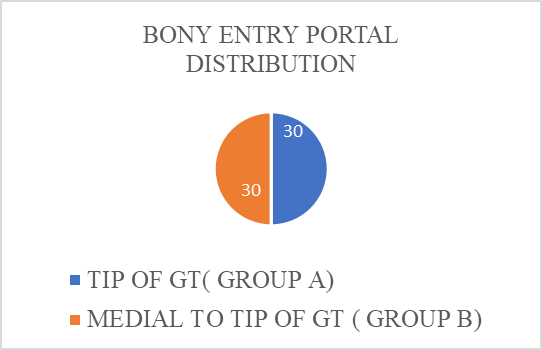
Two points of surgical entry were taken (Figure 7):
- Group A (n = 30) consisted of patients with entry portal taken at the tip of the apex of greater trochanter
- Group B (n = 30) consisted of patients with entry portal approximately 5 mm medial to the tip of greater trochanter
The present study had 38 patients with 31 A1 fracture pattern, 16 patients with 31 A2 fracture pattern and 6 patients with 31 A3 fracture pattern.
Intra-operative parameters: Average operating time (time taken from skin incision to skin closure) was significantly lower when bony entry was made approximately 5 mm medial to the tip of greater trochanter, as compared to when the entry was taken directly from the tip of the greater trochanter (p < 0 xss=removed>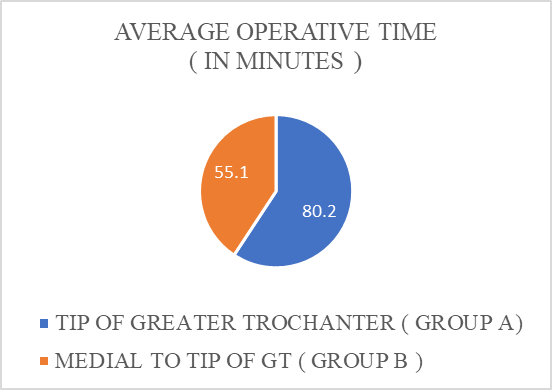
Radiological parameters: According to Cleveland Index, ideal positioning of the helical blade was observed in 21 out of 30 patients in Group A and 25 out of 30 patients in Group B . Sub-optimal positioning was observed in 9 out of 30 patients in Group A and 5 out of 30 patients in Group B (p = 0.034) According to RUSH score, the average time for radiological union was 14 +/- 2.4 weeks in Group A and 14 +/- 6.8 weeks in Group B (p = 0.84)
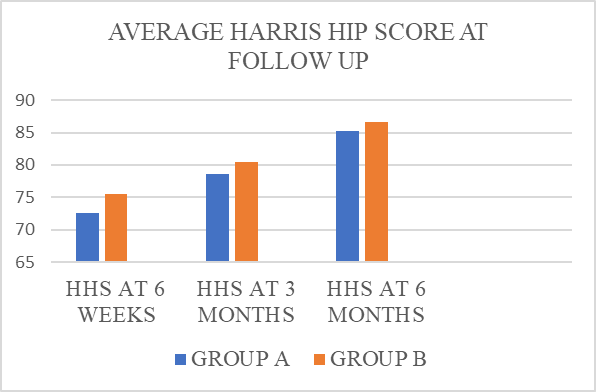
Functional outcome: The average Harris Hip Score at 6 weeks was 72.5 +/- 8.6 in Group A and 75.54 +/- 7.3 in Group B; at 3 months was 78 +/- 6.4 in Group A and 80.45 +/- 6.1 in Group B; and at 6 months was 85.31 +/- 5.9 in Group A and 86.59 +/- 7.4 in Group B (Figure 10). There was no significant difference in the functional outcome in both groups. (p = 0.72; p = 0.68; p = 0.69)
The results have been tabulated and depicted in Table 2.
GROUP A (n=30) Entry portal from tip of greater trochanter | GROUP B (n=30) Entry portal approx. 5 mm medial to tip of greater trochanter | P value | |
Average operative time (in minutes) | 80.2 +/- 5.6 | 55.1 +/- 6.9 | <0> |
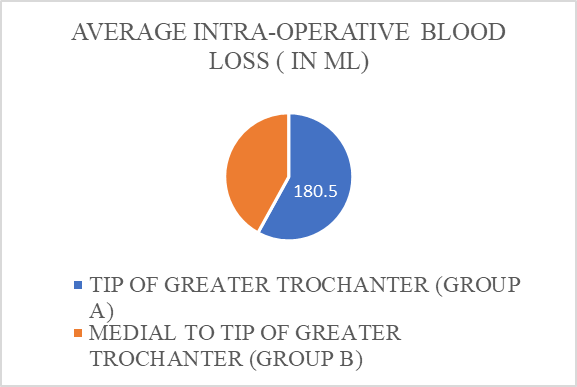
Average intra-operative blood loss (in ml) | 180.5 +/- 7.5 | 130.58 +/- 8.2 | 0.04 |
Cleveland Index:
|
21 9 |
25 5 |
0.041 0.034 |
Average time to radiological union in weeks (according to RUSH score) | 14 +/- 2.4 | 14 +/- 6.8 | 0.84 |
Harris Hip Score (HHS):
|
72.5 +/- 8.6 78 +/- 6.4 85.31 +/- 5.9 |
75.54 +/- 7.3 80.45 +/- 6.1 86.59 +/- 7.4 |
0.72 0.68 0.69 |
Table 2: Results
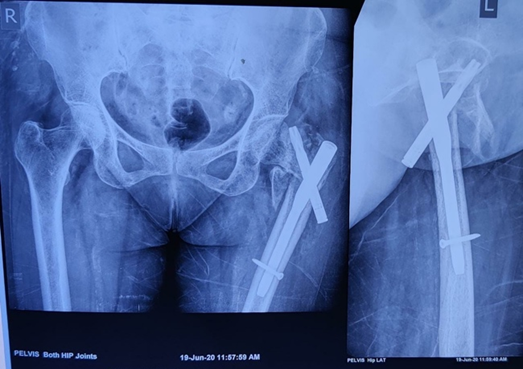
Complications: 2 patients in Group A with suboptimal Cleveland Index reported with varus collapse and helical screw backout. Revision surgery with exchange nailing was performed for both these patients. No such cases were reported in Group B . Figure 11 depicts varus collapse and helical blade backout at post-operative 4 months in a patient where entry was taken from tip of greater trochanter.
7 out of 30 patients in Group A reported with persistent abductor lurch and 6 out of 30 patients in Group A reported persistent lateral thigh pain at the end of 6 months. 3 out of 30 patients in Group B reported a persistent abducted lurch and 2 out of 30 patients in Group B complained of persistent lateral thigh pain at the end of 6 months. (p < 0 xss=removed> GROUP A (n=30) Entry portal from tip of greater trochanter GROUP B (n=30) Entry portal approx. 5 mm medial to tip of greater trochanter P value 2 0 0.036 7 3 <0> 6 2 0.028Varus collapse and helical screw backout Persistent abductor lurch Persistent lateral thigh pain
Table 3: Complications
Discussion
The bony entry portal is pivotal to the implant's success. It allows swift implant insertion, reducing the total operative time and intra-operative blood loss while also ensuring good fracture reduction. It also facilitates in the maintenance of reduction during the post-operative period and allows the patient to be mobilised at the earliest [2]. The baseline demographic data was similar in both groups.
When the entry point was taken approximately 5 mm medial to the tip of the greater trochanter as opposed to the tip of the greater trochanter, the average operative time and intra-operative blood loss were significantly lower (p <0>
In a study by Kane et al. [23], the ideal position of the screw was found to be in the lower-center and center-center positions, resulting in stable fixation. According to the Cleveland index, 9 of 30 patients with entry from the tip of the greater trochanter had sub-optimal entry, while 5 of 30 patients with medial entry had sub-optimal entry. Patients with medial entry had significantly better helical blade positioning in the femoral canal (p = 0.034). 2 patients in Group A with sub-optimal placement of the blade showed evidence of varus collapse and helical screw backout post-operatively . There have been no reports of such cases in patients with medial entry.
The complications of persistent abductor lurch and persistent lateral thigh pain were significantly higher in patients with entry from the tip of trochanter as compared to those in whom a medial entry was used. Our findings were consistent with those of Sharan Mallya et al (2020) [24], who found a significantly higher incidence of varus collapse, lateral cortex impingement, and helical screw backout in patients who underwent a lateral entry from the tip of greater trochanter. Macheras et al. [25] concluded that a medialised entry for PFNA-2 reduced lateral cortex impingement in unstable peri-trochanteric fractures. McConnell et al. described higher damage to the gluteus medius insertion due to a lateral entry from the tip, resulting in a persistent abductor lurch post-operatively [26].
There was no significant difference between the two groups when the average time required for radiological union of the fracture and clinical outcomes in terms of Harris Hip Score were compared. Tao et al. [27] emphasised that regardless of implant type and characteristics, the inserting technique is the most important factor in achieving stable fixation without complications.
Conclusion
Both entry points gave equivocal functional outcome post-operatively and did not bear influence on the time required for radiological union at fracture site (p > 0.05) However the ideal positioning of the blade according to Cleveland Index could be achieved smoothly with a shorter operative time with a medial entry. The complications of helical blade backout with varus collapse, persistent abductor lurch and persistent thigh pain were higher when entry was made directly through tip of greater trochanter. Overall, to achieve a smooth operative experience with minimal intra-operative blood loss, ensure better fixation at the fracture site with optimal implant positioning and a lower incidence of postoperative complications, we recommend a bony entry made approximately 5 mm medial to the tip of the greater trochanter.
Limitations of the Study
Our study had the limitation of a short follow-up period of 6 months, and small sample size.
Conflicts of Interest
The authors report no conflicts of interest.
References
- Endo Y, Aharonoff GB, Zuckerman JD, Egol KA, Koval KJ. (2005). Gender differences in patients with hip fracture: a greater risk of morbidity and mortality in men. J Orthop Trauma. 2005; 19:29–35.
View at Publisher | View at Google Scholar - S. Babhulkar, (2006). Management of trochanteric fractures, Indian Journal of Orthopaedics, 2006; vol. 40(4):210-218.
View at Publisher | View at Google Scholar - Kannus P Parkkari J, Sievancn H, Heinonen A, Vuori I, Jarvinen M. (1996). Epidemiology of hip fracture. Bone 1996; 18(l suppl):57S-63S.
View at Publisher | View at Google Scholar - Hwang LC, Lo WH, Chen WM, et al. (2001). Intertrochanteric fractures in adults younger than 40 years of age. Arch Orthop Trauma Surg. 2001; 121(3):123–126.
View at Publisher | View at Google Scholar - C. Dhamangaonkar, (2015). Management options and treatment algorithm in intertrochanteric fractures, Trauma International, 2015; vol. 1(1):12-16.
View at Publisher | View at Google Scholar - S.-Y. Kim, Y. G. Kim, and J. K. Hwang, (2005). Cementless calcar-replacement hemiarthroplasty compared with intramedullary fixation of unstable intertrochanteric fractures, The Journal of Bone and Joint Surgery (American), 2005; 87(10):2186-2192.
View at Publisher | View at Google Scholar - U. Bhakat and R. Bandyopadhayay, (2013); Comparative study between proximal femoral nailing and dynamic hip screw in intertrochanteric fracture of femur, Open Journal of Or- thopaedics, 2013; 3(7):291–295.
View at Publisher | View at Google Scholar - Sadowski C, Lu ̈bbeke A, Saudan M, Riand N, Stern R, Hoffmeyer P. (2002). Treatment of reverse oblique and transverse intertrochanteric fractures with use of an intramedullary nail or a 95 degrees screw plate: a prospective, randomized study. J Bone Joint Surg Am. 2002; 84(3):372–381.
View at Publisher | View at Google Scholar - Loo WL, Loh SYJ, Lee HC. (2011). Review of Proximal Nail Antirotation (PFNA) and PFNA-2–Our Local Experience. Malaysian Orthopaedic Journal. 2011; 5:1-5.
View at Publisher | View at Google Scholar - Seyhan M, Turkmen I, Unay K, Ozkut AT. (2015). Do PFNA devices and Intertan nails both have the same effects in the treatment of trochanteric fractures? A prospective clinical study. J Orthop Sci. 2015; 20:1053–1061.
View at Publisher | View at Google Scholar - Liu Y, Tao R, Liu F, Wang Y, Zhou Z, Cao Y, et al. (2010); Mid-term outcomes after intramedullary fixation of peritrochanteric femoral fractures using the new proximal femoral nail antirotation (PFNA). Injury. 2010; 41:810–817.
View at Publisher | View at Google Scholar - Sawaguchi T, Sakagoshi D, Shima Y, Ito T, Goldhahn S. (2014). Do design adaptations of a trochanteric nail make sense for Asian patients? Results of a multicenter study of the PFNA-II in Japan. Injury. 2014; 45:1624-1631.
View at Publisher | View at Google Scholar - Anastopoulos G, Chissas D, Dourountakis J, Ntagiopoulos PG, Magnisalis E, Asimakopoulos A, et al. (2010). Computer-assisted three-dimensional correlation between the femoral neck-shaft angle and the optimal entry point for antegrade nailing. Injury. 2010; 41:300-315.
View at Publisher | View at Google Scholar - Ansari Moein CM, Ten Duis HJ, Oey PL, de Kort GA, van der Meulen W, van der Werken C. (2011). Intramedullary femoral nailing through the trochanteric fossa versus greater trochanter tip: a randomized controlled study with in-depth functional outcome results. Eur J Trauma Emerg Surg. 2011; 37:615-622.
View at Publisher | View at Google Scholar - Crookshank MC, Edwards MR, Sellan M, Whyne CM, Schemitsch EH. (2014). Can fluoroscopy-based computer navigation improve entry point selection for intramedullary nailing of femur fractures? Clin Orthop Relat Res. 2014; 472:2720-2727.
View at Publisher | View at Google Scholar - Farhang K, Desai R, Wilber JH, Cooperman DR, Liu RW. (2014). An anatomical study of the entry point in the greater trochanter for intramedullary nailing. Bone Joint J. 2014; 96-B:1274-1281.
View at Publisher | View at Google Scholar - Zhao J, X Su, XY, Zhao Z, Zhang LC, Mao Z, Zhang H, et al. (2015). Predicting the optimal entry point for femoral antegrade nailing using a new measurement approach. Int J Comput Assist Radiol Surg. 2015; 10:1557-1565.
View at Publisher | View at Google Scholar - Ziran BH, Morganstein A. (2014). Preventing eccentric reaming of the trochanter during trochanteric nailing. J Orthop Trauma. 2014; 28:e88-e90.
View at Publisher | View at Google Scholar - Cleveland M, Bosworth DM, Thompson FR. (1947). Intertrochanteric fractures of the femur; a survey of treatment in traction and by internal fixation. J Bone Joint Surg Am. 1947; 29:1049-1067.
View at Publisher | View at Google Scholar - Vishwanathan K, Akbari K, Patel AJ. (2018). Is the modified Harris hip score valid and responsive instrument for outcome assessment in the Indian population with pertrochanteric fractures? J Orthop. 2018 Jan 3; 15(1):40-46.
View at Publisher | View at Google Scholar - Frank T, Osterhoff G, Sprague S, et al. (2016). The Radiographic Union Score for Hip (RUSH) Identifies Radiographic Nonunion of Femoral Neck Fractures. Clin Orthop Relat Res. 2016; 474(6):1396-1404.
View at Publisher | View at Google Scholar - Pan S, Liu XH, Feng T, Kang HJ, Tian ZG, Lou CG. Influence of different great trochanteric entry points on the outcome of intertrochanteric fractures: a retrospective cohort study. BMC Musculoskelet Disord. 2017; 18(1):107. Published 2017 Mar 14.
View at Publisher | View at Google Scholar - P. Kane, B. Vopat, W. Heard et al., (2014). Is tip apex distance as important as we think? a biomechanical study examining optimal lag screw placement, Clinical Orthopaedics and Related Research, 2014; 472(8):2492-2498.
View at Publisher | View at Google Scholar - Mallya S, Kamath SU, Annappa R, Nazareth NE, Kamath K, Tyagi P. (2020). The Results of Unstable Intertrochanteric Femur Fracture Treated with Proximal Femoral Nail Antirotation-2 with respect to Different Greater Trochanteric Entry Points. Adv Orthop. 2020 Mar 28; 2020:2834816.
View at Publisher | View at Google Scholar - G. A. Macheras, S. D. Koutsostathis, S. Galanakos, K. Kateros, and S. A. Papadakis, (2012). Does PFNA II avoid lateral cortex impingement for unstable peritrochanteric fractures? Clinical Orthopaedics and Related Research, 2012; 470(11):3067-3076.
View at Publisher | View at Google Scholar - T. Mc Connell, P. Tornetta, E. Benson, and J. Manuel, (2003); Gluteus medius tendon injury during reaming for gamma nail insertion, Clinical Orthopaedics and Related Research, 2003; 407:199-202.
View at Publisher | View at Google Scholar - Y. Tao, Z. Ma, and S. Chang, (2013). Does PFNA II avoid lateral cortex impingement for unstable peritrochanteric fractures? Clinical Orthopaedics and Related Research, 2013; 471(4):1393-1394.
View at Publisher | View at Google Scholar
