

Case Presentation | DOI: https://doi.org/10.31579/2835-785X/085
Inconsistency in Audiological Test Battery Entails Neuroimaging Study: A Child Case with Enlarged Vestibular Aqueduct.
1 Audiology Student (MS), Audiology Department, University of Social Welfare and Rehabilitation Sciences, Iran.
2 Audiology Student (Ph.D.), Audiology Department, Iran University of Medical Sciences, Iran.
3 Professor of Radiology, Radiology Department, Urmia University of Medical Sciences, Iran.
4 Assistant professor of audiology, Audiology Department, University of Social Welfare and Rehabilitation Sciences, Iran.
*Corresponding Author: Moslem Shaabani, Audiology department, Kodakyar Ave., Daneshjo Blvd., Evin, Tehran, Postcode: 1985713871, Iran.
Citation: Selva Samaei, Shima Iranfar, Afshin Mohammadi, Moslem Shaabani (2025), Inconsistency in Audiological Test Battery Entails Neuroimaging Study: A Child Case with Enlarged Vestibular Aqueduct, International Journal of Clinical Research and Reports. 4(3); DOI:10.31579/2835-785X/085
Copyright: © 2025, Moslem Shaabani. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 April 2025 | Accepted: 30 April 2025 | Published: 06 May 2025
Keywords: audiological test battery; cervical vestibular evoked myogenic potential; enlarged vestibular aqueduct; false conductive; high-resolution computerized tomography
Abstract
Enlarged vestibular aqueduct (EVA) is a bony labyrinthine disease. Several studies have shown EVA is associated with SNHL, which may also have a false conductive component.
The patient was a 4-year-old boy who presented with a complaint of hearing loss, accompanied by vomiting and true vertigo that occurred once every 45 days for the past year.
Pure tone audiometry revealed normal hearing in the right ear and moderate mixed hearing loss in the left ear with a false conductive component that is evident according to the normal results of tympanometry and acoustic reflexes in both ears. The findings of the cVEMP test followed a hydrops-like disease on the left side and/or an SSCD-like disease on the right side.
Based on the false conductive hearing loss and abnormalities/ inconsistencies in the vestibular test battery, the patient was referred for a high-resolution CT scan (HRCT). Results of HRCT showed a significant EVA on the left side. Referral for neuroimaging is critical when an audiological test battery reveals such inconsistencies.
Introduction
Enlarged vestibular aqueduct (EVA) is an inner ear abnormality often accompanied by sensorineural, conductive, or mixed hearing loss. Usually, the auditory and vestibular symptoms of EVA syndrome (EVAS or Large vestibular aqueduct syndrome (LVAS)) manifest during childhood [1,2]. Its occurrence has been reported in up to fifteen percent of all pediatric individuals with sensorineural hearing loss (SNHL). The vestibular aqueduct is a narrow bony canal that connects the inner wall of the vestibule of the inner ear to the posterior portion of the temporal bone. This aqueduct encompasses the endolymphatic duct and contains a portion of the endolymphatic sac, which serves as the site of endolymph reabsorption [3]. The canal's diameter is approximately less than 1.5 mm, which is about the same size as the posterior semicircular canal. The diagnosis of EVAS is established by using specialized temporal bone imaging techniques, such as high-resolution computed tomography (HRCT) or magnetic resonance imaging (MRI) studies. Several studies have shown that enlargement of the vestibular aqueduct is associated with sensorineural hearing loss, which may also have a false conductive component. In a study by Arkand et al., approximately twelve percent of individuals with congenital sensorineural hearing loss had large vestibular aqueduct syndrome [4].
Vestibular issues reported by EVA patients have been described less extensively than audiometric results. The reported prevalence of patient complaints varies notably from 12-71%, and symptoms vary from intermittent vertigo to unsteadiness [5,6]. While hearing loss can occur early in infancy, the manifestation of vestibular symptoms may be postponed until childhood. Moreover, individuals with vestibular problems may have episodic attacks of vertigo. However, these episodes rarely manifest consistently, as elucidated in the present case.
Case Presentation
The patient was a 4-year-old boy who presented with a complaint of hearing loss, accompanied by vomiting and true vertigo that occurred once every 45 days for the past year. His speech development was normal. From the age of 3, the parents had suspected the hearing loss in the left ear, which had started without a clear cause. There was no previous record of ear infections, seizures, head trauma, or meningitis in the patient's medical history. There was no history of hearing loss in the patient's family. Following admission, a thorough audiological evaluation was performed, including otoscopy, pure tone audiometry (PTA), tympanometry, acoustic stapedial reflex test, auditory brainstem response (ABR), videonystagmography (VNG), video head impulse test (VHIT), and cervical vestibular evoked myogenic potentials (cVEMPs). Moreover, neuroimaging data was gathered using CT scans.
Evaluations of hearing (PTA) revealed normal hearing in the right ear and moderate mixed hearing loss in the left ear with a false conductive component that is evident according to the normal results of tympanometry and acoustic reflexes in both ears (Figure 1). The speech test results (SRT and WRS) verified the audiogram, too. In addition, ABR results were in line with PTA. The morphology of ABR in the right ear was significantly better than in the left ear (Figure 1). In the right side, all peaks were sharper and had more amplitude comparing to the left side; however, the peaks’ latencies on the left side did not confirm the conductive loss. Therefore, the conductive component in PTA could not be a real one. We know that a false conductive component usually indicates a third-window disease [7], like superior semicircular dehiscence (SSCD), in which the patient has a pathological mobile window in addition to the natural oval and round windows [8].
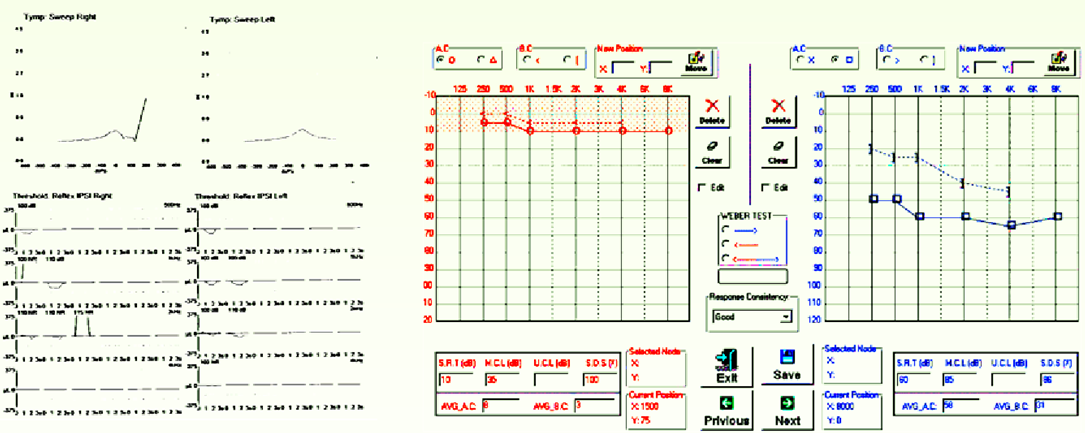
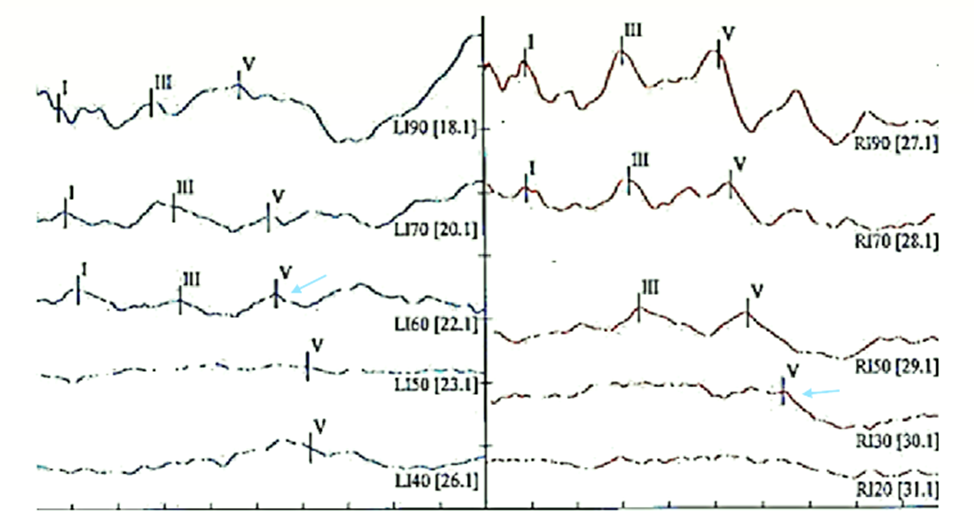
Figure 1: Up: Tympanogram and acoustic reflex results. As depicted, sharp reflexes recorded from the left-ear. Left-ear audiogram shows mixed hearing loss; Down: ABR results recorded via insert phone and click stimulus. Based on wave V recording, estimated thresholds were about 50 dB and 20 dB on the left and right sides, respectively (i.e., 10 dB below the sharp and reliable wave V marked with arrows).
Based on VNG subtests, the central oculomotor results were normal; for instance, the outcomes of the smooth pursuit test performed at a velocity of 0.45 Hz showed perfect conformity with the established norms. There was not any spontaneous nystagmus. However, we observed slight right-beating nystagmus in the head-shaking test, indicating an active or uncompensated vestibular disorder in the left ear. Conversely, caloric results showed no significant vestibular weakness or preponderance (Figure 2). Similarly, the video head impulse test had no catch-up saccades or weaknesses (VHIT).
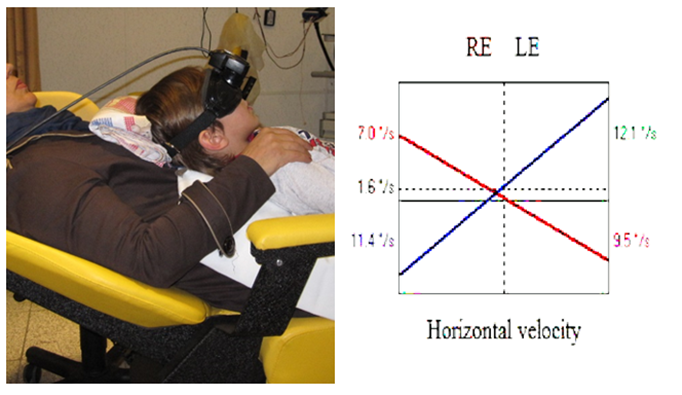
Figure 2: Bi-thermal caloric results. Left: caloric position for reducing the child’s anxiety. Right: caloric results. The results were in normal clinical range.
The cVEMP test results, performed with muscle monitoring, revealed that the responses on the right side had a better morphology, larger amplitude, and lower thresholds than those on the left side (Figure 3). Therefore, the findings of the cVEMP test were in accordance with a hydrops-like disease on the left side [9] and/or an SSCD-like disease on the right side [10].
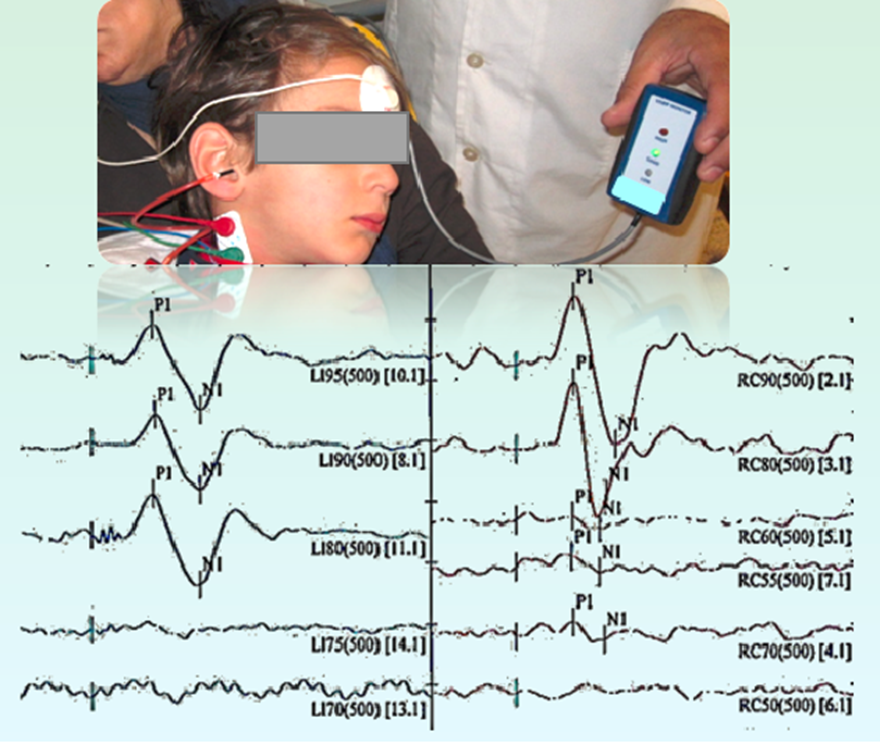
Figure 3: cVEMP results. Up: Recording of cVEMP with EMG monitoring. Down: The reliable response using 500 Hz tone burst recorded down to 80 dB and 70 dB for the left and right sides, respectively. Response amplitudes were significantly higher in the right-side.
Based on the false conductive hearing loss and abnormalities/ inconsistencies in the vestibular test battery, the patient was referred for a high-resolution CT scan (HRCT). Results of HRCT showed a significant EVA on the left side (Figure 4). VA diameter was about 1 mm and 4.2 mm on the right and left sides, respectively.
Therefore, in line with the diagnosis of unilateral EVA, corticosteroids are prescribed to control vestibular symptoms. On the other hand, the risks of head trauma in contact sports, the risk of barotrauma, and the need for periodic hearing evaluation were discussed with his parents.
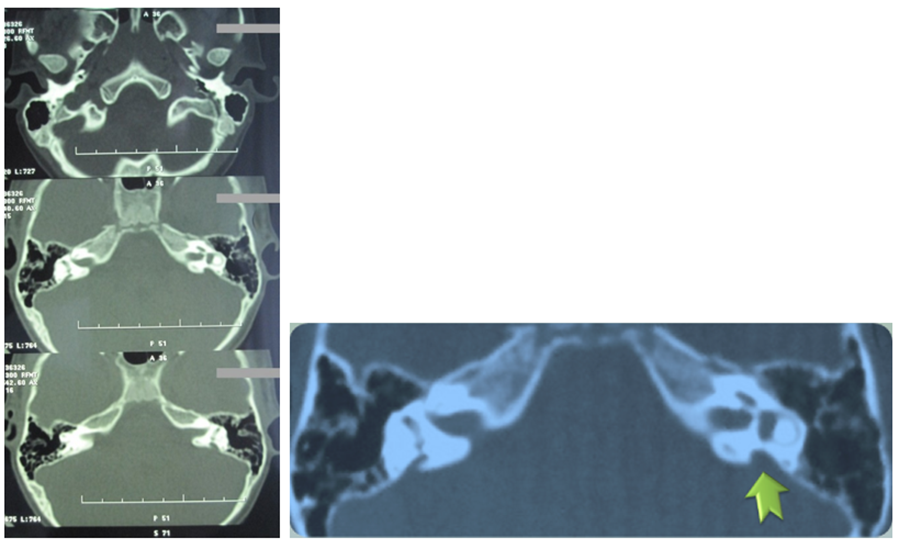
Figure 4: HRCT results. As marked with an arrow, EVA is obvious on the left side.
Discussion
We have reported a 4-year-old child with EVA in this case report. We have also presented the audiological and radiological results.
Sensorineural hearing loss is the most common type of hearing loss associated with EVA, although conductive and mixed types are also possible [11]. In many cases, hearing loss development reveals quick progress towards severe or profound sensorineural hearing loss and is characterized by incremental decreases in auditory thresholds; accordingly, assessing bone conduction thresholds is impossible. As a result, very few people have isolated conductive hearing loss caused by an enlarged vestibular aqueduct [12–14]. However, the results of our study suggest that the BC threshold should be taken cautiously because we may have a false conductive loss. Moreover, Sato et al. (2002) conducted a time-based study on a sample of 24 ears with EVA; all patients had a Type A tympanogram, like our case [15].
It is possible that the child may not respond well to the behavioral tests, so to investigate brainstem auditory neural pathways and validate the behavioral results, we used ABR testing, like previous research [16].
As a result, the presence of a false conductive component in the audiogram of a child, in the presence of obvious acoustic reflexes and a history of vertigo attacks, can be an alarming sign to identify a large vestibular aqueduct or other common structural abnormalities like the third window in the inner ear.
The incidence of vestibular symptoms in individuals with enlarged vestibular aqueduct (EVA) has been found to range from 4% to 100% in previous studies [17, 18]. In some studies, unilateral or bilateral caloric weakness was seen in the majority of individuals with EVA accompanied by vertigo [19, 20]. However, the caloric result was normal in our case. Our experience showed that performing caloric tests in the mentioned position (Figure 2) can reduce the children's anxiety.
The cervical vestibular evoked myogenic potential (C-VEMP) test revealed an unexpectedly low threshold on the right side (70 dB). The threshold level of 70 represents the threshold of the SSCD [10]. Therefore, it indicates the presence of a pathological condition on the corresponding side. On the other hand, we observed the VEMP's lower threshold on the right side, which could be a sign of LVAS [21, 22].
On the left side, however, the threshold was high, and the amplitude was less. And it's strange that even if a person has a reflex (has a false gap), his VEMP decreases on the same side. Despite this, our patient had a problem with his left ear. According to the VEMP test, the disorder appears on the left side (with lower amplitude). It appears that he has a disorder like endolymphatic hydrops [23] on the left side, which was matched with his history but not matched with his false conductive component. However, lower VEMP response is also reported in LVAS cases [24], like our case. Therefore, based on the literature, there is a discrepancy between VEMP results in LVAS cases.
Consequently, it is recommended that structural temporal diseases be ruled out in situations where these inconsistencies exist, especially considering the incidence of structural problems in children presenting with hearing loss and/or dizziness. Referral for neuroimaging is critical when an audiological test battery reveals such inconsistencies.
References
- Shiao A-S. Chronological changes of hearing in pediatric patients with large vestibular aqueduct syndrome. Laryngoscope. 2004 May;114(5):832–838.
View at Publisher | View at Google Scholar - Piromchai P, Kasemsiri P, Thanawirattananit P, Yimtae K. Congenital Malformations of the Inner Ear: Case Series and Review of the Literature. J Med Assoc Thai. 2015 Aug;98 Suppl 7:S217-24.
View at Publisher | View at Google Scholar - Fatterpekar GM, Doshi AH, Dugar M, Delman BN, Naidich TP, Som PM. Role of 3D CT in the evaluation of the temporal bone. Radiogr a Rev Publ Radiol Soc North Am Inc. 2006 Oct;26 Suppl 1:S117-132.
View at Publisher | View at Google Scholar - Arcand P, Desrosiers M, Dubé J, Abela A. The large vestibular aqueduct syndrome and sensorineural hearing loss in the pediatric population. J Otolaryngol. 1991 Aug;20(4):247–250.
View at Publisher | View at Google Scholar - Emmett JR. The large vestibular aqueduct syndrome. Am J Otol. 1985 Sep; 6(5):387–415.
View at Publisher | View at Google Scholar - Grimmer JF, Hedlund G. Vestibular symptoms in children with enlarged vestibular aqueduct anomaly. Int J Pediatr Otorhinolaryngol. 2007 Feb; 71(2):275–282.
View at Publisher | View at Google Scholar - Merchant SN, Rosowski JJ. Conductive hearing loss caused by third-window lesions of the inner ear. Otol & Neurotol Off Publ Am Otol Soc Am Neurotol Soc [and] Eur Acad Otol Neurotol [Internet]. 2008; 29(3):282–289. Available from: http://europepmc.org/abstract/MED/18223508
View at Publisher | View at Google Scholar - Iversen M, Rabbitt R. Biomechanics of Third Window Syndrome. Front Neurol. 2020 Aug 1; 11:891.
View at Publisher | View at Google Scholar - Grigol TA de A e S, Lopes K de C, Ganança FF. Cervical vestibular evoked myogenic potentials and video head impulse test in Ménière disease. Brazilian J Otorhinolaryngol (English Ed [Internet]. 2020; 86(5):534–544.
View at Publisher | View at Google Scholar - Noij KS, Rauch SD. Vestibular Evoked Myogenic Potential (VEMP) Testing for Diagnosis of Superior Semicircular Canal Dehiscence. Front Neurol. 2020; 11:695.
View at Publisher | View at Google Scholar - Ruthberg JS, Kocharyan A, Farrokhian N, Stahl MC, Hicks K, Scarborough J, et al. Hearing loss patterns in enlarged vestibular aqueduct syndrome: Do fluctuations have clinical significance? Int J Pediatr Otorhinolaryngol. 2022 May; 156:111072.
View at Publisher | View at Google Scholar - Merchant SN, Nakajima HH, Halpin C, Nadol Jr JB, Lee DJ, Innis WP, et al. Clinical investigation and mechanism of air-bone gaps in large vestibular aqueduct syndrome. Ann Otol Rhinol Laryngol. 2007; 116(7):532–541.
View at Publisher | View at Google Scholar - Yang N, Yang B-B. A Large Vestibular Aqueduct with Conductive Hearing Loss as the Only Manifestation. Ear, Nose Throat J. 2023; 01455613231183539.
View at Publisher | View at Google Scholar - Wendt W-J, Hashikawa A. Enlarged Vestibular Aqueduct Syndrome: Sudden Hearing Loss in a Child with a Cerebral Shunt. Pediatr Emerg Care. 2019 Jul; 35(7):e135–137.
View at Publisher | View at Google Scholar - Sato E, Nakashima T, Lilly DJ, Fausti SA, Ueda H, Misawa H, et al. Tympanometric findings in patients with enlarged vestibular aqueducts. Laryngoscope. 2002; 112(9):1642–1646.
View at Publisher | View at Google Scholar - Zhou G, Gopen Q, Kenna MA. Delineating the hearing loss in children with enlarged vestibular aqueduct. Laryngoscope. 2008 Nov; 118(11):2062–2066.
View at Publisher | View at Google Scholar - Madden C, Halsted M, Benton C, Greinwald J, Choo D. Enlarged vestibular aqueduct syndrome in the pediatric population. Otol Neurotol Off Publ Am Otol Soc Am Neurotol Soc [and] Eur Acad Otol Neurotol. 2003 Jul; 24(4):625–632.
View at Publisher | View at Google Scholar - Oh AK, Ishiyama A, Baloh RW. Vertigo and the enlarged vestibular aqueduct syndrome. J Neurol. 2001 Nov; 248(11):971–974.
View at Publisher | View at Google Scholar - Jung J, Suh MJ, Kim SH. Discrepancies between video head impulse and caloric tests in patients with enlarged vestibular aqueduct. Laryngoscope. 2017 Apr; 127(4):921–926.
View at Publisher | View at Google Scholar - Li M, Leng Y, Liu B. Clinical Implication of Caloric and Video Head Impulse Tests for Patients with Enlarged Vestibular Aqueduct Presenting with Vertigo. Front Neurol. 2021; 12:717035.
View at Publisher | View at Google Scholar - Zhou Y-J, Wu Y-Z, Cong N, Yu J, Gu J, Wang J, et al. Contrasting results of tests of peripheral vestibular function in patients with bilateral large vestibular aqueduct syndrome. Clin Neurophysiol Off J Int Fed Clin Neurophysiol. 2017 Aug; 128(8):1513–1518.
View at Publisher | View at Google Scholar - Sheykholeslami K, Schmerber S, Kermany MH, Kaga K. Vestibular-evoked myogenic potentials in three patients with large vestibular aqueduct. Hear Res. 2004; 190(1–2):161–168.
View at Publisher | View at Google Scholar - Timmer FCA, Zhou G, Guinan JJ, Kujawa SG, Herrmann BS, Rauch SD. Vestibular evoked myogenic potential (VEMP) in patients with Ménière’s disease with drop attacks. Laryngoscope. 2006 May; 116(5):776–779.
View at Publisher | View at Google Scholar - Zhang Y, Chen Z, Zhang Y, Hu J, Wang J, Xu M, et al. Vestibular-evoked myogenic potentials in patients with large vestibular aqueduct syndrome. Acta Otolaryngol. 2020; 140(1):40–45.
View at Publisher | View at Google Scholar
