

Research Article | DOI: https://doi.org/10.31579/2835-9291/016
Impacts of HIV Infection on Pulmonary Tuberculosis in Sub-Saharan Africa
1 Infectious and Tropical Diseases department of the University Teaching Hospital (UTH) point G of Bamako.
2 Faculty of Medicine and Odontostomatology of the University of Sciences, Techniques and Technologies of Bamako.
3 Tuberculosis and HIV Research and Training Center of Bamako.
4 Doctor Without Borders Cameroon.
*Corresponding Author: Ouo Loua, Infectious and Tropical Diseases department of the University Teaching Hospital (UTH) point G of Bamako.
Citation: Loua O., Soumaré M., Konaté I., Ngueta Sabeya Z., Cissoko Y., et al, (2024), Impacts of HIV Infection on Pulmonary Tuberculosis in Sub-Saharan Africa, International Journal of Clinical Case Studies, 3(1); DOI:10.31579/2835-9291/016
Copyright: © 2024, O Loua. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 January 2024 | Accepted: 16 February 2024 | Published: 20 February 2024
Keywords: immunosuppression; impact; sub-saharan Africa; tb/hiv co-infection
Abstract
Introduction: Tuberculosis is a major public health problem in developing countries where its incidence is increased by HIV infection. Our main objective was to determine the epidemiological, diagnostic and prognostic impacts of HIV infection on pulmonary tuberculosis. Methods: this was an analytical and descriptive retrospective study, from January 1, 2015 to June 30, 2017, on TB/HIV co-infected patients and cases of pulmonary tuberculosis hospitalized in the infectiology and pneumophtisiology departments of the UTH Point G in Bamako, with a usable radiological image and file. The sampling was exhaustive and the data collected was entered and analyzed using SPSS 21.0 software. The comparison of the proportions was made by the significant Pearson chi-square test of association if p<0.05 through a multivariate analysis in which the Fisher test was made in case of confusion between the qualitative variables. Results: the frequency of TB/HIV co-infection was an additional 3.2% of the 42.5% for cases of pulmonary tuberculosis. The diagnosis of TB/HIV co-infection was suggested in the face of deterioration in general condition (81.1%) associated with pulmonary condensation syndrome (73%) or normal pleuropulmonary examination (20.3%). The majority of patients had a CD4<200 cells/μl (88.2%). Bacilloscopic and Gene-Expert were negative in 85.3 and 52.9% of cases respectively and significantly influenced by severe immunosuppression (95%; p=0.000; CI = 0.000 – 0.040 and 95%; p=0.001, CI = 0.000 – 0.040). The chest radiography was mostly pathological (79.7%), made up of diffuse lesions (55.8%), of the military type (21.6%) and caverns (18.9%), respectively linked to severe immunosuppression (95%; p=0.024; CI = 0.000 – 0.064 and 95%; p=0.000; CI = 0.000 – 0.040). Lethality in TB/HIV co-infected was an additional 27% of the 4.2% lethality attributable to isolated pulmonary tuberculosis. Conclusion: the impact of HIV infection on pulmonary tuberculosis is global because it, through the immunosuppression it generates, modifies the clinical, biological and radiological aspects of pulmonary tuberculosis, worsens the vital prognosis of patients and increases the number of tuberculosis cases. A normal pleuropulmonary examination and/or a negative bacilloscopic and Gene-Expert and/or a normal aspect of the chest radiography in the immunocompromised does not exclude progressive pulmonary tuberculosis.
Introduction
Tuberculosis remains today a major public health problem in developing countries where infection with the human immunodeficiency virus (HIV) increases its incidence and reinforces its endemicity. About 15 million people worldwide are co-infected with Mycobacterium tuberculosis complex and HIV, 70% of whom live in sub-Saharan Africa [1–3] where its frequency varies between 50 and 79% [4]. The excess death rate from TB among people living with HIV is 14% globally [5] and 16–50% in sub-Saharan Africa [6–8].
In Mali, tuberculosis is endemic there and the most frequent opportunistic lung disease during HIV infection, with a frequency of 88.3 and 92.1% against 12.4 and 15.1% for TB/HIV co-infection respectively in 2015 and 2016 [9].
The clinical and paraclinical manifestations of progressive pulmonary tuberculosis are varied, ranging from paucity symptomatic forms to severe ones in Person living with HIV (PLHIV), compared to the typical form common in most non-HIV infected subjects [10–13].
The absence of a similar study focusing on the overall impact of HIV infection on pulmonary tuberculosis in Mali motivated this study aimed at describing the epidemiological, diagnostic and prognostic impacts of HIV infection on the pulmonary tuberculosis.
Materials and methods
This was an analytical and descriptive retrospective study, from January 1, 2015 to June 30, 2017, on TB/HIV co-infected patients and cases of isolated pulmonary tuberculosis hospitalized in the Infectiology and Pneumophtisiology departments of the Point G University Hospital of Bamako. Were included included in the study were TB/HIV co-infected patients with a frontal chest radiography and a usable medical file, and cases of isolated pulmonary tuberculosis. We’re not included the patients co-infected with TB/HIV who did not have an unusable file were not included in the study.
The TB/HIV co-infected patients were split into two immunological groups: CD4 ≥ 200 cells/mm3 and CD4 < 200>
The diagnosis of pulmonary tuberculosis was made based on the following arguments:
• Bacteriologically confirmed pulmonary tuberculosis: all cases of pulmonary tuberculosis confirmed by bacilloscopy and/or Gene-Xpert and/or culture [2,14];
• Radiologically confirmed pulmonary tuberculosis: all cases of pulmonary tuberculosis diagnosed on the basis of clinico-therapeutic and radiological arguments suggestive of pulmonary tuberculosis [2,15].
The sampling was exhaustive and involved all patients admitted to the two departments during the study period. Under anonymity, data were obtained from medical records and hospitalization registers. The epidemiological, clinical, paraclinical, therapeutic and evolutionary aspects were studied. Data processing and analysis were done using SPSS 21.0 software. For the comparison of the proportions, we carried out the Pearson chi-square association test with a significance level p < 0>
Results
Epidemiological aspect: from January 1, 2015 to June 30, 2017, we collected 970 pulmonary tuberculosis files including 74 cases of TB/HIV co-infection out of 2280 hospitalizations, Either a frequency of pulmonary tuberculosis of 42.5%, that of co-infection -TB/HIV infection at 3.2% (7.2% of all cases of pulmonary tuberculosis) (Table I). Among the TB/HIV co-infected: 44 (59.5%) had an age range of 35 to 54 years (40.5 ± 11.7 years on average) with extremes of 15 to 68 years; 43 (58.1%) were male with a sex ratio of 1.4 M/F; 51 (68.9%) were married; more than 3/4 (81.1%) came from the district of Bamako; 24 (32.4%) were housewives; and 4 (5.4%) had a notion of tuberculosis contagion a history of tuberculosis (table I).
Clinical aspect: among the TB/HIV co-infected: 60 (81.1%), 36 (48.6%), 34 (45.9%) and 34 (45.9%) had as functional signs respectively the deterioration of the general state, the fever, evening sweats and cough; pleuropulmonary examination was marked by pulmonary condensation syndrome in 54 (73%), and normal in 15 (20.3%); 65 (87.8%) patients were classified as WHO stage III (figure 1).
Paraclinical aspect: 72 (97.3%) patients were infected with HIV-1, 30/34 (88.2%) co-infected with TB/HIV had a CD4 count < 200mm3>
Therapeutic and evolutionary aspects: among the TB/HIV co-infected, there were 70 (94.6%) new cases of pulmonary tuberculosis and 36 (75%) were under the TDF+3TC+EFV regimen; the average duration of hospitalization was 31.7 days and 20 died, either a lethality of 27% against 38 (4.2%) deaths attribuable to isolated pulmonary tuberculosis (figure 2).
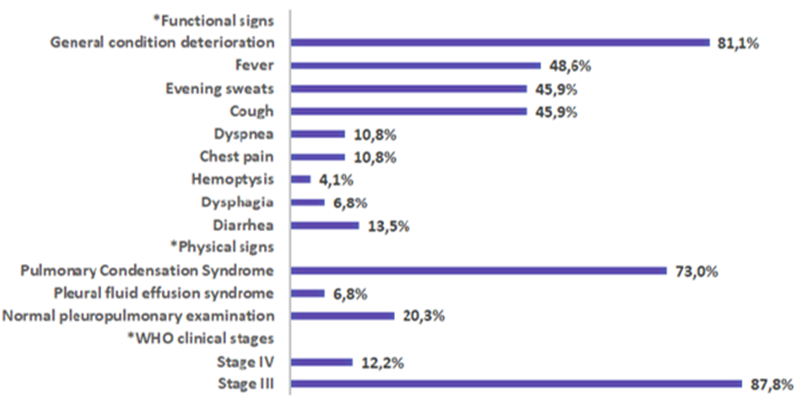
Figure 1: Distribution of patients according to clinical data
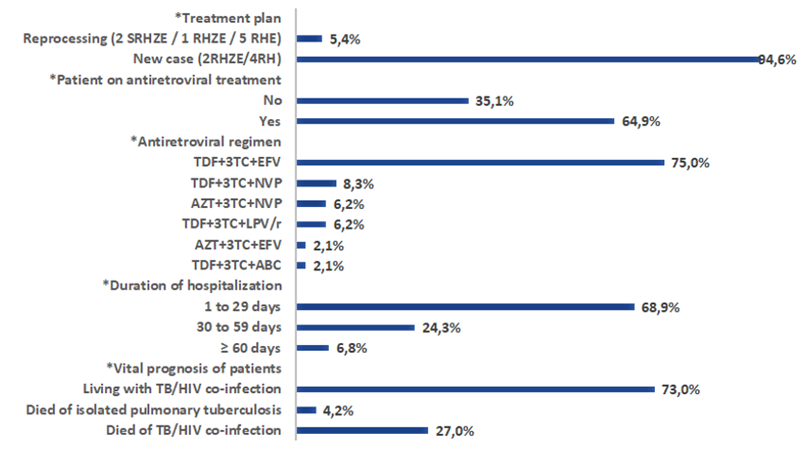
(S: streptomycin, R: rifampicin, H: isoniazid, Z: pyrazinamide, E: ethambutol, TDF: tenofovir, 3TC: lamivudine, EFV: efavirenz, NVP: nevirapine, AZT: zidovudine, LPV: lopinavir, r: ritonavir, ABC: abacavir)
Figure 2: Distribution of patients according to therapeutic and evolutionary data
The multivariate statistical analysis in TB/HIV co-infected: bacilloscopy and Gene-Xpert were mostly negative in patients with a CD4 count < 200>
respectively significant (95%; p = 0.000; CI = 0.000 – 0.040 and 95%; p = 0.001; CI = 0.000 – 0.040), the image of miliary predominated in patients with a CD4 count less than 200mm3
respectively significant (95%; p = 0.000; CI = 0.000 – 0.040 and 95%; p = 0.001; CI = 0.000 – 0.040), the image of miliary predominated in patients with a CD4 count less than 200mm3
(95percentage; p = 0.000; CI = 0.000 – 0.040 and 95percentage; p = 0.001; CI = 0.000 – 0.040), the image of miliary predominated in patients with a CD4 count less than 200 cells by mm3 (95percentage; p = 0.024; CI = 0.000 – 0.064), excavations and the fluid pleural effusion syndrome predominated in patients with a CD4 count ≥ 200 cells by mm3 (95percentage; p = 0.000; IC = 0.000 – 0.040), the other radiological aspects had no relationship with the degree of immunosuppression (p greater than 0.05); the majority of deaths occurred in patients with a CD4 count less than 200 cells bymm3 (95 percentage; p = 0.045; CI = 0.068 – 0.230) (table III).
Discussion
Active pulmonary tuberculosis is a serious pulmonary bacterial infection that can occur at any time, but its occurrence and evolution are favored by immunosuppression, in particular HIV infection, causing a clinical-biological, radiological change and prognosis of pulmonary tuberculosis [10,15–19].
The radiological aspects observed during TB/HIV co-infection are multiple and vary from one patient to another, depending on their immune responses, the associated pneumonitis and the time to diagnosis [3,16,18,20,21].
Epidemiological aspect: in Mali, the frequency of TB/HIV co-infection has decreased in recent years, going from 4.39% in previous years [22] to 4.30% from 2014 to 2016 [23], then 3.2 % from 2015 to mid-2017 (our study), unlike some African countries [1,6,7,24–26], due to early and routine screening for HIV infection and triple antiretroviral therapy in patients, and the inequality of study population sizes.
The predominant age range and average age in our study corroborate those of another study in Mali [23] and other similar African studies [1,18,24,25]. This could be explained by the fact that this age group is made up of subjects who are more sexually active on the one hand, thus exposing them to HIV infection which promotes the onset of tuberculosis, and on the other more dynamic in regular contact with each other, thus exposing them to tuberculosis contagion. Contrary to certain studies on HIV infection [27,28], the predominance of men in our study is explained by the fact that the study focused almost on TB/HIV co-infection and men, the most dynamic in society, are more at risk of tuberculous contagion.
Clinical aspect: the predominant clinical symptomatology (bacillary impregnation syndrome and pulmonary condensation syndrome), as described in certain similar studies and literature [1,25,29], could be explained by the fact that these are two active (chronic) infections affecting the whole system and diagnosis of advanced lung disease. The predominant WHO clinical stage III in our study could be explained by the use of consultation and late diagnosis for some patients and non-compliance with treatment for others.
Paraclinical aspect: the predominance of HIV type 1 infection in our study, also described in certain studies [23,24,28,30], is explained by the fact that this virus is historically the most widespread in Africa according to the literature [31,32]. As in a similar study [18], the CD4 count was mostly below 200 cells/mm3 due to late diagnosis for some and noncompliance with treatment for others, but also tuberculosis itself causes immunosuppression [33]. Of the 74 co-infected with TB/HIV, bacilloscopy was mostly positive, however of the 34 patients who performed their CD4 counts bacilloscopy and Gene-Xpert were mostly negative as in a similar study [1], because the majority of our patient had severe immunosuppression (CD4 count < 200>
Therapeutic aspects: the majority of our patients benefited from the TDF+3TC+EFV antiretroviral treatment regimen and the 2RHZE/4RH oral antituberculosis regimen in accordance with the recommendations of the literature [14,19,38], as in another study [23], because it was the first-line regimen recommended at the time in HIV-1 infected patients who represented the majority of our patients.
Evolutionary aspect: in our study, the death rate recorded among TB/HIV co-infected corroborates those of other similar studies [26,39], but lower than that of another similar study [23] and the death of patients was significantly linked to severe immunosuppression (CD4 count < 200>
Conclusion
The HIV infection increases the epidemiological data, modifies the diagnosis and increases the lethality of pulmonary tuberculosis, but it is not specific to all these variations due to the existence of other causes of qualitative immunosuppression and /or quantitative. A normal pleuropulmonary examination and/or a normal aspect of the chest radiography in an immunocompromised patient does not exclude active pulmonary tuberculosis. In TB/HIV co-infected, the more severe the immunosuppression, the worse the vital prognosis.
Conflict of interest:
The authors declare that they have no conflict of interest related to this article.
Author contributions
→ Design of the study, correction of the manuscript, critical contributions, supervision of the study and approval of the final version for publication: Mariam Soumaré
→ Design of the study, literature review, data analysis, drafting of the manuscript and approval of the final version for publication: Ouo – Ouo Loua
→ Drafting of the study protocol, literature review, data collection and analysis, and approval of the final version for publication: Zuride Ngueta Sabeya
→ Supervision of the study, critical contributions, correction of the manuscript and approval of the final version to be published: Jean Paul Dembélé, Assétou Fofana, Oumar Magassouba, Dramane Sogoba, Yacouba Cissoko, Issa Konaté and Sounkalo Dao.
References
- Ka D, Ndiaye R, Ndour CT, Mbaye Ndiaye N, Diouf A, et al. (2016), Radiological aspects of pulmonary tuberculosis in HIV-infected patients hospitalized at the Fann infectious and tropical diseases department in Dakar, Senegal. Med Afr Noire 63(5): 292-298
View at Publisher | View at Google Scholar - World Health Organization. Global tuberculosis report 2016. Geneva, Switzerland: World Health Organization
View at Publisher | View at Google Scholar - Lougue / Sorgho LC, Cisse R, Ouedraogo M, Koshinga BA, Kouanda S, et al. (2006), Radiological aspects of smear-positive pulmonary tuberculosis in adults in a country with a high tuberculosis/HIV prevalence. Sidanet 2(7): 810
View at Publisher | View at Google Scholar - Musafiri J, Mbayo PM, Bakaswa G, Kaswa M, Losimba Likwela J. (2013), Seroprevalence of HIV among tuberculosis patients in Kisangani in the Democratic Republic of Congo. San Publ Laxou. 25(4): 483-490
View at Publisher | View at Google Scholar - World Health Organization. Global tuberculosis report 2021. Geneva: World Health Organization
View at Publisher | View at Google Scholar - Okemba-Okombi FH, Itoua A, Bemba ELP, Ndion Gandzien J, Ossibi Ibara B, et al. (2015), Analysis of the report of the National Tuberculosis Control Program (PNLT-Congo) on tuberculosis/HIV co-infection. Rev Mal Respir 32(Supp): A211
View at Publisher | View at Google Scholar - Sylla A, Marchou B, Kassi N, Ello N, Aba T, et al. (2017), Tuberculosis/HIV co-infection: about 717 cases followed in an infectious disease’s unit in sub-Saharan Africa. Med Mal Infect; 47(Supp 4): S137-8
View at Publisher | View at Google Scholar - Glaziou P. (2009), The burden of tuberculosis in Africa and its international challenges. Thematic issue. Tuberculosis News. Bull Epidemiol Hebdom; 12(13): 221-224
View at Publisher | View at Google Scholar - Sangho O, Ouattara S, Telly N, Ballayira Y, Coulibaly CA, et al. (2021), Evaluation of the management of patients with drug-sensitive pulmonary tuberculosis at the Reference Health Center, Commune V of Bamako, 2015-2018. Rev Mal Infect Microbiol; 16(2): 26-31
View at Publisher | View at Google Scholar - Janah H, Souhi H, Kouismi H, Mark K, Zahraoui R, et al. (2014), Risk factors for mortality from pulmonary tuberculosis. Pan Afr Med J; 19:347
View at Publisher | View at Google Scholar - Loua OO, Ouedraogo D, Soumaré M, Allé Akakpo AE, Cissoko Y. (2022), Co-infection cerebral toxoplasmosis, miliary tuberculosis and HIV with CD4 count at 446 cells/mm3: an unusual observation. Ann Afr Med .15(4): e4839-4842
View at Publisher | View at Google Scholar - Ouedraogo M, Boncoungou K, Ouedraogo SM, Lougué C, Cissé R, et al. (2001). Tuberculous bacilliferous miliary: apropos of 44 cases. Med Afr Noire; 48(10): 419-422.
View at Publisher | View at Google Scholar - Nay N, Barbier F. (2017), Tuberculosis in intensive care patients. Med Intensive Rea; 26(3): 177-187.
View at Publisher | View at Google Scholar - Doctors Without Borders. HIV/TB Clinical Manual. 8th edition. 2015. South Africa: Doctor Without Borders
View at Publisher | View at Google Scholar - Kamamfu G, Nikoyagize E, Ndayirgije A, Mucikire E, Nzeyimana H, et al. (1990), Radiological aspects of pulmonary tuberculosis associated with human immunodeficiency virus (HIV) infection. Med Afr Noire; 37(10): 594-597.
View at Publisher | View at Google Scholar - Issa H, Cissoko Y, Soumaré M, Veltomtoh L, Loua O, et al. (2021), Concomitant pulmonary aspergillosis with tuberculosis and HIV immunosuppression, about a case in the Infectious Diseases Department of Point G University Hospital, Bamako-Mali. Jaccr Infectiol; 3(2): 1-5.
View at Publisher | View at Google Scholar - Dumas G, Bigé N, Lemiale V, Azoulay E. (2018), Immunocompromised patients, which pathogen for which immune deficiency? (Apart from HIV infection). Med Intensive Réa; 27(4): 344-366.
View at Publisher | View at Google Scholar - Bemba ELP, Bopaka RG, Moyikoua R, Ossibi-Ibara R, Ebenga-Somboko NB, et al. (2016), Pulmonary tuberculosis in Brazzaville in pneumological hospitalization: impact of late diagnosis of HIV infection on radiographic abnormalities. Pan Afr Med J ;24(259): 1‑8.
View at Publisher | View at Google Scholar - Harmouche H, Ammouri W. (2009), HIV-Tuberculosis co-infection. Rev Med Int; 30(S4): S273-276.
View at Publisher | View at Google Scholar - Kombila UD, Kane YD, Mbaye FBR, Diouf NF, Ka W, et al. (2018), Radiological particularities of microscopy-positive pulmonary tuberculosis in the Pneumology Department of the National University Hospital of FANN (CHNUF), Dakar (Senegal). Pan Afr Med J; 30:21.
View at Publisher | View at Google Scholar - International Union Against Tuberculosis and Lung Disease. (2019). Treatment of Tuberculosis. 7th edition. Paris: The Union
View at Publisher | View at Google Scholar - Samaké H, Cissé AB, Guindo I, Ongoïba S, Abdou M, et al. (2018), The challenges of implementing joint tuberculosis and HIV activities in the health districts of Bamako (Mali). Rev Mali Infect Microbiol; 11:4‑15..
View at Publisher | View at Google Scholar - Diarra S, Nasser MM, Konate I, Dembele M, Doucoure D, et al. (2019), HIV/Tuberculosis co-infection in the Infectious Diseases Department of the Center Hospitalier Universitaire du Point G: Epidemioclinical and therapeutic aspects about 48 cases. Health Sci Dis; 20(3): 11-13.
View at Publisher | View at Google Scholar - Ka D, Guéye NFN, Fall N, Touré-Badiane NO, Diop N, et al. (2017), Prevalence of tuberculosis/HIV co-infection in ARV-naïve patients followed at the Fann outpatient treatment center (CTA) in Dakar (Senegal). Med Health Too 27(4): 392-396.
View at Publisher | View at Google Scholar - Ammouri W, Akkaoui L, Harmouche H, Mezalek ZT, Adnaoui M, et al. (2009), Co-infection HIV - Tuberculosis. Morocco Med; 31(2): 91-9.
View at Publisher | View at Google Scholar - Fiogbé AA, Adjoh KS, Ouedraogo AR, Maïga AI, Wateba MI, et al. (2014), HIV/Tuberculosis co-infection in rural Benin: case of the Djougou-Ouake-Copargo health zone (North-West Benin). Mali Med; 29(1): 14-19.
View at Publisher | View at Google Scholar - Mbopi-Keou F-X, Nguefack-Tsague G, Kalla GCM, Abessolo SA, Angwafo F, et al. (2014), Risk factors for HIV infection in the Meyomessala health district in Cameroon. Pan Afr Med J; 18:161.
View at Publisher | View at Google Scholar - Dagnan NS, Tiembré I, Bénie Bi Vroh J, Diaby B, Zengbé-Acray P, et al. (2013), Seroprevalence of HIV infection in voluntary counseling and testing by mobile strategy in rural areas of Côte d'Ivoire. Public Health; 25(6): 849-856.
View at Publisher | View at Google Scholar - Tékpa G, Fikouma V, Téngothi RMM, Longo J de D, Woyengba APA, et al. (2019), Epidemiological and clinical aspects of tuberculosis in hospitals in Bangui. Pan Afr Med J; 33(31): 1‑12.
View at Publisher | View at Google Scholar - Eholie SP, Ehui E, Domoua K, Kakou A, Diarrassouba M, et al. (1999), Tuberculosis in the era of AIDS at the anti-tuberculosis center of Bouaké (Ivory Coast). Med Mal Infect; 29(2): 99-104.
View at Publisher | View at Google Scholar - Amat-Roze J-M. (2003), HIV/AIDS infection in sub-Saharan Africa, geographical considerations. Herodotus; 111(4): 117-155.
View at Publisher | View at Google Scholar - Anglaret X, Salamon R. (2004), AIDS epidemic in sub-Saharan Africa. Med Sci; 20(5): 593-598.
View at Publisher | View at Google Scholar - Afane Ze E, Guiedem E, Okomo Assoumou MC, Pefura Yone EW. (2013), Depressive impact of tuberculosis infection on immune defense cells. Health Sci Dis; 14(2): 1-5.
View at Publisher | View at Google Scholar - Diop SA, Massaly A, Ka D, Manga NM, Fortes-Déguénonvo L, et al. (2016), Use of the GeneXpert test for the diagnosis of tuberculosis in the infectious diseases department of the CHNU de Fann. Pan Afr Med J; 23(244): 1‑5.
View at Publisher | View at Google Scholar - Chauvet M, Wacker T. (1955), Tuberculous scar caves. RES; 12(4): 235-247.
View at Publisher | View at Google Scholar - Levy JA. (1993), Pathogenesis of human immunodeficiency virus infection. Microbiol Rev; 57(1): 183-289.
View at Publisher | View at Google Scholar - Tall F, Traoré A, Diallo I, Sanou I, Auregan G, et al. (2004), The determinants associated with “slow clinical progressors” in HIV infection in children in Burkina Faso. Mali Med; 19(2): 6‑11.
View at Publisher | View at Google Scholar - Padmapriyadarsini C, Narendran G, Swaminathan S. (2011), Diagnosis & treatment of tuberculosis in HIV co-infected patients. Indian J Med Res; 134(6): 850-865.
View at Publisher | View at Google Scholar - Kettani AE, Jebbar S, Takourt B, Maaloum F, Diraa O, et al. (2018), HIV co-infection in tuberculosis patients followed in the infectious diseases department of the CHU Ibn Rochd-Casablanca. Pan Afr Med J; 30:276.
View at Publisher | View at Google Scholar - Chakrabarti LA, Lortholary O. (2015), The IRIS - A paradoxical inflammatory response in patients treated concurrently for tuberculosis and HIV infection. Med Sci; 31(1): 53-59.
View at Publisher | View at Google Scholar
