

Case Report | DOI: https://doi.org/10.31579/2834-5118/035
Immediate Nipple Areolar Complex Reconstruction in A Patient With von Recklinghausen's Neurofibromatosis: A Clinical Case Report
- Iyadh Ghorbel
- Ghada Ben Othmane
- Amine Gargouri *
- Khelil Ennouri
University of Sfax,Tunisia
*Corresponding Author: Amine Gargouri, Biology Department, University of Sfax,Tunisia
Citation: Amine Gargouri. (2023). Immediate nipple areolar complex reconstruction in a patient with Von Recklinghausen's Neurofibromatosis: a clinical case report, International Journal of Clinical Surgery 2(3); DOI: 10.31579/2834-5118/035
Copyright: © 2023, Amine Gargouri, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 September 2023 | Accepted: 27 September 2023 | Published: 20 June 2023
Keywords: breast; neurofibromatosis; nipple; plastic surgery
Abstract
Von Recklinghausen's neurofibromatosis is an autosomal dominant condition commonly characterized by café au lait patches, axillary freckling, multiple neurofibromas, and Lisch nodules. In this context, we present a complex case involving a 32-year-old female who suffered from severe neurofibromatosis, leading to a significant impact on her bilateral nipple-areolar complexes. Furthermore, we illuminate the subsequent outcome of her immediate reconstruction procedure.
Introduction
Neurofibromatosis type 1 (NF1) is an autosomal dominant disorder, with an estimated incidence ranging from 1 in 2,500 to 1 in 3,000 [1], of which 50% of cases are sporadic [2]. Individuals with NF1 exhibit diverse manifestations, including café au lait spots, neurofibromas, intertriginous freckling, Lisch nodules, and bony dysplasia in long bones, all stemming from the deficiency of neurofibromin protein.
Neurofibromas in the breast are uncommun [3-5], particularly those affecting the nipple- areolar complex. This paper aims to present a case of a female patient with neurofibromas involving the nipple-areolar complex, while also discussing the surgical approach and the optimal timing for reconstruction.
Clinical Case
A 32-year-old woman diagnosed with NF1 based on the National Institutes of Health criteria
[6] was referred to our department due to the significant and deforming neurofibromatosis affecting both bilateral nipple-areolar complexes (fig1). Notably, there was no family history of NF1.
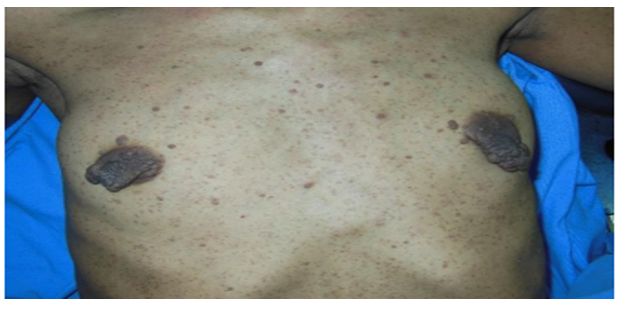
Upon examination, numerous cutaneous neurofibromas were evident across her chest and breasts, with particularly pronounced serpiginous, pedunculated neurofibromas on both sides. These lesions caused pain and protruded outward by 3 cm to 5 cm from the nippleand areola, resulting in deformity of both nipples. Over a span of two years, these neurofibromas had progressively increased in size.
The patient was significantly distressed by the disfigurement caused by these neurofibromas and actively sought their removal.Mammography revealed well-defined, dense, pedunculated nodulesoriginating from the areolar region.
In light of the clinical presentation, the decision was made to proceed with localized excision of the neurofibromas, coupled with minorplastic surgery interventions to restore symmetryto the areolar region. The nipples were reshaped using a CV flap technique, and the areola was reconstructed with a total skin graft (Figure 2).

Post-operatively, the patient experienced no complications and expressed satisfaction with the finalaesthetic outcome.
The histopathological examination verified the neural differentiation of spindle cells and the presence of Meissner corpuscles, demonstrating immunopositivity for S100. However, proliferation was observed to be negative for epithelial membrane antigen(EMA).
Discussion
Discussion
Neurofibromas occurring in the breast are exceedingly uncommon [3,4]. Only a limited number of reported cases have discussed treatment approaches, especially when these neurofibromas involve the nipple-areolar complex [5]. A study conducted by Freidrich et al, uncovered that tumor emerging in the areola and nipple region of NF1 patients, which resembled accessory nipples, were all identified as neurofibromas. This phenomenon was observed in both males and females, with occasional occurrences in children, showing a greater inclination for females to develop cutaneous neurofibromas in this particular location [3].
In general, neurofibromas tend to be asymptomatic; surgical intervention may be considered for cosmetic reasons when tumors reach a substantial size [7]. When these neurofibromas grow significantly and become unwieldy, they are characterized using terms such as "elephantiasis neuromatosa" or "fibroma pendulum" [4].
Therapeutic optionsinclude surgical excisionfor managing painfuland disfiguring lesions,as well as treatment using CO2 laser [8]. Previous reviews have showcased instances where surgical intervention was limited to localized removal of neurofibromas from the nipple area, involving procedures like nipple and areola reduction [3,4,9].
To our knowledge, this case report stands as the first documentation of immediate nipple reconstruction using a CV flap followingthe excision of neurofibromatous lesionsaffecting the nipple-areolar complex.
We performed a thorough excision of both nipple-areolar complexes, managing the resultant skin defect by utilizing purse-string sutures. Simultaneously, withinthe same surgicalsession,
we employed a CV technique to create the nipple and implemented a skin graft to reconstruct and restore the integrity of the areolar region.
Our patient reporteda high level of satisfaction following the surgery.
In cases similar cases, complete excision of neurofibromas coupled with reconstruction notonly ensures favorable aestheticoutcomes [10] but also servesas a safeguard against potentialsarcomatous transformation [11].
It's importantto acknowledge that NF1 patientsface an elevatedrisk of developing various benignand malignant neoplasms,including breast cancer [12-14].
There has been conjecture surrounding the possible effect of numerous neurofibromas within the breast and the nipple-areolar complex, which might inadvertently obscurethe detection of a breast mass during palpation, potentially leading to delayed clinical recognition [15-17]. In cases where a breast lesion is suspected in patients with NF1, it is recommended to undergo radiological imaging to gather additional diagnostic insights [7,18].
The breastholds significant importance within the framework of female identity.We firmly assert that preserving the nipple-areolar complex (NAC) is of utmost importance in the processof restoring a patient's body image [10,19].
Moreover, individuals with NF1, includingour patient, frequently encounter discrimination or rejection from society, and even within their own families. This can be attributed to the distressing appearance associated with NF1, as well as the potential presence of learning and behavioral disabilities that often accompany the condition [2,17]. In such cases, plastic surgery not only addresses the physical aspects but also offers a chance for these individuals to regain a sense of normalcyand social acceptance.
Conclusion
Our case of bilateral neurofibroma excision, which included the nipple-areolar complex, followedby immediate reconstruction in a femalediagnosed with NF1, remains an unusual occurrence in clinical practice.
The significance of plastic surgeryin the treatment of breast neurofibromas among NF1 patients cannot be overstated, as it plays a crucial role in preserving function and psychological equilibrium.
We advocate for an early and meticulous physical assessment, alongside the utilization of various imaging techniques for screening purposes, whenever any potentially concerningclinical indicators manifest in patients with NF1.
Author contributions
All authors contributed significantly and were in agreement with the content of the manuscript. All authors participated in data collection and in writing the manuscript.
Conflicts of Interest
No author has any financial or personal relations- hip with any person or organization that could inappropriately influence their work.
References
- Gutmann DH, Ferner RE, Listernick RH, Korf BR, Wolters PL, Johnson KJ. (2017). Neurofibromatosis type 1. Nat Rev Dis Primers. 23;3: 17004.
View at Publisher | View at Google Scholar - Ly KI, Blakeley JO. (2019). The Diagnosis and Management of Neurofibromatosis Type 1. Med Clin North Am. 103(6):1035-1054
View at Publisher | View at Google Scholar - Friedrich RE, Hagel C. (2010). Appendices of the nipple and areola of the breast in Neurofibromatosis type 1 patients are neurofibromas. Anticancer Res. 30(5):1815‑1817.
View at Publisher | View at Google Scholar - Hero E, Carey M, Hero I, Shaaban AM. (2018). Bilateral Neurofibromas of the Nipple-Areolar Complex: A Case Report and Approach to Diagnosis. Case Rep Pathol. 2018:6702561.
View at Publisher | View at Google Scholar - Lannon DA, Harris PA, Butler PEM. (2003). Treatment of severe neurofibromatosis of the nipple-areola complex. Plast Reconstr Surg. févr 111(2):952‑953.
View at Publisher | View at Google Scholar - Neurofibromatosis. Conference statement. National Institutes of Health Consensus Development Conference. Arch Neurol. mai 1988;45(5):575‑578.
View at Publisher | View at Google Scholar - Aljindan F, Aljehani L, Alsharif B, Mortada H. (2021). Management of Neurofibromatosis of the Nipple-Areolar Complex. Case Rep Surg. 2021:6622416.
View at Publisher | View at Google Scholar - Ostertag JU, Theunissen CCW, Neumann H a. M. (2002). Hypertrophic scars after therapy with CO2 laser for treatment of multiple cutaneous neurofibromas. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. mars;28(3):296‑298.
View at Publisher | View at Google Scholar - White CP, Martin S, Dal Cin A. (2012). Surgical treatment of areolar neurofibromas. Eur J Plast Surg. Août. 35(8):625‑627.
View at Publisher | View at Google Scholar - Satteson ES, Brown BJ, Nahabedian MY. (2017). Nipple-areolar complex reconstruction and patient satisfaction: a systematic review and meta-analysis. Gland Surg. févr;6(1):4‑13.
View at Publisher | View at Google Scholar - Waqar-uddin; Farooq Ahmad. (2007). Anjum Khawar. Recurrent neurofibroma in the head and neck. J Coll Physicians Surg Pak. Oct;17(10):629-631
View at Publisher | View at Google Scholar - Seo YN, Park YM. (2015). Association between Neurofibromatosis Type 1 and Breast Cancer: A Report of Two Cases with a Review of the Literature. Case Rep Med. 456205.
View at Publisher | View at Google Scholar - Seminog OO, Goldacre MJ. (2015). Age-specific risk of breast cancer in women with neurofibromatosis type 1. Br J Cancer. 28 avr 112(9):1546‑1548.
View at Publisher | View at Google Scholar - Da Silva AV, Rodrigues FR, Pureza M, Lopes VGS, Cunha KS. (2015). Breast cancer and neurofibromatosis type 1: a diagnostic challenge in patients with a high number of neurofibromas. BMC Cancer. 26 mars 15:183.
View at Publisher | View at Google Scholar - Bongiorno MR, Doukaki S, Aricò M. (2010). Neurofibromatosis of the nipple-areolar area: a case series. J Med Case Reports. 4:22.
View at Publisher | View at Google Scholar - Liu T, Liang Y, Lalwani SK, Zhang Y. (2023). Paget disease of the breast with underlying invasive ductal cancer in neurofibromatosis type 1: a case report. Transl Cancer Res. Mar 31;12(3):638-645
View at Publisher | View at Google Scholar - Zhou Y, Pan B, Mao F, Zhu Q, Huo Z, Wang H, et al. (2012). A hidden breast lump covered by nipple appendices in a patient with von recklinghausen disease: a case report and review of the literature. Clin Breast Cancer. févr 12(1):71‑75.Nasri S, Benmoussa Y, Abbou W, Mirali H, Aichouni N, Skiker I. (2021). Imaging appearance of isolated diffuse neurofibroma of nipple areolar area: a case report. Pan Afr Med J. 7;39:178.
View at Publisher | View at Google Scholar - Lee JS, Eom JR, Lee JW, Choi KY, Chung HY, Cho BC, et al. (2019). Safe delayed procedure of nipple reconstruction in poorly circulated nipple. Breast J. janv;25(1):129‑133.
View at Publisher | View at Google Scholar
