

Research Article | DOI: https://doi.org/10.31579/2834-5010/002
Hypertonic Sodium Therapy of 5%Nacl and 8.4%Naco3 for Acutely Ill and Shocked Patients
- Ahmed N Ghanem *
* NHS The UK and Mansoura University, Faculty of Medicine Egypt.
*Corresponding Author: Ahmed N Ghanem. NHS The UK and Mansoura University, Faculty of Medicine Egypt.
Citation: Ahmed N Ghanem (2022). Hypertonic Sodium Therapy Of 5%Nacl And 8.4%Naco3 for Acutely Ill and Shocked Patients. International Journal of Clinical Therapeutics. 2(2); DOI:10.31579/2834-5010/002
Copyright: © 2022 Ahmed N Ghanem, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 September 2022 | Accepted: 14 September 2022 | Published: 01 March 2023
Keywords: hypertonic sodium therapy; hyponatraemia; hyper-volumetric
Abstract
Fluid resuscitation using hypertonic saline results in volume expansion and less total infusion volume. It is a lifesaving therapy in many acute clinical conditions. This may be of interest in oedematous patients with intravascular volume depletion. When such strategies are employed, renal effects may differ markedly according to prior intravascular volume status. In hyper-volumetric states with depleted intravascular volume, hypertonic sodium therapy of 5% NaCl and 8.4% NaCo3 turns it into hypervolaemia with massive diuretic effect. Hypertonic saline induced changes in serum osmolality and sodium return to baseline within a limited period. Sparse evidence indicates that resuscitation with hypertonic saline results in less perioperative complications, ICU days and mortality in selected patients. In conclusion, the use of hypertonic saline may have beneficial features in selected critically ill patients when carefully chosen. Hypertonic sodium therapy of 5% NaCl and 8.4% NaCo3 has proved lifesaving in treating the TUR syndrome, hyponatraemia and ARDS. Further clinical studies assessing relevant clinical outcomes are warranted.
Introduction
Clinicians use hypertonic fluids to increase intravascular fluid volume and restore blood pressure. Hypertonic saline can be utilized in the treatment of hyponatremia. Hypertonic saline and mannitol are both indicated to reduce intracranial pressure.
Hypertonic saline is a crystalloid intravenous fluid composed of NaCl dissolved in water with a higher sodium concentration than normal blood serum. Both 3% and 5% hypertonic saline (HS) is currently FDA-approved for use in hyponatremia and increased intracranial pressure (ICP). Patients with hyponatremia with severe features should have their serum sodium gradually corrected with boluses of hypertonic saline. Patients should have their serum sodium monitored at regular intervals and can receive multiple boluses a day.[1]
Hypertonic Saline:
In patients with severe hyponatremia, serum sodium should undergo correction by 4 to 6 mEq/L per day, which can be achieved with 100 mL boluses of 3% HS at 10-minute intervals up to three total boluses. Some authorities recommend up to 8 mEq/L per day.[9] Less severe hyponatremia can achieve control with enough hypertonic saline to manage symptoms.[10] Due to the insufficient number of patients over age 65 in various trials, hypertonic fluids should start at the lowest ends of the dosing scale in the geriatric population. Pediatric traumatic brain injury generally receives treatment with a 6.5 to 10 mL/kg bolus of hypertonic saline.[11] Administration via a peripheral intravenous catheter is acceptable if no other access is available, but central venous access is the preferred route.
Recent evidence on the use of hypertonic sodium therapy (HST) of 5%NaCl and 8.4%NaCo3
Hypertonic sodium therapy (HST) of 5%NaCl and 8.4%NaCo3 has proved lifesaving for treating the acute severe cases of the TUR syndrome, acute dilutional hyponatraemia and the acute respiratory distress syndrome (ARDS).
This HST was used successfully in treating the TUR syndrome, acute dilutional hyponatraemia of <120>
The treatment was given in bolus therapy of 200 ml alternating both fluids given over a period of 10 minutes and repeated after rechecking serum sodium monitored by clinical improvement and urine output [15]. More than 4 L of urine was excreted by the end of one hour period of treatment matching a remarkable clinical recovery from shock and coma. The effect of hypertonic sodium infusion on serum sodium and osmolality are shown in (Figure 1).
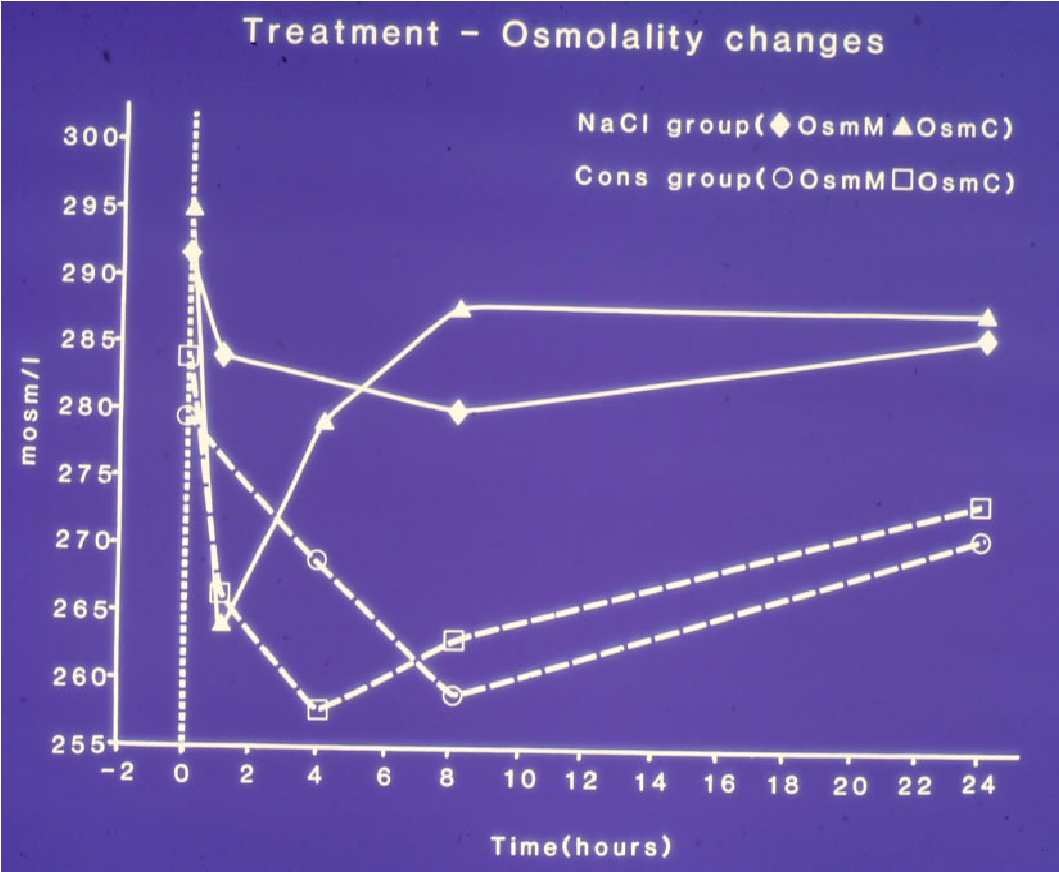
Figure: shows mean changes in measured serum osmolality (OsmM) and calculated osmolality (OsmC) in patients with the TURP syndrome comparing those infused with 5% hypertonic sodium (solid lines) and those treated conservatively (slashed lines). OsmC was calculated from the formula 2xNa+urea+glucose in mmol/l of serum concentration48 thus reflecting changes in serum sodium concentration. The vertical dotted line represents the start of operation (Time B) followed by C, C1, C2 (end of treatment) and D, respectively.
Conclusion
Fluid resuscitation using hypertonic saline results in volume expansion and less total infusion volume. This may be of interest in oedematous patients with intravascular volume depletion. When such strategies are employed, renal effects may differ markedly according to prior intravascular volume status. Hypertonic saline induced changes in serum osmolality and electrolytes return to baseline within a limited period. Sparse evidence indicates that resuscitation with hypertonic saline results in less perioperative complications, ICU days and mortality in selected patients. In conclusion, the use of hypertonic saline may have beneficial features in selected critically ill patients when carefully chosen. Further clinical studies assessing relevant clinical outcomes are warranted.
Conflict of interest
None
Funds Received:
None
References
- Williams DM, Gallagher M, Handley J, Stephens JW. (2016) The clinical management of hyponatraemia. Postgrad Med J. Jul;92(1089):407-411.
View at Publisher | View at Google Scholar - Sokhal N, Rath GP, Chaturvedi A, Singh M, Dash HH. (2017) Comparison of 20% mannitol and 3% hypertonic saline on intracranial pressure and systemic hemodynamics. J Clin Neurosci. 42:148-154.
View at Publisher | View at Google Scholar - Oddo M, Levine JM, Frangos S, Carrera E, Maloney-Wilensky E (2009) Effect of mannitol and hypertonic saline on cerebral oxygenation in patients with severe traumatic brain injury and refractory intracranial hypertension. J Neurol Neurosurg Psychiatry. 80(8):916-920.
View at Publisher | View at Google Scholar - Witherspoon B, Ashby NE. (2017) The Use of Mannitol and Hypertonic Saline Therapies in Patients with Elevated Intracranial Pressure: A Review of the Evidence. Nurs Clin North Am. Jun;52(2):249-260.
View at Publisher | View at Google Scholar - Honore PM, Barreto Gutierrez L, Spapen HD. (2019) Renal protection in sepsis: Is hypertonic sodium (lactate) the solution? Ann Intensive Care. Feb 08;9(1):28. [PMC free article]
View at Publisher | View at Google Scholar - Pfortmueller CA, Schefold JC. Hypertonic saline in critical illness - A systematic review. J Crit Care. 2017 Dec;42:168-177.
View at Publisher | View at Google Scholar - Joseph B, Aziz H, Snell M, Pandit V, Hays D, Kulvatunyou N, Tang A, O'Keeffe T, Wynne J, Friese RS, Rhee P. (2014) The physiological effects of hyperosmolar resuscitation: 5% vs 3% hypertonic saline. Am J Surg208(5):697-702.
View at Publisher | View at Google Scholar - Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000 May 25;342(21):1581-1589.
View at Publisher | View at Google Scholar - Sterns RH. Disorders of plasma sodium--causes, consequences, and correction. N Engl J Med. 2015 Jan 01;372(1):55-65. 3
View at Publisher | View at Google Scholar - Mason A, Malik A, Ginglen JG. (2021) Hypertonic Fluids. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; StatPearls Publishing LLC.
View at Publisher | View at Google Scholar - Niknam K, Mistry R, Lumba-Brown A. (2019) Pediatric hypertonic saline use in emergency departments. Am J Emerg Med. 37(5):981-983.
View at Publisher | View at Google Scholar - Ghanem KA and Ghanem AN. (2017) Volumetric overload shocks in the patho-aetiology of the transurethral resection prostatectomy syndrome and acute dilution hyponatraemia: The clinical evidence based on 23 case series. Basic Research Journal of Medicine and Clinical Sciences ISSN 2315-6864 Vol. 6(4): pp. 35-43 April
View at Publisher | View at Google Scholar - Ghanem AN, Ward JP. (1990) Osmotic and metabolic sequelae of volumetric overload in relation to the TURP syndrome. Br J Uro.; 66: 71-78.
View at Publisher | View at Google Scholar - Ghnem AN. (2020) Volume Kinetic Shocks in Surgical Practice. J Emerg. Med Trauma Surg. Care 2: 010.
View at Publisher | View at Google Scholar - Ghanem AN. (2018) Therapy of Hyponatremia: End of Era or Minority Report? Biomed J Sci & Tech Res 11(4). BJSTR. MS.ID.002130.
View at Publisher | View at Google Scholar
