

Research Article | DOI: https://doi.org/10.31579/2834-796X/077
Hyperbilirubinemia and Hepatic Dysfunction in Patients Undergoing Cardiac Surgery: Predictors and Outcome - A single Centre Prospective Study
- Kumar Rahul 1
- Bhupendra Kumar 1
- Vivek Tewarson 1
- Sarvesh Kumar 1
- Mohammad Zeeshan Hakim 1
- Vandana Chaudhary 2
- Sushil Kumar Singh 1*
1 Department of cardiovascular and thoracic surgery, King George’s Medical University, Lucknow, India.
2 Department of Physiology, King George’s Medical University, Lucknow, India.
*Corresponding Author: Sushil Kumar Singh, MCh, Professor, Department of Cardiovascular and Thoracic Surgery, King George’s Medical University, Lucknow.
Citation: Kumar Rahul, Bhupendra Kumar, Vivek Tewarson, Sarvesh Kumar, Mohammad Z. Hakim, et al, (2024), Hyperbilirubinemia and hepatic dysfunction in patients undergoing cardiac surgery: Predictors and outcome- A single centre prospective study, International Journal of Cardiovascular Medicine, 3(5); DOI:10.31579/2834-796X/077
Copyright: © 2024, Sushil Kumar Singh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 August 2024 | Accepted: 30 August 2024 | Published: 18 September 2024
Keywords: hyperbilirubinemia; hepatic dysfunction; cardiac surgery.
Abstract
Background: We aim to assess the incidence and perioperative risk factors for hyperbilirubinemia and hepatic dysfunction after cardiac surgery and determine its influence on early operative outcome.
Methods: This prospective observational study was conducted on 485 patients who underwent cardiac surgical procedures from June 2022 to October 2023. Postoperative hyperbilirubinemia was defined as serum total bilirubin >2.0 mg/dl.
Results: The overall incidence of post operative hyperbilirubinemia was 24.5% (119 patients). Total and indirect bilirubin, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase was measured preoperatively and at day 1, day 2 and day 5. Patients undergoing valve repair or replacement had the highest incidence of hyperbilirubinemia (37.1%), followed by coronary artery bypass grafting with concomitant valve surgery (35.3%), congenital heart surgery (24.5%), and coronary artery bypass alone (12.4%). Post operative hyperbilirubinemia was associated with increased duration of inotropic support (p=0.0001), mechanical ventilation (p=0.0001), intensive care unit stay (p=0.001), hospital stay (p=0.006), and mortality (p=0.014). The perioperative factors associated with postoperative hyperbilirubinemia were increased preoperative bilirubin level (p<0.0001), preoperative prothrombin time (p<0.0001), cardiopulmonary bypass time (p=0.026), aortic cross clamp time (p=0.004), and blood transfusion units (p=0.0001).
A significant increase of total bilirubin, aspartate aminotransferase, and alkaline phosphatase were noted in the second postoperative day. Significant relation was seen between hypotension and alkaline phosphatase, and aspartate aminotransferase change but hypothermia had not affected alanine aminotransferase, total bilirubin and indirect bilirubin change.
Conclusions: Post operative hyperbilirubinemia is seen in patients undergoing cardiopulmonary bypass and is associated with high hospital mortality. The factors associated with its occurrence are increased preoperative bilirubin level, preoperative prothrombin time, cardiopulmonary bypass time, aortic cross clamp time, and blood transfusion units. Persistent hyperbilirubinemia is associated with a worse outcome than early transient hyperbilirubinemia.
Introduction:
Early transient hyperbilirubinemia after cardiac surgery is well documented. The incidence of hyperbilirubinemia and hepatic injury is reported to be 10%–40% in various studies, and it has been associated with postoperative morbidity and mortality [1–3]. Even in the present era with improved extracorporeal circulation techniques, myocardial protection strategies, anaesthetic management and improved intensive care, postoperative hyperbilirubinemia with hepatic dysfunction is a common occurrence. Several factors have been documented for hepatic injury that includes systemic inflammatory response syndrome and oxidative stress [4]. However, several studies exhibits that most of these pathophysiologic mechanisms are based on centrilobular sinusoid ischemia and subsequent reperfusion injuries [5]. Some trials have shown that the consumption of coagulation factors during CPB leads to reduced coagulation factors and compromised liver function by micro thrombi formation in centrilobular hepatic sinusoids [6].
The careful recent medical literature review revealed that most studies have been focused on methods to protect organs from adverse effect of CPB; however, most of these studies missed evaluation of the liver function and focused on organs such as heart, lung and kidney. This study aimed to assess the incidence and pattern of postoperative hyperbilirubinemia and other liver enzymes and its influence on early operative outcome in terms of morbidity and mortality. We also aim to identify the perioperative factors associated with the development of postoperative hyperbilirubinemia and hepatic injury.
Patients and methods:
This is a prospective study conducted in Department of CVTS at the King George’s medical university from June 2022 to October 2023. The study was approved by institute ethics committee. Total 485 consecutive patients for cardiac surgery in the study period were enrolled, irrespective of their cardiac disease.
Inclusion criteria: All cardiac surgery patients of both genders.
Exclusion criteria:
1) Patients undergoing emergency surgery
2) Patients with sepsis
3) Patients with cerebrovascular accidents.
4) Patients with active hepatitis
The ages of the patients in the study group ranged from 5 years to 75 years, and it included both sexes. Postoperative hyperbilirubinemia was defined as total serum bilirubin >2.0mg dl/Lt. The patients were divided into two groups according to their postoperative bilirubin level. Normal ranges of the study parameters were: Serum total bilirubin: 0.1–1.0 mg/dL; Prothrombin time 9.5–13.8 sec; Aspartate transaminase (SGOT): 4–48 U/L and Alanine transaminase (SGPT): 7–55 U/L. All relevant preoperative details such as age, sex and preoperative diagnosis were recorded. Blood investigations and echocardiography were carried out on the day before surgery.
The various surgical procedures were coronary artery bypass grafting (CABG), valve repair or replacement, congenital heart surgery, and CABG with concomitant valve surgery. All operations were conducted as per the institute protocols for surgery and anaesthesia. The duration of surgery, cardiopulmonary bypass (CPB), and aortic cross clamping, and the blood transfusion details were recorded. Blood transfusion was carried out according to the institutional protocol. All patients were monitored for arterial pressure, central venous pressure, oxygen saturation and urine output. Blood transfusion shortly after surgery and intraaortic balloon pump usage was recorded. Duration of inotropic support, mechanical ventilation, and intensive care unit stay were recorded. Blood investigations were carried out on the first, second, and fifth postoperative day. Statistical analysis was carried out using SPSS version 10.0 software (SPSS, Inc., Chicago, IL, USA). The chi-square test and independent sample t test were used to compare categorical and continuous variables, respectively. Data are presented as mean standard deviation or proportions, as appropriate. A p-value less than 0.05 was considered significant.
Results:
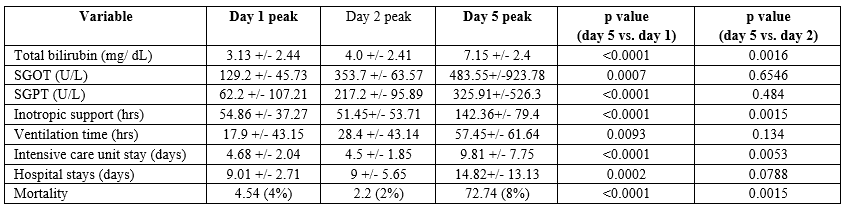
The overall incidence of post operative hyperbilirubinemia was 24.5% (119 patients). The incidence of hyperbilirubinemia was higher in patients who underwent mechanical valve replacement compared to bioprosthetic valve replacement or valve repair. None of the patients who underwent valve replacement developed a paravalvular leak. Off-pump procedures were used in 95 (19.5%) patients, the majority of off-pump procedures (17.5%, 85 patients) were for CABG. The incidence of postoperative hyperbilirubinemia was not significantly higher in on-pump CABG (5.2.0%) compared to off pump CABG (17.5%; p=0.9461). This might be because of disproportionate sample sizes between these groups; almost all isolated CABG operations were performed off-pump whereas on-pump CABG was associated with mitral valve surgery, and many on-pump CABG operations were emergency procedures which were excluded from the study. The perioperative factors contributing to postoperative hyperbilirubinemia were increased preoperative bilirubin level (p less than 0.0001), preoperative prolonged prothrombin time (p less than 0.0001), longer CPB time (p=0.026), longer aortic cross clamp time (p=0.002), and number of blood transfusion units (p=0.0001; Table 1). Patients with hyperbilirubinemia had increased postoperative morbidity and mortality (Table 2). Among the 16 patients who died in the normal bilirubin group, 6 (37.5%) died of a cardiac cause, 4 (25.0%) died of sepsis, and 3 (18.75%) died of a respiratory cause. None of the patients died of liver failure. Postoperative hyperbilirubinemia is associated with concomitant increases in aspartate transaminase and alanine transaminase levels. We noted significant increases in morbidity and mortality as the peak levels of serum total bilirubin, aspartate transaminase, and alanine transaminase were reached on or after the 5th postoperative day (Table 3,). In the hyperbilirubinemia group, 75 patients (63.0%) had peak levels of on the first postoperative day, 24 (20.1%) on the 2nd postoperative day and 20 (16.8%) on 5th postoperative day. Of the 21 patients in the hyperbilirubinemia group who died, 12 had peak bilirubin levels on the 2nd postoperative day and the cause of death was low cardiac output syndrome. The other 4 patients had peak bilirubin levels on the 5th postoperative day and among them, 3 died of multiorgan dysfunction 5 days after surgery, and 2 died of liver failure 10 days after surgery.
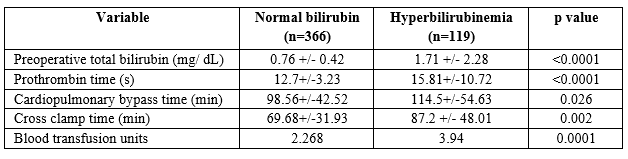
Table 1. Perioperative risk factors for postoperative hyperbilirubinemia
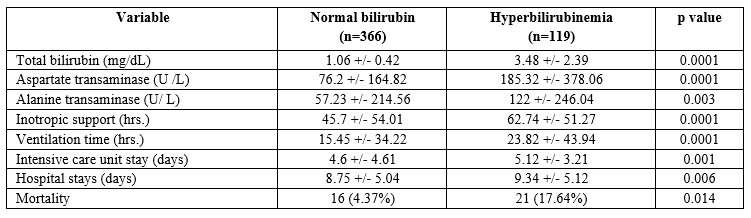
Table 2. Outcomes of cardiac surgery in 485 patients.
SGOT: serum glutamic oxaloacetic transaminase; SGPT: serum glutamic pyruvic transaminase.
Table 3. Outcome according to the day of peak bilirubin level.
Discussion:
The pathogenesis of liver dysfunction after cardiac surgery is multi-factorial. Despite demonstrable improvements in all aspects of surgical and perioperative care over the last decade, hepatic dysfunction remains a serious postoperative complication [7,8]. Study by Varghese et al. stated that alterations in hepatic blood flow to be a major factor in pathogenesis of postoperative hepatic function dysfunction. It has also been proposed that factors related to CPB such as activation of inflammatory system pose an additional risk for hepatic dysfunction [9]. In our study, the incidence of postoperative hyperbilirubinemia was 25%, which is similar to data reported previously. Hyperbilirubinemia and hepatic dysfunction can occur after CPB due to haemolysis caused by cardiotomy suction, the membrane oxygenator, and various other elements of CPB [10,11].
Liver cell damage can occur due to the non-pulsatile flow in CPB and its associated risk of regional malperfusion causing ischemic damage [12]. Haemodilution caused by CPB reduces tissue oxygen delivery, adding to the ischemic insult. The important tenets to be followed during CPB to prevent organ damage are maintaining adequate mean arterial pressure (>50 mm Hg), systemic flow rate, haematocrit (>24%), and tissue oxygen delivery (>300mL/min/m2) [13/10]. In our study, pump time has significant effect on hepatic function tests via hypothermia or hypotension (Table 3). Normothermic CPB does not lead to a significant or prolonged reduction of liver function but causes an increase of gastrointestinal permeability. The increased gastrointestinal permeability caused sepsis and multi organ failure [14]. Hypothermic CPB may benefit the hepatic circulation, although the additional advantages usually gained by the use of pulsatile perfusion may be partly lost when hypothermia is combined with a high pump flow rate. In our study, hypothermia significantly affected total bilirubin and alkaline phosphates levels on third post operative day. Results of our study showed that most sensitive test for postoperative evaluation of hepatic function in hypothermic and normothermic CPB is AST and ALT consequently. In our study, the perioperative factors significantly associated with postoperative hyperbilirubinemia and deranged hepatic enzymes were preoperative total bilirubin levels, preoperative prothrombin time, CPB time, aortic cross clamp time and volume of blood transfused. Our study found that patients with preoperative bilirubin >2mg/dL had an 85% incidence of postoperative hyperbilirubinemia with hepatic dysfunction. In Wang study, predictors of possible risk factors for postoperative hyperbilirubinemia were the numbers of replaced valves, raised preoperative right atrial pressure, and preoperative TB concentration [15]. We believe that high right atrial pressure in study by Wang caused hepatic congestion and centrilobular cell necrosis and jaundice leading to raised bilirubin and deranged hepatic enzymes.
Patients with congestive heart failure have congestive hepatomegaly and are at risk of developing postoperative hyperbilirubinemia [16]. Preoperative optimization such as treating anaemia and congestive heart failure will reduce the incidence of postoperative hyperbilirubinemia. Investigating patients with preoperative total bilirubin >2mg/dL for hepatic pathology and treating it before surgery should be routine. Persistent hyperbilirubinemia and deranged hepatic enzymes increase postoperative morbidity and mortality. It indicates serious underlying conditions such as persistent low cardiac output syndrome or sepsis, rather than being a direct causative factor for morbidity and mortality. Mechanical ventilation time, intensive care unit stay, and hospital stay were significantly longer in the hyperbilirubinemia group, which is comparable to the results of McSweeney and colleagues [17]. Similar results were demonstrated in our study. Transient postoperative high hepatic enzymes levels also may be seen in massive transfusion associated with low cardiac output. Prolonged low cardiac output, which may compromise the hepatic blood flow, caused alterations in the microcirculation. In our study, significant mortality was observed in patients with postoperative hyperbilirubinemia (17.6%) compared to those with normal bilirubin levels (4.3%). The management of patients with postoperative hyperbilirubinemia is watchful observation for acute liver failure, sepsis, or multiorgan dysfunction syndrome, because the majority of cases of isolated hyperbilirubinemia improve over time. Hepatotoxic drugs should be discontinued. Propofol and benzodiazepines can be used for sedation, and morphine is better avoided. Boluses of fentanyl, remifentanil, or sufentanil are more suitable for pain relief. Hemodynamics should be optimized to ensure adequate mean arterial pressure. These patients will have low systemic vascular resistance, and vasopressors might be required to maintain adequate systemic perfusion pressures. Noradrenalin is preferred over vasopressin or terlipressin which may accelerate development of cerebral oedema and worsen splanchnic vasoconstriction [18]. Bilirubin levels and liver enzyme levels increase transiently in many patients undergoing extracorporeal circulation, and normalize within one or two days. Our study shows that the majority of patients with hyperbilirubinemia had peak bilirubin levels within two days of surgery. Persistent and rising levels of bilirubin after surgery may precede the development of liver failure which is associated with increased morbidity and mortality. In our study, patients with persistently elevated or peak levels of bilirubin 5 days after surgery developed liver failure and associated multiorgan dysfunction syndrome, with increased mortality (72.7%). Similarly increased mortality due to persistent hyperbilirubinemia has been observed in other studies [19,20,21,23]. Persistent hyperbilirubinemia with deranged hepatic enzymes leading to liver failure is an ominous condition with limited therapeutic options. Drugs such as lactulose and Hepa-Merz, and a high carbohydrate diet are used to prevent encephalopathy.
Intermittent peritoneal dialysis, hemodialysis, and plasmapheresis have been reported anecdotally [16,18,19]. Newer innovations such as molecular adsorbent recirculation system and fractionated plasma separation and adsorption have shown promising results in nonsurgical and noncardiac surgical patients [22]. Persistent hyperbilirubinemia in postcardiac surgical patients carries a grave prognosis, and all measures should be taken to prevent it. We further need a more prospective randomized study with detailed and serial postoperative investigatory tools to know more about the etiology of hyperbilirubinemia and its effects in postoperative cardiac surgical patients. However, we concluded that postoperative hyperbilirubinemia is common in patients undergoing extracorporeal circulation and is associated with high morbidity and mortality. Factors involved in causing postoperative hyperbilirubinemia are increased preoperative total bilirubin levels, preoperative prolonged prothrombin time, prolonged CPB time, prolonged aortic cross-clamp time, and more blood transfusions. Persistent hyperbilirubinemia 5 days after surgery should alarm the surgeon of impending liver failure.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Collins JD, Bassendine MF, Ferner R, et al. Incidence and prognostic importance of jaundice after cardiopulmonary bypass surgery. Lancet 1983; 1: 1119–1123.
View at Publisher | View at Google Scholar - Wang MJ, Chao A, Huang CH, et al. Hyperbilirubinemia after cardiac operation. J Thorac Cardiovasc Surg 1994;108: 429–436.
View at Publisher | View at Google Scholar - Chu CM, Chang CH, Liaw YF and Hsieh MJ. Jaundice after open-heart surgery: a prospective study. Thorax 1984; 39: 52–56.
View at Publisher | View at Google Scholar - Wark HJ. Hepatic failure after cardiopulmonary bypass is unlikely to be isoflurane hepatitis. Anesthesiology 2002; 97: 1323-1324.
View at Publisher | View at Google Scholar - Hayashida N, Shoujima T, Teshima H, et al. Clinical outcome after cardiac operations in patients with cirrhosis. Ann Thorac Surg 2004; 77: 500-5.
View at Publisher | View at Google Scholar - Varghese D, Varghese B, Kelley K, et al. Prospective randomized study to evaluate changes in alpha-GST as a novel marker of hepatocellular necrosis in patients at high-risk of hepatic injury undergoing coronary revascularization with and without cardiopulmonary bypass. Ind J Thorac Cardiovasc Surg 2007; 23: 63.
View at Publisher | View at Google Scholar - Olsson R, Hermodsson S, Roberts D and Waldenstrom J. Hepatic dysfunction after open-heart surgery. Scand J Thorac Cardiovasc Surg 1984; 18: 217–222.
View at Publisher | View at Google Scholar - Michalopoulos A, Alivizatos P and Geroulanos S. Hepatic dysfunction following cardiac surgery: determinants and consequences. Hepatogastroenterology 1997; 44: 779–783.
View at Publisher | View at Google Scholar - Farag M, Veres G, Szabó G, Ruhparwar A, Karck M, Arif R. Hyperbilirubinaemia after cardiac surgery: the point of no return. ESC Heart Fail. 2019 Aug;6(4):694-700.
View at Publisher | View at Google Scholar - Gregoretti S. Suction-induced hemolysis at various vacuum pressures: implications for intraoperative blood salvage. Transfusion 1996; 36: 57–60.
View at Publisher | View at Google Scholar - Garcia MJ, Vandervoort P, Stewart WJ, et al. Mechanisms of hemolysis with mitral prosthetic regurgitation study using transesophageal echocardiography and fluid dynamic simulation. J Am Coll Cardiol 1996; 27:399–406.
View at Publisher | View at Google Scholar - Hornick P and Taylor K. Pulsatile and non-pulsatile perfusion: the continuing controversy. J Cardiothorac Vasc Anesth 1997; 11: 310–315.
View at Publisher | View at Google Scholar - Laupacis A, Fergusson D. Drugs to minimize perioperative blood loss in cardiac surgery: metaanalysis using perioperative blood transfusion as the outcome. Anesth Analg 1997; 85: 1258-67.
View at Publisher | View at Google Scholar - Sabzi F, Faraji R. Liver Function Tests Following Open Cardiac Surgery. J Cardiovasc Thorac Res. 2015;7(2):49-54.
View at Publisher | View at Google Scholar - Wang MJ, Chao A, Huang CH, et al. Hyperbilirubinemia after cardiac operation. Incidence, risk factors, and clinical significance. J Thorac Cardiovasc Surg 1994; 108: 429-36.
View at Publisher | View at Google Scholar - Kraev AI, Torosoff MT, Fabian T, Clement CM, Perez-Tamayo RA. Postoperative hyperbilirubinemia is an independent predictor of long-term outcomes after cardiopulmonary bypass. J Am Coll Surg 2008; 206: 645–653.
View at Publisher | View at Google Scholar - McSweeney ME, Garwood S, Levin J, et al. Adverse gastrointestinal complications after cardiopulmonary bypass: can outcome be predicted from preoperative risk factors? Anesth Analg 2004; 98: 1610–1617.
View at Publisher | View at Google Scholar - Schilsky ML, Honiden S, Arnott L and Emre S. ICU management of acute liver failure. Clin Chest Med 2009; 30: 71–87.
View at Publisher | View at Google Scholar - Kraev AI, Torosoff MT, Fabian T, Clement CM, Perez-Tamayo RA. Postoperative hyperbilirubinemia is an independent predictor of long-term outcomes after cardiopulmonary bypass. J Am Coll Surg 2008; 206:645–653.
View at Publisher | View at Google Scholar - Mastoraki A, Karatzis E, Mastoraki S, Kriaras I, SfirakisP, Geroulanos S. Postoperative jaundice after cardiac surgery. Hepatobiliary Pancreat Dis Int 2007; 6: 383–387.
View at Publisher | View at Google Scholar - Arias JI, Aller MA and Arias J. Surgical inflammation: a pathophysiological rainbow. J Transl Med 2009; 7: 19.
View at Publisher | View at Google Scholar - Sauer IM, Goetz M, Steffen I, et al. In vitro comparison of the molecular adsorbent recirculation system (MARS) and single-pass albumin dialysis (SPAD). Hepatology 2004; 39: 1408–1414.
View at Publisher | View at Google Scholar - Raveendran D, Penny-Dimri JC, Segal R, Smith JA, Plummer M, Liu Z, Perry LA. The prognostic significance of postoperative hyperbilirubinemia in cardiac surgery: systematic review and meta-analysis. J Cardiothorac Surg. 2022 May 26;17(1):129.
View at Publisher | View at Google Scholar
