

Research article | DOI: https://doi.org/10.31579/ 2834-5126/011
Heterogeneity Of Renal Pathogenicity on The Background of Asymptomatic Hyperuricemia in Patients with Dual Metabolic Syndrome Diseases (Essential Hypertensive Disease and Type 2 Diabetes Mellitus)
Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine
*Corresponding Author: A.O. Ikwuka Mohiuddin, Alumni, Faculty of Pharmacy, Dhaka University
Citation: A.O. Ikwuka. (2023). Heterogeneity Of Renal Pathogenicity on The Background of Asymptomatic Hyperuricemia in Patients with Dual Metabolic Syndrome Diseases (Essential Hypertensive Disease and Type 2 Diabetes Mellitus). Clinical trials and clinical research. 2(1); Doi: 10.31579/ 2834-5126/011
Copyright: © 2023 A.O. Ikwuka, this is an open access article distributed under the creative common’s attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 November 2022 | Accepted: 15 December 2022 | Published: 02 January 2023
Keywords: heterogeneity, renal pathogenicity, asymptomatic hyperuricemia, metabolic syndrome diseases, essential hypertensive disease, type 2 diabetes mellitus
Abstract
Introduction: Asymptomatic hyperuricemia is believed to be more severe and more common in patients with dual metabolic syndrome diseases (essential hypertensive disease (EHD) and type 2 diabetes mellitus (T2DM)) and comparatively less severe and less common in patients with either of these dual metabolic syndrome diseases.
Aim: To determine the heterogeneity of renal pathogenicity on the background of asymptomatic hyperuricemia in the clinical course of EHD combined with T2DM using correlations between uric acid levels in the blood, systolic blood pressure levels, glycated hemoglobin, dyslipidemia, inflammatory processes, kidney damage, etc.
Materials and methods: The research included 105 patients (50 males and 55 females), aged 41-70 years, average age being (54.2±4.0) years. Patients were divided into 3 groups: Group I (GI) consisted of 25 patients with treatment-compensated EHD, 1–2-degree, stage II; Group ІІ (GII) was made up of 25 patients with subcompensated T2DM (glycated hemoglobin (HbA1C) - from 7.0 to 11.0%); Group III (GIII) had 55 patients with EHD, 1–2-degree, stage ІІ combined with subcompensated T2DM. Control group consisted of 15 practically healthy volunteers, 10 (66.7%) females and 5 (33.3%) males, aged (54.6±4.2) years. Groups were randomized according to age, sex, BMI, duration of EHD and T2DM. In addition to general clinical examination conducted; blood levels of uric acid (UA), lipids, tumour necrosis factor alpha (TNF-α), high-sensitivity C-reactive protein (hs-CRP) were determined. Urine levels of neutrophil gelatinase-associated lipocalin (NGAL) was also determined using immuno-fermentation methods.
Results: Asymptomatic hyperuricemia characterized by an increase in blood uric acid level of more than 410 μmol/l was observed in 34.6% of GI patients, in 21.8% of GII patients and most commonly in 55.7% of GIII patients with EHD combined with T2DM. Correlations between blood uric acid level with albuminuria was found (r=+0.42; p<0.05); with decrease in GFR (r=-0.51; p<0.05); with increase in NGAL level in urine (r=+0.56; p<0.05), which indicate an adverse effect of asymptomatic hyperuricemia on the functional state of the kidneys in patients with EHD and concomitant T2DM.
Conclusion: Positive correlative relationships exist between asymptomatic hyperuricemia, increased albuminuria and a decrease in GFR, dyslipidemia, SBP, HbA1C, inflammatory processes and kidney damage, which indicate the heterogeneity of renal pathogenicity in patients with EHD combined with T2DM and a higher risk of cardiovascular disease in such patients.
Introduction
Essential hypertensive disease (EHD) and type 2 diabetes mellitus (T2DM) remain among the most common diseases in the world. Today, diabetes mellitus (DM) ranks third in the overall structure of morbidity and mortality after cardiovascular disease and oncological diseases. According to the forecasts of the World Health Organization (WHO), its prevalence by 2030 will increase to 500 million people [1, 2, 12]. According to WHO, in recent decades, the prevalence of diabetes mellitus in the countries of the world has increased by 1.5-2.0 times and ranges from an average of 1.5% to 3-4%, and in developed countries - up to 8-10%. Every 10-15 years, the number of patients with diabetes mellitus doubles [12].
The prevalence of essential arterial hypertension in patients with diabetes mellitus type 2 is 2-3 times higher than in the general population, and 70% of patients with type 2 diabetes mellitus have high blood pressure, which significantly increases the risk of developing cardiovascular complications that deteriorate the prognosis and quality of life of patients and is the main cause of mortality [2, 4]. In type 2diabetes mellitus combined with essential arterial hypertension, the risk of developing renal failure increases by 15-20 times [1, 4, 11].
In patients with diabetes mellitus type 2 and essential hypertensive disease, there is a severe impairment of kidney function with increased microalbuminuria (MAU) and decreased glomerular filtration rate (GFR) [14]. Prognostic unfavourable factors for nephropathy in essential hypertensive disease (EHD) and concomitant type 2 diabetes mellitus (T2DM) are characterized by increase in albuminuria and neutrophil gelatinase-associated lipocalin (NGAL) in urine; and with decrease in GFR, increase in systolic blood pressure, hyperglycemia, dyslipidemia, hyperuricemia, subclinical inflammation (with respect to TNF-α and hs-CRP levels in the blood) and with subsequent activation of fibrogenesis due to increased CTGF levels in the blood [5].
Defects of kidneys in patients with diabetes mellitus type 2 and concomitant essential arterial hypertension are accompanied by an increase in the levels of TNF-α, NT-proBNP, HIF-1α, CTGF in blood serum and NGAL in the urine, which may act as additional diagnostic and prognostic markers for the clinical progression of these combined pathologies [15].
Uric acid is the ultimate purine metabolism product, its increase is associated with the development of gout [3]. Recently, the issue of the relationship between asymptomatic hyperuricemia and the development of cardiovascular pathology in the absence of gout has been actively discussed [10, 13]. Asymptomatic hyperuricemia is common in patients with essential arterial hypertension: it is found in 25-40% of patients with the first (preliminary) diagnosis of essential arterial hypertension, in approximately 80% of patients with severe hypertension and in 50% of patients who use diuretics [16, 17]. It has been shown that in the presence of hyperuricemia, arterial hypertension develops due to a decrease in renal blood flow with subsequent partial renal ischemia, which contributes to the activation of the renin-angiotensin system [3, 9, 13]. According to the results of a 5-year prospective study, the initial hyperuricemia determined the rate of progression of hypertensive kidney damage [9]. Presently, hyperuricemia is considered as an independent predictor of the development and progression of chronic kidney disease [8].
Materials and Methods
The research included 105 patients (50 males and 55 females), aged 41-70 years, average age being (54.2±4.0) years. Patients were divided into 3 groups: Group I (GI) consisted of 25 patients with treatment-compensated EHD, 1–2-degree, stage II; Group ІІ (GII) was made up of 25 patients with subcompensated T2DM (glycated hemoglobin (HbA1C) - from 7.0 to 11.0%); Group III (GIII) had 55 patients with EHD, 1–2-degree, stage ІІ combined with subcompensated T2DM. Control group consisted of 15 practically healthy volunteers, 10 (66.7%) females and 5 (33.3%) males, aged (54.6±4.2) years. Groups were randomized according to age, sex, BMI, duration of EHD and T2DM. In addition to general clinical examination conducted; blood levels of uric acid (UA), lipids, tumour necrosis factor alpha (TNF-α), high-sensitivity C-reactive protein (hs-CRP) were determined. Urine levels of neutrophil gelatinase-associated lipocalin (NGAL) was also determined using immuno-fermentation methods.
In order to determine renal function state in patients with diabetes mellitus type 2 and essential hypertensive disease, it is necessary to constantly monitor MAU, GFR, along with systolic blood pressure (SBP), HbA1C and blood lipid profile [14]. To study the clinical dynamics of nephropathy in patients with T2DM and concomitant EHD, it is necessary to constantly monitor the MAU, GFR, HbA1C, serum lipid levels and blood pressure [6].
All patients underwent general clinical examination, determination of systolic blood pressure (SBP) and diastolic blood pressure (DBP). Characteristics of glucose metabolism were assessed by the level of fasting blood glucose, glycated hemoglobin (HbA1C); lipid metabolism - by the level in the blood of total cholesterol (TC), triglycerides (TG), low density lipoprotein (LDL), and high density lipoprotein (HDL).
The level of uric acid in the blood was determined using fermentative colorimetric test. The level of microalbuminuria (MAU) was determined using test strip (PentaPhan, "LaChema"). Glomerular filtration rate (GFR) was calculated using the CKD-EPI formula [11]. Reduction of GFR from 89 to 60 ml/ min/1.73m2 was considered a dysfunction of the kidneys of a mild degree, from 59 to 30 ml/min/1.73m2 - as moderate, from 29 to 15 ml/min/1.73m2 - as moderate for 3 months or more with or without signs of kidney damage, which is consistent with the definition of chronic kidney disease [1].
The research did not include patients diagnosed with gout, type 1 diabetes mellitus, type 2decompensated diabetes mellitus (HbA1C >11.0%), 3rd degree or severe hypertension, primary kidney disease, other somatic pathology in active or decompensated form with a decrease in GFR of less than 60 ml/min/1.73m2, presence of ketoacidosis in history.
In addition, patients with decompensated somatic pathology, oncological and lymphoproliferative diseases; chronic bronchitis in the active phase; chronic kidney disease (CKD) of another etiology, except for diabetic etiology; diabetic nephropathy of stages III, IV and V with macroalbuminuria and reduction of GFR below 60 ml/min/1.73m2; alcoholic liver disease of viral or toxic etiology; non-alcoholic steatohepatitis with a steady increase in liver transaminase by 1.5 times; history of abuse of alcohol and use of narcotic drugs; and with absence of individual consent of the patient for the research were all excluded from the research.
Clinical and laboratory studies were carried out in accordance with the recommendations of the manufacturers of diagnostic test kits and systems using modern laboratory technologies and with due observance of the ethical principles of the Declaration of Helsinki (DoH) in 2013 concerning human research.
Statistical analyses of the results of the research were carried out using the Microsoft Excel computer program from methods of variation statistics, the Student's t-distribution and the program "Statistica 13.0 for Windows". Estimates of the statistical significance of the difference, % were determined by the
chi-squared distribution (also known as chi-square or
χ2
{\displaystyle \chi ^{2}}-distribution)
method. To determine the correlation between individual parameters, a pair factor correlation analysis was performed with the calculation of the Pearson correlation coefficient (r) and its reliability (p).
Results and Discussion
Uric acid levels in the blood of Group I patients with EHD was (422.52 ± 11.85) μmol/L, in Group II patients with subcompensated T2DM, it was (349.25 ± 9.60) μmol/L. The highest uric acid levels in the blood was observed in Group III patients with EHD combined with subcompensated T2DM, and it was (490.23 ± 14.27) μmol/L, as compared with (287.60 ± 6.53) μmol/L in patients in the control group (p<0>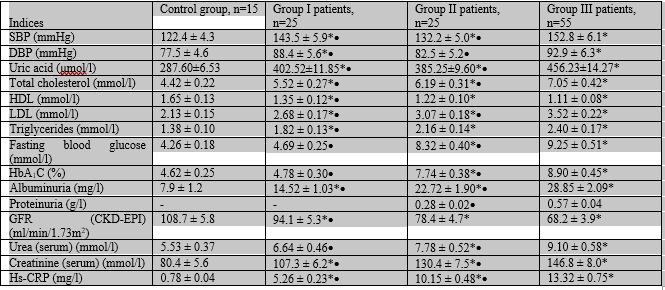
Notes: n – number of patients in a group; * – probability of difference from control group, р<0>
Тable 1: Clinical and laboratory indices of patients with diabetes mellitus type 2 and concomitant essential arterial hypertension, M±m
Asymptomatic hyperuricemia characterized by an increase in blood uric acid level of more than 410 μmol/l was observed in 34.6% of GI patients, in 21.8% of GII patients and most commonly in 55.7% of GIII patients with EHD combined with T2DM. Correlations between blood uric acid level with albuminuria was found (r=+0.42; p<0 r=-0.51; r=+0.56;>
Identified correlations between increased MAU, SBP, HbA1C, lipid profile indices and decreased GFR indicate the multifactorial process of nephropathy in patients with diabetes mellitus type 2 and essential hypertensive disease, and a higher risk of cardiovascular disease [14]. In patients with diabetes mellitus type 2 and concomitant essential hypertension, there is more severe dyslipidemia and a higher risk of cardiovascular disease [7].
The analyses of the results of the research made it possible to determine changes in the kidneys within patients of all the examined groups according to the results of laboratory tests and were most pronounced in Group III patients, whereas clinical manifestations were not observed. In particular, MAU was diagnosed in 20.0% of Group I patients, in 52.0% of Group II patients and in 72.0% of Group ІІІ patients. The average level of albuminuria in Group III patients exceeded that in the control group by 87.54% (p<0>
In addition, in 16.0% of Group II patients and in 28.0% of Group III patients non-significant proteinuria was detected - up to 0.66 g/l. The most decreased GFR was in GIII and was (68.2 ± 3.9) ml/min/1.73m2, which was lower than that of control group by 37.72% (p<0>
HbA1C is an index of glucose metabolism which is prognostic of the clinical course of type 2 diabetes mellitus, amounted to (8.90 ± 0.45)% in GIII patients, which exceeded the level in the control group by 47.68% (p<0>
The studied relationship between lipid profile levels, HbA1C levels and the SBP values shows the adverse effects of dyslipidemia on the clinical course of diabetes mellitus type 2 with essential hypertension comorbidity [7]. According to the results of the research, the atherogenic orientation of disturbances in lipid metabolism in studied patients was revealed. In particular, the increased total cholesterol level in GIII patients exceeded that in GI patients by 19.88% (p<0>
According to the statistical analyses, correlations were found between the indices of hyperuricemia, systolic blood pressure, glucose metabolism, lipid metabolism, inflammatory processes and kidney damage in GIII patients (Table 2).
Table 2: Pearson correlation coefficients between the indices of systolic blood pressure, glucose and lipid metabolism, inflammatory processes and kidney damage in patients with dual metabolic syndrome diseases (essential hypertensive disease and type 2 diabetes mellitus)
These were most pronounced in Group III patients with comorbidity. This, in our opinion, points to the heterogeneity of renal pathogenicity with respect to the effects of asymptomatic hyperuricemia, systolic blood pressure, HbA1C, dyslipidemia, microalbuminuria and renal dysfunction by decreasing GFR, which in general reflects the important role of uric acid on the clinical course of essential hypertensive disease combined with type 2 diabetes mellitus.
Results and Discussion
Uric acid levels in the blood of Group I patients with EHD was (422.52 ± 11.85) μmol/L, in Group II patients with subcompensated T2DM, it was (349.25 ± 9.60) μmol/L. The highest uric acid levels in the blood was observed in Group III patients with EHD combined with subcompensated T2DM, and it was (490.23 ± 14.27) μmol/L, as compared with (287.60 ± 6.53) μmol/L in patients in the control group (p<0>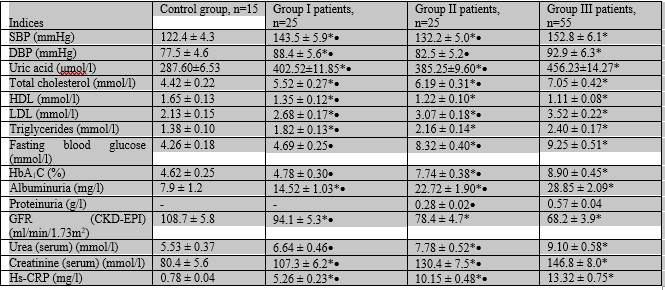
Notes: n – number of patients in a group; * – probability of difference from control group, р<0>
Тable 1: Clinical and laboratory indices of patients with diabetes mellitus type 2 and concomitant essential arterial hypertension, M±m
Asymptomatic hyperuricemia characterized by an increase in blood uric acid level of more than 410 μmol/l was observed in 34.6% of GI patients, in 21.8% of GII patients and most commonly in 55.7% of GIII patients with EHD combined with T2DM. Correlations between blood uric acid level with albuminuria was found (r=+0.42; p<0 r=-0.51; r=+0.56;>
Identified correlations between increased MAU, SBP, HbA1C, lipid profile indices and decreased GFR indicate the multifactorial process of nephropathy in patients with diabetes mellitus type 2 and essential hypertensive disease, and a higher risk of cardiovascular disease [14]. In patients with diabetes mellitus type 2 and concomitant essential hypertension, there is more severe dyslipidemia and a higher risk of cardiovascular disease [7].
The analyses of the results of the research made it possible to determine changes in the kidneys within patients of all the examined groups according to the results of laboratory tests and were most pronounced in Group III patients, whereas clinical manifestations were not observed. In particular, MAU was diagnosed in 20.0% of Group I patients, in 52.0% of Group II patients and in 72.0% of Group ІІІ patients. The average level of albuminuria in Group III patients exceeded that in the control group by 87.54% (p<0>
In addition, in 16.0% of Group II patients and in 28.0% of Group III patients non-significant proteinuria was detected - up to 0.66 g/l. The most decreased GFR was in GIII and was (68.2 ± 3.9) ml/min/1.73m2, which was lower than that of control group by 37.72% (p<0>
HbA1C is an index of glucose metabolism which is prognostic of the clinical course of type 2 diabetes mellitus, amounted to (8.90 ± 0.45)% in GIII patients, which exceeded the level in the control group by 47.68% (p<0>
The studied relationship between lipid profile levels, HbA1C levels and the SBP values shows the adverse effects of dyslipidemia on the clinical course of diabetes mellitus type 2 with essential hypertension comorbidity [7]. According to the results of the research, the atherogenic orientation of disturbances in lipid metabolism in studied patients was revealed. In particular, the increased total cholesterol level in GIII patients exceeded that in GI patients by 19.88% (p<0>
According to the statistical analyses, correlations were found between the indices of hyperuricemia, systolic blood pressure, glucose metabolism, lipid metabolism, inflammatory processes and kidney damage in GIII patients (Table 2).
Table 2: Pearson correlation coefficients between the indices of systolic blood pressure, glucose and lipid metabolism, inflammatory processes and kidney damage in patients with dual metabolic syndrome diseases (essential hypertensive disease and type 2 diabetes mellitus)
These were most pronounced in Group III patients with comorbidity. This, in our opinion, points to the heterogeneity of renal pathogenicity with respect to the effects of asymptomatic hyperuricemia, systolic blood pressure, HbA1C, dyslipidemia, microalbuminuria and renal dysfunction by decreasing GFR, which in general reflects the important role of uric acid on the clinical course of essential hypertensive disease combined with type 2 diabetes mellitus.
Conclusion
Positive correlative relationships exist between asymptomatic hyperuricemia, increased albuminuria and a decrease in GFR, dyslipidemia, systolic blood pressure, HbA1C, inflammatory processes and kidney damage, which indicate the heterogeneity of renal pathogenicity in patients with essential hypertensive disease combined with type 2 diabetes mellitus; and there also exists a higher risk of cardiovascular disease in such patients.
Prospects for further research
Further research should be aimed at finding effective treatment regimens for patients with dual metabolic syndrome diseases (essential hypertensive disease and type 2diabetes mellitus) on the background of asymptomatic hyperuricemia.
References
- Adapted clinical guidelines, based on evidence
View at Publisher | View at Google Scholar - American Diabetes Association (ADA) (2017). Standards of Medical Care in Diabetes.
View at Publisher | View at Google Scholar - El Ridi R, Tallima HJ (2017). Physiological functions and pathogenic potential of uric acid: A review. Adv. 8(5):487-493
View at Publisher | View at Google Scholar - Guidelines and clinical protocol for the provision of medical aid
View at Publisher | View at Google Scholar - Ikwuka AO, Virstyuk N (2022) Prognostic markers of nephropathy in patients with dual metabolic syndrome diseases (essential hypertensive disease and concomitant type 2 diabetes mellitus). Abstract #1184087 Endocrine practice 28(5):65-66
View at Publisher | View at Google Scholar - Ikwuka AO (2019). Clinical dynamics of nephropathy in patients in patients with diabetes mellitus type 2 and concomitant essential hypertensive disease.
View at Publisher | View at Google Scholar - Ikwuka AO (2017). Influence of dyslipidemia in patients with diabetes mellitus type 2 and essential hypertension. The Pharma Innovation Journal.
View at Publisher | View at Google Scholar - Johnson RJ, Nakagawa T, Jalal D, et al (2013). Uric acid and chronic kidney disease: which is chasing which? Nephrol. Dial. Transplant. 28(9):2221-2228
View at Publisher | View at Google Scholar - Mishchenko LA. (2016) Hyperuricemia and arterial hypertension - Is there a connection? Ukrainian Cardiology Journal 3:24-29.
View at Publisher | View at Google Scholar - Tashchuk VK, Vasek OASM (2016). Comorbidity, cardiovascular pathology and treatment of hyperuricemia - does allopurinol prevent the development of pathology? Bukovinsky Medical Bulletin. 20(2):209-212
View at Publisher | View at Google Scholar - Trifirò G, Sultana J, Giorgianni F, et al (2014). Chronic Kidney Disease Requiring Healthcare Services: A New Approach to Evaluate Epidemiology of Renal Disease. BioMed Research International (268362):6
View at Publisher | View at Google Scholar - Tronko MD (2014) Directory of Basic Indicators of the Endocrinology Service of Ukraine for 2013. Endocrinology 19(1):40
View at Publisher | View at Google Scholar - Vassalle C, Mazzone A, Sabatino L, Carpeggiani C (2016). Uric Acid for Cardiovascular Risk: Dr. Jekyll or Mr. Hide? Diseases 4(1):12-16
View at Publisher | View at Google Scholar - Virstyuk NG, Ikwuka AO (2019). Nephropathic characteristics in patients with diabetes mellitus type 2 and essential hypertensive disease. Art of Medicine 1(5):44-47 Available online.
View at Publisher | View at Google Scholar - Virstyuk NG, Ikwuka AO (2017). Diagnostic and prognostic markers of the diabetes mellitus type 2 course in connection with essential arterial hypertension taking into account the kidney function. Precarpathian Journal Pulse 8(44):53-62
View at Publisher | View at Google Scholar - Yakimenko IL (2014). Features of arterial hypertension combined with hyperuricemia in men. Ukr. Med. J 99(1):37
View at Publisher | View at Google Scholar - Zhdan VМ, Kitura OE, Kitura EM (2015). Hyperuricemia and arterial hypertension in general medicine practice. Family medicine 4:48-50
View at Publisher | View at Google Scholar
