

Review Article | DOI: https://doi.org/10.31579/2834-8761/034
Hard-to-Reach District in South Punjab of Pakistan: Challenges in Access to Childhood Brain Health Services and Interim Solutions
1 Chief Paediatric Neurologist for project Top-Down- Bottom-up
2 Children Hospital and Institute of Child Health Faisalabad
3 FCPS Paediatrics. Fellow Paediatric Neurology. Paediatric Neurologist for project Top-Down- Bottom-up.
4 Paediatric Neurology. FCPS, Paediatric Neurology Children Hospital and Institute of Child Health Multan
5 Consultant Paediatric Neurologist. The Brain Associates Lahore
*Corresponding Author: Muhammad Akbar Malik, Chief Paediatric Neurologist for project Top-Down- Bottom-up.
Citation: Muhammad Akbar Malik, Ahmad Omair Virk, Zia ur Rehman, Faisal Zafar, Arshad Rafiq, (2023), Hard-to-Reach District in South Punjab of Pakistan: Challenges in Access to Childhood Brain Health Services and Interim Solutions, Clinical Endocrinology and Metabolism, 2(6) DOI:10.31579/2834-8761/034
Copyright: © 2023, Muhammad Akbar Malik. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 November 2023 | Accepted: 28 November 2023 | Published: 30 November 2023
Keywords: Primary Health Care; healthcare; Pediatric Brain Health
Abstract
Background: Global health was founded on an egalitarian promise: improve health care for everyone, everywhere. However, treating and caring for children with brain disorders (CBDs), such as neurology, neuropsychiatry, and neuro-disability disorders, is a serious concern in low-income nations like Pakistan. Quality health service provision together with equitable geographic access and service delivery are important components that constitute g Universal Health Coverage (UHC).
Aim: The project aims to improve charitable primary care services and provide free health services in hard-to-reach districts, particularly in financially deprived districts of low-income countries like Pakistan, to address childhood brain disorders.
Methods: The monthly childhood brain health outreach program (CBHOP) was initiated to increase the geographic accessibility, availability, affordability, and acceptance of pediatric brain health treatments in District Bhakkar, a difficult-to-reach district in South Punjab, Pakistan. In 2012, Monthly camps were held throughout the three Tehsils and the city of Bhakkar as part of the program. As of 2018, in addition to the rotatory camps in various parts of the district, a partnership was established with the existing charity urban primary health care center next to DHQ Hospital Bhakkar, where various neurology subspecialty camps are held on set weekdays for each subspecialty each month. In addition to these the relative brain subspecialists provide free Tele-consultations and advices as and when required for their respective patients.
Results: The impact of the multifaceted strategy on the diagnostic gap (DG), treatment gap (TG), a and nonadherence (NDH) among children with epilepsy (CWE) was assessed after ten years of this endeavor. Four monthly pediatric neurology camps as the activity of the multidisciplinary brain health outreach program (MBHOP) did impact evaluation upon CWE from September to December 2022. Two newly joined pediatric neurologists, unaware of data collection purpose, reported that childhood epilepsy diagnostic gap decreased from 77.7% to 3.2%, treatment gap decreased from 89.2% to 4.2%, and nonadherence to prophylactic antiseizure medicines decreased from 66.1% to 19.3% among 280 CWE being treated at this brain health facility. This study also found no regional brain health care facility (BHCF) in the whole district. Multidisciplinary teams of pediatric and adult neurologists, psychiatrists, neutralizability experts, and therapists provide neurology services at this MBHCF.
Recommendations: Promoting and delivering brain health services for children in underserved, difficult-to-reach areas should be supported through a collaboration between public and private sector stakeholders. To provide specialized care in these remote places, it is advised to set up a network of relative visiting brain subspecialists from tertiary care centers.
Conclusion: The District Bhakkar CBHOP program has shown the effectiveness of such initiatives. The program has demonstrated that it is possible to change the situation for children with epilepsy by decreasing the diagnosis gap, treatment gap and adherence gap. The access framework identified various innovations enhancing BHCF access, highlighting disparities between supply and demand, and identifying areas needing further attention to address equity gaps for vulnerable populations,
Introduction
Epilepsy, a global disease, predominantly affects low and middle-income countries, with 80% of affected individuals in these regions, largely due to risk factors like head trauma and CNS infections. which are more common in poor regions, especially in rural areas. The median lifetime epilepsy prevalence for developed countries is 5.8 per 1.000, whereas in rural areas of developing countries is 15.4 per 1.000. [1] The incidence of epilepsy is 45/100.000/year in high income countries, compared to 81.7/100.000/year in LMIC. [2] The difference of prevalence and incidence among high income countries and LMIC is partly explained by some risk factors such as, poor obstetric care, head trauma, CNS infections and perinatal injuries, which are more common in poor regions, particularly in rural areas. [3] Approximately 70% of those diagnosed with epilepsy have seizure control by the use of antiseizure medications (ASM). [4] Nevertheless, even if the prognosis may seem "benign," a staggering 73.3% of patients with active epilepsy in rural areas of low- and middle-income countries (LMIC) do not obtain proper treatment or receive it in an unsuitable manner. [5] There have been efforts to improve epilepsy care, particularly in low- and middle-income countries (LMIC) where the treatment gap is greatest. However, significant childhood management barriers on demand and supply side remain on demand an especially in outreach financially deprived areas of these countries. [6]
Gaps in childhood epilepsy care range from lack of access to care and delayed diagnosis, to delayed treatment and lack of treatment optimization. Beyond quantifying the treatment gap, identifying barriers to care on demand and supply side for improving the quality of reporting, collaborative efforts in clinical care, research, education, and advocacy is critical for developing sustainable improvements. [7] An enduring observation across several areas is that individuals who are most susceptible tend to have the greatest disparity in access to treatment. There are significant differences in healthcare access and quality between regions with high and low socioeconomic status. Specifically, places with higher income and urban settings have smaller gaps in brain disorders treatment, while areas with lower income and rural settings have larger gaps in treatment. [8-10] The treatment gap worldwide is mostly determined by the availability of economic and healthcare resources. It is mainly a result of limited access to medication and healthcare services. [11] In order to organize preventive, promotive, curative, and rehabilitative services for PWE (the public health approach); understanding the risk factors, and determinants of epilepsy through epidemiological approaches becomes crucial. Despite tremendous progress over the last decades, there are still unaddressed health needs of people in all parts of the world. [12] Many people, particularly the poor and people living in hard-to-reach financially deprived rural areas and those who are in vulnerable circumstances, face challenges to remain healthy. [13]
Consistently provided monthly outreach children brain health program (OCBHP) services to economically disadvantaged communities that are difficult to access are linked to enhanced implementation of crucial treatments to address gaps in childhood epilepsy management. This research examines the effects of the combined approach of Outpatient Care for Brain Health Promotion (OCBHP) and integrative brain health care at an urban charity primary health care institution located in a financially disadvantaged district in the South-Punjab region of Pakistan. It specifically focuses on the demand and supply side challenges related to the provision of childhood brain health care in specific circumstances.
Our Pediatric Brain Health Care Outreach Program is for Hard-to-Reach District
In 2012, the corresponding author and one of his pediatric neurologist colleagues along with their chief neurotechnologist established BHOP for child neurological illnesses in South Punjab, Pakistan's remote and financially strapped Bhakkar district. They began this BHOP on their own, with no assistance from pharmaceutical companies or any other financial support. Later, other pediatric neurologists joined, and a group of five pediatric neurologists has been running the free services district ever since. Through these camps and surveys (BHOP) of pediatric brain disorders in 2015, they discovered a 90% treatment gap for childhood epilepsy (CETG), 54% of children with active epilepsy did not take their prophylactic antiseizure medications as directed, and 8% of children with epilepsy (CWE) had never seen a licensed doctor (primary treatment gap). The main causes of these were poverty and a lack of medically qualified personnel. [14] Costs associated with health care and other related expenses are a significant contributor to poverty in low-income countries (LIC) like Pakistan. Krishna from India determined that the expense of medical care is the root of 85% of all cases of poverty. [15] Heltberg and Lund discovered that only 12% of the poor in Pakistan were able to recover from the economic shock caused by the costs associated with illness. These costs of medical expenditure included decreased food consumption, withdrawal of children from school, sale of major assets, forced labor of children, and even bonded labor. [16] In fact, we discovered that inhabitants of Bhakkar pay an average of Rs. 16,000 for a single pediatric neurologist consultation from Multan or Lahore. [17] Whereas this can be managed at the cost of PRS 100-200 locally in Bhakkar city within an hour or so for most of these patients.
Activities and Goals of the program
Outreach health care strategies for hard-to-reach areas can be divided into three categories: 1) facility-based models for remote locations with limited financial resources, 2) mobile strategies, and 3) telecommunications techniques. These three categories have been integrated in our BHOP. In order to support realistic clinical and social outcomes for these illnesses, the provision of services for pediatric brain disorders in tandem with well-established primary care services leverages on already available human and financial resources. [18] A feasible and cost-effective way to achieve this goal may be to offer diagnosis &, in many cases, treatment for brain disorders at the first point of medical care, in conjunction with secondary, tertiary, or brain health specialists' support. This is supported by limited but significant evidence from developing countries that have established such programs.[19]Top-down approaches to community engagement, where modalities of participation are prescribed by outside financing projects, are typically less successful than bottom-up alternatives, which are developed by and through the community.[20] Implementing both Top-Down and Bottom Up strategies at a community health care facility could help the neglected and underserved communities, especially when telemedicine support is scarce, according to our healthcare team with ten years of experience. Despite free monthly camps for treatment and initiatives to educate healthcare professionals about pediatric neurology, there was no such facility in Bhakkar City. Parents continued to seek out specialized consultations when needed despite the expenses associated with travel, lodging, and consulting public teaching hospitals. To address the shortcomings of the government financed PHC system, a philanthropist and his family from Bhakkar City founded and ran Rukhsana Shafqat Urban Primary Health (RHUPHC) care as a non-profit organization. Even though free monthly camps were offered for treatment, raised awareness of pediatric neurology and advised health care professionals on how to properly manage childhood brain disorders, parents continued to seek consultation for their children from Lahore or Multan costing around 20,000 Pakistani Rupees due to their impulsivity in seeing the specialists as and when necessary. [17] These costs only cover travel, housing, and meals, as well as consulting with public teaching hospitals. A philanthropist from Bhakkar city and his family started and run Rukhsana Shafqat Urban Primary Health (RHUPHC) care as a nonprofit in response to the publicly funded PHC system's generally subpar performance. The philanthropist agreed to hire a general practitioner and other medical and paramedical staff in accordance with the demands of the healthcare team after being approached and expressed his joy at maintaining the facility accordingly. He also prepared to deploy telemedicine assistance for patients seeking treatment at this brain health care facility. RSUPHC and a diverse team of brain health subspecialists started working together in 2018 to enhance the lives of financially disadvantaged people of all ages with chronic, non-communicable neurological illnesses. The project's objectives were to encourage brain fitness and offer community members free services related to brain health. Since the center's services have grown over time, professionals from Multan, Faisalabad, and Lahore regularly visit to provide care for both children and adults. The following two main goals have been accomplished due to the cooperation of the subspecialists in brain health and the center's investors.
Objective 1: To strengthen the capacity of charity urban primary health care
Objective2: Establishment of free community facility for brain subspecialties health care.
Objective 1: To strengthen the capacity of charity primary health care
Strengthening primary health care has been shown to improve population health outcomes and reduce all-cause mortality and is a cost-effective strategy for achieving universal health coverage (UHC). [21] Community and civil society engagements are fundamental components of any strategy to achieve all health goals and targets of the health sustainable developmental goals (SDGs).[22] Our program is to strengthen the capacity of RSUPHC center through a layered support system involving volunteer/paid community members and paid staff working at this center. Majority of the health workers of this center had little or no prior experience in providing health services for brain disorders, but have been trained in heath provision for children with brain disorders. After the collaboration with RSPHC, a team of pediatric neurologists, neuropsychiatrists, consultant neurorehabilitation and childhood behavior therapy consultants began traveling on the monthly basis from three metropolitan cities (Lahore, Multan and Faisalabad) to the facility, a journey of approximately 5-7 hours by car, without receiving any monetary benefit. They work in conjunction with two clinical psychologists and two resident doctors of physical medicine who are employed in Bhakkar city by this BHCF. To ensure continuity, sustainability, and ongoing awareness of brain disorders in the outreach communities of this financially constrained district, each team member holds monthly camps. All visiting healthcare professionals maintain a consistent teaching schedule for the RSUPHC medical and paramedical staff in addition to their clinical duties. Additionally, they assist in identifying the enablers and inhibitors of the supply and demand sides of the provision of brain health care in their respective subspecialties. Co-developing services with engaged persons and communities promotes cultural sensitivity and increases patient satisfaction, which eventually leads to higher service utilization and better health outcomes. This patient-centered approach strengthens the use of patient-centered metrics in assessing effective primary care and is consistent with the central role that patients play in basic healthcare, which is supported by other studies. Bottom-up approaches to community participation, developed by and through the community, tend to be more successful, according to prior research. [23]
Objective2: Establishment of free community center for pediatric brain health care
Primary Health Care (PHC) is the most practical method for nations to achieve universal access because it has been found to be cost-effective.[17] While some Pakistani towns, such as Lahore and Islamabad, may claim of having established infrastructure and effective healthcare services, other places, such as Bhakkar, are financially underdeveloped and located in remote areas, making it difficult for residents to get healthcare. The 436-mile trip from Lahore to Bhakkar takes more than 6 hours to complete by car, whereas the 311 km fly takes just over 53 minutes. Although there are ways to increase access to healthcare, it is clear that some areas confront more difficulties because poverty is a major roadblock to development. Geographic accessibility, availability, cost, and acceptability are the four components of access to healthcare. [24] Accessibility issues can be caused by either the supply or demand for healthcare services.[25] Supply side determinants are characteristics of the health system that prevent service uptake by individuals, families, or the community. Demand-side determinants are factors influencing the ability to use health services at the individual, home, or community level. To develop effective treatments, it is necessary to distinguish between supply- and demand-side constraints. [24,25] The access restrictions, however, could not always be mutually exclusive and might also interact with one another. [26] The two types of physical methods are 1) facility mobile strategies a 2) facility-based models, and both can be integrated as we have done, among the various options for providing health facilities for communities' members of remote, financially challenged places. According to the country, its health requirements and priorities, and the quality of local health care supply, the stakeholders change and the methods likewise do. We adhere to Peters et al.'s definition of access to health services, which denotes "the timely use of service in accordance with need." [27]
As there were no governmental or private healthcare facilities that provided care for brain diseases for children and/or adults, a brain health outreach program (BHOP) was established in 2012 by holding monthly camps for children. The goals were to: 1) raise awareness of pediatric neurological diseases (PNDs); and 2) treat PNDs in the community at the children' doorsteps. 3) PNDs should only be referred to public teaching hospitals when necessary and under guidance. The supply-side and demand-side components of each of the four access dimensions are used to evaluate the obstacles to the provision of brain health care (BHCP). However, each of the four dimensions includes an essential element related to care quality. Important demand-side and supply-side barriers include the location of the service and the household. As consumers of healthcare services, the general population has no control over these aspects. We held monthly camps in various cities in an effort to break down these barriers, but people continued to travel to Lahore or Multan at a cost of PRS 20,000 for a single neurology consultation, not to mention lost wages, expensive medications, and even investigation from a free public teaching hospital. Communities initially lacked confidence in our services and the intermediaries connecting the populace with our team of pediatric neurologists by offering free consultations in pediatric neurology at the doorsteps of these underserved neighborhoods. This gave people the impression that we were only there to divert patients to our private clinics, which discouraged them from taking advantage of the offered services.[28] With the participation of practically all the stakeholders, the community's response was astonishing within a few years. From 20–30 patients per camp, it climbed to an average of 180–220 patients per camp, regardless of the distance and accessibility of the location.
Pediatric Brain Health Services Access Enablers
Our interventions were designed to make it easier for district to implement access to health services while simultaneously addressing the supply and demand sides, as this is proven to be the best geographic setting for improved PHC.[29] These interventions can be carried out at the district level by a team of specialists, the health sector on its own, or in partnership with other governmental agencies, nongovernmental organizations, or civil society organizations through the public and/or private sectors, as we did when we worked with the RSPHC facility. As it "reduces the power gaps between the population and health systems," we have included community involvement in initiatives addressing access barriers. [30] The majority of interventions appear to be non-financial and supply-side based, despite the fact that financial demand-side interventions are given more attention in international research. Demand-side financing refers to the direct allocation of resources to a population for the purpose of obtaining healthcare. [31] Our goals for promoting the demand side approach include: (1) improving care seeking by targeted populations; (2) focusing on service delivery; (3) enhancing provider behavior; (4) encouraging competition and subsequently improving care quality. Based on the quantity of financial input, supply-side financing is regarded as a way to improve the delivery of healthcare services. [32] We briefly outline our supply-side or demand-side, non-monetary or monetary, access-enabling interventions.
Demand-side, non-monetary interventions
Visiting consultant, employed community workers of RSUPHC center and all community stakeholders provide counseling about brain health services, including their availability, intention and associated costs (free services), address barriers related to Lack of Information on Health Care Service/Providers (availability) and Health Awareness (acceptability). Community leaders’ participation is a cross-cutting intervention that addresses the four access dimensions: 1) reduces transport costs; 2) improves information about services as well as health aspects;3) donates cash within the community when needed; and ;4) address household expectations and community cultural preferences. With empowerment strongly embedded in its features, community participation overcomes community and cultural preferences and stigma (acceptability), and enables greater availability of visiting brain subspecialists (availability). Professional health workers (employed in the RSUPHC center) can carry out a variety of preventive and curative interventions through so-called community-based interventions, which address issues with service location, transportation-related costs and means (geographical accessibility), free integrative brain health care, (affordability), and treatment accessibility. [33] Many acceptability hurdles for the health treatments these medical and paramedical professional health professionals promote about the full spectrum of services being provided by RSUPHC center are minimized because they are chosen from within the community. Similar to earlier studies,[34] these workers don't leave the center after receiving training and experience because they come from remote locations and are paid competitive wages to work in their local communities. They also act as key informants and are very useful for overcoming the disease stigma.
Demand-side, financial (DSF) interventions
Demand side finance (DSF) initiatives are frequently employed in LMICs to encourage "healthy behaviors" by reducing some of the financial expenses for consumers or by raising household income. Demands for out-of-pocket formal fees and unofficial payments for care services or supplies such medications, sutures, gloves, and diagnostic tests are prevalent in many nations [25,35]. By placing BHSs in the heart of impoverished neighborhoods, with the RSUPHC bearing the financial burden, we have eliminated these hurdles. The following list includes five different forms of DSF that have been employed in the medical field, each of which has a distinct intended mechanism of action. Regular payments to homes are made subject to certain "conditionalities," such as participation at community meetings and usage of government health services. Unconditional cash transfers are similar to regular payments, but without explicit requirements for service use. 3;)Short-term cash payments to offset expenditures are generally offered retroactively in medical facilities to patients who regularly visit the facility in question. 4;) In order to lower the cost of specific care services, vouchers are offered. Vouchers for "merit" items are intended to lower the price of commodities that support brain health, such as AEDs for epileptic patients. Schemes for vouchers may be created to include services from the public and private sectors as well as nonprofit organizations [36, 37]. Numerous LMICs have verified the value of DSF [38, 39]. We now provide monetary reimbursements for travel expenses and AED purchases made during an emergency or when AEDs are not available at the institution, but we require greater financial support to achieve these goals.
Supply-side, non-monetary interventions
The organization offers the residents of an outreach district affordable access to basic healthcare facilities. This is essential because adult or pediatric neurology services are unavailable in the public or private sectors. Their intervention focuses on geographic accessibility, ensuring that free medicines and other consumables are available to eligible people, and providing customized health services that are given by top-notch brain health specialists that match the needs of the community. The services are well regarded because they are free and offered in areas that households choose. A medical officer who works six days a week from 9 AM to 4 PM has been hired by the organization. The medical officer is qualified to handle common child neurological conditions and consult with the appropriate physician as required. By taking particular courses and hiring people from the same ethnic communities as the people whose issues need to be addressed, the provision of culturally sensitive health care is improved (acceptability).[40] Better management results in financial resources that are generated in accordance with local demands (availability), and accountability makes it possible for providers to be more responsive to the preferences and expectations of the community (acceptability).[41,42] Additionally, the management committee addresses all matters pertaining to money, service delivery, human resources (visiting consultants and local staff), and human resources in general.
Supply-side, financial interventions
The main goal of supply side initiatives is to make medications free (or heavily subsidized) at public facilities.[43] The supply side intervention includes building up the capacity of the healthcare facilities through service provider retraining, round-the-clock service availability, the addition of pharmaceuticals supplies, and provider incentives. This MDBHCF have hired two clinical psychiatrists, two physicians of physical medicine, a speech therapist, and the supporting staff at competitive salaries. This has somewhat increased the facility's capacity to meet the demands of various brain subspecialties in line with being implemented elsewhere in world. [44, 45] Distance to medical facilities, a lack of transportation, insufficient financial resources for care, and poor-quality care—all of which are frequently connected—are fairly typical issues in difficult-to-reach and resource-limited regions. [46, 47] About 15% of the nonadherent CWE in our sample, who lived less than 30 km from RSUPHC, agreed that the cost of transportation and the distance were the only factors contributing to their non-adherence to AEDs. Our long-term goal is to provide the necessary medications to such communities once a month. To deliver evidence-based care for chronic diseases, clinician visits, drug access, and modifications to treatment plans are necessary. However, delays in clinical interventions happen without transportation. These care delays may result in inadequate medical care, exacerbations of chronic diseases, or unmet medical demands, all of which can compound and worsen health outcomes [48].
The primary financier contributes significantly to the entire financial assistance for this healthcare facility's expenses. Affordability is improved by eliminating user fees or allowing exemptions, but only if these actions are taken in conjunction with other initiatives, such as increased drug supply and management oversight. The abolition of user fees boosts the use of curative public health care, as shown by Pariyat et al., although distance from the facilities continues to be a significant access barrier for the poor. [49] As Ensor and Cooper have shown, there are many access barriers that have been discovered, but the body of research on treatments to remove them is disproportionately tiny. [50] In contrast, where the access restrictions are understood, the framework of useful treatments can be utilized to evaluate the suitability of current solutions. All four characteristics of access barriers tend to be addressed through community involvement, community-based initiatives, health equity funds, provision of necessary essential services, improved management, and pay-for-performance. Although the aforementioned interventions are listed separately to help with the development of the analytical framework, the majority of them are actually employed in tandem, and the success of each one may rely on how it is combined and applied. [51, 52] We concur with O'Donnell that for the greatest impact, supply-side and demand side constraints must be removed together. [53] However, we stress that before any other intervention can be properly adopted, the quality of care must be developed.
Impact Evaluation of Outreach Brain Health Project upon Children with epilepsy (CWE).
Bhakkar Top-Down-Bottom-Up childhood epilepsy initiative has demonstrated a model that is cost and clinical effective in reducing the childhood epilepsy treatment gap (CETG). [14,17] A relationship with RSPHC was established in October 2019 after this epilepsy Initiative was initiated in 2012 using a staged method. In order to increase sustained access to antiseizure medications (AEDs), the program includes strengthening local brain health services offered by RSUPHC, strengthening referral systems, ensuring better monitoring of childhood epilepsy, providing free antiepileptic drugs (AEDS) for deserving patients, and raising awareness to support those who have epilepsy and their families.
A study was done in RSUPHC by the two newly joined pediatric neurologists in four monthly pediatric camps on September 10, October 16, November 20, and December 19, 2022, with no knowledge of the intent to collect data. In these four pediatric neurology camps at RSUPHC, all CWE being monitored at least for 3 months had their diagnostic gap (DG), treatment gap (TD), and nonadherence to antiseizure medicines were evaluated. For these three first benchmark improvements, the effectiveness of the Top-Down-Bottom-Up program techniques was evaluated in this comparative analysis (intervention vs. control CWE documented in 2015). All three baseline benchmarks have shown a significant improvement, with the youngest age groups showing the most increased improvements, Table-1.
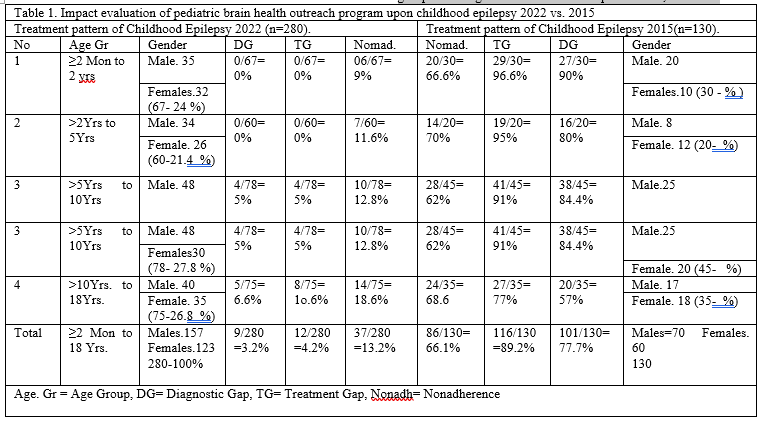
It has been recognized that effective guidelines must be adapted to local contexts, implemented, and assessed for impact before program revisions are made. In 2015, an agreement was reached to document the issue of improper diagnosis of epilepsy, which was found to be highest (90%) among individuals aged ≥2 months to 2 years and relatively lower (57%) among those aged ≥10 to 18 years, as shown in Table 1. It is worth noting that the diagnosis of epilepsy can be challenging, and research has suggested that up to 30% of patients referred for management of refractory seizures do not actually have epilepsy.
The proportion of people with epilepsy (PWEs) who are not properly treated, or the treatment gap (TG), is greater than 80% in several nations. The TG in Asian nations ranges between 30 and 98% and is higher in rural than in urban areas [54, 55] [. In Bhakkar City, we also discovered highly high CETG in 2015 [14,17], with the greatest levels in the youngest age groups and relatively lower levels in older age groups. The treatment gap was greatly minimized by our multifaceted approach to treating CWE, which included monthly camps of pediatric neurologists and the establishment of a free pediatric neurology center supported by telemedicine in RSUPHC-Bhakkar.
The treatment gaps between the age groups of 2 Mon 2 yrs. and >2 yrs. to 5 yrs. were 98% and 94%, respectively, at baseline. However, it took the entire local and visiting staff more than a decade of hard work to fully manage this enormous CETG. The base line treatment gaps for the older age groups (>5yrs to 10yrs and >10yrs to 18yrs) were reduced from 92% and 77% to 5% and 10.6%, respectively. The difference between the CETG at RSPHC before and after the intervention served as the primary outcome. Antiepileptic drug (AED) therapy has been shown to be successful in controlling seizures in 70% of patients. [56]. However, treatment compliance is still a key factor in successful]. Rate of adherence can be described as the percentage of the prescribed doses of the medication actually taken by the patient over a specified time period [57]. Accordingly in 2015 very high percentages of the CWE were found to be nonadherent to the prescribed antiepileptic drugs (AEDs), varying from 62% to 70% in different age groups, Table- 1. The childhood epilepsy is a chronic condition that can be treated by cost-effective first-line antiepileptic drugs (AEDs) [58] but adherence to the prescribed medicines is essential for seizure control. However, despite provision of free consultations and free AEDS, nonadherence decreased from 66% to 13%. Most of the nonadherent CWE are resident at places >30km, hard to reach and belong to the extremely poor families.
The population faces significant challenges in terms of access to healthcare, with some individuals experiencing difficulties traveling to the Regional Public Primary Health Care (RSUPHC) facility. Although the district is the primary geographic unit for intervention implementation in this case, other interventions may focus on scaling up access to healthcare in broader or narrower geographic areas. While this framework has been developed with a focus on a financially deprived, hard-to-reach district in South Punjab, it is worth noting that the conceptual similarities between barriers and interventions remain significant, despite the potential influence of socio-economic and cultural factors. The following are the future aspirations of our organization: 1) Developing an appropriate and cost-effective diagnostic and treatment plan, including laboratory, neurophysiology, and imaging studies, for pediatric neurology patients admitted to the inpatient service for a short stay of 4-24 hours;2) Providing around-the-clock management of pediatric neurological emergencies through the availability of one pediatric neurologist on video call; 3) Reaching the residents of far-flung localities with poor road connectivity and limited access to Regional Public Primary Health Care (RSUPHC) on a monthly basis; 4) Provision of neuroimaging studies for pediatric neurology patients. It is worth noting that we have not received any funding for these future aspirations, and we declare no conflicts of interest.
References
- Ngugi AK, Bottomley C, Kleinschmidt I, Sander JW, Newton CR. (2010). Estimation of the burden of active and life-time epilepsy: a meta-analytic approach. Epilepsies; 51:883–890.
View at Publisher | View at Google Scholar - Ngugi AK, Kariuki SM, Bottomley C, Kleinschmidt I, Sander JW, Newton CR. (2011). Incidence of epilepsy: a systematic review and meta-analysis. Neurology; 77:1005–1012.
View at Publisher | View at Google Scholar - Newton CR, Garcia HH. (2012). Epilepsy in poor regions of the world. Lancet; 380:1193–201.
View at Publisher | View at Google Scholar - Brodie MJ, Barry SJ, Bamagous GA, Norrie JD, Kwan P. (2012). Patterns of treatment response in newly diagnosed epilepsy. Neurology; 78:1548–1554.
View at Publisher | View at Google Scholar - Mbuba CK, Ngugi AK, Newton CR, Carter JA. (2008). The epilepsy treatment gap in developing countries: a systematic review of the magnitude, causes, and intervention strategies. Epilepsia 49:1491–1503.
View at Publisher | View at Google Scholar - Zelano J, Klecki J, Christensen J, Tomson T, Malmgren K, et al. (2019). The provision of epilepsy care across Europe: A 17-year follow-up survey. Epilepsia Open; 4:144–152. doi: 10.1002/epi4.12306
View at Publisher | View at Google Scholar - Spiciarich MC, von Gaudecker JR, Jurasek L, Clarke DF, Burneo J,et all., (2019). . Global health and epilepsy: update and future directions. Curr Neurol Neurosci Rep; 19:30. doi: 10.1007/s11910-019-0947-6
View at Publisher | View at Google Scholar - Kwon CS, Wagner RG, Carpio A, Jetté N, Newton CR, Thurman DJ. (2022).The worldwide epilepsy treatment gap: a systematic review and recommendations for revised definitions – a report from the ILAE Epidemiology Commission. Epilepsia. 63:551–564. doi: 10.1111/epi.17112.
View at Publisher | View at Google Scholar - Meyer AC, Dua T, Ma J, Saxena S, Birbeck G. (2010). Global disparities in the epilepsy treatment gap: a systematic review. Bull World Health Organ. 88:260–266.
View at Publisher | View at Google Scholar - Mbuba CK, Ngugi AK, Newton CR, Carter JA. (2008). The epilepsy treatment gap in developing countries: a systematic review of the magnitude, causes, and intervention strategies. Epilepsia. 49:1491–503.
View at Publisher | View at Google Scholar - Meyer ACL, Dua T, Boscardin WJ, Escarce JJ, Saxena S, Birbeck GL. (2012). Critical determinants of the epilepsy treatment gap: a cross-national analysis in resourcelimited settings. Epilepsia; 53:2178–2185.
View at Publisher | View at Google Scholar - Hartley D. (2004). Rural health disparities, population health, and rural culture. Am J Public Health.;94(10):1675–1678.
View at Publisher | View at Google Scholar - Walraven G. The 2018 Astana declaration on primary health care, is it useful? J Glob Health. 2019;9(1).
View at Publisher | View at Google Scholar - Malik MA, Malik H, Wali MW, Shabbir N, Saeed M (2015) Treatment gap in childhood epilepsy (TGCE): Pakistan regional study in under-resourced community. J Neurol Psychol;3: 7-10
View at Publisher | View at Google Scholar - Krishna A. (2006). Pathways out of and into poverty in 36 villages in Andhra Pradesh, India. World Development; 34: 271–288.
View at Publisher | View at Google Scholar - Helthberg R, Lund N. Shocks, (2009). coping and outcomes for Pakistan’s poor: health risks predominate. Journal of Development Studies; 45:899–910
View at Publisher | View at Google Scholar - Malik MA, Rafiq A, Virk O. (2019). Cost and Clinical-Effectiveness of Implementing Integrated
View at Publisher | View at Google Scholar - Services for Children with Epilepsy in Primary Care in an Outreach District in Pakistan. Medical Case Reports: Vol.5 No.2:115. ISSN 2471-8041
View at Publisher | View at Google Scholar - Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al. (2018). High-quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob
View at Publisher | View at Google Scholar - Health. November;6(11): e1196–252.
View at Publisher | View at Google Scholar - Kruk ME, Porignon D, Rockers PC, Van Lerberghe W. (2010). The contribution of primary care to health and health systems in low- and middle-income countries: a critical review of major primary care initiatives. SocSci Med.;70(6):904- 911.
View at Publisher | View at Google Scholar - Primary Health Care Performance Initiative. [Internet]. Per capita current primary health care expenditure ($USD). (https://phcperformanceinitiative.org /indicator/capita-current-primary-health-care-penditexure-usd; accessed 30 August 2022).
View at Publisher | View at Google Scholar - Universal health coverage. Sustainable Developmental Goal 3: Health. Geneva: World Health Organization; 2017. Available: http://www.who.int/universal_ health_coverage/en/ (accessed 2022 December 23).
View at Publisher | View at Google Scholar - Levesque J.F, Harris F. M and Grant Russell.G. (2013). Patient-centred access to health care:
View at Publisher | View at Google Scholar - conceptualising access at the interface of health systems and populations. International Journal for Equity in Health, 12:1-9.
View at Publisher | View at Google Scholar - World Health Organization. 20072018a. Declaration of Astana. Geneva. O’Donnell O. Access to health care in developing countries: breaking down demand side barriers. Cadernos de Sau´dePu´blica; 23: 2820–2834.
View at Publisher | View at Google Scholar - Ensor T and Cooper S. (2004) Overcoming barriers to health service access: influencing the demand side. Health Policy Planning; 19: 69–79.
View at Publisher | View at Google Scholar - Peters DH, Garg A, Bloom G et al. (2008). Poverty and access to health care in developing countries. Annals of the New York Academy of Sciences 1136: 161–171.
View at Publisher | View at Google Scholar - Rasanathan K, Montesinos EV, Matheson D, Etienne C, Evans T. Primary Health Care and the social determinants of health: essential and complementary approaches for reducing inequities in health. Journal of Epidemiology and Community Health 2009.
View at Publisher | View at Google Scholar - Muhorakeye O and Biracyaza E (2021) Exploring Barriers to Mental Health Services Utilization at Kabutare District Hospital of Rwanda: Perspectives from Patients. Front. Psychol.; 12:638377.
View at Publisher | View at Google Scholar - Viswanathan M, Kraschnewski JL, Nishikawa B, et al. (2010). Outcomes and costs of community health worker interventions: a systematic review. Med Care; 48(9):792-808
View at Publisher | View at Google Scholar - Borghi J, Ensor T, Somanathan A, Lissner C, Mills A. (2006). Mobilising financial resources for maternal health. Lancet.; 368:1457–1465.
View at Publisher | View at Google Scholar - Murray SF, Hunter B, Bisht R, Ensor T, Bick D. (2012). Demand-side financing measures to increase maternal health service utilization and improve health outcomes: a systematic review of evidence from low- and middle-income countries. Joanna Briggs Institute Library of Systematic Reviews.;10:4165–4567.
View at Publisher | View at Google Scholar - Murray SF, Hunter BM, Bisht R, Ensor T, Bick D. (2014). Effects of demand-side financing on utilization, experiences and outcomes of maternity care in low- and middle-income countries: a systematic review. BMC Pregnancy Childbirth.; 14:30.
View at Publisher | View at Google Scholar - Hunter BM, Portela A, Bick D. (2017). The effects of cash transfers and vouchers on the use and qualty of maternity care services: a systematic review. PLoS One.;12(3): e0173068
View at Publisher | View at Google Scholar - Haines A, Palmer N. (2007). Conditional cash transfers for improving uptake of health interventions in low- and middle-income countries: a systematic review. JAMA. Oct 24; 298(16):1900 Epub 2007/10/24. eng.
View at Publisher | View at Google Scholar - HJORTSBERG, C.A. & C.N. MWIKISA. (2002). Cost of access to health services in Zambia. Health Policy Plan. 1: 71– 77. 34. HJORTSBERG, C. Why do the sick not utilize health care? The case of Zambia. Health Econ. 9: 755–770
View at Publisher | View at Google Scholar - HJORTSBERG, C. (2003). Why do the sick not utilize health care? The case of Zambia. Health Econ. 9: 755–770.
View at Publisher | View at Google Scholar - Rasanathan K, Montesinos EV, Matheson D, Etienne C, Evans T. (2009). Primary Health Care and the social determinants of health: essential and complementary approaches for reducing inequities in health. Journal of Epidemiology and Community Health.
View at Publisher | View at Google Scholar - Bright, T., Felix, L., Kuper, H. et al. (2017). A systematic review of strategies to increase access to health services among children in low- and middle-income countries. BMC Health Serv Res ;17;252.
View at Publisher | View at Google Scholar - Hanson K, Ranson MK, Oliveira-Cruz V, Mills A. (2003). Expanding access to priority health interventions: a framework for understanding the constraints to scaling-up. J Int Dev.;15(1):1–14.
View at Publisher | View at Google Scholar - Ali GKM. (2009). How to establish a successful revolving drug fund: the experience of Khartoum state in the Sudan. Bulletin of the World Health Organization.; 87:139–142.
View at Publisher | View at Google Scholar - Haines A, Sanders D, Lehmann U et al. (2007). Achieving child survival goals: potential contribution of community health workers. The Lancet;369: 2121–2131.
View at Publisher | View at Google Scholar - Bohren MA, Hunter EC, Munthe-Kaas HM, Souza JP, Vogel JP, et all., (2014). Facilitators and barriers to facility-based delivery in low- and middle-income countries: a qualitative evidence synthesis. Reproductive Health. 11:71.
View at Publisher | View at Google Scholar - Bohren MA, Hunter EC, Munthe-Kaas HM, Souza JP, Vogel JP, Gulmezoglu AM. (2014). Facilitators and barriers to facility-based delivery in low- and middle-income countries: a qualitative evidence synthesis. Reprod Health.;11:71.
View at Publisher | View at Google Scholar - Varela, C., Young, S., Mkandawire, N. et al. (2019). TRANSPORTATION BARRIERS TO ACCESS HEALTH CARE FOR SURGICAL CONDITIONS IN MALAWI a cross sectional nationwide household survey. BMC Public Health 19, 264.
View at Publisher | View at Google Scholar - Chronic diseases and health promotion. 2012a Retrieved May 15, 2012, from Ma-Nitu SM. Financing primary health care: seeing the bigger picture. Lancet Glob Health. 2022 May;10(5):e611-e612. Epub 2022 Apr 4. PMID: 35390343; PMCID: PMC8979560.
View at Publisher | View at Google Scholar - Xu K, Evans DB, Kadama P, Nabyonga J, Ogwal PO, Nabukhonzo P, Aguilar AM. (2005 ). Understanding the impact of eliminating user fees: utilization and catastrophic health expenditures in Uganda. Soc Sci Med. 2006 Feb;62(4):866-76. doi: 10.1016/j.socscimed.2005.07.004. EpubSep 1. PMID: 16139936.
View at Publisher | View at Google Scholar - Pariyo GW, Ekirapa-Kiracho E, Okui O et al. (2009). Changes in utilisation of health services among poor and rural residents in Uganda: are reforms benefitting the poor? International Journal of Equity in Health; 8: 39.
View at Publisher | View at Google Scholar - Peters DH, Mirchandani G, Hansen PM. (2004). Strategies for engaging the private sector in sexual and reproductive health: how effective are they? Health Policy and Planning;19(Suppl. 1):15–21.
View at Publisher | View at Google Scholar - Ashford LS, Gwatkin DR, Yazbeck A. (2006). Designing Health & Population Programs to Reach the Poor. Washington, DC: Population Reference Bureau.
View at Publisher | View at Google Scholar - O’Donnell O. (2007). Access to health care in developing countries: breaking down demand side barriers. Cadernos de Sau´de Pu´blica ;23: 2820–2834
View at Publisher | View at Google Scholar - Newton CR, Garcia HH. (2012). Epilepsy in poor regions of the world. Lancet; 380: 1193–201.
View at Publisher | View at Google Scholar - Meinardi H., Scott R.A., Reis R., Sander J.W. (2001). World Ikot. The treatment gap in epilepsy: the current situation and ways forward. Epilepsia.; 42:136–149. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Trinka E., Kwan P., Lee B., Dash A. (2018). Epilepsy in Asia: Disease burden, management barriers, and challenges. Epilepsia. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Mac T.L., Tran D.S., Quet F., Odermatt P., Preux P.M.,et all., (2007). . Epidemiology, aetiology, and clinical management of epilepsy in Asia: a systematic review. Lancet Neurol.; 6:533–553. [PubMed] [Google Scholar].
View at Publisher | View at Google Scholar - Chisholm D, (2005). WHO-CHOICE. Cost-effectiveness of first-line antiepileptic drug treatments in the developing world: a population-level analysis. Epilepsia. ; 46: 751–759.
View at Publisher | View at Google Scholar - Lavsa S. M., Holzworth A., Ansani N. T. (2011). Selection of a validated scale for measuring medication adherence. Journal of the American Pharmacists Association. ;51(1):90–94. doi: 10.1331/JAPhA.2011.09154.
View at Publisher | View at Google Scholar - Chowdhury. S, Ashok Kumar Phani. K.A, Priyatosh Das.P etc. (2020). Chattogram Maa-O-Shishu Hospital Medical College Journal Volume;19; 1-6.
View at Publisher | View at Google Scholar
