

Research Article | DOI: https://doi.org/10.31579/2834-5177/049
Gestational Age as a Predictor of Oxygen Needs and ABG Patterns in Preterm Neonates with RDS: Evidence from a Resource-Limited NICU in Pakistan
Senior Department of Health Professional Technologies (DHPT), Faculty of Allied Health Sciences (FAHS), The University of Lahore, Pakistan.
*Corresponding Author: Ruhamah Yousaf, PhD Senior Department of Health Professional Technologies (DHPT), Faculty of Allied Health Sciences (FAHS), The University of Lahore, Pakistan.
Citation: Ruhamah Yousaf, (2025), Gestational Age as a Predictor of Oxygen Needs and ABG Patterns in Preterm Neonates with RDS: Evidence from a Resource-Limited NICU in Pakistan, International Journal of Clinical Infectious Diseases, 4(6); DOI:10.31579/2834-5177/049
Copyright: : © 2025, Ruhamah Yousaf. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 January 2025 | Accepted: 15 January 2025 | Published: 30 January 2025
Keywords: : respiratory distress syndrome; gestational age; preterm neonates; oxygen therapy; arterial blood gas (abg); neonatal intensive care
Abstract
Abstract
Respiratory Distress Syndrome (RDS) remains a leading cause of morbidity and mortality among premature infants. Their immature lungs lack surfactant, making breathing difficult. These infants need close monitoring with arterial blood gas (ABG) checks to guide oxygen therapy. While gestational age is known to influence disease severity, locally relevant data on oxygen requirements and arterial blood gas (ABG) changes across gestational age groups remain scarce in Pakistan
Introduction
Respiratory distress syndrome (RDS) is a major cause of morbidity and mortality among preterm neonates. It results from pulmonary immaturity and insufficient surfactant, leading to alveolar collapse, impaired oxygenation, and respiratory failure. Infants born before 36 weeks are at greatest risk, although antenatal corticosteroids, surfactant therapy, and modern respiratory support have improved survival.(1, 2)
The pathophysiology of RDS involves alveolar collapse due to surfactant deficiency, which increases the work of breathing and reduces oxygen delivery to tissues. Many affected infants require supplemental oxygen, continuous positive airway pressure (CPAP), or invasive ventilation in severe cases. However, oxygen therapy carries risks. Hypoxia can result in organ dysfunction, while hyperoxia contributes to complications such as bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), and impaired neurodevelopment. Therefore, careful titration of FiO₂ with close arterial blood gas (ABG) monitoring is essential to balance safety and efficacy.(3)
Gestational age strongly influences the severity of RDS and the level of support required. Extremely preterm infants often require higher FiO₂, prolonged respiratory support, and demonstrate more deranged ABG values compared with more mature preterm.(4) Non-invasive strategies, particularly CPAP and high-flow nasal cannula (HFNC), are now widely preferred to reduce ventilator-induced lung injury.(5) In addition, less invasive surfactant administration techniques, such as thin-catheter delivery, have shown promise in reducing the need for intubation and improving outcomes.(6) In resource-limited settings where surfactant is scarce, CPAP has proven to be an effective first-line therapy and improves survival when initiated early.(7)
Management guidelines now recommend targeting oxygen saturation ranges between 90–95% to avoid both hypoxia and hyperoxia. This requires continuous FiO₂ adjustment and ABG evaluation.(8) Evidence shows that very preterm infants (<28>
Globally, preterm birth affects nearly 15 million infants each year, with a large proportion at risk of RDS. The burden is higher in low-resource countries where advanced interventions remain limited.(11) Despite improvements, oxygen-related complications continue to be a major concern.(12) Antenatal corticosteroids remain a cornerstone for promoting lung maturation and reducing disease severity.(13)
In Pakistan and other low- and middle-income countries, standardized oxygen protocols and advanced monitoring are not always available. There is limited local data on how oxygen requirements, ABG parameters, and respiratory support vary by gestational age in neonates with RDS. Addressing this evidence gap is essential to optimize oxygen therapy and reduce preventable complications.
Therefore, this study was conducted to compare oxygen requirements, ABG parameters, and respiratory support across gestational age groups in preterm neonates with RDS. By providing locally relevant data, it aims to support individualized, evidence-based neonatal care and improve outcomes in resource-constrained NICUs.
Objective:
To evaluate gestational age–related variations in oxygen demand, ABG parameters, and respiratory support among preterm neonates with RDS, with the goal of identifying physiologic and management differences that may guide tailored interventions in low-resource NICU settings.
Methodology:
This four-month cross-sectional study was conducted in the NICU of the University of Lahore Teaching Hospital, Pakistan. Sixty-five preterm neonates (28–36 weeks) with RDS were enrolled through consecutive sampling. Data on gestational age, oxygen requirement (FiO₂), mode of respiratory support, and ABG parameters were collected before and after stabilization on respiratory support. Data were analysed in SPSS 27 using ANOVA, Kruskal–Wallis, Chi- square, paired t-tests, and Spearman’s correlation.
Results:
Lower gestational age was linked to higher oxygen needs (FiO₂ 83% at 28–30 weeks vs. 55% at 34–36 weeks, p < 0 xss=removed xss=removed>
Conclusion:
Gestational age is a key predictor of oxygen needs, ABG derangements, and intensity of respiratory support in preterm neonates with RDS. This first locally relevant evidence from Pakistan underscores the need for gestation-specific oxygen protocols to improve care in resource-limited NICUs and similar low-resource settings worldwide.
What is already known on this topic
Respiratory distress syndrome is a leading cause of illness and death in preterm babies. Oxygen therapy and arterial blood gas monitoring are central to care, but both under- and over-treatment can cause harm. Gestational age strongly influences oxygen needs and outcomes, yet data from local NICUs remain limited.
What this study adds
This study shows that babies born at lower gestational ages need higher FiO₂ and more invasive support. Blood gas values such as pH, PaO₂, PaCO₂, and SaO₂ vary significantly with gestational age, while HCO₃⁻ does not. It also provides locally relevant evidence from Pakistan to guide neonatal care.
How this study might affect research, practice or policy
These findings highlight the need for gestation-specific oxygen therapy and monitoring strategies in NICUs. They support the development of standardized oxygen protocols in resource-limited settings. The results may also inform future research to improve outcomes and reduce preventable complications in preterm infants
Methodology
Study Design and Setting:
This hospital-based, observational analytical study with a comparative cross-sectional design was conducted in the Neonatal Intensive Care Unit (NICU) of University of Lahore Teaching Hospital, a tertiary care centre for preterm neonates with respiratory distress syndrome (RDS).
Participants:
Preterm neonates (<37>
Sample Size and Sampling:
The sample size was calculated using a correlation-based formula:(14)
N = (Zα + Zβ / C) ² + 3, C=0.5×ln 1−r/1+r where ???????? = 1.96(α = 0.05), ???????? = 0.84(power = 80%), and r = 0.35 (expected correlation). Based on this, 62 neonates were required; 65 were enrolled using consecutive sampling to account for potential exclusions.(14, 15)
Data Collection:
Demographic details, gestational age, oxygen delivery device, FiO₂, and ABG parameters (pH, PaO₂, PaCO₂, HCO₃⁻, SaO₂) were extracted from medical records using a structured questionnaire (attached). ABGs were collected just before starting respiratory support and after stabilization. Gestational age was the independent variable; FiO₂, oxygen delivery device, and ABG parameters were dependent variables.
Statistical Analysis:
Continuous variables were summarized as mean ± SD and categorical variables as frequencies (%). Comparisons across gestational age groups used ANOVA or Kruskal-Wallis tests. Paired t-tests compared pre- and post-support values. Correlations between gestational age and oxygen/ABG parameters were assessed using Pearson or Spearman correlation. A p-value <0>
Ethical Approval and Informed Consent
This study was approved by the Departmental Review Board of The University of Lahore, Pakistan (Approval Letter No. Centre/Admin FAHS/195/25). The study was performed in accordance with the ethical standards of the institutional research committee and the principles outlined in the Declaration of Helsinki. Informed consent for participation was obtained verbally from the parents or legal guardians of all preterm neonates after explaining the purpose and procedures of the study. Verbal consent was chosen because most participants were approached during emergency NICU admissions, when obtaining written consent was not feasible. The verbal consent process was reviewed and approved by the Institutional Review Board.
Patient and Public Involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Results
A total of 65 preterm neonates with respiratory distress syndrome (RDS) were included in the study. The distribution of participants by gestational age, sex, and baseline characteristics is summarized in Table 1. The majority of neonates (38.5%) were born at 31–33 weeks of gestation, followed by 28–30 weeks (30.8%) and 34–36 weeks (30.8%). Males constituted 56.9% of the study population, while 43.1% were females. Most neonates were of low birth weight (60.0%), and 30.8% were very low birth weight. Caesarean section was the predominant mode of delivery (73.8%), and 63.1% of neonates were inborn. Antenatal corticosteroids were administered in 78.5% of cases, and 63.1% received surfactant therapy. The 5-minute Apgar score was ≥7 in 60.0% of neonates, indicating satisfactory initial adaptation (Table 1).
Analysis of oxygen requirements and types of respiratory support across gestational age groups (combined in Table 2) revealed that younger preterm neonates required significantly higher oxygen concentrations and were more likely to need mechanical ventilation. The mean maximum FiO₂ was 83.1 ± 18.5% in the 28–30-week group, decreasing progressively with gestational maturity (p < 0>
Baseline (pre-support) arterial blood gas (ABG) analysis demonstrated mild respiratory acidosis across all gestational groups, with mean pH values ranging between 7.22 and 7.24, as summarized in Table 3. Younger neonates had higher PaCO₂ and lower PaO₂ values, indicating more severe respiratory compromise. Following initiation of respiratory support, significant improvement was observed in all groups. The mean pH increased to 7.28–7.31, PaCO₂ decreased, and both PaO₂ and SaO₂ improved markedly (p < 0>
Spearman’s correlation analysis further illustrated the relationship between gestational maturity and oxygenation parameters (Table 5). A strong negative correlation was found between gestational age and both maximum (ρ = –0.558, p < 0 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed>
The types of respiratory support used across gestational age groups are presented in Table 2 and Figure 2. Overall, 40% of neonates were managed with continuous positive airway pressure (CPAP), 35.4% required mechanical ventilation (MV), and 24.6% were treated with nasal cannula (NC). The distribution of support types differed significantly across gestational groups (p = 0.011). The youngest neonates (28–30 weeks) were more frequently managed with mechanical ventilation, while older preterms were more often stabilized using CPAP or nasal cannula, reflecting the influence of lung maturity on respiratory support needs.
The effect of respiratory support on oxygenation status is detailed in Table 6, which shows a significant improvement in both PaO₂ and SaO₂ following stabilization. In the 28–30-week group, PaO₂ increased from 37.35 ± 6.47 mmHg to 51.85 ± 6.75 mmHg, while SaO₂ improved from 68.73 ± 7.60% to 84.53 ± 4.06%. Similar improvements were observed in the 34–36- week group, where PaO₂ rose from 43.50 ± 10.19 mmHg to 56.50 ± 9.25 mmHg and SaO₂ from 75.29 ± 10.53% to 87.60 ± 4.92%. Despite differences in baseline values, all neonates achieved the target saturation range of 90–94?ter respiratory stabilization.
Overall, the findings demonstrate that younger gestational age was consistently associated with higher oxygen requirements, more frequent need for mechanical ventilation, and greater baseline respiratory acidosis, as shown in Tables 2 and 3. However, after the initiation of appropriate respiratory support, significant improvement occurred in all groups. Correlation and graphical analyses (Table 5 and Supplementary Figures 1–5) further confirmed that advancing gestational maturity is associated with better baseline gas exchange and reduced oxygen dependency, emphasizing the physiological benefits of pulmonary development in preterm neonates with RDS.
Variable | Category | Frequency (n) | Percent (%) |
Gestational Age Group (weeks) | 28-30 | 20 | 30.8 |
31-33 | 25 | 38.5 | |
34-36 | 20 | 30.8 | |
Total | 65 | 100.0 | |
Sex | Female | 28 | 43.1 |
Male | 37 | 56.9 | |
Total | 65 | 100 | |
Birth Weight | VLBW (<1500> | 20 | 30.8 |
LBW (1500-2499 g) | 39 | 60.0 | |
Normal (≥2500g) | 6 | 9.2 | |
Total | 65 | 100 | |
Delivery Mode | Caesarean | 48 | 73.8 |
Vaginal | 17 | 26.2 | |
Total | 65 | 100.0 | |
Place of birth | Inborn | 41 | 63.1 |
Outborn | 24 | 36.9 | |
Total | 65 | 100.0 | |
Antenatal Corticosteroids | No | 14 | 21.5 |
Yes | 51 | 78.5 | |
Total | 65 | 100.0 | |
Surfactant | No | 24 | 36.9 |
Yes | 41 | 63.1 | |
Total | 65 | 100.0 | |
5min APGAR | <7> | 26 | 40.0 |
≥7 | 39 | 60.0 | |
Total | 65 | 100.0 |
Values are expressed as frequency (n) and percentage (%). VLBW = Very low birth weight (<1500 xss=removed>
Table 1: Baseline and Demographic Characteristics of Preterm Neonates with Respiratory Distress Synd
Gestational Age (weeks) | Frequency (n) | Maximum FiO₂ (%) Mean ± SD | Minimum FiO₂ (%) Mean ± SD | p-value (Kruskal- Wallis) | Type of Respiratory Support (n, %) | p-value (Pearson Chi- Square) |
|
|
|
|
| CPAP: 7 |
|
28-30 | 20 | 83.10 ± | 57.05 ± 9.81 |
| (35%), MV: |
|
|
| 18.49 |
|
| 12 (60%), |
|
|
|
|
|
| NC: 1 (5%) |
|
|
|
|
|
| CPAP: 9 |
|
31-33 | 25 | 68.52 ± | 45.24 ± |
| (36%), MV: |
|
|
| 20.39 | 13.73 |
| 9 (36%), |
|
|
|
|
| <0> | NC: 7 (28%) | 0.011 |
|
|
|
|
| CPAP: 10 |
|
34-36 | 20 | 55.60 ± | 37.25 ± 9.84 |
| (50%), MV: |
|
|
| 16.54 |
|
| 2 (10%), |
|
|
|
|
|
| NC: 8 |
|
|
|
|
|
| (40%) |
|
|
|
|
|
| CPAP: 26 |
|
Total | 65 | 68.17 ± | 46.42 ± |
| (40%), MV: |
|
|
| 21.41 | 13.79 |
| 23 (35.4%), |
|
|
|
|
|
| NC: 16 |
|
|
|
|
|
| (24.6%) |
|
Values are presented as mean ± standard deviation (SD) or number(percentage).
FiO₂ = Fraction of inspired oxygen; CPAP = Continuous positive airway pressure; MV = Mechanical ventilation; NC = Nasal cannula.
Table 3: Baseline (pre-support) and stabilized (post-support) arterial blood gas (ABG) parameters by
Parameter | 28–30 wks (mean ± SD) | 31–33 wks (mean ± SD) | 34–36 wks (mean ± SD) | Paired p- value (all groups) | ANOVA F | ANOVA p- value |
ΔPH | 0.06 ± 0.04 | 0.07 ± 0.07 | 0.07 ± 0.04 | < 0> | 0.595 | 0.555 (NS) |
ΔPaCO₂ | -8.55 ±2.67 | -6.84 ±3.28 | -7.05 ±3.30 | < 0> | 1.897 | 0.159 (NS) |
ΔPaO₂ | 14.50 ± 5.36 | 12.8 ± 5.01 | 13.00 ± 3.67 | < 0> | 0.804 | 0.452 (NS) |
ΔHCO₃⁻ | 1.15 ± 0.93 | 1.04 ± 0.84 | 1.40 ± 0.82 | < 0> | 0.987 | 0.378 (NS) |
ΔSaO2 | 15.81 ± 5.76 | 11.79 ± 5.28 | 12.30 ± 6.63 | < 0> | 2.93 | 0.061 (NS) |
Values are mean ± SD. Δ = change from pre- to post-support. Within-group changes assessed by paired t-test (p-values shown); between-group comparisons by one-way ANOVA. PaO₂ = Partial pressure of oxygen; PaCO₂ = Partial pressure of carbon dioxide; HCO₃⁻ = Bicarbonate; SaO₂ = Arterial oxygen saturation; NS = not significant.
Table 4: Within-group changes (Δ) in arterial blood gas (ABG) parameters and between- group comparis
Variable | Correlation Test | Correlation Coefficient | Sig. (2-tailed) | Interpretation |
| Min. FiO2 vs. GA | Spearman's rho | -0.571** | < 0.001 | ↑ GA → ↓ FiO2 (Strong negative) |
| Max. FiO2 vs. GA | Spearman's rho | -0.558** | < 0.001 | ↑ GA → ↓ FiO2 (Strong negative) |
| Min. FiO2 vs. Max. FiO2 | Spearman's rho | +0.901** | < 0.001 | very strong positive |
pH_avg. vs. GA | Spearman's rho | 0.377** | 0.002 | ↑ GA → ↑pH (Moderate positive) |
| PaCO2 avg. vs. GA | Spearman's rho | -0.464** | < 0.001 | ↑ GA → ↓ PaCO₂ (Moderate negative) |
PaO2 avg. vs GA | Spearman's rho | 0.251** | 0.044 | ↑ GA → ↑ PaO₂ (weak positive) |
- HCO3 avg. vs.GA | Spearman's rho | 0.126** | 0.316 | No meaningful correlation |
SaO2 avg. vs. GA | Spearman's rho | 0.274** | 0.027 | ↑ GA → ↑ SaO₂ (weak positive) |
Values are Spearman’s correlation coefficients (ρ) with corresponding 2-tailed significance. “Average” values were calculated as the mean of pre- and post-support measurements. **p < 0 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed>
Table 5: Correlation of gestational age with oxygen requirements and average arterial blood gas (ABG
Gestational Age (weeks) | Start FiO2 (%) Mean ± SD | FiO₂ Band (IQR range: P25–P75) | PaO2 Pre (mmHg) Mean ± SD | PaO2 Post (mmHg) Mean ± SD | SaO2 Pre (%) Mean ± SD | SaO2 Post (%) Mean ± SD | Target SaO2 (%) |
28-30 | 57.05 ± 9.81 | 50-99 | 37.35 ± 6.47 | 51.85 ± 6.75 | 68.73 ±7.60 | 84.53 ± 4.06 | 90-94 |
31-33 | 45.24 ± 13.73 | 32-92 | 43.16 ± 7.11 | 55.96 ± 7.99 | 75.66 ± 7.98 | 87.45 ± 4.46 | 90-94 |
34-36 | 37.25 ± 9.84 | 28-65 | 43.50 ± 10.19 | 55.50 ± 9.25 | 75.29 ± 10.53 | 87.60 ± 4.92 | 90-94 |
Oxygen requirement and arterial blood gas parameters in preterm neonates with respiratory distress syndrome by gestational age. Data are presented as mean ± SD unless otherwise stated; FiO₂ band shown as interquartile range (P25–P75). Pre = values before initiation of respiratory support; Post = values after stabilization.
Table 6: Oxygen requirement and oxygenation status of preterm neonates with RDS stratified by gestat
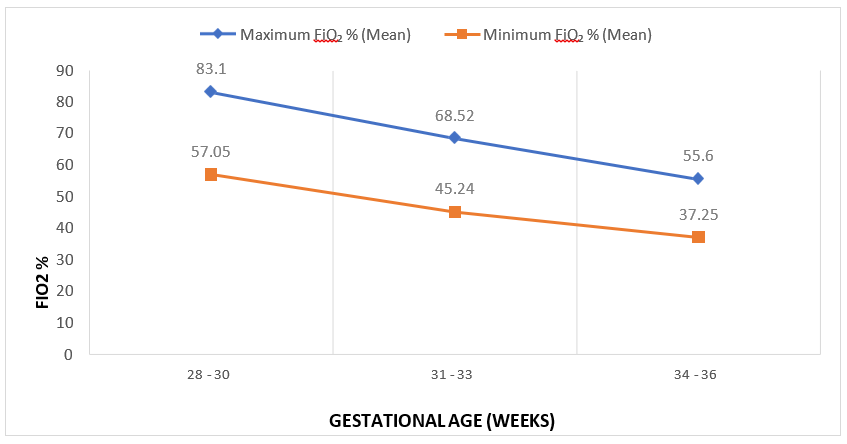
The graph illustrates the mean maximum and minimum fraction of inspired oxygen (FiO₂) across different gestational age groups (28–30, 31–33, and 34–36 weeks). Both maximum and minimum FiO₂ levels decrease with increasing gestational age, reflecting improved respiratory maturity. The Kruskal–Wallis test was applied to compare FiO₂ values among the groups.
Figure 1: Mean FiO₂ (%) across Gestational Age groups
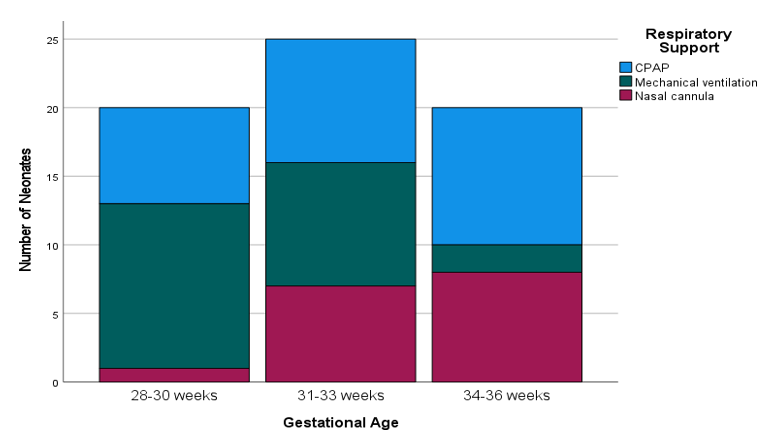
Distribution of respiratory support modalities among neonates by gestational age groups (28– 30 weeks, 31–33 weeks, and 34–36 weeks). Respiratory support includes continuous positive airway pressure (CPAP), mechanical ventilation, and nasal cannula. The y-axis represents the number of neonates in each category.
Discussion
This study demonstrated that gestational age strongly influences respiratory management in preterm infants with respiratory distress syndrome (RDS). Neonates born at 28–30 weeks required substantially higher FiO₂ and were more frequently managed with mechanical ventilation, whereas those at 34–36 weeks responded better to non-invasive support. These findings are consistent with earlier reports from high-resource countries, which have shown that lung immaturity and surfactant deficiency in very preterm infants increase oxygen needs and the likelihood of invasive ventilation.(3, 4, 7) However, unlike studies from high-income settings where surfactant use is routine and non-invasive support is increasingly successful, our cohort demonstrated a higher proportion of very preterm neonates requiring intubation and mechanical ventilation, reflecting differences in treatment resources and protocols in Pakistan.
Arterial blood gas parameters improved significantly after initiation of support, with increases in pH, PaO₂, and SaO₂ and a decline in PaCO₂, although the magnitude of change did not differ by gestational age. This suggests that oxygen therapy is beneficial across maturity levels when titrated appropriately, in line with earlier reports.(1, 8) yet the persistence of suboptimal SaO₂ values (<90>
Our results therefore extend existing knowledge by providing the first evidence from Pakistan that gestational age not only predicts oxygen and ventilation needs but also influences the success of stabilization under conditions where surfactant, high-flow nasal cannula, and advanced monitoring are not routinely available. These insights are particularly relevant for low- and middle-income countries, where neonatal care guidelines must adapt to resource constraints.
This study has several limitations. It was conducted in a single centre with a relatively small cohort, which may limit generalizability. Only three modes of respiratory support (CPAP, mechanical ventilation, and nasal cannula) were assessed, while high-flow nasal cannula was not included. Although variables such as birth weight, antenatal steroid use, and surfactant therapy were recorded, they were not analysed in detail as potential confounders. Other important factors, such as neonatal sepsis, were also not included. In addition, long-term outcomes like bronchopulmonary dysplasia or neurodevelopment were not evaluated. As with all observational studies, residual confounding cannot be excluded. Future multicentre studies with larger samples, inclusion of additional clinical variables, and follow-up of long-term outcomes are needed to strengthen these findings.
Conclusion
Gestational age is a key determinant of oxygen requirements and respiratory support in preterm neonates with RDS. Infants at earlier gestations required higher FiO₂ and more invasive ventilation, whereas those closer to term were more often stabilized with non-invasive support. Most ABG parameters (pH, PaCO₂, PaO₂, SaO₂) varied with gestational age, while HCO₃⁻ did not, indicating that metabolic compensation was relatively uniform across groups. This study provides the first locally relevant evidence from Pakistan, demonstrating how gestational age can be used to anticipate oxygen needs and guide respiratory management in resource-limited NICUs. These findings highlight the importance of developing gestation-specific oxygen protocols to reduce the risks of both hypoxemia and hyperoxia. Future multicentre studies with larger cohorts are warranted to validate these results and inform national and regional neonatal care guidelines.
Acknowledgment:
The authors would like to thank the Neonatal Intensive Care Unit (NICU) staff of the University of Lahore Teaching Hospital, Lahore, Pakistan, for their cooperation during data collection and clinical support. The encouragement of colleagues and family members during manuscript preparation is also gratefully acknowledged.
Funding:
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests
The authors declare no competing interests
Author contributions
SM: Conceptualization, data collection, data analysis, drafting of the manuscript.
RY: Supervision, methodology guidance, critical revision of the manuscript.
Both authors approved the final version and are accountable for the integrity of the work.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Due to patient confidentiality and institutional restrictions, the data are not publicly available
References
- Ali S,, Mohammed N, Qureshi N, Gupta S. 2020 Oxygen therapy in preterm infants: recommendations for practice. Paediatrics and Child Health.;31;
View at Publisher | View at Google Scholar - Bahadue FL, Soll R. 2012 Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database of Systematic Reviews. (11); 10.1002/14651858.CD001456.pub2.
View at Publisher | View at Google Scholar - Mathias M, Chang J, Perez M, Saugstad O. Supplemental Oxygen in the Newborn: Historical Perspectiveand Current Trends. Antioxidants. 2021;10(12):1879;
View at Publisher | View at Google Scholar - Norman M, Jonsson B, Söderling J, Björklund LJ, Håkansson S. 2023Patterns of respiratory support by gestational age in very preterm infants. Neonatology.;120(1):142–52;
View at Publisher | View at Google Scholar - Manley BJ, Arnolda GRB, Wright IMR, 2019Owen LS, Foster JP, Huang L, et al. Nasal High-Flow Therapy for Newborn Infants in Special Care Nurseries. N Engl J Med.;380(21):2031-40; 10.1056/NEJMoa1812077.
View at Publisher | View at Google Scholar - Abdel-Latif ME, Davis PG, Wheeler KI, De Paoli AG, Dargaville PA. Surfactant therapy via thin catheter in preterm infants with or at risk of respiratory distress syndrome. Cochrane Database Syst Rev. 2021;5(5):Cd011672; 10.1002/14651858.CD011672.pub2.
View at Publisher | View at Google Scholar - Abdallah Y, Mkony M, Noorani M, Moshiro R, Bakari M, Manji K 2023;. CPAP failure in the management of preterm neonates with respiratory distress syndrome where surfactant is scarce. A prospective observational study. BMC Pediatrics. 23(1):211;
View at Publisher | View at Google Scholar - Obst S, Herz J, Alejandre Alcazar MA, Endesfelder S, Möbius MA, Rüdiger M, 2022; et al. Perinatal Hyperoxia and Developmental Consequences on the Lung-Brain Axis. Oxidative Medicine and Cellular Longevity. 2022(1):5784146;
View at Publisher | View at Google Scholar - Sweet DG CV, Greisen G, et al. 2023 European Consensus Guidelines on the management of RDS – 2022 update. Neonatology.;119;
View at Publisher | View at Google Scholar - Subramaniam P, Ho JJ, Davis PG. 2021;Prophylactic or very early initiation of continuous positive airway pressure (CPAP) for preterm infants. Cochrane Database Syst Rev. 10(10):Cd001243;
View at Publisher | View at Google Scholar - Ohuma EO, Moller A-B, Bradley E, Chakwera S, Hussain-Alkhateeb L, Lewin A, et al. 2023 National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis. The Lancet.;402(10409):1261-71;
View at Publisher | View at Google Scholar - Thébaud B, Goss KN, Laughon M, Whitsett JA, Abman SH, Steinhorn RH, 2019et al. Bronchopulmonary dysplasia. Nature Reviews Disease Primers.;5(1):78;
View at Publisher | View at Google Scholar - McGoldrick E, Stewart F, Parker R, Dalziel SR. 2020 Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database of Systematic Reviews.;2020(12);
View at Publisher | View at Google Scholar - Hulley SB, Cummings SR, Browner WS, Grady D, Newman TB 2013.. Designing Clinical Research. 4th ed. Philadelphia: Lippincott Williams & Wilkins;
View at Publisher | View at Google Scholar - Kohn MA. 2022 Sample Size Calculators
View at Publisher | View at Google Scholar
