

Short Communication | DOI: https://doi.org/10.31579/2835-8325/121
Gastric Heterotopia of the Proximal Esophagus : A Case Report
Guelmim Faculty of Medicine and Pharmacy - Ibnou Zohr Agadir University Guelmim- Morocco.
Al AMAL Pathological Anatomy Laboratory, Guelmim-Morocco 81000.
*Corresponding Author: Imane Boujguenna. Guelmim Faculty of Medicine and Pharmacy - Ibnou Zohr Agadir University Guelmim- Morocco.
Citation: Imane Boujguenna and Fatima Boukis, (2024), Gastric Heterotopia of the Proximal Esophagus: A Case Report, Clinical Research and Clinical Reports 5(3): DOI: 10.31579/2835-8325/121
Copyright: © 2024, Imane Boujguenna. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 October 2024 | Accepted: 02 November 2024 | Published: 11 November 2024
Keywords: gastric heterotopia ; proximal esophagus ; pathology
Abstract
Gastric heterotopia of the proximal esophagus, also known as "Inlet Patch," is characterized by the presence of gastric mucosa within the esophagus. We present the case of a 21-year-old patient with no significant medical history, who came in with chronic abdominal pain and vomiting indicators of Gastric Heterotopia of the Proximal Esophagus.
Introduction
Gastric heterotopia of the proximal esophagus, also known as "Inlet Patch," is characterized by the presence of gastric mucosa within the esophagus. These patches can be distal, which differentiates them from Barrett's esophagus, or more commonly proximal at the cervical esophagus level.
Case Report
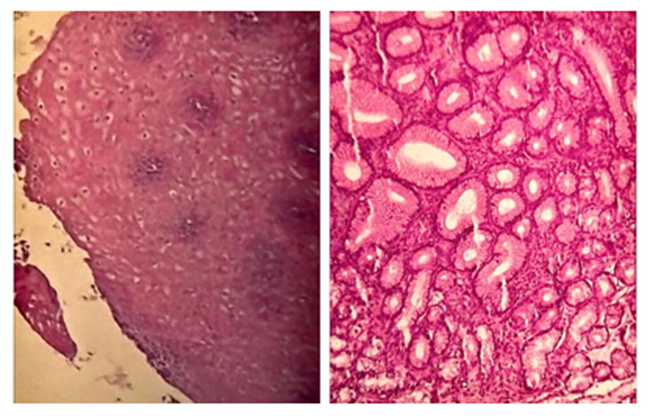
We present the case of a 21-year-old patient with no significant medical history, who came in with chronic abdominal pain and vomiting. The clinical examination was unremarkable except for abdominal tenderness. An abdominal ultrasound showed no abnormalities. Upper digestive endoscopy revealed an erythematous gastritis with a suspected inlet patch at the proximal esophagus. Biopsies were taken. Histopathological examination showed moderately active gastritis with Helicobacter Pylori and a gastric heterotopia at the proximal esophagus without signs of dysplasia or malignancy (Figure 1). The therapeutic management included treating the symptoms, Helicobacter Pylori gastritis, and monitoring the patient.
Discussion
The most widely accepted theory regarding the origin of gastric heterotopia in the esophagus is embryonic origin. Another hypothesis suggests these glands originate from esophageal glands. The prevalence of gastric heterotopia of the proximal esophagus ranges from 0.1% to 13.8%. Gastric heterotopias can be asymptomatic or present with symptoms such as dyspepsia, epigastric pain, heartburn, or regurgitation. Our patient experienced abdominal pain with vomiting, which might be due to chronic gastritis. Endoscopic diagnosis relies on identifying a lesion between 15 and 21 cm from the dental arches, appearing as a velvety, oval or round, pink or salmon-colored patch. It is best to examine the proximal esophagus by slowly withdrawing the endoscope with short, repeated insufflations while rotating the instrument clockwise or counterclockwise. Endoscopic diagnosis is confirmed by histopathological examination showing gastric mucosa. The main differential diagnosis is gastric metaplasia, particularly when the lesion is located distally in the esophagus. Complications of gastric heterotopia of the proximal esophagus include dysphagia, gingivitis, and rare neoplastic complications such as dysplasia and adenocarcinoma. Treatment involves symptomatic management and endoscopic surveillance.
Conclusion
Gastric heterotopia of the proximal esophagus is relatively rare and usually asymptomatic. Diagnosis is endoscopic and confirmed by histopathological examination. The main differential diagnosis is gastric metaplasia, especially in distal esophageal locations.
Acknowledgements
To anyone who has participated in the care of this patient directly or indirectly
Conflicts of interest
None declared.
Funding
No funding sources
ethical approval
ethics approval was not required for this study
Consent for publication
Yes
References
- Vui Heng Chong. (2013), Clinical significance of heterotopic gastric mucosal patch of the proximal esophagus. World J Gastroenterol. 19(3) :331338.
View at Publisher | View at Google Scholar - Sarhani Asmae, Paupard Thierry, Ghani Sara, Salihoun Mouna and Kabbaj Nawal. (2020), Heterotopic Gastric Mucosa of the Proximal Esophagus: An Under recognized Entity. Ann Clin Gastroenterol Hepatol. 4: 001-005.
View at Publisher | View at Google Scholar - Yoshida T, Shimizu Y, Kato M. (2010), Image du mois. Utilisation de l'endoscopie grossissante pour identifier l'adénocarcinome œsophagien précoce dans la muqueuse gastrique ectopique de l'œsophage cervicale. Clin de Gastroentol Hepatol. 8: e91-e93.
View at Publisher | View at Google Scholar - Avidan B, Sonnenberg A, Chejfec G, Schnell TG, Sontag SJ. (2001), Is there a link between cervical inlet patch and Barrett’s esophagus? Gastrointest Endosc. 53:717–721.
View at Publisher | View at Google Scholar - Meining A, Bajbouj M. (2010), Erupted cysts in the cervical esophagus result in gastric inlet patches. Gastrointest Endosc. 72:603–605.
View at Publisher | View at Google Scholar - Maconi G, Pace F, Vago L, Carsana L, Bargiggia S, Bianchi Porro G. (2000), Prevalence and clinical features of heterotopic gastric mucosa in the upper oesophagus (inlet patch) Eur J Gastroenterol Hepatol. 12:745–749. =
View at Publisher | View at Google Scholar - Ohara M. (2010), Incidence of heteroptopic gastric mucosa in the upper esophagus in first time narrow banding image endoscopy of consecutive 900 patients. Gastrointest Endosc. 71:AB316–317.
View at Publisher | View at Google Scholar - Chong VH, Jalihal A. (2010), Heterotopic gastric mucosal patch of the esophagus is associated with higher prevalence of laryngopharyngeal reflux symptoms. Eur Arch Otorhinolaryngol. 267:1793–1799.
View at Publisher | View at Google Scholar - Georges A, Coopman S, Rebeuh J, Molitor G, Rebouissoux L, et. al., (2011), Inlet patch: clinical presentation and outcome in children. J Pediatr Gastroenterol Nutr. 52:419–423.
View at Publisher | View at Google Scholar - Kim EA, Kang DH, Cho HS, Park DK, Kim YK, (2001), Acid secretion from a heterotopic gastric mucosa in the upper esophagus demonstrated by dual probe 24-hour ambulatory pH monitoring. Korean J Intern Med. 16:14–17.
View at Publisher | View at Google Scholar
