

Research Article | DOI: https://doi.org/10.31579/2835-2971/034
Frequency of Infection After Cerebrospinal Fluid Shunting Procedures
1FCPS, Senior Registrar, Department of Neurosurgery, Rawalpindi medical university and allied hospitals, Rawalpindi, Pakistan
2 PhD Scholar, Department of Sociology, PMAS ARID Agriculture University Rawalpindi, Pakistan
3Head of Department of Neurosurgery, Rawalpindi Medical University and allied hospitals, Rawalpindi, Pakistan
4FCPS, Senior Registrar, Department of Neurosurgery, Rawalpindi Medical University and allied hospitals, Rawalpindi, Pakistan
5Resident of MS Neurosurgery, Rawalpindi Medical University, Holy Family Hospital, Rawalpindi, Pakistan.
*Corresponding Author: Saad Javed. Resident of MS Neurosurgery, Rawalpindi Medical University, Holy Family Hospital, Rawalpindi, Pakistan.
Citation: Kashif Ramooz, Eesha Yaqoob, Nadeem Akhtar, Fraz Mehmood, Saad Javed, (2024), Frequency of Infection After Cerebrospinal Fluid Shunting Procedures, J. Clinical Pediatrics and Mother Health, 3(1); Doi:10.31579/2835-2971/034
Copyright: © 2024, Saad Javed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 January 2024 | Accepted: 20 February 2024 | Published: 28 February 2024
Keywords: CSF shunts; post-operative infection
Abstract
Hydrocephalus is routinely treated by surgical procedures. Cerebrospinal fluid shunt placement is a critical therapeutic intervention for hydrocephalus. CSF shunting has multiple complications among which infection is very common. The major cause of morbidity and mortality in patients with CSF shunts is the infection of the central nervous system (CNS). It can lead to prolonged hospital stay, increase the number of operative procedures 03 times more than then none infected cases and has twice the fatality rate. Study of such type of complication will help the patients to improve their health and also improve our sterilization techniques and reduce burden of hospital and patient’s expenditures. The objective of the study was to determine the frequency of infection after cerebrospinal fluid shunting procedures. Case series study was used as study design. Study was conducted from 10-2010 to 10-06-2011.One hundred and forty-four patients with both genders of all age groups undergoing cerebrospinal fluid shunting, meeting inclusion and exclusion criteria, were selected for the present study after informed consent of patient or guardian and approval by the hospital ethical committee. Follow up was ensured by taking the telephonic contact and address of patient. Total no of patients were 144 among which, 89 were males and 55 were females. Age distribution was from 01 month to 75 years with the mean age of 15.280 and standard deviation was ± 20.450. Post-operative infection was present in 20(13.9%) patients.
Introduction
The eradication of infection in patients with colonized shunts has always been a great challenge to the treating surgeon. Various methods have been tried with variable success. Meticulous aseptic measures, preoperatively and pre-operatively are essential in preventing colonization [1]. Shunt infections occur generally within two months of shunt insertion and most common organism is staphylococcus epidermis. Despite the high incidence of infection, optimal management is still debatable, and research on prevention has been hampered by single-institution series and small numbers [2].CSF shunting has various complications among which shunt infections is the commonest [3].As data is not available, it is not possible to make early diagnosis of shunt infection in patients with nonspecific clinical features. Among common predisposing factors for shunt infection are infants with <6months>
So, it is evident that hydrocephalus is a syndrome in which there is disturbance in the dynamics of cerebrospinal fluid due to different types of diseases. There were different potential sites at which CSF flow obstruction occurs and they also thought that all hydrocephalus is obstructive in nature [12]. Hydrocephalus is a condition in which excess fluid accumulates in the brain [13]. Antibiotic-impregnated catheter shunt systems, in particular, appear to reduce infection risk in some, but not all, reported series. Unfortunately, none of these studies were performed in a prospective, double-blinded, randomized controlled fashion [14]. Infection of the central nervous system (CNS) is a major cause of morbidity and mortality in patients with CSF shunts [15]. During the eighteenth and nineteenth centuries, diets and dehydration cures were suggested [16]. Long-term follow-up of shunted children is necessary to evaluate the real incidence of shunt Infection and the functional outcome after shunt Infection [17].
Objective of Study:
• To determine the frequency of infection after cerebrospinal fluid shunting procedures.
Materials and Methods
Study Design: Case series study.
Duration Of Study: Eight months (16th October 2010 to 16 June 2011)
Sample size: Total 144 patients were taken for this study among which 89 were males and 55 were females. All of which operated for CSF shunts.
Sampling Technique: Non-probability consecutive sampling
Sample Collection:
Inclusion criteria:
1. All cases with communicating and non-communicating hydrocephalus.
2. All age groups with both genders.
3. Cerebrospinal fluid shunting under same type of anesthesia and antibiotic cover.
Exclusion criteria:
1. Diagnosed case of active meningitis.
2. History of previous cerebrospinal fluid shunting.
3. Patients having co morbid conditions like diabetes mellitus, end stage renal disease, ischemic heart diseases, malnutrition and cirrhosis of liver.
Data Collection Procedure:
Patients with both genders of all age groups underwent cerebrospinal fluid shunting, meeting inclusion and exclusion criteria have been selected for the present study after informed consent of patient or guardian and approval by the hospital ethical committee. Operation has been done by consultant neurosurgeon. Pre- and post-operative antibiotic prophylaxis such as Oxidil (Sammi), Vanccare (Citicare Laboratories Pvt. Ltd.) and Flagyl (Pfizer) has been given according to CSF shunt (Medtronic USA VP shunt medium pressure) protocol. Every patient has been examined clinically for infection by the trainee Researcher on 3rd, 7thand 15th postoperative day. Clinically suspected cases have been confirmed by blood C-reactive protein, cerebrospinal fluid analysis and complete blood profile with ESR. Patients with no complications have been discharged on 3rdpost-operative day and kept on follow up till 15th postoperative day to consider complication free patient. Follow up has been ensured by taking the telephonic contact and address of patient.
Data Analysis Procedure:
Data has been analyzed using software named “Statistical Package for Social Sciences” version 11. Frequency and percentages have been calculated for qualitative variables like infection, gender and type of hydrocephalus. Mean and standard deviation has been calculated for quantitative variables i.e., age
Results
There was total 144 patients in which CSF shunting was done for hydrocephalus from 16-10-2010 to 16-06-2011.
Diagnosis of patients; Among 144 numbers of patients, maximum number of cases operated for non- communicating and communicating hydrocephalus was congenital hydrocephalus and minimum number of cases wascerbellopontine angle tumors. Table 1: Values in table 1 showed that 85% of patients were low grade fever while 60% of patients faced the problem of vomiting and 30% of patients had the symptom of irritabilit
Symptoms | Number of patients | % age |
Low grade fever | 17 | 85 % |
Vomiting | 6 | 60 % |
Irritability | 12 | 30 % |
Table no 1showed that 85% of patients were low grade fever while 60% of patients faced the problem of vomiting and 30% of patients had the symptom of irritability.
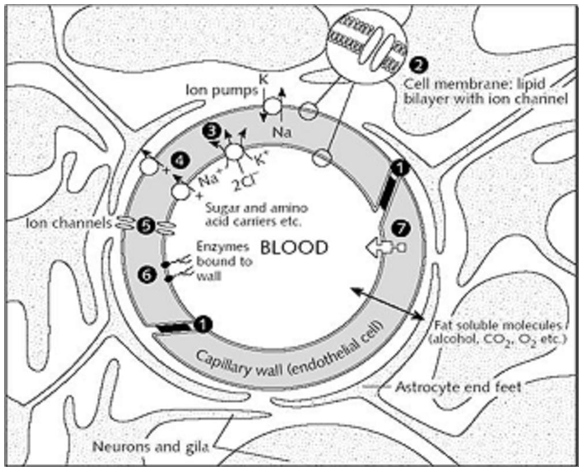
Figure 1: Diagram of a cerebral capillary enclosed in astrocyte end-feet. Characteristics of the blood-brain barrier are indicated: (1) tight junctions that seal the pathway between the capillary (endothelial) cells; (2) the lipid nature of the cell membranes of the capillary wall which makes it a barrier to water-soluble molecules; (3), (4), and (5) represent some of the carriers and ion channels; (6) the 'enzymatic barrier' that removes molecules from the blood; (7) the efflux pumps which extrude fat-soluble molecules that have crossed into the cells.
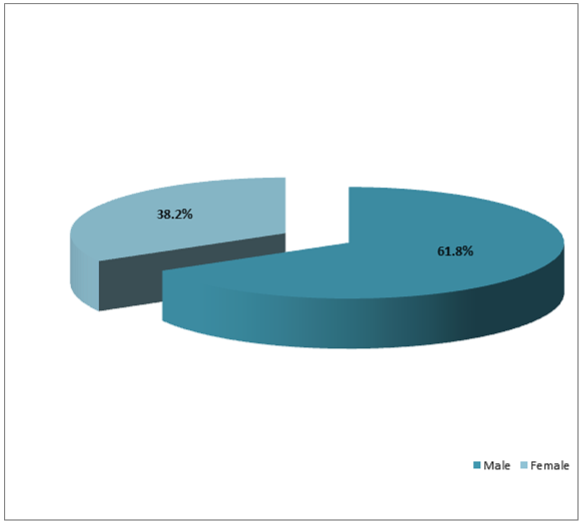
Figure 2: Out of these 144 patients, there were 89 (61.8%) males and 55 (38.2%) females with the ratio of 1:0.6.
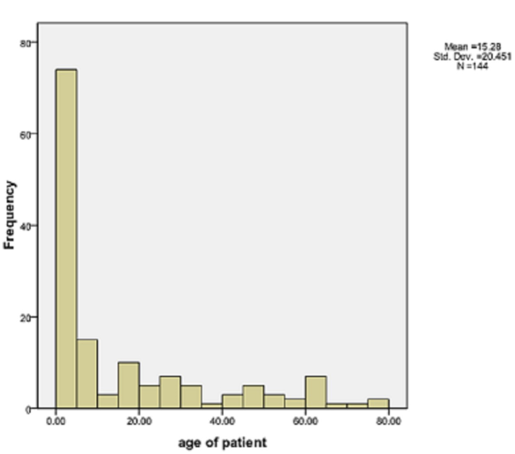
Figure 3: Patients were between the ages of 01 month to 75 years with the mean age of 15.280 and standard deviation was ± 20.450. Maximum age was 75 years and minimum were 01 month but no patient was under 1 month of age at operation. Highest number of patients was between the ages of 01 month to 07 years. Lowest figure was between the ages of 16 to 45 years.
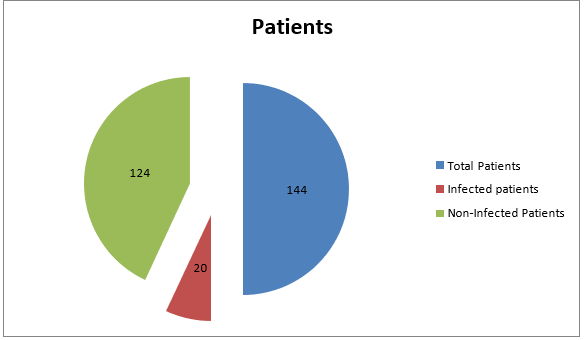
Clinically confirmed infection in post-operative periods: Among 144 patients, 20 (13.9%) had post-operative infection while 124(86.1%) had no evidence of infection. The infected patients had the symptoms of low-grade fever (85%), irritability (60%) and vomiting (30%).
Laboratory findings:
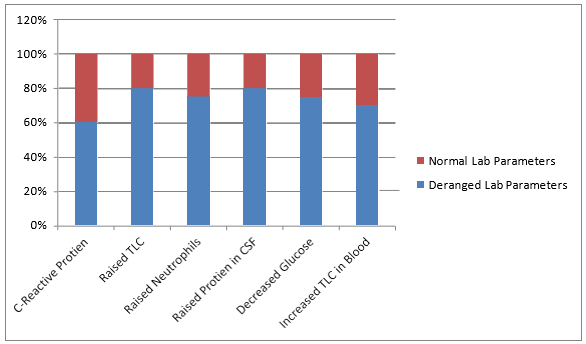
Post-operative 60% infected patients had C-reactive protein of more than 10mg/dl while some infected and all non-infected patients had value of 10 or less than 10mg/dl. Among these, 80% infected patients had raised TLC, 75% had raised neutrophils and 80% had raised protein in CSF. 75% had decreased glucose in CSF. 70% infected cases also had increased TLC in blood.
Discussion
The purpose of study was to determine the frequency of infection after cerebrospinal fluid shunting procedures and to improve our sterilization techniques, patients’ health and to reduce the burden of hospital, patient’s expenses and hospital stay.In this study total number of cases were144 who were treated for hydrocephalus with CSF shunts. Patients were between the ages of 01 month to 75 years with the mean age of 15.4197± 20.820 and minimum age was 01 month and maximum was 75 years. Highest number of patients was between the ages of 01 month to 07 years. Lowest figure was between the ages of 16 to 45 years. Maximum number of patients had congenital hydrocephalus (26.7%), then patients with blocked shunts (20%). Among 144 patients, 20 (13.9%) had post-operative infection while 124(86.1%) had no evidence of infection. The infected patients had the symptoms of low-grade fever, irritability and vomiting and maximum had showed high value of C-reactive protein considering the normal rang 0-10. All those infected cases were confirmed by laboratory investigations of CSF and blood. These infected patients had raised TLC, neutrophils and protein in CSF while they had decreased glucose in CSF. Also, there was raised TLC and ESR in blood. Two hundred and twenty-six cerebrospinal fluid (CSF) shunt related procedures performed. During the study period, nine shunt infections resulted from 226 shunt procedures, giving an overall infection rate of 3.98%. Of the nine patients who got infected, there were seven males and two females. Six of the males and one female were below 15 years of age. In this study, infection rate was very low as compared to our study.
Recommendations
This study helps us to improve patients’ health and to reduce the burden of hospital, patient’s expenses and hospital stay by improving our sterilization techniques, prophylactic antibiotics and proper follow up.
Declaration
• Ethics approval and consent to participate: Taken from the department and chair
• Consent for publication: All authors consented for publication
• Availability of data and material: available
• Competing interests: none
• Funding: none
Authors' contributions
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work: Dr Kashif Ramooz, Dr Saad Javed, Eesha Yaqoob Drafting the work or revising it critically for important intellectual content: Dr Saad Javed Final approval of the version to be published; Eesha Yaqoob Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: Dr Saad Javed, Eesha Yaqoob
Acknowledgements
For the Rawalpindi medical university which gave us the platform to work and research
Author’s approval
All the authors have seen the manuscript and approved it.
Data availability statement
All the data is available with me and can be produced whenever required by the editor
Disclosure of Funding
None.
References
- Bhatnagar V, Mitra DK, Upadhyaya P. Shunt related infections in hydrocephalic children. Indian Pediatr 1986; 23:255–7.
View at Publisher | View at Google Scholar - Bokhary MMA, HM Kamal. Ventriculo-Peritoneal Shunt Infectionsin Infants and Children. Libyan J Med. 2008;3(1):20-22.
View at Publisher | View at Google Scholar - 3Browd SR, Gottfried ON, Ragel, Duham, Nakahara, Shimizu. Failure of cerebrospinal fluid shunts. Pediatr Neurol. 2006; 34:171- 6.
View at Publisher | View at Google Scholar - 4Dallacasa, Dappozo A, Sandri F, Cochhi G. Cerebrospinal fluid shunt infections in infants. Child nerv syst. 1995; 11:643-49.
View at Publisher | View at Google Scholar - Dandy W. Internal hydrocephalus, an experimental, pathological and clinical study. Am J Dis Child 1914; 8:406-82.
View at Publisher | View at Google Scholar - Garton HJ, Piatt JH “Hydrocephalus” J PediatrClin North Am. 2004;51:305-25.
View at Publisher | View at Google Scholar - Jansen J. Etiology and prognosis in hydrocephalus. Childs NervSyst 1988; 4:263- 7.
View at Publisher | View at Google Scholar - Khan I, Burhan M, Nadeem M. a reappraisal of contibuting factors leading to shunt infection. J Ayyub Med Coll Abbot. 2009; 21:66-8 home > Vol 21, No 1 (2009) >Khan.
View at Publisher | View at Google Scholar - Mwang'ombe NJ, Omulo T. ventriculoperitoneal shunt surgery and shunt infections in children with non-tumour hydrocephalus. East African Med Jour 2000;77.
View at Publisher | View at Google Scholar - 10Nicholas JL, Kamal IM, Eckstein HB. Immediate shunt replacement in the treatment of bacterial colonization of Holter valves. Dev Med Child Neurol1970; 22:110.
View at Publisher | View at Google Scholar - Pudenz R. The surgical treatment of hydrocephalus- a historical review. Surgical neurology. 1981; 15:15-25.
View at Publisher | View at Google Scholar - Ransohoff J, Shulman K, Fishman RA: Hydrocephalus: a review of etiology and treatment. J Pediatr 1960; 56:399-411.
View at Publisher | View at Google Scholar - Rizvi R, Anjum Q. Hydrocephalus in children. J Pak Med Assoc. 2005; 55:502-6Journal of Surgery Pakistan (International) 16 (3) July - September 2011.
View at Publisher | View at Google Scholar - Rozzelle CJ, Leonardo J, Veetai L. Antimicrobial suture wound closure for cerebrospinal fluid shunt surgery. J Neurosurg Pediatrics 2008; 2:111–17.
View at Publisher | View at Google Scholar - Sacar S, Turgut H, Toprak S, Cirak B, Koskun E, Yilmaz O et al. A retrospective study of central nervous system shunt infections. BMC infect dis. 2006; 6:43.
View at Publisher | View at Google Scholar - 16Torack, R. M. (1982). Historical aspects of normal and abnormal brain fluids: II. Hydrocephalus. Archives
View at Publisher | View at Google Scholar - 17Vinchon M, Dhellemmes P.
View at Publisher | View at Google Scholar
