

Research Article | DOI: https://doi.org/10.31579/2834-5126/103
Formation And Regression of Sports Vagotonia (Based on Heart Rate Variability Data Under Conditions of Active Orthostasis)
1Vyatkа State University, 36 Moskovskaya St., Kirov, 610000, Russia.
2Kirov Regional State Autonomous Institution of Additional Education "Sports School of the Olympic Reserve "Perekop", 1A Sverdlova St., Kirov, 610011, Russia.
3Kazan State Medical University, 49 Butlerova St., Kazan, 420012, Russia.
4Kirov State Medical University, 112 K. Marx Street, Kirov, 610998, Russia.
*Corresponding Author: V. I. Tsirkin. Vyatkа State University, 36 Moskovskaya St., Kirov, 610000, Russia.
Citation: D. A. Kataev, V. I. Tsirkin, A. N. Trukhin, S. I. Trukhina, (2026), Formation and Regression of Sports Vagotonia (Based on Heart Rate Variability Data Under Conditions of Active Orthostasis), Clinical Trials and Clinical Research,5(1); DOI:10.31579/2834-5126/103
Copyright: © 2026, I. Tsirkin. This is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 September 2025 | Accepted: 16 January 2026 | Published: 26 January 2026
Keywords: heart rate variability; clinostasis; orthostasis; cross-country skiers; parasympathetic and sympathetic divisions; autonomic nervous system, non-neuronal acetylcholine; sports vagotonia
Abstract
Analysis of 15 heart rate variability (HRV) indices recorded during active orthostasis showed that elite skiers of the Republic of Tatarstan (ESRT) in the preparatory period had higher medians of 9 HRV-indices, including TP, APHF, APVLF, APLF, RRNN, pNN50%, RMSSD, SDNN, MxDMn, than ranked skiers (YSRT), while medians of HR and SI, on the contrary, were lower, and medians of HF%, VLF%, LF% and APLF/APHF were the same as in YSRT. Consequently, ESRT had higher activity of the parasympathetic division (PD) of the autonomic nervous system (ANS) and, probably, the intensity of NN-Ach synthesis than in YSRT. It was established that ESRT and YSRT differ in the nature of changes in ortho-HRV during the 6-month preparatory period, which is a consequence of a higher level of PO activity and, probably, NN-Ach synthesis in ESRT. It was shown that a 7-month (from April to October 2024 inclusive) forced cessation of training in elite skier K.D. is accompanied by a gradual decrease (to the level typical for non-athletes) in the medians of 11 ortho-HRV indicators (TP, APHF, HF%, APVLF, VLF%, APLF, RRNN, pNN50%, RMSSD, SDNN and MxDMn) and an increase in the medians of LF%, APLF/APHF, HR and SI, which reflects a decrease in the activity of the sympathetic division (SD) and PD, and, probably, NN-Ach synthesis. But there is a partial preservation of NN-Ach synthesis in K.D. indirectly evidenced by lower medians of ortho-АPLF and ortho-HR, and a higher median of ortho-RRNN than in non-athletes, as well as the nature of the change in the medians of ТР, АPVLF, pNN50%, SDNN and MxDMn during the transition from clinostasis to active orthostasis. Thus, the regression of sports vagotonia occurs much faster (in a few months in the absence of training) than its formation, which requires many years (13-20 years) of continuous large-volume training loads.
Introduction
Previously, based on literature data [1-8] on the ability of the human and animal heart to synthesize non-neuronal acetylcholine (NN-Ach), as well as on the basis of analysis of heart rate variability (HRV), it was postulated [8, 9] that sports vagotonia, characteristic of endurance athletes, including for skiers-riders, due to the fact that along with an increase in the activity of the parasympathetic division (PD) of the autonomic nervous system (ANS), cardiomyocytes of the ventricles of the heart begin to synthesize NN-Ach as a component of the anti-apoptotic system, thanks to which the heart is doing a lot of work (like a pump) under the influence of catecholamines, it remains viable, despite the presence of high levels of reactive oxygen species (ROS) and the damaging effects of catecholamines that activate beta1-AR of the myocardium. The purpose of this article is to further confirm this hypothesis based on a comparative analysis of the dynamics of the medians of 15 HRV indicators recorded during the transition from clinostasis to active orthostasis in elite skiers (MS and MSIC) and young skiers aged 17-18 (1st and 2nd adult sports categories) during the 6-month preparatory period, as well as on based on the analysis of the dynamics of the medians of 15 ortho-HRV indicators of an elite skier for 7 months after the forced cessation of training loads. The study is based on a working hypothesis, according to which, in the process of endurance training, along with an increase in the activity of SD and PD of ANS, the synthesis of NN-Ach begins in the myocardium, the intensity of which gradually (from year to year) reaches a maximum in elite skiers as the experience of skiing increases, and in skiers for 1-2 adult categories, its level is still not high enough. Therefore, the values of HRV indicators reflecting the activity of the PD of ANS and, probably, the level of synthesis of NN-Ach should be higher in elite skiers than in discharge skiers, and the process of adaptation of the body of a ski racer in the preparatory period will take place both in elite skiers and in there are different ways for young skiers. In particular, during the transition from clinostasis to active orthostasis, the activity of the SD of ANS should increase in both groups, but it is opposed by the activity of the PD of ANS, which is realized by neuronal (vagal) Ach (N-Ach) and non-neuronal Ach (NN-Ach). The higher the level of NN-Ach synthesis and the higher the activity of PD ANS, the activity of the SD ANS should be the more strongly suppressed under conditions of active orthostasis. In addition, if an elite skier is forced to stop training loads, there should be a gradual (over several months?) in addition to a decrease in the activity of SD of ANS, a decrease in the activity of PD ANS, including due to a decrease in the synthesis of NN-Ach.
Materials and research methods
Heart rate variability (HRV) was recorded in two groups of skiers and in an elite skier, K.D., who had to stop training due to a sports injury, and therefore served as an object of research into the regression of sports vagotonia. The first group consists of 8 elite ski racers, members of the men's national team of the Republic of Tatarstan (hereinafter – ESRT), including 6 Masters of Sports (MS) and 2 masters of sports of international class (MSIC). Their ages ranged from 23 to 31 years old, and their work experience ranged from 13 to 20 years. Among them was skier K.D. (MS, the first author of the article), who represents the third object of our research. Training camps (TC) and competitions at the ESRT were held in different regions of Russia and beyond, including in lowland and mountainous climatic conditions, as previously reported in detail [9]. In this paper, HRV indicators registered with the ESRT during the preparatory period, which took place from June to November 2019, were analyzed. The second group of the study, or the comparison group, consists of 11 ski racers of the 1st and 2nd adult categories – members of the youth national team of the Republic of Tatarstan (hereinafter referred to as the YSRT), who represent the age group "senior boys 17-18 years old". Their skiing experience was 5-7 years, i.e. less than that of the ESRT. HRV registration in conditions of orthostasis was also carried out in the preparatory period of 2023 (from June to November). The training camps of this group took place in June at the Yalchik recreation center (Republic of Mari El); in July – in Mirny (Republic of Tatarstan); in August – in Dombay (Republic of Karachay-Cherkessia) at an altitude of 1600 m; in September and October – in Mirny (Republic of Tatarstan), in the first half of November – at the Pearl of Siberia Winter Sports Center (Tyumen Region), and in the second half of November – at the R. Smetanina Ski Complex (Komi Republic) It should be noted that the preparatory period for ESRT and YSRT was carried out for 6 months. Each month consisted of 3 microcycles, i.e. 3 weeks, and a week of rest at home. Each week, or microcycle, consisted of 5 training days (2 workouts + morning exercises), one unloading day (1 workout per day) and a day off (without training). During the week-long rest period between the next TC, the skiers conducted 1 training session per day at home. In both groups, track and field and cross-country running, roller skiing (roller skiing), and cross-country skiing in November formed the basis of training in the preparatory period. According to the data recorded by the skier K.D. in 2019, during the preparatory period, the total load of the ESRT was 5278 km or 375.5 hours, in particular, in June – 989 km (66.5 hours/month), in July – 1180 km (70 h/month), in August – 857 km (72 h/month), in September – 876 km (57.5 h/month), in October – 578 km (50 h/month), in November – 597 km (55 h/month). According to the data recorded by the leader of the YSRT, the total training load for the entire preparatory period was 3495 km or 371 hours/month, in particular, in June – 771 km (82 h/month), in July – 672 km (62 h/month), in August – 450 km (55 h/month), in September – 636 km (61 h/month), in October – 369 km (56 h/month), in November – 597 km (55 h/month). Thus, although the total duration of training for the YSRT was the same as for the ESRT, the mileage was lower, and therefore the average speed of movement was lower (9.4 km/h versus 13.1 km/h), since their physical fitness did not allow them to develop the same performance as the ESRT. The third object of the study was skier K.D., whose HRV registration (in conditions of clinostasis and orthostasis) was carried out from April 2024 to October 2024. Due to damage to the tendons of the adductor muscles of the left thigh, which is known [10] to be characteristic of Adduktor-Rectus-Symphysis syndrome (ARS), he was forced to stop training at the end of March 2024, performing only everyday physical activity, although before the injury he was a "playing" ski coach races for the YSRT team. Therefore, it was possible to assess the regression process of sports vagotonia, taking into account the availability of HRV data for the athlete K.D., when he was a member of the Tatarstan national team (ESRT) in 2019 and 2020. In all the subjects, the cardiointervalogram (CIG) was recorded personally by K.D. Initially, it was performed for 5 minutes in the "supine" position of the subject (clinostasis), and then for 5 minutes in the orthostasis position, the transition to which is carried out actively, i.e. with independent lifting of the subject. When analyzing ortho-cardiointervalograms (ortho-CIG), the first 10 seconds of recording were excluded, i.e. the transition process was not analyzed. Previously, each subject was informed that in the event of discomfort (dizziness, etc.) during standing, the subject should immediately take a "sitting" or even a "lying" position (in passing, we note that the need for this arose only once in one of the members of the USRT team). All the studies were conducted after a night's sleep, before breakfast, in comfortable conditions using the VNS-Micro system (Neurosoft, Russia), and the CIG analysis was performed using the Polyspectr program (Neurosoft, Russia). The generally accepted 8 spectral and 7 temporal parameters of HRV were analyzed. Among the spectral indicators of HRV are the total power of the spectrum (TP, mc2), or total power; the absolute power (mc2) of fast (HF-) waves, slow (LF-) waves and very slow (VLF-) waves (further, respectively, APНF, APLF and APVLF); the ratio APLF/APHF; the relative power of HF-, LF-, and VLF- waves, i.e., the wave power expressed as a percentage of TP (further – HF%, LF%, and VLF%, respectively). Among the time indicators, the duration of normal R-R intervals (RRNN, ms) was analyzed, which is analogous to heart rate (HR, beats/min); the ratio of consecutive NN-intervals, the difference between which exceeds 50 ms, as a percentage of the total number of normal (NN) R-R intervals (pNN50%); the square root of the average the square of the differences in the values of consecutive pairs of NN intervals (RMSSD, ms); the standard deviation of all NN intervals (SDNN, ms); the variation range (MxDMn, ms), i.e. the difference between the maximum and minimum R-R intervals; as well as the stress index (SI, conventional units), which was calculated using the formula: SI = AMo / Mo × 2MxDMn, where AMo is the amplitude of the mode, i.e. the most common value of the R-R-intervals of ECG, expressed as % of all R-R intervals; Mo – is the absolute value of the mode (s), and MxDMn is the variation range, i.e. the difference between the maximum and minimum values of the R-R intervals (s). To quantify the manifestation of the orthostatic test (Prevel reflex), a "delta" was calculated, i.e., the difference in the medians of the indicators recorded under conditions of clinostasis and orthostasis, respectively. For indicators that were expressed in ms, ms2, or b/pm (RRNN, HR, pNN50%, RMSSD, SDNN, MxDMn, TP, APHF, APVLF, APLF), as well as for pNN50%, the delta was expressed as a percentage and calculated using the formula: Delta = 100% - Delta = 100% - (PORTO/PCLINO)x100, where P is the HRV indicator. The delta for the relative values (SI, HF%, VLF%, LF% and APLF\APHF), expressed in conventional units or as a percentage, was calculated using the formula: Delta = PORTO - PCLINO. The assessment of these indicators was formed by summing up the results of individual studies in each month of the preparatory period. The ESRT had 146 registrations (i.e., almost daily), the YSRT had 141 СIG registrations; and the elite skier, K.D., had 19, 22, 29, and 15 СIG registrations in April, June, August, and October, respectively. All the results were expressed as medians, 25 and 75 centiles [11]. The Mann-Whitney criterion was used to evaluate the differences, considering them statistically significant at p < 0.05 [11]. The research was approved by the local Bioethical Committee of Vyatka State University (Protocol No. 1 dated 17.01.2020).
The results of the study and their discussions
1. Comparison of the medians of 15 indicators of ortho-HRV in ESRT and in YSRT, which are characteristic in general for the entire preparatory period (July-November) This comparison revealed (Table. 1; Fig. 1, 2), that the medians of 11 ortho-HRV indicators differed, and 9 of them, reflecting mainly PD of ANS activity, were higher in ESRT than in YSRT (these are TP, APHF, APVLF, APLF, RRNN, pNN50%, RMSSD, SDNN, MxDMn), and the medians of HR and SI were lower than those of YSRT. At the same time, the medians of the other 4 HRV-indicators, namely, HF%, VLF%, LF% и АPLF/АPHF did not differ between ESRT and YSRT. At the same time, the structure of the total power of the HRV spectrum, i.e. the TP structure of ESRT and YSRT turned out to be the same – the power of LF-waves is in the first place, the power of VLF-waves is in the second place, and the power of HF-waves is in the last place, i.e. LF>VLF>HF. This indicates that in the vertical position of both ESRT and YSRT is dominated by the influence of SD ANS on the activity of the heart.
2. The difference (delta) between the median of the corresponding ortho-HRV and clino-HRV indices, or the change in the median HRV indices during the active transition from clinostasis to orthostasis in general for the entire preparatory period for ESRT and YSRT
Shown (Table. 2 and 3, Fig. 1 and 2), that the change in the medians of 10 HRV-indices during the active transition from clinostasis to orthostasis, i.e. the difference between ortho-HRV and clino-HRV (or delta-HRV) was the same in the ESRT and YSRT groups. These are such indicators as delta-TP (it was minus 52% of the median clino-TP for ESRT, and minus 56% for YSRT); delta-APHF (minus 91% and minus 92%, respectively), delta-APVLF (minus 44% and minus 56%), delta-VLF% (plus 4% and plus 4%), delta-АPLF/АPНF (plus 6.2 conc. units, and 6.3 conc. units), delta-RRNN (minus 35% and minus 32%), delta-HR (plus 66% and plus 51%), delta-RMSSD (minus 70% and minus 60%), delta-SDNN (minus 32% and minus 33%) and delta-MxDMn (minus 31% and minus 32%). But the medians of the delta of the 5 HRV indices had statistically significant differences (p<0.05). These are: 1) delta-HF% (minus 33% for ESRT versus minus 22% for YSRT); 2) delta-APLF (plus 23% versus minus 28%); 3) delta-LF% (plus 14% versus plus 28%); 4) delta-pNN50% (minus 82% versus minus 89%) and 5) delta-SI (plus 28% versus plus 57%). These differences indicate that YSRT probably has a lower level of NN-Ach synthesis compared to ESRT, since the inhibition of the growth of SD ANS activity during the transition from clinostasis to orthostasis in YSRT is less than in ESRT. This is indicated, in particular, by HRV indicators such as delta-HF%, delta-LF% and delta-SI.
Indicators HRV | Preparatory period | |||||||||||||
| June (6) | July (7) | August (8) | September (9) | October (10) | November (11) | Overall | ||||||||
| YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | |
| TP, ms2 | 1937 1300/4750 | 4928* 3724/8362 | 4401 2551/8567 | 6020 3822/8464 | 2746 1747/5508 | 5696* 3956/7244 | 3229 2442/5138 | 5282* 4463/7428 | 2727 1784/4321 | 4184 3062/5342 | 3421 2094/6133 | 6025* 4301/7954 | 3241 1844/5663 | 5317* 3742/7547 |
| Differ | - | - | 6 | - | 7 | - | - | - | - | 7,9 | - | 10 | - | - |
| АPHF, ms2 | 281 132/361 | 365 * 238/826 | 272 146/412 | 570 * 362/1087 | 197 113/381 | 434 * 268/587 | 235 137/325 | 306 204/596 | 223 91/293 | 175 137/225 | 189 120/406 | 400* 180/505 | 220 126/379 | 390* 188/617 |
| Differ | - | - | - | - | - | - | - | 7 | - | 6,7,8,9 | - | 7,10 | - | - |
HF, % | 7,5 5/10 | 7,5 4/16 | 6 3/8 | 12,1* 5/17 | 6,4 5/9 | 8,5 5/10 | 5,5 3/7 | 5,4 3/9 | 8,4 3/11 | 4,1 3/5 | 6 4/7 | 6,4 4/8 | 6,4 4/10 | 6,8 4/12 |
| Differ | - | - | - | - | - | - | - | 7 | - | 6,7,8 | - | 7,10 | - | - |
| АPVLF, ms2 | 808 622/1770 | 1602* 1197/2317 | 1586 849/2566 | 2048 1099/2989 | 919 484/1650 | 1604* 1098/2304 | 810 540/1587 | 2032* 1399/3353 | 924 517/1174 | 1331 930/1982 | 1165 565/1695 | 1706* 1300/2253 | 1063 584/1824 | 1643* 1110/2719 |
| Differ | - | - | - | - | 7 | - | 7 | - | - | 9 | - | - | - | - |
| VLF, % | 43,5 27/59 | 33,2 20/48 | 35,4 23/50 | 40,7 26/49 | 41,5 17/60 | 35,7 22/54 | 35,4 19/38 | 46,1 29/66 | 48,9 19/68 | 41,5 23/46 | 34,8 21/52 | 34,7 23/42 | 35,6 21/57 | 36,4 22/51 |
| Differ | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| АPLF, ms2 | 797 438/2342 | 2624* 1430/4380 | 2716 898/4674 | 1969 1494/3921 | 1156 526/3659 | 3101 961/4047 | 2074 920/3494 | 2365 1734/3389 | 1030 493/1927 | 2515* 1489/3417 | 1569 1044/3942 | 3189* 2276/4913 | 1592 684/3620 | 2496* 1442/3942 |
| Differ | - | - | 6 | - | - | - | - | - | - | - | - | - | - | - |
LF, % | 44,5 32/62 | 55,8 41/67 | 48,5 16/67 | 43,6 30/65 | 52,4 32/70 | 53,6 33/66 | 61,5 43/72 | 44,8 27/64 | 42,1 17/71 | 53,6 49/73 | 59,4 41/69 | 56,5 50/69 | 50,8 30/69 | 53,0 34/69 |
| Differ | - | - | - | - | - | - | - | - | - | 7,9 | - | 7 | - | - |
АPLF/ АPH, rel. u. | 5,3 3,1/9,4 | 7,0 2,3/12,8 | 8,9 4,3/16,8 | 3,5* 1,3/9,6 | 4,5 3,4/10,6 | 6,3 2,3/10,8 | 11,1 6,4/12,5 | 6,1 3,9/13,9 | 4,9 3,8/8,4 | 13,6* 10,5/19,1 | 8,1 6,0/12,7 | 9,4 5,4/15,3 | 7,76 4,0/12,7 | 7,0 3,0/14,0 |
| Differ. | - | - | - | - | - | - | 6 | 7 | - | 6,7,8,9 | - | 7,8 | - | - |
| RRNN, мс | 693 659/768 | 901* 883/963 | 726 666/872 | 1017* 902/1099 | 646 581/762 | 900* 814/950 | 708 634/760 | 906* 830/973 | 746 550/769 | 782 * 738/850 | 700 651/728 | 909* 835/962 | 705 623/774 | 906* 835/989 |
| Differ | - | - | - | 6 | 7 | 7 | - | 7 | - | 6,7,8,9 | 7 | 7 | - | - |
| HR, bpm | 86,6 78/91 | 66,6 * 62/68 | 82,6 68/90 | 59,0 * 54/66 | 92,9 78/103 | 66,6* 63/73 | 84,7 79/94 | 66,2* 61/72 | 80,5 77/109 | 76,7* 70/81 | 85,7 82/92 | 66,0* 62/71 | 85,1 77/96 | 66,2* 60/71 |
| Differ | - | - | - | 6 | 7 | 7 | - | 7 | - | 6,7,8,9 | 7 | 7,10 | - | - |
| pNN50, % | 3,3 1/7 | 14,5* 5/22 | 6,9 2/13 | 22,7* 10/37 | 2,6 0/11 | 12,4* 5/17 | 5,1 4/8 | 8,0* 5/15 | 4,6 1/9 | 5,0 2/6 | 4,9 1/8 | 10,4* 5/16 | 4,9 1/10 | 10,8* 5/19 |
| Differ | - | - | - | - | - | 7 | - | 7 | - | 6,7,8,9 | - | 7,10 | - | - |
RMSSD, ms | 22 16/33 | 35* 30/45 | 31 20/40 | 44* 33/63 | 20 13/33 | 35* 27/43 | 25 22/30 | 33* 28/38 | 23 12/31 | 26 19/31 | 25 19/30 | 37* 26/42 | 26 18/34 | 35* 27/43 |
| Differ | - | - | - | - | - | 7 | - | 7 | - | 6,7,8,9 | - | 7,10 | - | - |
| SDNN, ms | 44 36/68 | 70* 60/90 | 66 49/90 | 78 62/92 | 52 41/71 | 74* 58/84 | 54 48/70 | 71* 66/84 | 52 41/65 | 63 55/71 | 57 47/74 | 77* 66/91 | 56 43/75 | 72* 61/85 |
| Differ | - | - | 6 | - | 7 | - | - | - | - | 7,9 | - | 10 | - | - |
| MxDMn, ms | 230 180/318 | 343* 294/428 | 331 258/402 | 410* 327/508 | 251 208/356 | 382* 277/445 | 273 218/359 | 377* 325/419 | 256 207/332 | 322* 285/361 | 277 224/368 | 392* 345/434 | 276 212/364 | 368* 300/450 |
| Differ | - | - | 6 | - | - | - | - | - | 7 | 7,9 | - | - | - | - |
SI, con. u. | 141,1 58/213 | 47,3* 31/63 | 66,8 40/143 | 34,7* 23/48 | 113,1 64/206 | 42,4* 33/73 | 99,0 64/147 | 42,0* 36/55 | 99,8 58/232 | 74,1 49/91 | 97,2 57/132 | 43,9* 35/68 | 96,9 50/162 | 44,3* 32/68 |
| Differ | - | - | 6 | - | 7 | 7 | - | 7 | - | 6,7,8,9 | - | 7,10 | - | - |
Table 1: Median, 25 and 75 values of spectral and temporal indicators of ortho-HRV in ESRT and YSRT during each of the 6 months of the preparatory period and in general for the entire period.
Note: * – the differences between the months and, in general, for the entire preparatory period between the groups of athletes are statistically significant, p<0.05; the numbers in the "Difference" lines reflect the month with which the indicator in this month of the preparatory period differs statistically significantly (p<0.05, according to the Mann-Whitney criterion) from the indicators of other months of this period/and the dash indicates that there are no differences. The interpretation of HRV indicators is given in the "Methodology" section.
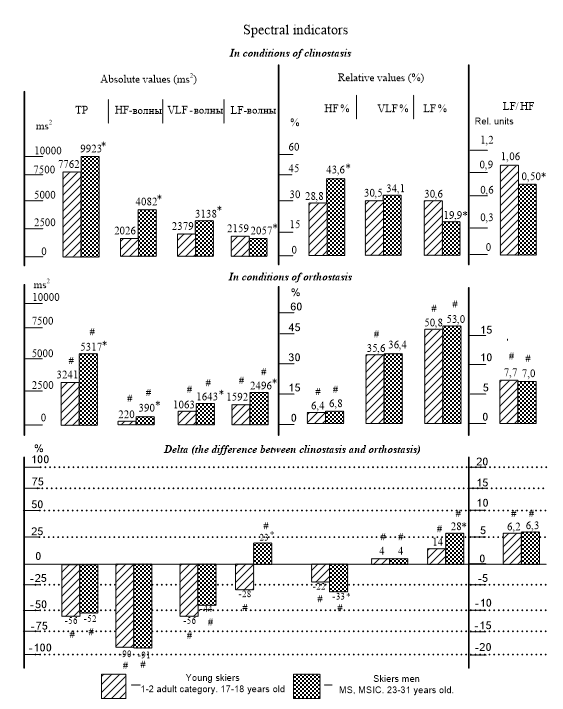
Figure 1: Medians of clino-HRV (upper row), ortho-HRV (middle row) and delta (lower row) indicators, i.e. the difference between clino-HRV and ortho-HRV in YSLRT and ESRT (in general, for the entire preparatory period), including TP (mc2), absolute the power of HF-, VLF-, and LF-waves (mc2), the relative (in % to TP) power of these waves, the APLF/APHF ratio.
Note: the * symbol means that the differences between the indicators of the groups are statistically significant, p<0.05; the # symbol in the second row means that the differences between clinostasis and orthostasis are statistically significant, p<0.05; the # symbol in the third row means that the changes, i.e. the median delta (the difference between orthostasis and clinostasis) in the corresponding periods are statistically significant, p<0.05. The interpretation of HRV indicators and the calculation of the delta are described in the "Methodology" section.
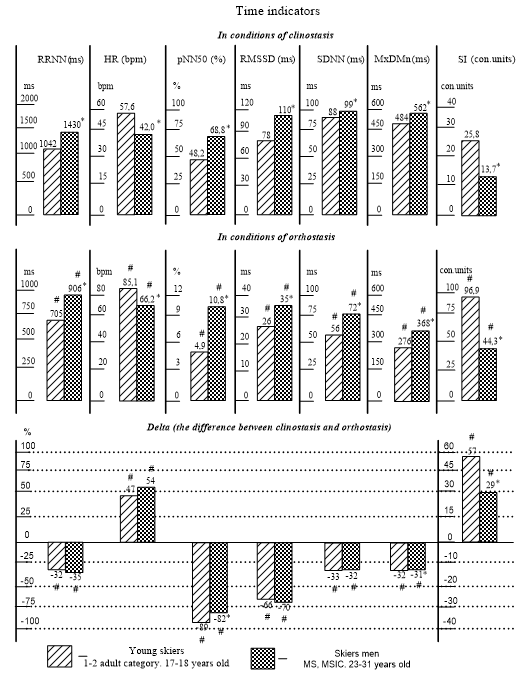
Figure 2: Medians of clino-HRV (upper row), ortho-HRV (middle row) and delta (lower row), i.e. the difference between clino- and ortho-HRV in YSRT and ESRT (in general, for the entire preparatory period), including RRNN (ms), HR (b/pm), pNN50% (%), RMSSD (ms), SDNN (ms), MxDMn (ms), SI (conl. units).
Note: * – the differences between the months and, in general, for the entire preparatory period between the groups of athletes are statistically significant, p<0.05; the numbers in the "Difference" lines reflect the month with which the indicator in this month of the preparatory period differs statistically significantly (p<0.05, according to the Mann-Whitney criterion) from the indicators of other months of this period. period, and the dash indicates that there are no differences. The interpretation of HRV indicators is given in the "Methodology" section.
Delta -HRV index | Preparatory period | |||||||||||||
| June (6) | July (7) | August (8) | September (9) | October (10) | November (11) | Overall | ||||||||
| YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | |
| TP, % | -63 -88/-17 | -55 -63/-46 | -32 -79/24 | -43 -66/-16 | -45 -79/-30 | -59 -76/-29 | -65 -87/-9 | -44 -62/-17 | -64 -89/-57 | -53 -68/-30 | -64 -89/0 | -45 -68/-20 | -56 -85/-3 | -52 -69/-27 |
| Differ. | - | - | - | - | - | - | - | 8 | - | - | - | - | - | - |
| АPHF, % | -91 -97/-73 | -92 -95/-84 | -85 -93/-69 | -88 -95/-64 | -90 -95/-84 | -89 -96/-80 | -86 -98/-75 | -91 -95/-77 | -93 -96/-84 | -96 -97/-93 | -91 -94/-84 | -16 -24/-11 | -90 -96/-76 | -91 -96/-81 |
| Differ. | - | - | - | - | - | - | - | - | - | 6,7,8,9 | 10 | 6,8 | - | - |
HF, % | -28 -42/-16 | -36 -42/-22 | -19 -28/-13 | -24 -33/-14 | -30 -37/-17 | -32 -41/-17 | -16 -25/-12 | -32* -41/-18 | -27 -38/-12 | -52* -58/-38 | -16 -24/-11 | -34 -40/-27 | -22 -32/-13 | -33* -44/-20 |
| Differ. | - | - | - | 6 | - | - | 6,8 | - | - | 6,7,8,9 | 6,8 | 7,11 | - | - |
| АPVLF, % | -59 -77/56 | -53 -68/-19 | -14 -64/52 | -38 -79/31 | -63 -74/6 | -61 -80/11 | -67 -87/4 | -31 -71/25 | -57 -81/-11 | -33 -60/44 | -59 -86/3 | -46 -71/-18 | -56 -81/14 | -44 -73/16 |
| Differ. | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| VLF, % | 18 0/29 | 4* -3/11 | 3 -5/15 | 3 -14/15 | 2 -11/21 | -3 -8/16 | -3 -12/10 | -7 -10/17 | 19 2/29 | 12 -3/18 | 6 -8/18 | 3 -13/8 | 4 -8/14 | 4 -11/14 |
| Differ. | - | - | - | - | - | - | 6 | - | 9 | - | - | - | - | - |
| АPLF, % | -48 -71/23 | 7* -27/68 | 8 -56/73 | 24 -24/71 | -31 -70/21 | 6 -27/57 | -35 -76/46 | 22* -13/57 | 61* 11/130 | 1 -7/33 | -52 -89/54 | 39* 7/124 | -28 -75/46 | 23* -18/89 |
| Differ. | - | - | - | - | - | - | - | - | 8 | - | - | - | - | - |
LF, % | 13 0/35 | 36* 17/49 | 13 16/67 | 20 * 9/46 | 18 8/34 | 27 14/43 | 23 4/32 | 19 8/42 | 1 -7/33 | 40* 27/57 | 9 -4/33 | 37* 25/47 | 14 -1/32 | 28* 15/46 |
| Differ. | - | - | - | - | - | - | - | - | - | 7,8,9 | - | 7,9 | - | - |
АPLF/ АPHF, rel. u. | 4,6 2/8 | 6,1 1/12 | 7,3 3/14 | 3,0* 0/9 | 4,2 3/8 | 5,7 2/10 | 9,2 5/11 | 5,3 3/12 | 4,4 1/7 | 13,2* 10/18 | 6,6 4/11 | 8,9 4/13 | 6,25 3,0/10,9 | 6,3 2/13 |
| Differ. | - | - | - | - | - | - | - | 7 | - | 6,7,8,9 | - | 7,8,10 | - | - |
| RRNN, % | -33 -41/-25 | -34 -37/-29 | -31 -38/-22 | -29 -35/-21 | -32 -47/-25 | -33 -37/-29 | -30 -46/-23 | -35 -37/-33 | -32 -51/-24 | -42 -45/-41 | -33 -40/-23 | -39* -41/-36 | -32 -44/-23 | -35 -39/-29 |
| Differ. | - | - | - | 6 | - | 7 | - | 7 | - | 6,7,8,9 | - | 6,7,8,9,10 | - | - |
HR, % | 49 33/71 | 51 41/60 | 45 29/62 | 41 26/54 | 47 33/91 | 51 42/59 | 43 29/88 | 55 49/60 | 48 32/105 | 73 71/83 | 51 30/69 | 66* 56/69 | 47 30/79 | 54 42/65 |
| Differ. | - | - | - | 6 | - | 7 | - | 7 | - | 6,7,8,9 | - | 6,7,8,9,10 | - | - |
| pNN50, % | -92 -98/-77 | -79* -91/-67 | -85 -95/-60 | -68* -84/-37 | -93 -98/-75 | -80 -90/-75 | -86 -93/-78 | -87 10 -92/-74 | -92 -97/-76 | -93 -96/-91 | -90 -96/-73 | -83 -92/-78 | -89 -97/-71 | -82* -92/-72 |
| Differ. | - | - | - | 6 | - | 7 | - | 7 | - | 6,7,8,9 | - | 7,10 | - | - |
RMSSD, % | -75 -85/-48 | -70 -74/-66 | -57 -77/-37 | -64 -72/-38 | -69 -53/-81 | -70 -61/-81 | -63 -87/-49 | -67 -72/-61 | -74 -89/-59 | -78 -84/-72 | -72 -50/-84 | -69 -73/-60 | -66 -83/-48 | -70 -77/-60 |
| Differ. | - | - | - | - | - | 7 | - | - | 7 | 6,7,8,9 | - | 10 | - | - |
| SDNN, % | -40 -65/-11 | -34 -50/-26 | -22 -55/2 | -28 -44/-10 | -31 -59/-17 | -39 -53/-17 | -41 -65/-11 | -23 -38/-7 | -41 -67/-34 | -34 -44/-17 | -46 -66/-5 | -22 -37/-9 | -33 -62/-6 | -32 -46/-15 |
| Differ. | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
MxDMn, % | -45 -65/-17 | -38 -50/-27 | -21 -54/-3 | -23 -41/-5 | -35 -55/-21 | -34 -50/-13 | -46 -69/-8 | -32 -40/-21 | -55 -60/-29 | -40 -46/-16 | -37 -60/-19 | -29 -41/-10 | -32 -61/-14 | -31* -46/-13 |
| Differ. | - | - | - | 6 | - | - | - | - | - | - | - | - | - | - |
SI, con. u. | 102 20/175 | 33* 17/52 | 37 10/111 | 19* 9/35 | 56 29/122 | 30* 14/59 | 66 24/136 | 26* 21/34 | 75 29/208 | 54 40/68 | 57 31/119 | 30* 20/45 | 57 24/134 | 29* 18/50 |
| Differ. | - | - | - | - | - | 7 | - | 7 | - | 6,7,8 | - | 7,9,10 | - | - |
Table 2: Median, 25 and 75 delta cents, i.e. the difference between the medians of the spectral and temporal parameters of clino-HRV and ortho -HRV in ESRT and YSRT during each of the 6 months of the preparatory period and in general for the entire period.
Note: * – the differences between the months and, in general, for the entire preparatory period between the groups of athletes are statistically significant, p<0.05; the numbers in the "Difference" lines reflect the month with which the indicator in this month of the preparatory period differs statistically significantly (p<0.05, according to the Mann-Whitney criterion) from the indicators of other months this period, and the dash indicates that there are no differences. The interpretation of HRV indicators is given in the "Methodology" section.
Indicators clino-HRV | Preparatory period | Overall | ||||||||||||
| June (6) | July (7) | August (8) | September (9) | October (10) | November (11) | |||||||||
| YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | YSRT | ESRT | |
| TP, ms2 | 7101 5369/13952 | 10862* 7724/19020 | 7412 5448/9370 | 10071* 5862/15784 | 8520 5561/10521 | 11201 8143/21088 | 8339 5208/11614 | 9420 6545/11993 | 7705 5846/10695 | 8612 4736/11822 | 7574 5118/20160 | 9913 7188/12358 | 7762 5267/11514 | 9923* 6658/14428 |
| Differ. | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| АPHF, ms2 | 2060 1473/6856 | 5142 3343/8243 | 1847 1323/3650 | 3990* 2209/7039 | 2706 1698/4206 | 4541* 2608/7656 | 1885 921/3393 | 3264* 2493/4552 | 3747 936/5369 | 4102 2938/5647 | 1541 1223/4709 | 3359* 2391/4910 | 2026 1307/4313 | 4082* 2576/6336 |
| Differ. | - | - | - | - | - | - | - | 6 | - | - | - | - | - | - |
HF, % | 35,3 25/61 | 45,0* 35/52 | 26,6 20/34 | 41,4* 32/49 | 33,9 23/47 | 44,2* 26/53 | 22,6 18/31 | 39,9* 26/46 | 43,6 19/51 | 56,5* 45/61 | 21,2 17/30 | 44,0* 34/48 | 28,8 20/39 | 43,6* 32/52 |
| Differ. | - | - | 6 | - | 7 | - | 6,8 | - | - | 7,8,9 | 6,8 | 10 | - | - |
| АPVLF, ms2 | 2083 1134/3229 | 3726* 2239/4462 | 1849 1173/3978 | 2941* 1800/5577 | 2764 1389/3869 | 3540 2090/6190 | 2361 1543/5577 | 3397 1961/5952 | 2627 1662/3416 | 1711 1096/3075 | 2539 1526/5028 | 3495 2222/5891 | 2379 1329/3874 | 3138* 1818/5611 |
| Differ. | - | - | - | - | - | - | - | - | - | 6,7,8, 9 | - | 10 | - | - |
| VLF, % | 28,7 16/39 | 35,6 20/39 | 30,5 22/45 | 39,1 32/48 | 31,1 25/42 | 33,2 26/52 | 35,5 22/46 | 36,7 29/55 | 28,9 15/41 | 25,0 15/31 | 30,5 21/41 | 34,1 24/42 | 30,5 21/43 | 34,1 24/45 |
| Differ. | - | - | - | - | - | - | - | - | - | 6,7,8, 9 | - | 10 | - | - |
| АPLF, ms2 | 1741 1425/2965 | 2300 1373/3605 | 2480 1537/4101 | 2013 1123/2994 | 1526 1108/5260 | 2912 974/4305 | 2791 1514/4398 | 1912 1403/2684 | 1734 1366/3557 | 1316 895/2755 | 3037 1611/6225 | 2101 1298/3220 | 2159 1402/4480 | 2057* 1119/3202 |
| Differ. | - | - | - | - | - | - | - | - | - | 6 | 8 | - | - | - |
LF, % | 26,3 15/37 | 21,0* 15/22 | 35,9 19/47 | 19,3* 13/24 | 24,3 17/43 | 21,1 12/27 | 34,3 23/50 | 20,8* 14/24 | 24,4 20/34 | 16,3* 12/23 | 37,7 29/55 | 21,8* 14/26 | 30,6 20/48 | 19,9* 14/25 |
| Differ. | - | - | - | - | - | - | - | - | - | - | 6,8 | - | - | - |
АPLF/ АPHF, rel. u. | 0,76 0,23/1,65 | 0,48 0,32/0,64 | 1,07 0,78/2,24 | 0,48 * 0,38/0,65 | 0,59 0,43/1,32 | 0,51 0,33/0,71 | 1,28 0,83/2,34 | 0,55* 0,4/0,75 | 0,84 0,39/1,66 | 0,34* 0,22/0,48 | 1,3 0,98/2,97 | 0,56* 0,41/0,65 | 1,06 0,6/2,2 | 0,50* 0,34/0,65 |
| Differ. | - | - | 6 | - | 7 | - | 6,8 | - | - | 7,8,9 | 6,8 | 10 | - | - |
| RRNN, ms | 1007 943/1120 | 1388 * 1272/1460 | 1086 983/1218 | 1438 * 1324/1539 | 1112 882/1189 | 1339 * 1236/1466 | 1036 965/1185 | 1464* 1293/1521 | 1038 962/1107 | 1420* 1282/1484 | 1049 934/1179 | 1506* 1398/1540 | 1042 951/1189 | 1430* 1291/1515 |
| Differ. | - | - | - | - | - | 7 | - | - | - | - | - | 6,8,10 | - | - |
| HR, bpm | 59,5 53/63 | 43,2 * 41/47 | 55,3 49/61 | 41,7* 39/45 | 54,0 50/68 | 44,7 * 40/48 | 57,9 50/62 | 41,0* 39/46 | 57,8 54/62 | 42,2* 40/46 | 57,2 50/64 | 39,8* 38/42 | 57,6 50/63 | 42,0* 39/46 |
| Differ. | - | - | - | - | - | 7 | - | - | - | - | - | 6,8,10 | - | - |
| pNN50, % | 48,9 40/61 | 70,1* 56/79 | 48,0 39/53 | 68,2* 58/74 | 51,6 40/65 | 67,8* 47/73 | 44,0 26/59 | 66,3* 60/71 | 51,7 37/57 | 71,4* 66/78 | 44,0 32/62 | 68,4* 63/74 | 48,2 37/61 | 68,8* 58/75 |
| Differ. | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| RMSSD, ms | 79 61/110 | 129 * 108/154 | 78 64/99 | 115* 92/156 | 81 71/110 | 114* 80/177 | 70 57/104 | 100* 90/110 | 80 65/98 | 118* 93/125 | 72 55/136 | 101* 91/119 | 78 60/102 | 110* 92/135 |
| Differ. | - | - | - | - | - | - | - | 6 | - | - | - | - | - | - |
| SDNN, ms | 85 76/112 | 112* 88/135 | 87 75/101 | 104* 81/124 | 94 74/104 | 102 91/136 | 89 74/111 | 88 82/116 | 88 78/103 | 91 74/103 | 90 71/142 | 95 82/110 | 88 74/107 | 99* 84/123 |
| Differ. | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| MxDMn, ms | 492 396/557 | 584* 549/617 | 446 366/553 | 584* 424/640 | 497 389/585 | 578 462/644 | 487 408/543 | 503 452/643 | 485 431/507 | 529 389/585 | 503 407/653 | 518 472/609 | 484 389/565 | 562* 451/636 |
| Differ. | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
SI, con. u. | 28,7 20/35 | 13,1* 8/19 | 23,4 18/34 | 12,1* 9/19 | 25,8 16/37 | 13,9* 8/21 | 25,7 17/37 | 16,8* 10/19 | 26,9 22/35 | 16,1 12/28 | 21,3 16/41 | 14,2* 10/19 | 25,8 17/38 | 13,7* 10/20 |
| Differ. | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
Table 3: Median, 25, and 75 cents of the spectral and temporal parameters of clinо-HRV in ESRT and YSRT for each of the 6 months of the preparatory period and for the entire period as a whole.
Note: * – the differences between the months and, in general, for the entire preparatory period between the groups of athletes are statistically significant, p<0.05; the numbers in the "Difference" lines reflect the month with which the indicator in this month of the preparatory period differs statistically significantly (p<0.05, according to the Mann-Whitney criterion) from the indicators of other months of this period. period, and the dash indicates that there are no differences. The interpretation of HRV indicators is given in the "Methodology" section.
An analysis of the changes in the structure of TP-waves during the transition from clinostasis to active orthostasis showed that in ESRT, in conditions of clinostasis, the TP structure had the form "HF>VLF>LF", i.e. 43.6%>34.1%>19.9%. This means that in the structure of clino-TP, HF-waves are in the first place, and LF-waves are in the last place. But in conditions of orthostasis, the TP-structure of ESRT had the form "LF>VLF>HF" (53.0%>36.4%>6.8%), that is, LF-waves have moved to the first place. In other words, in ESRT during the transition from clinostasis to active orthostasis, as predicted by theory, the activity of LF-waves increases significantly. In the case of YSRT in a state of clinostasis, the TP structure had the form "LF>VLF>HF" (36.6%>30.5%>28.8%), that is, LF-waves were in the first place, and HF-waves were in the third place. But in conditions of orthostasis, the TP structure in YSRT had the form "LF>VLF>HF" (50.8%>35.6%>6.4%), that is, as expected when implementing the Prevel reflex, the activity of the SD ANS increases and the activity of the PD ANS decreases significantly. Thus, there was no significant difference between the ESRT and YSRT groups in the structure of TP-waves and its change during the transition from clinostasis to orthostasis. Although, based on the ideas about the inhibitory effect of NN-Ach on the activity of the SD ANS during the implementation of the Prevel reflex [12], it was expected that the growth of the median of LF% in YSRT would be more pronounced than in ESRT, since, according to the working hypothesis, the intensity of synthesis of NN-Ach in YSRT is probably lower than in ESRT. But this was not really revealed (Tables 1, 2; Fig. 3) – in ESRT the median of LF% increased during the transition to active orthostasis from 19.9% to 53.0%, and in YSRT – from 30.6% to 50.8%. At the same time, attention is drawn to the fact that ESRT has a lower median of clino-LF% than YSRT (19.9% versus 30.6%). Indirectly, this can be interpreted as a reflection of the inhibitory effect of NN-Ach on the activity of CD ANS, manifested in ESRT in clinostasis. For further indirect comparative analysis of the level of NN-Ach synthesis in ESRT and YSRT, we used five criteria proposed earlier [12] for the presence of NN-Ach synthesis based on the nature of differences between the median of ortho-HRV and clino-HRV indices. According to the first criterion, in the presence of NN-Ach synthesis in the myocardium, the median of TP is characterized by high values in conditions of clinostasis and its decrease during the active transition to orthostasis, and in the absence of NN-Ach synthesis, the median of TP is characterized by low values in clinostasis and their increase in orthostasis. According to this criterion, it can be argued that both ESRT and YSRT have NN-Ach synthesis, but differences in the intensity of NN-Ach synthesis, judging by the delta-TR value, are not detected between them. Indeed (Tables 2 and 3; Fig. 1) in conditions of clinostasis, the median of TP for ESRT was 9923 ms2, for YSRT – 7762 ms2, and with active orthostasis, the median of TP decreased by 56% and 52%, respectively. According to the second criterion, the median of absolute power of VLF waves (APVLF) decreases during the transition from clinostasis to active orthostasis in the presence of NN-Ach synthesis, and increases in the absence of NN-Ach synthesis. According to this criterion, both ESRT and YSRT synthesize NN-Ach, but there are no differences in the intensity of NN-Ach synthesis. Indeed (Tables 2 and 3; Fig. 1), in conditions of clinostasis, the median of APVLF in ESRT was 3138 ms2, in YSRT – 2349 ms2, and with active orthostasis, the median decreased by 44% and 56%, respectively. According to the third criterion, a marker of the presence of NN-Ach synthesis in the heart are high (above 60%) values of the median pNN50% in conditions of clinostasis and their marked decrease with active orthostasis, and in the absence of NN-Ach synthesis, extremely low values of the median of pNN50% in clinostasis (no higher than 20%) and low values (1-2%) in conditions of orthostasis. It is established (Tables 2 and 3; Fig. 2) that in conditions of clinostasis, the median of pNN50% for ESRT was 68.8%, and for YSRT – 48.2%, and with active orthostasis, the median decreased to 10.8% and 4.9%, respectively. This allows us to conclude that ESRT and YSRT have a synthesis of NN-Ach, but YSRT has a lower synthesis of NN-Ach than ESRT. According to the fourth criterion, a marker of the presence of NN-Ach synthesis in the heart is a decrease in the median of SDNN by 20% or higher during the transition from clinostasis to active orthostasis. It is established (Tables 2 and 3; Fig. 2) that in conditions of clinostasis, the median of SDNN in ESRT was 99 ms, and in YSRT – 88 ms, and with active orthostasis, the median decreased by 32% and 33%, respectively. This indicates that NN-Ach synthesis occurs in both groups, but no differences in the intensity of NN-Ach synthesis are detected. According to the fifth criterion, a marker of the presence of NN-Ach synthesis in the heart is a decrease in the median MxDMn during the transition from clinostasis to active orthostasis by 10% or higher. It is established (Tables 2 and 3; Fig. 2) that in conditions of clinostasis, the median of MxDMn in ESRT was 562 ms, and in YSRT – 484 ms, and with active orthostasis, the median decreased by 31% and 32%, respectively. This indicates that NN-Ach synthesis occurs in both groups, but no differences in the intensity of NN-Ach synthesis are detected. Thus, all five criteria indirectly confirm the presence of NN-Ach synthesis among the ESRT and the YSRT. However, only one of these criteria, namely pNN50%, indirectly indicates that the synthesis of NN-Ach in YSRT is lower than in ESRT. At the same time, attention is drawn to the fact that the values of all five indicators in the conditions of clinostasis were significantly higher for ESRT than for YSRT (for TP – 9923 ms2 versus 7762 ms2, for APVLF – 3138 ms2 versus 2349 ms2, for pNN50% – 68.8% versus 48.2%, for SDNN – 99 ms versus 88 ms, and for MxDMn – 562 ms versus 484 ms). This fact, as noted above, indirectly confirms the idea that the intensity of synthesis of NN-Ach in ESRT is higher than that in YSRT. Summing up this section, we can conclude that we have confirmed the literature data that elite ski racers in conditions of orthostasis have medians of indicators reflecting activity in ANS, higher than those of discharge skiers, higher than those of representatives of other sports, and higher than those of non-athletes what is described in more detail below. This confirms our assumption that as the experience of skiing increases and as athletic skills increase, the activity of PD ANS increases in the heart of a ski racer, including by increasing the synthesis of NN-Ach by cardiomyocytes of the ventricles of the heart as a component of the anti-apoptotic system of the heart. It is obvious that the synthesis of NN-Ach reaches its maximum values precisely among elite skiers, which, with a significant increase in the activity of the SD ANS, allows them to achieve high athletic results. It has also been shown that with active orthostasis, the activation of SD ANS occurs, since in both groups (ESRT and YSRT) in an upright position, the activity of LF-waves dominates in the structure of TP rather than the activity of HF-waves, which is typical for clinostasis.
3. Dynamics of median ortho-HRV indicators during the preparatory period in ESRT and YSRT groups
Since the preparatory period lasted 6 months, it allowed for a monthly analysis of changes in the medians of ortho-HRV. It is established (Table 1; Fig. 3, 4), that the medians of the 3 indicators of ortho-HRV differed between the groups of ESRT and YSRT in each of the 6 months of the preparatory period, and in general throughout the period. At the same time, the medians of two of them (RRNN, MxDMn) were higher in ESRT than in YSRT, and the median of heart rate in ESRT was lower than in YSRT. The medians of the 9 indicators differed between the groups either in only one of the 6 months or in several months, and differed in the preparatory period as a whole. These are TP (no differences in July, October), APHF (no differences in September, October), APVLF (no differences in July, October), APLF (no differences in July, August, September), APLF/АPHF (no differences in June, August, September, November), pNN50% (no differences in October), RMSSD (no differences in October), SDNN (no differences in October) and SI (no differences in October). The medians of HF%, VLF%, and LF% did not differ between the groups in any of the months, as well as in the whole period.
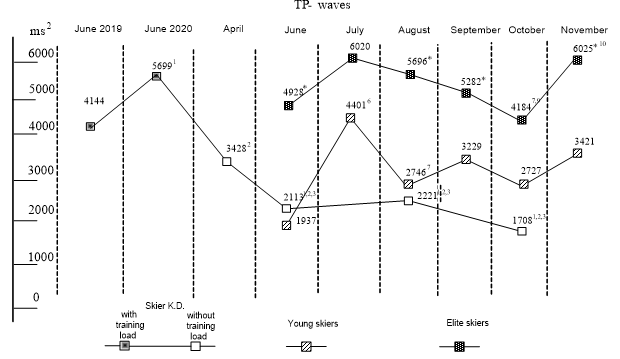
Figure 3: Medians of the absolute power of ortho-TP waves (mc2) for YSRT (outlined squares) and ESRT (dark squares) during the 6 months of the preparatory period, as well as for K.D. under training conditions, i.e. in June 2019 and June 2020 (partially dark squares) and with a 7-month absence of training (light squares).
Note: the * symbol means that the difference between ESRT and YSRT is statistically significant according to the Mann-Whitney criterion, p<0.05; uppercase numbers for EART and YSRT mean that the differences from the first month (June) are statistically significant, p<0.05; uppercase numbers for K.D. mean that the differences between the months (1–June 2019, 2 – June 2020, 3 – April, 4 – June, 5 – August 2024) are statistically significant, p<0.05. It is shown (Table 1; Fig. 3, 4) that of the 15 ortho-HRV indicators, the dynamics of the medians of 10 indicators during the 6 months of the preparatory period for ESRT and YSRT were different. In particular, in ESRT, change the median of 8 indicators ortho-VSR; in particular, the medians of 5 indicators decreased, namely median of АPHF (from 365 ms2 to 175 ms2, that is by 52%, in October); HF% (from 7.5% to 4.1%, that is by 3,4%, in October), HR (from 66.9 b/m to 59.0 b/min, that is by 11.4%, in July), pNN50% (from 14.4% to 5.0%, that is by 9.5%, in October) and RMSSD (from 35 ms to 26 ms, that is by 25.7%, in October), but the medians of 3 indicators increased, including АPLF/АPHF (from 7.0 con. u. up to 13.6 con. u., that is by 6.4 con. u., in October), RRNN (from 901 ms to 1017 ms, that is by 12.9%, in July) and и SI (from 47.3 con. u. to 74.1 con. u.. that is by 26.8 con. u., in November). The remaining 7 indicators (TP, АPVLF, VLF%, АPLF, LF%, SDNN and MxDMn) did not change, as did not change the structure of the TP-components. During the preparatory period in YSRT (Table 1; Fig. 3, 4, 5), the medians of 7 ortho-HRV indicators changed. In particular, lower the median of the 2 indicators, namely HR (from 86.6 b/min to 59.0 b/min, that is by 32,0%, in July) and SI (from 141 con. u. to 66,8 con. u., that is by 74,2 con. u., in November) and the medians of 5 indicators increased, including the medin of TP (from 1937 ms2 to 4401 ms2, that is by 127%, in July), АPLF (from 797 ms2 to 2716 ms2, that is by 241%, in July), ratio АPLF/АPHF (from 7.0 con. u. up to 11.1 con. u., that is by 4.1 con. u., in September), SDNN (from 44 ms to 66 ms, that is by 50%, in July) and MxDMn (from 230 ms to 331 ms, that is by 43.9%, in July). The medians of the remaining 8 indicators did not change during the preparatory period – these are the medians of APHF, HF%, APVLF, VLF%, LF%, RRNN, pNN50% and RMSSD. Also, the structure of the TP-components has not changed in YSRT.
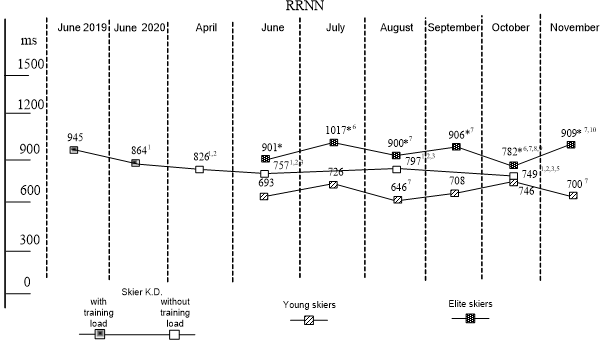
Figure 4: Medians of ortho-RRNN (ms) in YSRT (outlined squares) and ESRT (dark squares) during the 6 months of the preparatory period, as well as in K.D. under training conditions, i.e. in June 2019 and June 2020 (partially dark squares) and at 7-and monthly absence of training (light squares).
Note: the * symbol means that the difference between ESRT and YSRT is statistically significant according to the Mann-Whitney criterion, p<0.05; uppercase numbers for EART and YSRT mean that the differences from the first month (June) are statistically significant, p<0.05; uppercase numbers for K.D. mean that the differences between the months (1–June 2019, 2 – June 2020, 3 –April, 4 – June, 5 – August 2024) are statistically significant, p<0.05. So, during the preparatory period, the medians of the 3 ortho-HRV indicators in ESRT and in YSRT did not change – these are APVLF, VLF% and LF%. In both groups, the median of АPLF/АPHF increases, and the median of HR decreases. Consequently, the pattern of changes in the medians of the 5 ortho-HRV indices in both groups was the same. The dynamics of the medians of the remaining 10 indicators of ortho-HRV were different in the ESRT and YSRT groups. At the same time, there are 4 variants of this dynamic. Option 1: the medians of TP, APLF, SDNN, and MxDMn do not change for ESRT, while for YSRT they increase. Option 2: the medians of АPНF, НF% and RMSSD decrease for ESRT, while they do not change for YSRT. Option 3: medians of pNN50% and RRNN increase in ESRT, but they do not change in YSRT. Option 4: the median of SI increases in ESRT, and decreases in YSRT. Thus, in ESRT (Table 1) during the preparatory period, the medians of 7 ortho-HRV indicators do not change (TP, APLF, APVLF, VLF%, LF%, SDNN and MxDMn); the medians of 4 indicators increase (APLF/APNF, RRNN, pNN50% and SI) and the medians of 4 indicators are decreasing (APHF, HF%, HR, RMSSD). At the same time, in YSRT (Table 1) the medians of 8 indicators (APHF, HF%, APVLF, VLF%, LF%, RRNN, pNN50%, RMSSD) do not change, the medians of 5 indicators of ortho-HRV (TP, APLF/APHF, APLF, SDNN and MxDMn) are increasing, and the medians of 2 indicators of ortho-HRV (HR and SI) are decreasing. All this suggests that the change in ortho-HRV indicators during the preparatory period in ESRT and YSRT occurs in different ways. In particular, in ESRT retains high activity of PD ANS during the preparatory period, including, probably, a high level of synthesis of NN-Ach and in YSRT activity of PD ANS increases, periodically reaching the level of elite skiers, which is probably also due to an increase in synthesis of NN-Ach. It is possible that during the preparatory period, in ESRT develops fatigue (as a result of high loads), judging by the increase in the median of SI, while in YSRT shows no signs of fatigue, judging by the decrease in the median of SI.
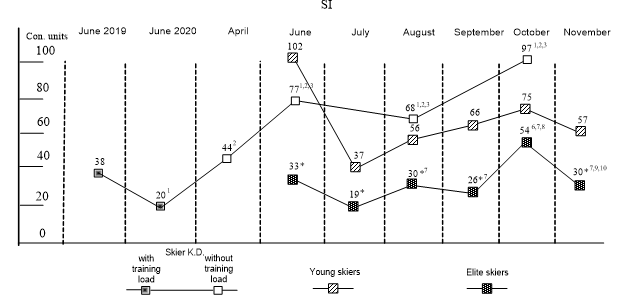
Figure 5: Median of the delta- SI (conl. units), i.e. the difference between the medians of the corresponding clino-SI and ortho-SI indices for YSRT (outlined squares) and ESRT (dark squares) during the 6 months of the preparatory period, as well as for K.D. in training conditions, i.e. in June 2019 in June 2020 (partially dark squares) and with a 7-month absence of training (light squares).
Note: the * symbol means that the difference between ESRT and YSRT is statistically significant according to the Mann-Whitney criterion, p<0.05; uppercase numbers for ESRT and YSRT mean that the differences from the first month (June) are statistically significant, p<0.05; uppercase numbers for K.D. mean that the differences between the months (1–June 2019, 2 – June 2020, 3 – April, 4 – June, 5 – August 2024) are statistically significant, p<0.05. When discussing this section of the work, 2 questions arise – 1) what is the reason for the dynamics of ortho-HRV indicators during the preparatory period for ESRT and YSRT, and 2) what is the reason for the differences between these two groups of skiers in relation to the dynamics of the medians of ortho-HRV indicators? Probably, one of the reasons for the change in the median HRV indicators during the 6 months of the preparatory period is the monthly change in the volume of training loads (in accordance with the goals of the training process), which is typical for both groups (this is noted in the "Methodology" section). And the reason that the nature of the change in the medians of HRV indicators in ESRT and in YSRT was different is the differences in the "mileage" of training, since the workload of ESRT was much greater than that of YSRT. Indeed, as already noted in the "Methodology" section, according to skier K.D., a member of the ESRT team, the total duration of the load (TDL1-5) from June to November 2019 was equal, respectively (h/month) 66.5; 70.0; 72.0; 57.5; 50.0 and 59.5, and "monthly mileage", that is, km/month – respectively 989; 1180; 857; 876; 578 and 798. The leader of the YSRT team had a total duration of training loads (TDL1-5), respectively (h/month) 82.0; 62.0; 55.0; 61.0; 56.0 and 55.0, and the "monthly mileage" – respectively 771; 672; 450; 636; 369; 597 km/month. Thus, although the total duration of training for the YSRT was about the same as for the ESRT, the mileage was lower, and therefore the average movement speed was lower, since their physical fitness did not allow them to develop the same performance as the ESRT. According to our data [13], the medians of HRV indicators reflecting activity of PD ANS including those reflecting synthesis of NN-Ach, are higher the higher the load volume. An analysis of the dynamics of ortho-HRV indices occurring during the 6 months of the preparatory period shows that an increase in the synthesis of NN-Ach, which increases under the influence of training, prevents an increase in the activity of the SD ANS in orthostasis, judging by the fact that this increase was less in ESRT than in YSRT (Table 1). Indeed, for ESRT the median of ortho APLF increases from 2624 ms2 (June) to 3189 ms2 in August, i.e. by 21.5%, and for YSRT it increases from 797 ms2 (in June) to 2716 ms2 (July), i.e. by 241%. The median of ortho-LF% for ESRT increases from 55.8% (June) to 56.5% (in November), i.e. by 1.0%, and for YSRT it increases from 44.5% (June) to 59.4% (November), i.e. by 33.4%. The median of ortho-RMSSD for ESRT in June was 35 ms, it increased to 44 ms (July), i.e. by 25.7%, and for YSRT, respectively, it was 22 ms and 31 ms (July), i.e. the increase was 40.9%. The median of ortho-SDNN for ESRT in June was 70 ms, it increased to 78 ms (July), i.e. by 11.4%, and for YSRT it increased from 44 ms (June) to 66 ms (July), i.e. by 50%. Median of ortho-MxDMn for ESRT in June was 343 ms, it increased to 410 ms (July), i.e. by 19.5%, and for YSRT these values were respectively 230 ms, 331 ms and 43.9%. In general, the revealed differences between ESRT and YSRT in terms of the dynamics of ortho-HRV indices occurring during in the 6-month preparatory period can be regarded as another indirect evidence of the presence of NN-Ach synthesis in the heart of a person exercising endurance. In conclusion of this section, we note that according to our data on clino-HRV indicators (Table 3), in the preparatory period for ESRT the medians of 6 out of 15 indicators do not change (TP, LF%, pNN50%, SDNN, MxDMn, SI), and the medians of 9 indicators change (these are APHF, HF%, APVLF, VLF%, APLF, APLF/APHF, RRNN, HR and RMSSD), of which only the medians HF% and RRNN are increasing, while others are decreasing. Unlike ESRT, in YSRT, the medians of 12 clino-HRV indices do not change, and only 3 change (LF%, HF% and APLF/APHF), of which the median HF?creases, and the medians LF% and APLF/APHF – increasing. Thus, the nature of changes in clino-HRV parameters during the preparatory period depends on the skier's level of training. The data on clino-HRV also demonstrate the ability of NN-Ach to prevent an increase in the activity of SD ANS caused by training, since changes in the median of clino-АPLF, clino- LF% and clino-APLF/APHF, reflecting the activity of SD ANS during the preparatory period were less pronounced in ESRT than in YSRT (Table 3). Indeed, for ESRT the median of clino-APLF increased from 2300 ms2 (June) to 2912 ms2 in August, i.e. by 26.7%, and for YSRT, it increased from 1740 ms2 (in June) to 3037 ms2 (November), i.e. by 74.5%. The median of clino-LF% for ESRT increased from 21.0% (June) to 21.8% in November, i.e. by 0.8%, and for YSRT it increased from 26.3% (June) to 37.7% (November), i.e. by 11.4%. The median of clino-APLF/APHF in ESRT increased from 0.48 con. u. (June) to 0.56 con. u. (November), i.e. by 0.08 con. u., and for YSRT it increased from 0.76 con. u. (June) to 1.30 con. u. (November), i.e. by 0.54 con. u. It should also be noted that, judging by the literature data, no previous analysis of changes in ortho-HRV and clino-HRV parameters in ski racers was carried out during all the months of the preparatory period.
4. The dynamics of ortho-HRV indicators of an elite skier for 7 months from the moment of the forced cessation of training loads What happens to the medians of ortho-HRV indices after an acute cessation of training loads in an elite skier K.D. for 7 months? They are gradually changing, and in October, the medians of 12 indicators out of 15 indicators of ortho-HRV were statistically significantly lower than the initial values (Table 4; Fig. 3, 4, 5). In particulars, the median of TP has decreased from 4144 to 1708 ms2, i.e. by 58.8%; the median of АPHF has decreased from 283 to 43 mc2, i.e. by 84%; the median of HF% has decreased from 6.3% to 1.9%, i.e. by 4%; the median of АPVLF has decreased from 1646 to 776 mc2, i.e. by 52%; the median of VLF% has decreased from 43.5 to 41.0%, i.e. by 2,5%; the median of АPLF has decreased from 2267 to 886 ms2, i.e. by 61%; the median of RRNN has decreased from 945 to 749 ms, i.e. by 20,7%; the median of pNN50% has decreased from 11,7 до 1,3%, i.e. by 26,3%; the median of RMSSD has decreased from 34 до 15 ms, i.e. by 55,9%; the median of SDNN has decreased from 65 to 42 ms, i.e. by 35.3%; and the median of MxDMn has decreased from 325 to 232 мs, i.e. by. 28.6%. However, the medians of 4 indicators increased, including LF% (from 49.1% to 56.4%, i.e. by 7.3%), АPLF/АPHF (from 9.0 to 26.7 con. u., i.e. on 17.5 con. u.), HR (from 63.5 to 80.1 beats/min, i.e. by 26%) and SI (from 51.1 to 142.0 con. u., i.e. by 90 con. u. (Fig. 5). All this can be explained by a decrease in activity of SD ANS and of PD ANS, including, probably, a decrease in the synthesis of NN-Ach. In order to answer the question of whether the synthesis of NN–ACh in K.D. was preserved in October 2024, i.e. in the absence of training for 7 months, an analysis of the delta, i.e. the difference between the medians of the corresponding indicators of clino-HRV and ortho-HRV in K.D. (October 2024), was carried out. It was found (Tables 2, 3, and 4) that there is no significant difference in direction and delta value between ESRT, YSRT, and K.D. in relation to the medians of 11 HRV indicators (these are TP, APHF, HF%, APVLF, RRNN, HR, pNN50%, RMSSD, SDNN, and MxDMn). For example, in October 2024 in K.D. the median of ortho-TP (Fig. 3) was 47% lower than the median clino-TP, while in the ESRT was 56% lower and in the YSRT was 55% lower, i.e. the delta was minus 47%, minus 56% and minus 55%. However, differences were found between ESRT, YSRT and K.D. in such 4 indicators as delta-VLF%, delta-АPLF, delta- АPLF/АPНF, and delta-SI (Tables 2, 3, and 4). Thus, it is shown that in October 2024, the median of ortho-VLF% was lower than the median of clino-VLF% by 9.2% (i.e. the delta was minus 9.2%), while in ESRT and in YSRT, the median of ortho-VLF% was higher than the median clino-VLF% by 4% ( i.e. the delta was plus 4%). With respect to delta-APLF, it was shown that in October 2024, the median of ortho-APLF was 50% higher than the median of clino-APLF, i.e. the delta was plus 50%, while in ESRT the delta was plus 23%, and in YSRT it was minus 28%.For delta-APLF/АPНF in K.D. shows that in October 2024 it was plus 25.8 con. u., while in ESRT and YSRT it was only plus 6.3 con. u. The delta - SI for K.D. in October 2024 was plus 97.3 con. u., while for ESRT it was plus 28 ,0 con. u.s, and for YSRT it was plus 57 con. u.s, (Fig. 5). All these differences can be explained by the fact that K.D. in October 2024, produced NN-ACh if there was one, but it was minimal and did not inhibit the activation of the SD ANS, which, as shown earlier [12], is characteristic of the implementation of active orthostasis (Prevel reflex) in elite skiers In addition, to answer the question of whether the synthesis of NN–ACh in was preserved at K.D. in October 2024, i.e. after 7 months of absence of the usual training for an elite skier, an analysis was carried out in two directions: 1) comparison of the medians of the ortho-HRV parameters of the athlete K.D. (October 2024) with the corresponding medians of ESRT and YSRT; 2) comparison with the literature data concerning the values of the corresponding ortho-HRV parameters of non-athletes, novice skiers and elite representatives of other sports. The first direction showed that only the median of one indicator out of 15, namely, the median of ortho-RRNN in K.D. (October, 2024) is between the medians of ortho-RRNN for ESRT and YSRT. Indeed, the median of ortho-RRNN in ESRT was 782 ms, in YSRT - 746 ms, and in K.D. - 749 ms (Table. 1 and 4, fig. 4). But the remaining 14 indicators of ortho-HRV (Table. 1 and 4) in K.D. was either lower than that in ESRT and in YSRT (these are 10 indicators – TP, APHF, HF%, APVLF, VLF%, APLF, pNN50%, RMSSD, SDNN and MxDMn), or higher (three indicators – LF%, APLF/APHF, SI), or the same ( HR). This means that it was not possible to detect the presence of NN-ACh synthesis in K.D. 7 months after stopping training with this variant of ortho-HRV analysis, with the exception of such an indicator as ortho-RRNN.
| Indicators HRV | |||||||||||||||
Conditions regist. | TP, ms2 | АМHF, ms2 | HF, % | АМVLF, ms2 | VLF, % | АМLF, ms2 | LF, % | АМLF/АМHF, rel. u. | RRNN, ms | HR, bpm. | pNN50, % | RMSSD, ms | SDNN, ms | MxDMn, ms | SI, con. u. |
| June 2019 (1-st point) | |||||||||||||||
| Load volume | TDL1-5 – 211,5 (166/269); DL1-3 – 201,5 (116/260); DL4-5 – 6,5 (1,2/10) | ||||||||||||||
| Clino | 9764 6958/ 10789 | 3959 3161/ 4962 | 41,0 33/ 46 | 3333 2367/ 3968 | 35,4 30/ 43 | 2188 1443/ 3132 | 21,1 19/ 24 | 0,61 0,44/ 0,83 | 1452 1374/ 1484 | 41,3 40/ 43 | 70,3 69/ 75 | 119 108/ 132 | 101,5 90/ 111 | 605 557/ 655 | 11,2 10/ 14 |
| Ortho | 4144 3578/ 4903 | 283 173/ 367 | 6,3 3/ 9 | 1646 1276/ 2260 | 43,5 33/ 48 | 2267 1564/ 2724 | 49,1 42/ 60 | 9,05 4,43/ 18,36 | 945 898/ 1009 | 63,5 59/ 66 | 11,7 5/ 15 | 34 28/ 35 | 65 60/ 70 | 325 302/ 347 | 51,4 44/ 63 |
| Delta | -55 -63/ -46 | -91 -95/ -87 | -33 -38/ -22 | -58 -64/ -7 | +2,7 0/ 12 | -25 -28/ 16 | +23 18/ 33 | +8,18 3,9/ 17,4 | -34 -37/ -31 | +51 45/ 59 | -83 -92/ -78 | -69 -75/ -67 | -33 -43/ -29 | -44 -51/ -36 | +38 33/ 52 |
| June 2020 (2-st point) | |||||||||||||||
| Load volume | TDL1-5 – 101 (85/118); DL1-3 – 101 (85/117); DL4-5 – 0 (0/2) | ||||||||||||||
| Clino | 7559 6568/ 8617 | 3702 3130/ 3970 | 49,31 42/ 53 | 17691 1271/ 2222 | 24,11 20/ 27 | 1930 1466/ 2181 | 25,0 21/ 28 | 0,51 0,41/ 0,58 | 1483 1454/ 1528 | 40,5 39/ 41 | 68,5 65/ 72 | 1001 91/ 108 | 761 68/ 87 | 3671 342/ 451 | 22,11 17/ 25 |
| Ortho | 56991 4550/ 6708 | 264 196/ 349 | 4,7 3/ 5 | 1550 1293/ 2689 | 27,8 23/ 41 | 33401 2609/ 4345 | 68,2 51/ 72 | 13,66 10,81/ 15,72 | 8641 846/ 919 | 69,51 65/ 70 | 7,9 5/ 10 | 32 29/ 35 | 731 68/ 81 | 4111 368/ 439 | 40,41 32/ 47 |
| Delta | -221 -33/ 2 | -93 -94/ -89 | -451 -48/ -37 | +111 -31/ 70 | +7,0 -2/ 18 | +761 44/ 144 | +44 20/ 48 | +13,15 10,24/ 15,2 | -401 -43/ -38 | +681 62/ 76 | -88 -91/ -84 | -66 -71/ -64 | -31 -12/ 7 | +31 -9 16 | +201 14/ 25 |
| Load volume | 1 month without load, April 2024 (3rd point) | ||||||||||||||
| Clino | 59841,2 5271/ 7187 | 26531,2 2334/ 2912 | 40,92 36/ 48 | 18361 1157/ 2543 | 29,4 24/ 36 | 1594 1205/ 1872 | 25,9 20/ 30 | 0,63 0,45/ 0,80 | 13221,2 1247/ 1357 | 45,41,2 44/ 48 | 66,41 64/ 70 | 1001 91/ 102 | 801 75/ 87 | 4641,2 379/ 522 | 21,31 17/ 28 |
| Ortho | 34282 2936/ 4289 | 1281,2 74/ 153 | 3,31,2 2/ 3 | 1396 799/ 1990 | 41,1 27/ 42 | 20662 1771/ 2540 | 56,4 54/ 69 | 18,941,2 15,79/ 22,76 | 8261,2 779/ 864 | 72,61,2 69/ 77 | 2,81,2 2/ 4 | 231,2 20/ 24 | 602 54/ 65 | 3222 273/ 355 | 64,01,2 53/ 76 |
| Delta | -462 -53/ -30 | -951,2 -97/ -93 | -38,5 -44/ -33 | -422 -53/ -9 | +3,2 -4/ 12 | +321,2 5/ 53 | +35,7 27/ 38 | 17,811,2 15,22/ 22,2 | -371,2 -39/ -34 | +591,2 53/ 66 | -961,2 -96/ -92 | -761,2 -79/ -74 | -312 -34/ -19 | -311,2 -36/ -16 | +442 33/ 48 |
| Load volume | 3 months without load, June 2024 (4th point) | ||||||||||||||
| Clino | 59921 5164/ 8019 | 26801,2 2105/ 2827 | 39,32 34/ 46 | 28142,3 2160/ 3323 | 39,52,3 34/ 50 | 11101,2,3 907/ 1311 | 16,92,3 13/ 22 | 0,423 0,33/ 0,57 | 12721,2 1219/ 1324 | 47,11,2 45/ 49 | 68,1 60/ 70 | 911,2 79/ 96 | 77,51 72/ 87 | 4071 373/ 456 | 25,41 20/ 27 |
| Ortho | 21131,2,3 1647/ 2644 | 681,2,3 55/ 98 | 3,31,2 3/ 3 | 7471,2,3 642/ 930 | 35,8 32/ 44 | 12081,2,3 997/ 1593 | 58,8 52/ 64 | 17,491,2 16,32/ 20,99 | 7571,2,3 725/ 780 | 79,21,2,3 77/ 82 | 1,21,2,3 0/ 2 | 161,2,3 15/ 19 | 461,2,3 40/ 50 | 2441,2,3 220/ 273 | 111,81,2,3 91/ 157 |
| Delta | -681,2,3 -72/ -68 | -971,2,3 -98/ -95 | -35,92 -43/ -31 | -711,2,3 -81/ -60 | -2,02 -9/ 5 | +0,52 -14/ 58 | +411,3 33/ 50 | +17,01,2 15,69/ 20,4 | -401,3 -42/ -38 | +681,3 63/ 73 | -971,2,3 -98/ -96 | -811,2,3 -84/ -77 | -432,3 -47/ -32 | -362,3 -53/ -28 | +771,2,3 63/ 125 |
| Load volume | 5 months without load, August 2024 (5th point) | ||||||||||||||
| Clino | 35921,2,3,4 3100/ 4742 | 13801,2,3,4 1108/ 1885 | 39,62 31/ 45 | 14001,4 964/ 1753 | 39,72,3 30/ 50 | 6941,2,3,4 600/ 912 | 19,82,3 17/ 22 | 0,51 0,40/0,74 | 12581,2,3 1229/ 1285 | 47,71,2,3 46/ 48 | 50,71,2,3,4 46/ 59 | 641,2,3,4 58/ 75 | 591,2,3,4 56/ 69 | 3041,2,3,4 279/ 332 | 43,31,2,3,4 36/ 50 |
| Ortho | 22211,2,3 1598/ 3019 | 481,2,3,4 42/ 62 | 2,11,2,4 1/ 2 | 9591,2 517/ 1444 | 43,12 32/ 49 | 12091,2,3 950/ 1410 | 54,82 47/ 65 | 22,411,2,4 17,66/ 28,31 | 7971,2,3 762/ 808 | 75,31,2,3 74/ 78 | 1,41,2,3 0/ 2 | 161,2,3 14/ 18 | 461,2,3 40/ 57 | 2361,2,3 205/ 297 | 107,51,2,3 82/ 161 |
| Delta | -392,4 -53/ -20 | -961,2,4 -97/ -94 | -36,92 -43/ -28 | -392,4 -63/ 9 | +2,2 -14/ 17 | +651,4 26/ 117 | +35,24 26/ 44 | +21,791,2,4 17,0/ 27,8 | -371,2,4 -38/ -36 | +601,2,4 57/ 63 | -971,2,3 -98/ -95 | -762,4 -78/ -70 | -241,2,4 -30/ -6 | -181,2,4 -34/ -2 | +68,81,2,3 45/ 99 |
| Load volume | 7 months without load, October 2024 (6th point) | ||||||||||||||
| Clino | 36821,2,3,4 2957/ 3727 | 11411,2,3,4,5 874/ 1267 | 312-5 21/ 39 | 15871,4 1040/ 2310 | 40,82,3 38/ 63 | 7521,2,3,4 564/ 883 | 21,13 15/ 25 | 0,632,4,5 0,56/ 0,83 | 11971,2,3,4,5 1148/ 1241 | 50,11,2,3,4,5 48/ 52 | 45,41,2,3,4,5 36/ 47 | 581,2,3,4 52/ 63 | 581,2,3,4 53/ 62 | 3051,2,3,4 279/ 322 | 49,01,2,3,4 42/52 |
| Ortho | 17081,2,3 1298/ 2560 | 431,2,3,4 27/ 55 | 1,91,2,3,4 1/ 2 | 7761,2,3 462/ 1164 | 41 30/ 47 | 8861,2,3 751/ 1383 | 56,4 50/ 66 | 26,71,2,3,4 21,14 30,71 | 7491,2,3,5 734/ 769 | 80,11,2,3,5 77/ 81 | 1,31,2,3 0/ 1 | 151,2,3 13/ 17 | 421,2,3 36/ 49 | 2321,2,3 202/ 298 | 142,11,2,3 93/ 168 |
| Delta | -472,4 -65/ -32 | -96%1,2 -97/ -94 | -28,72,3,5 -35/ -19 | -53%2 -67/ -41 | -9,22 -16/ 11 | +50%1 -14/ 85 | 36,9 31/ 45 | 25,81,2,3,4 20,51/ 30,0 | -37%1,2,4 -39/ -35 | +60%1,2,4 54/ 64 | -97%1,2,3 -99/ -96 | -73%2,4 -76/ -69 | -28%2,3,4 -39/ -19 | -231,2,4 -33/ -12 | +97,31,2,3 63/ 119 |
Table 4: Median, 25 and 75 cents of the spectral and temporal indicators of clino-HRV, ortho-HRV and delta, i.e. the difference between clino- and ortho-HRV in an elite skier with training loads (June 2019, June 2020) and in the absence of loads (April, June, August, October 2024).
Note: the interpretation of HRV indicators is given in the "Methodology" section. The numbers in uppercase indicate the month with which the indicator in this month differs statistically significantly (according to the Mann-Whitney criterion, i.e. p<0.05) from the indicators of other months; TDL1-5 – total duration of exercise (working pulse zones 1-5); DL1-3 – duration of aerobic exercise (working pulse zones 1-3); DL4-5 – duration of anaerobic exercise (zones 4 and 5), min/day.
A comparison of the medians of ortho-HRV in K.D. (October 2024) with literature data concerning the medians of ortho-HRV in elite skiers, unskilled skiers, athletes of other sports, and non-athletes [14-20], showed that of the 15 ortho-HRV indicators, the presence of NN-Ach synthesis in K.D. in October 2024 indirectly reflects there are only three indicators, namely ortho-APLF, ortho-RRNN, ortho-HR. Thus, with respect to the median of ortho-APLF, which is known to reflect the activity of SD ANS, it is shown (Table 1, 4), that in October 2024, athlete K.D. had 886 ms2, ESRT had 2496 ms2, and YSRT had 1592 ms2. According to [14], ortho-APLF values for hockey players were 2058 ms2, for swimmers – 1654 ms2, and for weightlifters – 1735 ms2. According to [15], ortho-APLF values for novice sympathicotonic skiers were 890 ms2, for 14 normotonic skiers – 1302 ms2, and for 12 vagotonic skiers – 1950 ms2. According to [17], ortho-APLF values for male contract soldiers were 1204 ms2, for non-athletes – 1234 ms2, for track and field athletes – 1859 ms2, for parachutists – 1446 ms2, for professional football players – 1404 ms2, and for 16-year-old hockey players – 2165 ms2. According to [19], swimmers (MS, 17-23 years old) had ortho-APLF values of 3771 ms2. So, for K.D. the median of ortho-APLF is much lower than for ESRT and YSRT, and lower than for representatives of other sports, and even lower than for non-athletes. Indirectly, this means that after a 7-month absence of training, K.D. retain NN-Ach synthesis (although at a lower level than active elite skiers), which slows down the activation of SD ANS, i.e. the median of ortho-APLF decreases. Relative to the median of ortho-RRNN is shown (Table 1, 4; Fig. 4) that For K.D., in October 2024 it was 749 ms, for ESRT – 906 ms, for YSRT – 705 ms. According to [17], ortho-RRN values for male contractors are 692 ms, for track and field athletes – 768 ms, for parachutists – 702 ms, for professional football players – 844 ms, and for hockey players – 755 ms. According to [18], the ortho-RRNN value increased from 765 ms to 856 ms for 35 amateur half-marathon runners over the course of 10 years. According to [20], ortho-RRNN values in 32-year-old triathletes were 915 ms, and in 30-year-old crossfit athletes – 824 ms. According to [16], for elite ski racers from Russia, Norway, and Switzerland, the ortho- RRNN value was relatively constant throughout the season and ranged from 817 ms to 848 ms. So, in October 2024 K.D.'s median ortho-RRNN was lower than that of elite skiers and elite marathon runners, but higher than that of young skiers and non-athletes. This indicates that K.D. (October 2024) has a synthesis of NN-Ach, the level of which, however, is lower than that of elite skiers. Relative to the median of ortho-HR is shown (Table 1, 4), that in K.D. (October) ortho-HR was 80.1 beats per minute, in ESRT – 66.2 beats per minute, and in YSRT – 85.1 beats per minute. According to [17], ortho-HR values were 86.7 beats/min for male contract soldiers, 78.1 beats/min for track and field athletes, 85.5 beats/min for parachutists, 71.0 beats/min for professional football players, 79.5 beats/min for 16-year-old hockey players. So, in October 2024, K.D. had a median of ortho-HR higher than that of ESRT, but lower than that of YSRT and lower than that of non-athletes. These data probably reflect the presence of NN-Ach synthesis in K.D. in October 2024, the level of which, however, is lower than that of ESRT. The remaining 12 ortho-HRV indicators indicate the absence of NN-Ach synthesis in the athlete K.D. in October 2024. As an example, we will give data on the median of TP. For the athlete K.D. in October 2024 it was 1708 ms2, while for the ESRT it was 5317 ms2, and for the YSRT it was 3241 ms2 (Table 1, 4). According to [14], hockey players, swimmers, and weightlifters had ortho-TP values – 4189 ms2, 2899 ms2, and 3466 ms2, respectively. According to [15], the ortho-TP value for novice sympathotonic skiers was 2332 ms2, for 14 normotonics – 4397 ms2, and for 12 vagotonics – 4973 ms2. According to [17], the ortho-TP value for male contractors was 2463 ms2, for Neurosoft employees (non-athletes) – 1966 ms2, for athletes of the I and II categories – 4144 ms2, for parachutists – 3730 ms2, for professional football players – 3510 ms2, for hockey players – 4746 ms2. So, K.D. has a median of ortho-TP much lower than that of ESRT and YSRT, and lower than that of representatives of other sports, and almost the same as that of non-athletes. This means that after a 7-month absence of training, according to the medians of 12 ortho-HRV indices, the synthesis of NN-Ach probably stopped completely. However, another type of analysis confirms the idea that in October 2024, in K.D. the synthesis of NN-Ach was preserved, although at a lower level than that of in the presence of training. It is based on the nature of changes in the medians of five HRV indicators (TP, APLF, pNN50%, SDNN and MxDMn) during the transition from clinostasis to active orthostasis, named as the "five criteria for the presence of NN-Ach synthesis" [12] and which was already mentioned above. Here we will allow you to recall these criteria once again. According to the first criterion, in the presence of NN-Ach synthesis in the myocardium, the median of TP is characterized by high median values in conditions of clinostasis and low values in conditions of active orthostasis, i.e. a significant decrease during the active transition to orthostasis, and in the absence of NN-Ach synthesis, median of TP is characterized by low values in clinostasis and their increase in orthostasis. According to this criterion, it can be argued that in K.D. (October 2024), the synthesis of NN-Ach occurs, although at a lower level than in ESRT and YSRT. Indeed, in K.D. (October 2024) the median of the clino-TP was 3682 ms2, and the median of ortho-TP was 1708 ms2, i.e., it decreased with an active transition to orthostasis (Table 4; Fig. 3). According to the second criterion, the median of APVLF decreases during the transition from clinostasis to active orthostasis in the presence of NN-Ach synthesis, and increases in the absence of NN-Ach synthesis. According to this criterion, K.D. (October 2024) had a synthesis of NN-Ach, since the median of clino-APVLF was 1587 ms2, and the median of ortho-APVLF was 776 ms2, i.e. it decreased during the transition to orthostasis (Table 4). According to the third criterion, a marker of the presence of NN-Ach synthesis in the heart are high (above 60%) values of the median of pNN50% in conditions of clinostasis and their marked decrease with active orthostasis, and in the absence of NN-Ach synthesis, extremely low values of the median pNN50% in clinostasis (no higher than 20%) and low values (1-2%) in conditions of orthostasis. According to this criterion, K.D. had a synthesis of NN-Ach in October 2024, but significantly lower. Indeed, in K.D., the median of clino-pNN50% was 45.4%, and the median of ortho-pNN50% was 1.3% (Table 4). According to the fourth criterion, a marker of the presence of NN-Ach synthesis in the heart is a decrease in the median SDNN by 20% or higher during the transition from clinostasis to active orthostasis. According to this criterion, the synthesis of NN-Ach was present in K.D. (October 2024), since the median of clino-SDNN was 58 ms, and the median of ortho-SDNN was 42 ms, i.e. the decrease was minus 28% (Table 4). According to the fifth criterion, a marker of the presence of NN-Ach synthesis in the heart is a decrease in the value of MxDMn during the transition from clinostasis to active orthostasis by 10% or higher. According to this criterion, the synthesis of NN-Ach was present in K.D. (October 2024), since the median of clino-MxDMn was 305 ms, and the median of ortho-MxDMn was 232 ms, i.e. the decrease was minus 23% (Table 4). Thus, all five criteria proposed by us earlier [12] indirectly confirm the presence of NN-Ach synthesis in the athlete K.D. (October 2024), although it is obvious that its intensity is much lower than that in K.D. in the presence of training. Earlier, when analyzing the dynamics of 15 clino-HRV indicators in a athlete K.D. during the period of cessation of exercise, we showed [21] that after 7 months, i.e. in October 2024, K.D. retains the synthesis of NN-Ach, although significantly reduced. In particular, when comparing with the values of clino-HRV indices in non-athletic students obtained [22], such indicators of clino-HRV as RRNN, HR, pNN50% and SI indirectly indicate the presence of NN-Ach synthesis in K.D. When comparing with the data on clino-HRV obtained [17] during the examination of contract soldiers, it was shown that the presence of NN-Ach synthesis in K.D. (October 2024) is indicated by such indicators of clino-HRV as TP, APVLF, VLF%, RRNN and pNN50%. When comparing with the data on clino-HRV obtained [17] during the examination of Neurosoft employees, it follows that such indicators of clino-HRV as TP, APHF, APLF, APVLF, RRNN, pNN50%, RMSSD, SDNN, as well as the APLF/APHF ratio. Together with the above data, this indirectly means that the indicators of clino-HRV better reflect the presence of NN-Ach synthesis than the indicators of ortho-HRV. But in general, our data indicate that, if the synthesis of NN-Aсh persists in K.D. after 7 months of absence of training loads, then the intensity of this synthesis is lower than in in K.D. in the presence of training. Of course, for other elite ski racers, the regression of vagotonia in the event of a sudden cessation of endurance training may occur at a different rate than for an athlete K.D. But we considered it possible to cite our data concerning athlete K.D., since we have not found such a description of vagotonia regression in HRV indicators in the literature. So, we assume that in the absence of stimuli that cause the synthesis of NN-Ach, for example, the accumulation of reactive oxygen species (ROS), or myocardial damage, the synthesis of NN-Ach gradually stops. At the same time, the data obtained demonstrate that regular physical activity is necessary to maintain athletic vagotonia, i.e., high activity of PD ANS and the presence of NN-Ach synthesis. It follows from our results that the regression of vagotonia does not occur instantly, but gradually, as the duration of the absence of systematic endurance training increases (up to 7 months), but much faster than its formation, which takes many years of continuous high-volume training.
Competing interests
The authors declare no competing interests.
Funding
This research received no external funding.
Author's reference
Denis A. Kataev is a Russian Master of Sports in cross-country skiing, Postgraduate student of the Department of Biology and Methods of Teaching Biology, Vyatka State University; coach-teacher of the Kirov Regional State Autonomous Institution of Additional Education "Sports School of the Olympic Reserve "Perekop". ORCHID 0000-0002-8051-3521. The author's contribution: registration of a cardiointervalogram in the field, analysis of its parameters, writing a text, literature analysis.
Viktor I. Tsirkin, Dr. Sci. (Med.). Professor, Senior Researcher at the Institute of Neuroscience, Kazan State Medical University. ORCHID 0000-0003-3467-3919. Author's contribution: head of scientific work, literature analysis, scientific text editing.
Andrey N. Trukhin Cand. Sci. (Biol.), Doсent, Associate Professor of the Department of Biology and Methods of Teaching Biology, Vyatka State University. ORCID 0000-0001-7259-7078. Author's contribution: scientific editing, article and necessary docu mentation design.
Svetlana I. Trukhina Cand. Sci. (Biol.), Doсent, Associate Professor of the Department of Anatomy, Kirov Medical University. ORCID 0000-0003-3888-1993. Author's contribution: scientific editing of the text, article and neces sary documentation design.
Conclusions
- A comparison of the medians of 15 ortho-HRV indicators in elite skiers of the Republic of Tatarstan (ESRT) and youth skiers of 1-2 adult categories (YSRT) shows that in the preparatory period, the median of 9 indicators reflecting the activity of the parasympathetic division (PD) of the autonomic nervous system (ANS) and, probably, the synthesis of non-neuronal acetylcholine (NN-Ach), were higher in ESRT than in YSRT. Among these indicators are TP, APHF, APVLF, APLF, RRNN, pNN50%, RMSSD, SDNN, MxDMn. The medians of HR and SI were lower in ESRT, and the medians of HF%, VLF%, LF% and APLF/APHF were the same as those of ESRT, as well as the ortho-TP structure (APLF>APVLF>APHF), which indicates the dominance of SD ANS under orthostasis.
- The difference (delta) between the median of the corresponding indicator in conditions of clinostasis and active orthostasis in both groups (ESRT and YSRT) was the same for 10 indicators (TP, APHF, APVLF, VLF%, APLF/APHF, RRNN, HR, RMSSD, SDNN and MxDMn), but for 5 indicators of the delta differences were statistically significant (HF%, APLF, LF%, pNN50% and SI). They indirectly indicate a higher level of NN-Ach synthesis in ESRT, due to which ESRT has a more pronounced inhibition of SD ANS activation during the transition to active orthostasis.
- Five criteria that allow us to talk about the presence of NN-Ach synthesis by the nature of changes in the medians of such indicators as TP, APVLF, pNN50%, SDNN, MxDMn during the transition from clinostasis to active orthostasis indirectly indicate that YSRT like ESRT, probably has NN-Ach synthesis, but Its intensity is lower in YSRT than in ESRT.
- During the preparatory period lasting six months (from June to November), the change in ortho-HRV indicators in ESRT and in YSRT occurs in different ways, which is probably due to different levels of sports vagotonia, including the level of synthesis of NN-Ach. Thus, during the preparatory period, ESRT retains high activity of PD ANS, and probably the synthesis of NN-Ach, while in YSRT activity of PD ANS increases, periodically approaching the level of elite skiers, which is probably due to an increase in the synthesis of NN-Ach. Indeed, during the preparatory period for ESRT the medians of the 7 ortho-HRV indicators (TP, APLF, APVLF, VLF%, LF%, SDNN and MxDMn) did not change, the medians of the 4 indicators (APLF/APHF, RRNN, pN50% and SI) increased and the medians of the 4 indicators (APHF, HF%, HR, RMSSD) decreased. At the same time, the medians of 8 indicators (APHF, HF%, APVLF, VLF%, LF%, RRNN, pNN50%, RMSSD) do not change in YSRT, the medians of 5 indicators of ortho-HRV (TP, APLF/APHF, APLF, SDNN and MxDMn) do not change, and the medians of 2 indicators of ortho-HRV(HR and SI) decrease. This means that for the formation of sports vagotonia, which, in addition to an increase activity of PD ANS, is probably based on an increase in the synthesis of NN-Ach by cardiomyocytes, long-term (13-20 years) continuous high-volume training is required, and 5-7 years of experience in skiing, as in YSRT, is insufficient to achieve a high level of NN-Ach synthesis and high athletic performance.
- For an elite skier K.D. over the course of 7 months from the moment of forced cessation of training loads, the medians of 11indicators ortho-HRV (as well as clino-HRV) decrease to the level typical for non-athletes – these are TP, APHF, HF%, APVLF, VLF%, APLF, RRNN, pNN50%, RMSSD, SDNN and MxDMn, and the medians LF%, AMLF/AMHF, HR, and SI increase. All this reflects a decrease of SD and PD ANS activity, including, probably, a decrease in NN-Ach synthesis. The decrease of level of NN-Ach synthesis is indirectly indicated by changes in the median delta-VLF%, delta-АPLF, delta-APLF/APHF and delta-SI. At the same time, the partial preservation of NN-Ach synthesis in K.D. even after 7 months of relative inactivity, is indirectly evidenced by lower medians od ortho-APLF and ortho-HR, and a higher median of ortho-RRNN than in non-athletes, as well as the nature of changes in the medians of such indicators as TP, APVLF, pNN50%, SDNN and MxDMn that occur during the transition from clinostasis to active orthostasis. All this allows us to conclude that if long-term aerobic training of a large volume is required for the formation of sports vagotonia, then a short period of time (no more than 7 months) is sufficient for its regression in the absence of training loads.
References
- Abramochkin D.V., Borodinova A.A., Rosenshtraukh L.V., Nikolsky E.E. (2012). Both neuronal and non-neuronal acetylcholine take part in non-quantal acetylcholine release in the rat atrium. Life Sci.; 91 (21–22): 1023–1026.
View at Publisher | View at Google Scholar - D’Souza A., Sharma S., Boyett M.R. (2015). Crosstalk opposing view: bradycardia in the trained athlete is attributable to a downregulation of a pacemaker channel in the sinus node. J. Physiol.; 593 (8): 1749–1751.
View at Publisher | View at Google Scholar - Saw E.L., Kakinuma Y., Fronius M., Katare R. (2018). The non-neuronal cholinergic system in the heart: A comprehensive review. J. Mol. Cell. Cardiol.; 125:129–139.
View at Publisher | View at Google Scholar - Kakinuma Y. (2021). Characteristic effects of the cardiac non-neuronal acetylcholine system augmentation on brain functions. Int. J. Mol. Sci.; 22 (2): 545.
View at Publisher | View at Google Scholar - Oikawa S., Kai Y., Mano A., Ohata H., Kurabayashi A., Tsuda M., Kakinuma Y. (2021). Non-neuronal cardiac acetylcholine system playing indispensable roles in cardiac homeostasis confers resiliency to the heart. J. Physiol. Sci.; 71 (1): 2.
View at Publisher | View at Google Scholar - Munasinghe P.E., Saw E.L., Reily-Bell M., Tonkin D., Kakinuma Y., et al. (2023). Non-neuronal cholinergic system delays cardiac remodelling in type 1 diabetes. Heliyon.; 9 (6): e17434.
View at Publisher | View at Google Scholar - Braczko F., Skyschally A., Lieder H., Kather J.N., Kleinbongard P., Heusch G. (2024). Deep learning segmentation model for quantification of infarct size in pigs with myocardial ischemia/reperfusion. Basic. Res. Cardiol.; 119 (6): 923–936.
View at Publisher | View at Google Scholar - Kataev D.A., Tsirkin V.I., Trukhin A.N., Trukhina S.I. (2024). Sports vagotonia as a result of increased synthesis of non-neuronal acetylcholine by cardiomyocytes. Anatomy Physiol. Biochem. Int. J.; 7 (3): 555711.
View at Publisher | View at Google Scholar - Kataev D.A., Tsirkin V.I., Zavalin N.S., Morozova M.A., Trukhin A.N., et al. (2023). Dynamics of TP-, HF-, LF- and VLF-waves of the cardiointervalogram (under clinostasis conditions) of an elite cross-country skier in the preparatory, competitive and transition periods depending on the volume and intensity of training loads. Human Physiology.; 49 (5): 87–100.
View at Publisher | View at Google Scholar - Strakhov M.A., Zagorodniy N.V., Egiazaryan K.A., Gaev T.G. (2019). Stabilized hyaluronates with a combined composition in the treatment of tendinitis and tendinopathies in professional athletes. R.M.J. Medical Review.; 11 (2): 96.
View at Publisher | View at Google Scholar - Stenton G. (1998). Medical and biological statistics / Translated from English. Moscow, Praktika,. 459 p.
View at Publisher | View at Google Scholar - Kataev D.A., Tsirkin V.I., Trukhin A.N., Trukhina S.I. (2025). Cardiointervalogram indicators under conditions of clinostasis and orthostasis in elite cross-country skiers during the annual macrocycle. Human Physiology. 51 (2): 96–119.
View at Publisher | View at Google Scholar - Kataev D.A., Tsirkin V.I. Trukhin A.N., Trukhina S.I. (2025). Dependence of the parameters of clinostatic and orthostatic cardiointervalography on the duration (volume) of aerobic and anaerobic training and competitive loads in elite cross-country skiers. The successes of modern biology.; 145 (1): 20–34.
View at Publisher | View at Google Scholar - Kudrja O.N. (2009). The influence of physical activity of different directions on heart rate variability in athletes. Bulletin of Siberian Medicine.; 8 (1): 36–42.
View at Publisher | View at Google Scholar - Efremova R.I., Spicin A.P., Voronina G.A. (2015). Reactivity of regulatory systems of young skiers depending on the type of vegetative regulation. Vyatka Medical Bulletin.; 4: 15–18.
View at Publisher | View at Google Scholar - Schäfer D., Gjerdalen G.F., Solberg E.E., Khokhlova M., Badtieva V., et al. (2015). Sex differences in heart rate variability: a longitudinal study in international elite cross-country skiers. Eur. J. Appl. Physiol.; 115 (10): 2107–2114.
View at Publisher | View at Google Scholar - Mihajlov V.M. (2017). Heart rate variability (a new look at an old paradigm). Ivanovo: LLC Neurosoft. 516 p.
View at Publisher | View at Google Scholar - De Maria B., de Oliveira Gois M., Catai A.M., Marra C., Lucini D., et al. (2021). Ten-year follow-up of cardiac function and neural regulation in a group of amateur half-marathon runners. Open Heart.; 8 (1): e001561.
View at Publisher | View at Google Scholar - Litvin F.B., Kalabin O.V., Bruk T.M. (2023). Group and individual characteristics of heart rate variability in qualified young swimmers. Modern issues of biomedicine.; 7 (3): 37.
View at Publisher | View at Google Scholar - Morlin M.T., da Cruz C.J.G., Guimarães F.E.R., da Silva R.A.S., Porto L.G.G., et al. (2022). High-intensity interval training combined with different types of exercises on cardiac autonomic function. An analytical cross-sectional study in CrossFit® Athletes. Int. J. Environ. Res. Public. Health.; 20 (1): 634.
View at Publisher | View at Google Scholar - Kataev D.A. Tsirkin VI, Trukhin A.N. Trukhina S.I. (2025). Formation and regression of sports vagotonia (based on heart rate variability data under clinostasis conditions). Anatomy Physiol. Biochem. Int. J.; 7 (5): 555724.
View at Publisher | View at Google Scholar - Dmitrieva S.L., Khlybova S.V., Khodyrev G.N., Tsirkin V.I. (2013). Heart rate variability at different stages of the gestational process. Publishing house of the Department of Health of the Kirov Region. Kirov, 132 p.
View at Publisher | View at Google Scholar
