

Review Article | DOI: https://doi.org/10.31579/2834-5126/029
Foot Problems in Patients with Diabetes
- Rehan Haider 1*
Riggs Pharmaceuticals Karachi, Department of Pharmacy, University of Karachi, Pakistan
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Karachi, Department of Pharmacy, University of Karachi, Pakistan.
Citation: Rehan Haider (2023), Foot Problems in Patients with Diabetes, Clinical Trials and Clinical Research, 2(4); DOI:10.31579/2834-5126/029
Copyright: © 2023, Rehan Haider. this is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 July 2023 | Accepted: 25 July 2023 | Published: 01 August 2023
Keywords: foot problems; hyperglycemia; peripheral neuropathy; sensory neuropathy; autonomic neuropathy; peripheral arterial disease; foot ulcers; regular foot care; infection; charcot arthropathy
Abstract
Foot problems are common and significant complications in patients with diabetes. Chronic hyperglycemia associated with diabetes can lead to various systemic complications, and the feet are particularly vulnerable owing to their complex anatomy and dependence on proper blood circulation and nerve function. This abstract aims to provide an overview of foot problems in patients with diabetes, highlighting their prevalence, etiology, clinical presentation, and management strategies. Peripheral neuropathy, characterized by nerve damage, is a key contributor to foot problems in individuals with diabetes. Sensory neuropathy diminishes the ability to detect pain, temperature, and pressure, making patients susceptible to unnoticed injuries, whereas autonomic neuropathy causes reduced sweating and dryness, leading to skin fissures and ulcers. Peripheral arterial disease, a common comorbidity, restricts blood flow to the lower extremities, impairs wound healing, and increases the risk of infection. Foot problems commonly observed in patients with diabetes include foot ulcers, infections, Charcot arthropathy, and peripheral arterial disease. Foot ulcers, often triggered by minor trauma, can become chronic and difficult to heal, necessitating comprehensive wound care, offloading techniques, and infection control. Infections, primarily caused by bacteria, can progress rapidly, leading to cellulitis, osteomyelitis, or even gangrene, demanding prompt diagnosis and aggressive treatment with antibiotics or surgical interventions. Charcot arthropathy is a condition characterized by bone and joint deformities, resulting from repetitive micro trauma and neuropathy. Early detection and immobilization are crucial to prevent severe deformities and fractures. Peripheral arterial disease contributes to ischemia and tissue damage, necessitating management strategies, such as revascularization procedures or amputation in severe cases. Preventive measures and regular foot care are of paramount importance in the management of foot problems in diabetic patients. Education regarding self-examination, appropriate footwear, and meticulous hygiene practices can significantly reduce the risk of complications. Multidisciplinary teams involving podiatrists, endocrinologists, and wound care specialists play vital roles in comprehensive foot care and management. In conclusion, foot problems pose a substantial burden on patients with diabetes, significantly impacting their quality of life and requiring a multi-dimensional approach t prevention and management. Early detection, patient education, and effective interventions are crucial to reduce the incidence of foot complications and improve outcomes in this vulnerable population.
Introduction
the disease. Mediocre doctors treat the disease before it becomes evident. Inferior doctors treat full-blown diseases. " [Huang Dee, China, 2600 BC] The Chinese proverb suggests that inferior doctors treat full-blown disease, and until recently, this was sadly the case with diabetic foot disease. Realizing the global importance of diabetic foot disease, the International Diabetes Federation (IDF) focused on the diabetic foot throughout the year 2005, during which there was a worldwide campaign to " put feet first" and highlight the all-common problem of amputation among patients with diabetes worldwide. To coincide with World Diabetes Day in 2005, The Lancet launched an issue almost exclusively dedicated to the diabetic foot: this was the first time that any major non - specialist journal had focused on this worldwide problem; however, major challenges remain in getting across Important messages related to diabetic foot
1 Foot ulceration is common, affecting up to 25% of patients with diabetes during their lifetime [1]. 2 Over 85% of lower limb amputations are preceded by foot Ulcers and diabetes remain the most common causes of non-traumatic amputation in Western countries [2]. 3 Prevention is the first step towards solving diabetic foot problems. Although it was estimated that a leg is lost to diabetes, somewhere in the world every 30 seconds, a more important fact Is that up to 85% of all amputations in patients with diabetes should be? preventable [2].4 Reductions in amputations will only be achieved if healthcare professionals from all specialties realize that, as Brand once stated, "Pain is God's greatest gift to mankind ": it is the loss of pain that permits patients with neuropathy to develop ulcers and continue walking despite the presence of an overwhelming infection [3]. 5 Strategies aimed at preventing foot ulcers are cost-effective and can even be cost-saving if increased education and effort are focused on those patients with recognized risk factors for the Development of foot problems [4].
6 Diabetes is now the most common cause of Charcot neuroarthropathy in Western countries, another condition that should be generally preventable [3].
Much progress has been made in our understanding of the pathogenesis and management of diabetic foot over the last quarter-century. This has been matched by an increasing number of publications published in peer-reviewed journals. Taken as a percentage of all PubMed-listed articles on diabetes, those on the diabetic foot increased from 0.7% in the 1980–1988 period to more than 2.7% in the years 1998–2004 [3]. Before 1980, little progress had been made in the previous 100 years, even though the association between gangrene and diabetes was recognized in the mid-19th century [5]. For the first 100 years following these descriptions, diabetic foot problems were considered predominantly vascular and complicated by infection. It was not until the Second World War that McKeown performed the first ray excision in a patient with diabetes and osteomyelitis, but a good blood supply, which was performed under the encouragement of Lawrence, who had diabetes himself and became a co-founder of the British Diabetic Association, now Diabetes UK [6]. Over the last few years, many primary countrywide and worldwide societies have been shaped, including diabetic foot examination businesses, and the I pressure from operating groups international on diabetic foot was mounted in 1991. New editions of the main international textbooks on diabetic foot have been published in recent years [7,8]. and numerous collaborative studies agencies are tackling brilliant problems concerning the pathogenesis and management of diabetic foot diseases.
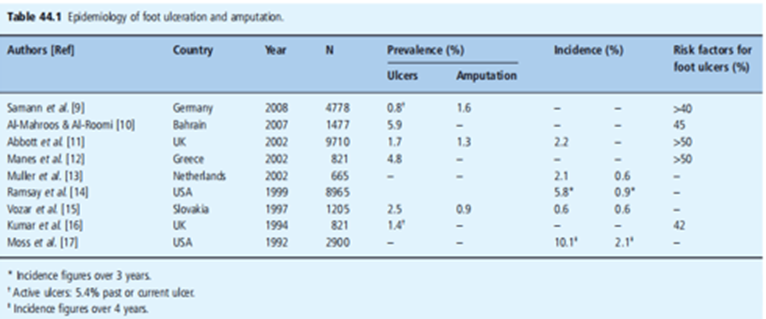
In this study, the global period of " diabetic foot " might be used to talk about a variety of pathological conditions that could affect the feet of people with diabetes. First, the epidemiology and economic impact of diabetic foot ailments are mentioned, observed through the contributory elements that bring about diabetic foot ulceration. The potential for prevention of these late sequelae of neuropathy and vascular sickness is discussed, followed by a phase in the management of foot ulcers. The bankruptcy closes with a brief description of the pathogenesis and management of Charcot neuroarthropathy, a quit-level worry of diabetic neuropathy. during this, pass-referencing may be supplied to other studies that also cowl factors of diabetic foot disease, specifically the ones on diabetic neuropathy, peripheral vascular disease, bone and rheumatic disorders in diabetes. Epidemiology and economic aspects of d diabetic foot disease as foot ulceration and amputation are closely interrelated in diabetes [2]. they are considered together in this section. A selection of epidemiologic data for foot ulceration and amputation, originating from studies from numerous nations [9-17]. is provided in Desk 44.1. Globally, diabetic foot complications remain the primary clinical, social, and monetary problems that might be seen in all types of diabetes, and every U.S.A [18].however, the pronounced frequencies of amputation and ulceration vary considerably, thus of different diagnostic standards used as well as nearby differences [19]. Diabetes remains a first-rate reason for non-disturbing amputation across the world with quotes being as much as 15 instances higher than inside the non-diabetic population. although the research referred to and listed in Table 44.1 were nicely performed, and methodologic troubles remain which make it tough to carry out direct comparisons among studies and/or countries. First, definitions of what constitutes a foot ulcer vary, and second, surveys forever include the most effective patients with previously identified diabetes, while with type 2 diabetes, foot troubles can be the offering function. In one study in the UK, for example, 15% of patients undergoing amputation had been first diagnosed with diabetes on that sanatorium admission [20]. 0.33, suggested foot ulcers aren't constantly shown by way of direct examination using the investigators concerned within the examination. finally, as may be visible from the desk, in those studies that determine the proportion of the population that had dangerous elements for foot ulcerations, 40–70% of patients fell into that category. Such observations indicate the need for all diabetes offerings to have an everyday screening application to identify such high-risk individuals.
Health economics of diabetic foot disease
In addition to causing substantial morbidity and mortality, foot lesions in patients with diabetes have substantial economic consequences. Diabetic foot ulceration and amputations were estimated to cost US healthcare payers $10.9 billion in 2001 [21,22]. Corresponding estimates from the UK based upon similar methodology suggested that the total annual costs of diabetes-related foot complications was £ 252 million [23]. however, similar problems to those noted with epidemiology exist when comparing data on the costs of diabetic foot lesions relating to methodology and whether direct or indirect costs were included. Moreover, few studies have estimated the costs of long-term follow-up of patients with foot ulcers or amputations [2]. The most recent data from the USA suggest that in 2007 $18.9 billion was spent on the care of diabetic foot ulcers, and $11.7 billion on lower extremity amputations [24]. Having estimated the total cost of diabetic foot disease to be $30.6 billion in 2007, the authors went on to estimate the potential savings based upon realistic reductions in ulceration and amputation, to be as high as $21.8 billion. Such strong economic arguments may help drive improvements in preventative foot care, which could potentially lead to significant savings for healthcare systems.
Etiopathogenesis of diabetic foot lesions
" Coming events cast their shadows earlier. " [Thomas Campbell] If we are to be successful in reducing the high incidence of foot ulcers and ultimately amputation, a thorough understanding of the pathways that result in ulcer development is increasingly important. The words of the Scottish poet Thomas Campbell can be applied to the breakdown of diabetic foot. Ulceration does not occur spontaneously: rather, it is combination of causative factors that result in the development of a lesion. Many warning signs or " shadows " can identify those at risk before the occurrence of an ulcer. It is not an inevitable consequence of having diabetes that ulcers
Occurrence
Ulcers invariably result from an interaction between specific pathologies in the lower limb and environmental hazards. The breakdown of the diabetic foot traditionally has been considered to result from an interaction between peripheral vascular disease (PVD), peripheral neuropathy, and some form of trauma. Other causes are briefly described.
5.1 Peripheral vascular disease
A brief mention of the role of PVD in the development of foot ulcers must be made here. PVD tends to occur at a younger age in patients with diabetes and is more likely to involve distal vessels. Reports from the USA and Finland have confirmed that PVD is a major contributory factor in the pathogenesis of foot ulceration and subsequent major amputations [25,26]. In the pathogenesis of ulceration, PVD itself rarely causes ulceration, and as will be discussed for neuropathy, it is a combination of risk factors with minor trauma that inevitably leads to ulceration (Figure 44.1). Thus, minor injury and subsequent infection increase the demand for blood supply beyond the circulatory capacity, and ischemic ulceration and the risk of amputation ensue. In recent years, neuro ischemineuro ulcers in which a combination of neuropathy and PVD exists in the same patient, together with some form of trauma, are becoming increasingly common in diabetic foot clinics.
5.2 Diabetic neuropathy
Diabetic neuropathies represent the most common form of long-term complication of diabetes, affect different parts of the nervous system, and may present with diverse clinical manifestations [27]. The most common neuropathies are chronic sensorimotor distal symmetrical polyneuropathy and autonomic neuropathy. It is the common sensorimotor neuropathy together with peripheral Autonomic sympathetic neuropathy plays an important role in ulceration pathogenesis.
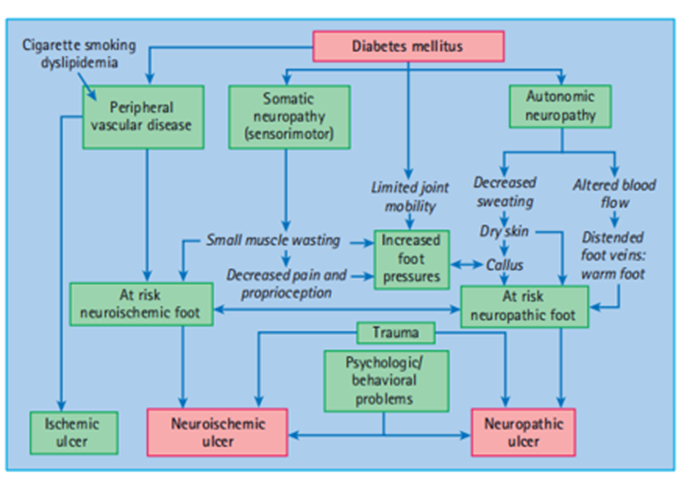
Figure 44.1 Pathways to foot ulceration in diabetes. Reproduced from Boulton et al. [7], with permission.
5.21 Sensorimotor neuropathy
This type of neuropathy is very common, and it has been estimated that up to 50% of older patients with type 2 diabetes have evidence of sensory loss on clinical examination, and therefore must be considered at risk of insensitive foot injury [27]. This type of neuropathy commonly results in a Sensory loss confirmed on examination by a deficit in the stocking distribution to all sensory modalities: Evidence of motor dysfunction in the form of small muscle wasting is also often present. While some patients may give a history (past or present) of typical neuropathic symptoms such as burning pain, stabbing pain, and paresthesia with nocturnal exacerbation, others may develop sensory loss with no history of symptoms. Other patients may have the " painful - painless " leg with spontaneous discomfort secondary to neuropathic symptoms but who on examination the have both small and large fiber sensory deficits: Such patients are at great risk of painless injury to their feet. From the above, it should be clear that a spectrum of symptomatic severity may be present with some patients experiencing severe pain, and at the other end of the spectrum, patients who had no spontaneous symptoms, but both groups may have experienced significant sensory loss. The most challenging patients are those who develop sensory loss with no symptoms because it is often difficult to convince them that they are at risk of foot ulceration because they feel no discomfort, and the motivation to perform regular foot self-care is difficult. The important message is that neuropathic
symptoms correlate poorly with sensory loss, and their absence must never be equated to a lack of foot ulcer risk. Thus, assessment of foot ulcer risk must always include a careful foot examination after the removal of shoes and socks, whatever the neuropathic history [27].
5.22 The patient with sensory loss
A reduction in neuropathic foot problems will only be achieved if we remember that those patients with insensitive feet have lost their warning signal–pain–that ordinarily brings patients to their doctors. Thus, the care of patients with sensory loss is a new challenge for which we have no training. It is difficult for us to understand, for example, that an intelligent patient would buy and wear a pair of shoes of three sizes that are too small to come to the clinic with extensive shoe-induced ulceration. The explanation is simple: with reduced sensation, a very tight fit stimulates the remaining pressure nerve endings and is thus interpreted as a normal fit – hence the common complaint when we provide patients with custom-designed shoes that " these shoes are too loose ". We can learn much about the management of such patients from the treatment of patients with leprosy [28]. Although the cause of sensory loss is very different from that in diabetes, the result is the same; thus, work on leprosy has been very applicable to our knowledge of the pathogenesis of diabetic foot lesions. It became Logo (1914 – 2003), who labored as a physician and a missionary in South India, who defined the ache as "God's the greatest present to mankind’ [29]. He emphasized the electricity of medical remarks to his students, and one statement of his became very relevant to diabetic foot ulceration was that any affected person with a plantar ulcer who walked into the hospital without a limp had neuropathy. The brand additionally taught us that if we're to prevail, we have to realize that with the loss of pain, there may also be dwindled motivation within the recuperation of, and prevention of, damage. 5.23Peripheral sympathetic and autonomic neuropathy Sympathetic autonomic disorder of the decreased limbs leads to reduced sweating and effects in dry skin that is prone to cracking and fissures and booms blood drift (in the absence of large vessel obstructive PVD) with arteriovenous shunting mainly to the nice and cozy foot. The complicated interactions of the neuropathies and different contributory factors to the causation of foot ulcers are summarized in determining the value of 44. 1. 5.3 Other risk factors
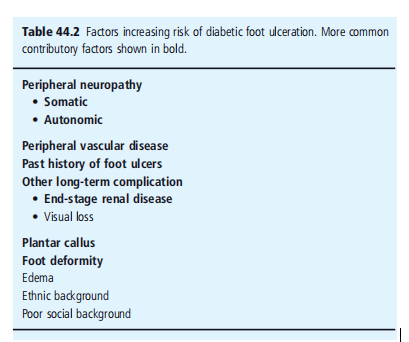
Of all of the different hazard factors for ulceration (table 44.2) one of the maximum essential is a history of similar issues. in lots of series, this has
Plantar callus
Callus bureaucracy beneath weight-bearing regions because of dry pores and skin (autonomic dysfunction), insensitivity, and repetitive moderate pressure from a high foot strain. It acts as a foreign body and reasons ulceration [31]. The presence of a callus in an insensate foot need to alert the doctor that this affected person is at a high risk of ulceration, and the callus should be eliminated through the podiatrist or a different trained fitness care professional. Elevated foot pressures Several studies have confirmed the contributory function of abnormal plantar pressure in the pathogenesis of foot ulcers [3-32].
Foot deformity
A mixture of motor neuropathy, neuroarthropathy, and altered gait styles is thought to result in the " excessive danger " of the new allopathic foot, with clawing of the ft, prominent metatarsal heads, high arch, and small muscle loss (figure 44.2).
Ethnicity and Gender
Male intercourse has been associated with a 1.6 - fold increase in ulcers [11]. With appreciation to the ethnic starting place, facts from the pass-sectional studies in Europe suggest that foot ulceration is extra, not unusual in Europid topics than other racial groups: for instance, the North-West Diabetes Foot Care examination within the United Kingdom confirmed that the age-adjusted occurrence of diabetic foot ulcers (past or gift) for Europeans, South Asians, and African - Caribbeans became 5.5%, 1.8% and 2.7%, respectively [33]. reasons for these ethnic variations without a doubt warrant additional investigation. In contrast, in southern America, ulceration becomes plentiful, not unusual in Latino people and native individuals compared to White humans of Northern ecu ancestry [34]. however, the latest statistics confirmed this increased risk in Latinos, despite the foot pressures being lower in this group [35].

Figure 44.2 The high-risk neuropathic diabetic foot demonstrating high arch, prominent metatarsal heads, clawing of toes and callus under first metatarsal h
Pathway to ulceration
It is a combination of two or more risk factors that ultimately result in diabetic foot ulceration (Figure 44.1). Both Pecoraro et al. [25]. and later Reiber et al. [36] have taken the Rothman model for causation and applied this to amputation and foot ulceration in diabetes. This model is based on the concept that a component cause (e.g., neuropathy) is not sufficient in itself to lead adopted to ulceration, but when the component causes act together, they result in a sufficient cause, which will inevitably result in ulceration. Applying this model to foot ulceration, a small number of causal pathways were identified: the most common triad of component causes, present in nearly two out of three incident foot ulcer cases were neuropathy, deformity, and trauma. Edema and ischemia were also common component causes. Other simple examples of two-component cause of ulceration include loss of sensation and mechanical trauma, such as standing on a nail, wearing shoes that are too small, or neuropathy and thermal trauma (e.g., walking on hot surfaces or burning feet in the bath), and neuropathy and chemical trauma may result in ulceration from inappropriate use, for example, of chemical " corn cures. " Similarly, this model can be applied to neuro ischemic ulcers, in which the three components cause ischemia, trauma, and neuropathy are often seen.
Prevention of diabetic foot ulcers
10.1 Screening
It is estimated that the vast majority of foot ulcers are potentially preventable, and the first step in prevention is the identification of the "at-risk" population. Many countries have now adopted the principle of the " annual review " for patients with diabetes, whereby every patient is screened at least annually for evidence of diabetic complications. Such a review can be carried out either in primary care centers or hospital clinics. A task force of the American Diabetes Association recently addressed the question of what should be included in the annual review of the " comprehensive diabetic foot examination (CDFE) " [37]. The task force addressed and concisely summarized the recent literature in this area and recommended, where possible using evidence-based medicine, which should be included in the CDFE for adult patients with diabetes. While a brief history was regarded as important, a careful examination of the foot, including an assessment of its neurologic and vascular status, was regarded as essential. There is strong evidence to support the use of simple clinical tests as predictors of foot ulcers [11-37]. A summary of the key components of CDFE is provided in Table 44.3. Although each potential simple neurologic clinical test has advantages and disadvantages, it was felt that the 10 g mono filament had much evidence to support its use; hence, the recommendation that the assessment of neuropathy should comprise the use of a 10 g mono filament plus one other test. In addition to the simple tests listed in Table 44.3, one possible test for neuropathy is the assessment of the vibration perception threshold.

Although this is a semi-quantitative test of sensation, it was included in many centers in both Europe and North America. As can be seen from Table 44.3, this is not regarded as essential, but strong evidence supports the use of the vibration perception threshold as an excellent predictor of foot ulceration [38,39].
Concerning vasculature, the ankle-brachial index was recommended, although it was realized that many centers in primary care may not be able to perform this in day-to-day clinical practice.
10.2 Intervention for high - risk patients
Any abnormality in the above screening test would put the patient at a higher risk of foot ulceration. Potential interventions are discussed in several headings, the most important of which is education.
10.3Education
Previous studies have suggested that patients with foot ulcer risk lack knowledge and skills and are consequently unable to provide appropriate foot self-care [40]. Patients need to be informed of the risk of having insensate feet, the need for regular self-inspection, foot hygiene, and chiropody/podiatry treatment as required, and they must be told what action to take in the event of an injury or discovery of a foot ulcer. Recent studies summarized by Vileikyte et al. [41,42] suggest that patients often have distorted beliefs about neuropathy, thinking that this is a circulatory and linking neuropathy directly to amputation. Thus, an education program that focuses on reducing foot ulcers will be doomed to failure if patients do not believe that foot ulcers precede amputations. Much work is required in this area if appropriate education is to succeed in reducing foot ulcers and subsequent amputation. The potential for education and self-care at various points in the pathway of neuropathic ulceration is shown in Figure 44.3. There have been a small number of reports that assess educational interventions, but these have mostly been small single-center studies. In the most recently published study, even though the foot care education program was followed by improved foot care behavior, there is no evidence that such targeted education was associated with a reduced incidence of recurrent foot ulcers [43]. It has been suggested that patients find the concept of neuropathy difficult to understand; they are reassured because they have no discomfort or pain in their feet. It may be that using Visual aids (which can also be used for diagnosis of the at-risk foot) may help patients understand that there is something different about their feet compared with their partner's, for example. This might include the use of the administered indicator plaster (Neuro pad): when applied to the foot this changes color from blue to pink if there is normal sweating [44]. The absence of sweating, such as in high-risk feet, results in no color change, enabling patients to see that there is something different about their feet. A similar visual aid is the Pressure Stat (Podotrack) (Figure 44.4) [45]. This is a simple, inexpensive, and semi-quantitative footprint mat that can identify high plantar pressures. The The higher the pressure, the darker the color of the footprint. Similarly, this can be used as an educational aid and might help the patient realize that specific areas under their feet are at particular risk of ulceration.
In summary, foot care education is believed to be crucial for the prevention of ulceration, although there is little support from randomized controlled trials. Further studies in this area are Therefore, this is an urgent requirement.
10.4 Podiatry/chiropody
Even though no longer available in each use of normal nails and pores, skincare from a podiatrist/chiropodist is essential in excessive-threat neuropathic foot. attempted self-care has been mentioned in numerous cases to cause ulceration, and the self-care of calluses should be discouraged. Chiropodists and podiatrists have to be connected to the foot care group if to be had and also can educate the patient at the same time as treating the feet.
10.5 shoes/othoses/hosiery
Besides-the-point shoes are not unusual motives for foot ulceration in insensitive feet, whereas proper footwear can reduce ulcer occurrence [40]. This announcement is supported by randomized managed trials [46]. There is evidence from the literature to aid the use of professional hosiery, which might lessen foot pressure and provide all-spherical protection to excessive-threat neuropathic feet [47,48].
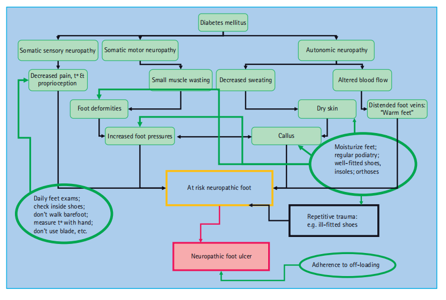
Figure 44.3 The potential for education and self - care in prevention of neuropathic foot ulcers. t °, temperature. Courtesy of L. Vileikyte MD, PhD.
10.6 Self-monitoring of skin temperature
It has been known for some time that prior to skin breakdown and ulceration, the involved area of the foot tends to warm up as a consequence of local inflammation. In an appropriately designed randomized controlled trial, Lavery et al. [49]. Randomized patients with a history of neuropathic foot ulceration in too one of three groups, the main intervention being self-monitoring of skin temperature of both fee, and patients who received this skin temperature thermometer were advised to rest or contact their foot clinic should have maintained a difference in temperature between the two feet. This study clearly showed that patients who monitored their skin temperature and followed the advice had a markedly reduced incidence of recurrent ulceration (8% vs. 30%). Thus, infrared temperature home monitoring might help to identify the " pre - ulcerative " foot and permit intervention before actual skin breakdown. A more recent study has provided further support for this notion [50].
10.7 Injected liquid silicone
Injected liquid silicone under high-pressure areas of the diabetic foot has been used for some years in the USA and is supported by a randomized controlled trial [51]. which confirmed that those Patients receiving active agents had reduced foot pressure and increased subcutaneous tissue under the high-pressure areas of the forefoot. This therapy is now available in certain European countries, and a follow-up study [52]. confirmed that the effect of this " injectable orthosis "lasts for up to 2 years, although booster injections may be required occasionally.
Foot ulcers: diagnosis and management
11.1Foot ulcer classification
Despite increasing efforts in the early identification and preventative foot care education of high-risk patients, foot ulcers continue to be a major issue in diabetes management and may indeed be presenting features of type 2 diabetes. The principles of management depend on a careful assessment of the causative factors, presence or absence of infection, and degree of neuropathy and/or ischemia in the foot. Before discussing the management of specific types of ulcers, it is important to consider the classification of foot lesions. Numerous classification systems for diabetic foot ulcers have been proposed [53]. but only a few have been described.
The most widely used foot ulcer classification system worldwide at the time of writing is the Meggitt – Wagner grading system, as shown in Table 44.4. Despite its wide use, this system does lack specific city, and does not refer to the neuropathic, ischemic, or infective status of the ulcers. The newer University of Texas (UT) wound classification system is currently widely used (Table 44.5) [54]. This is based on the Meggitt – Wagner system, but with the addition of grades of ulcers and stages, each grade for the presence or absence of infection and ischemia. In a comparative study of these two systems, the UT system was shown to be a useful predictor of outcomes, although the Meggitt – Wagner system was still confirmed to be useful [55]. A high-risk foot with pre - ulcerative lesions (Wagner grade 0, UT1A) are shown in Figure 44.5. The two more recently described classification systems, S(AD) SAD system, (size (area, depth), sepsis, arteriopathy, and denervation) and the Perfusion, extent, depth, infection, and sensation (PEDIS) systems appear to have some advantages over earlier systems but are not widely used [53]. Thus, the UT system will be used to describes the ulcer classification.
11.2 Wound healing in the diabetic foot
Wound healing is a tissue response to injury and passes through the phases of inflammation, chemotaxis, cellular proliferation, extracellular matrix deposition, and finally wound remodeling and scarring. Diabetes may influence foot wound healing in several ways, including impairment of peripheral circulation, altered leukocyte function, disturbed balance of cytokines and proteases, and chronic hyperglycemia itself [3-56].
Thus, foot ulcers in patients with diabetes are as follows: recalcitrant to healing owing to many cellular and molecular aberrations. When compared with normal acute wound healing, chronic foot ulcers are often stalled in the chronic inflammatory phase, with impaired granulation tissue formation. A key question is, therefore, whether there is a fundamental impairment of wound healing in diabetes, and if so, what are the molecular and cellular impairments that are specific to chronic wounds? Several studies have reported abnormalities in cytokines and growth factors in tissues of chronic diabetic foot ulcers [57 – 59]. Most recently, it has been suggested that the levels of matrix metalloproteinases (MMP) are important for predicting the likelihood of wound healing, and a high level of MMP - 1 is essential for wound healing [59]. Another contributory factor to impaired wound healing in diabetes appears to be the repetitive pressure on the wound. The pivotal role of offloading is therefore considered in the next section
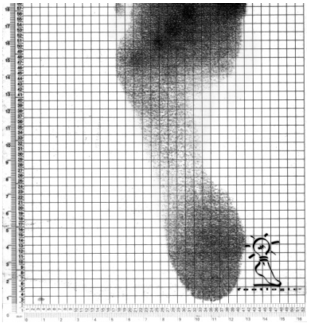
Figure 44.4 A black and white pressure distribution of one footstep using Pressure Stat: the darkest areas represent highest pressures, in this case under metatarsal heads 1 and 3 and the hallux.
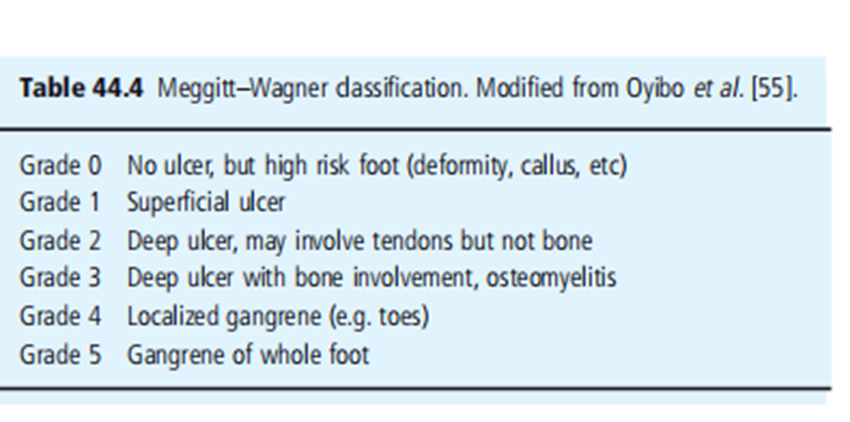
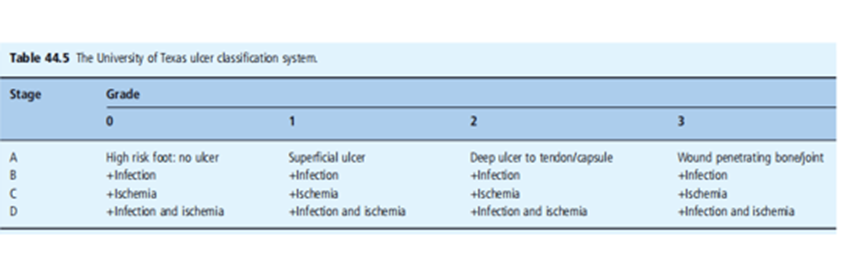

Figure 44.5 Wagner grade I ulcer, UT1A foot ulcer, showing a rim of callus and a punched out neuropathic ulcer in the metatarsal head region with no evidence of infection.
11.3 Offloading
A normal individual with a foot wound will limp: it has been known for some time that neuropathic plantar foot wounds will heal satisfactorily when offloaded in a Total Contact Cast (TCC) [3]. The principle of TCC management is that the pressure is mitigated; however, the device is irremovable, thus enforcing compliance with therapy. Several randomized controlled trials have compared the TCC with other removable offloading devices in plantar diabetic foot ulcers and invariably, healing is most rapid in those randomized to TCC treatment [3-60]. As it is known that Removable Cast Walkers (RCW) similarly redistribute pressure to the TCC, the question remains as to why the TCC usually demonstrates superiority in terms of speed of wound closure. The most likely explanation is the offloading device in the management of neuro ischemic ulcer ulcers, but only if they may not be clinically infected (UT 1C, 2C) [65].
For the one's sufferers handled with irremovable forged walkers, it is advocated that the forged be eliminated, to begin with on a weekly foundation for wound assessment, d é abridgment, and cleansing. recuperation can commonly be carried out in a duration of 6 – 12 weeks in a cast: it's far strongly advocated that when the plantar wound has healed, the cast should be worn for similarly four weeks to permit the scar tissue to firm up. Thereafter, the affected person may be progressively transferred to the appropriate footwear, which may additionally want extra depth or, in the case of extreme deformity, custom-molded.
11.4 Dressings
The danger of dressings and bandages is that some healthcare professionals may draw a false sense of security from them, believing that by dressing an ulcer, they are curing it. Nothing could be further from the truth regarding neuropathic ulcers. The three most important factors in the healing of foot ulcer are freedom from pressure, freedom from infection, and good Vascularity. The purpose of dressings is to protect the wound from local trauma, minimize the risk of infection, and optimize the wound environment, which should be moist in most cases. The evidence bases to support the choice of any particular dressing is woefully inadequate, with a few trials generally hampered by small numbers, inappropriate comparator, and poor study design [66,67]. There is little evidence that any specific dressing has a major effect on the rate of wound healing.
- 11.5 Management of infection
- One of the first steps in the management of a foot ulcer is to determine whether the infection is present or not: remember that all foot ulcers are colonized with potentially pathogenic organisms It is generally accepted by the international working group on diabetic foot that the diagnosis of infection in diabetic foot ulcers remains a clinical one [68]. Thus, the presence of signs such as purulent discharge, erythema, local warmth, and swelling suggest an infection requiring appropriate treatment.
11.6 Clinically on - infected ulcers
where ulcers aren't inflamed and predominantly neuropathic (UT grades 1A, 2A), the usage of antibiotics can be withheld as Chantelau et al. [69]. have shown that with appropriate wound control, patients performed similarly with or without systemic antibiotics in a randomized controlled trial. However, frequent assessment, de abridgment, and callus elimination collectively with offloading is a crucial part of the control of neuropathic foot ulcers, and must signs and symptoms of contamination develop, and antibiotics may be needed. For the ones with ulcers with an ischemic factor that do now not have gross symptoms of contamination (UT 1C, 2C) antibiotics need to Probably, in most instances, the aggregate of infection and ischemia in the diabetic foot is not an unusual purpose of closing lower extremity amputation.
- 11.7 Clinically it infected ulcers
non-limb-threatening inflamed ulcers (UT 1 B, 1D, 2 B, and 2nd) can normally be treated on an outpatient basis, and oral wide-spectrum antibiotics must be used until the effects of touchyties are acquired. As reviewed by Lipsky, international pointers have been published in recent years [68-71]. One critical thing of these recent guidelines has been the development of standards by which to classify the severity of diabetic foot contamination. generally, slight infections are highly superficial and constrained, moderate infections involve deeper tissues, and severe Infections are observed using systematic signs, symptoms, or symptoms of infection or metabolic disturbances [68]. Any ulcer with clinical evidence of contamination must have tissue taken and despatched for lifestyle and sensitivity in the microbiological branch. Although great-facial swabs are normally taken, deep (preferably tissue) specimens are optimal in terms of diagnostic accuracy [68]. The most infective ulcers are poly microbial, regularly with a combination of anaerobes and aerobes. A systematic evaluation of antimicrobial treatments for diabetic foot ulcers revealed that few of them should be designed. Randomized controlled research has been carried out, and it is difficult to present precise guidelines on antibiotic regimens for particular infective organisms [72]. however, if there is any suspicion of osteomyelitis (signs that include a sausage-shaped toe or the ability to probe to the bone may advocate this prognosis) have to have a radiograph taken of the inflamed foot and probable in addition investigations (see under and Chapter 50). Then. methicillin-resistant methicillin-resistant Staphylococcus aureus (MRSA). In most cases, MRSA is isolated as an opportunistic colonizing organism following treatment with inappropriate long-duration broad-spectrum antibiotics. If MRSA is felt to be an infecting organism, there are useful new agents, such as linezolid [68]. which can be administered parenterally or orally and are effective against such organisms. There is a suggestion that larval therapy [74]. might be useful in eradicating MRSA that contaminates diabetic foot wounds.
11.71 Osteomyelitis
The diagnosis of osteomyelitis is controversial and several diagnostic tests have been recommended. Amongst these, " probing to bone " has been shown to have a relatively high predictive value, whereas plain radiographs are insensitive to the natural history of osteomyelitis. In most clinical cases, however, the diagnosis is ultimately made by Plain radiograph of the foot (Figure 44.7). Magnetic resonance imaging (MRI) has an increasing role in diagnosis owing to its high sensitivity [75]. The combination of an ulcer area > 2 × 2 cm, a positive probe-to-bone test, an elevated sedimentation rate, and an abnormal radiograph is most helpful in diagnosing the presence of osteomyelitis in the diabetic foot, whereas a negative MRI makes a diagnosis much less likely [76]. The most recent review on this topic suggests that a combination of clinical and laboratory findings can significantly improve the diagnostic accuracy for osteomyelitis in the diabetic foot, and the specific combination of ulcer depth and serum inflammatory markers appears to be particularly sensitive [77]. Contrary to traditional teaching, it is increasingly recognized that some cases of localized osteomyelitis can be managed by long-term (10 – 12 weeks) antibiotic therapy [78]. however, localized bony resection after appropriate antibiotic therapy is a common treatment approach. Cases with osteomyelitis confined to one bone without the involvement of a joint are most likely to respond to antibiotic therapy, particularly in the absence of peripheral vascular disease. It must be pointed out that data to inform treatment choices in osteomyelitis of the diabetic foot for randomized controlled trials is limited, and further research is urgently required [79].
11.72 Adjunctive therapies
Several new approaches to promote more rapid healing in diabetic feet have been described over the last two decades. Some of those are mentioned below but many were also recently reviewed by the International Working Group on Diabetic Foot [80].
11.73 Growth factors
Several growth factors and other agents designed to modify abnormalities in the biochemistry of the wound bed or surrounding tissues have been described, but there is still no consensus on their use in day-to-day clinical practice [80]. One such example is platelet-derived growth factor (PDGF), which is available for clinical use in several countries. Although there is some support for their use in randomized clinical studies [81]. their expense, together with the fact that most neuropathic ulcers can be healed with appropriate offloading, has limited their use. Unfortunately, PDGF, together with other topically applied agents, such as epidermal growth factor, do not have sufficient robust data to support their day-to-day use in routine clinical practice.
Hyperbaric oxygen
Hyperbaric oxygen (HBO) has been widely used for the management of non-healing diabetic foot ulcers, particularly in the USA, for several years. Many of the reported studies have been poorly designed or anecdotal and have given rise to serious concerns about the widespread use of this treatment [82]. however, there have been several small well - designed randomized controlled trials to assess the efficacy of HBO in ischemic diabetic foot wounds [83]. Whereas the systematic review of the International Working Group that considered HBO accepted that there was some evidence to support its use, it is clear that more data are required from larger controlled trials not only to confirm the efficacy but also to clarify which wounds might best benefit from this expensive treatment [80-84].
Negative pressure wound therapy
Over the past several years, negative pressure wound therapy (NPWT) using vacuum-assisted closure has emerged as a commonly employed option in the treatment of complex wounds in diabetic foot [85]. Previous work has suggested that the application of negative pressure optimizes blood flow, decreases local tissue edema, and removes excessive fluid and pro-inflammatory Exudate from the wound bed. There is now controlled trial evidence for the use of NPWT in both local postoperative wounds in diabetic foot [86] and, more recently, in the management of complex but non-surgical diabetic foot ulcers [87]. It is clear that this treatment helps promote the formation of granulation tissue, but its cost will limit its use to those complex diabetic foot wounds that did not respond to standard therapies.
Bioengineered skin substitutes
Similar to other treatments in this group of adjunctive therapies although there is some evidence to support the use of bio-engineered skin substitutes in non-infected neuropathic ulcers, its use is somewhat restricted by cost [80]. A systematic review of this topic concluded that the trials assessed were of questionable quality, and until high-quality studies were performed, recommendations for the use of these skin substitutes could not be made [88].
Charcot neuroarthropathy
Charcot neuroarthropathy (CN) is a non-infective arthropathy that takes place in a properly perfused insensate foot. even though the precise mechanism underlying the improvement of CN remains uncertain, development has been made in our statistics on the retinopathy genesis of this disorder in the remaining decade. it's far clear that the conventional non traumatic and neurotrophic theories for the pathogenesis of acute CN in diabetes do not cope with high-quality key competencies of the disorders [89]. If the preceding principle has been correct, CN is probably a bargain greater common and ought to be symmetrical: in assessment, acute CN is rather unusual amongst patients with neuropathy and is commonly asymmetrical, even though there is an extended hazard of a growing CN in the contralateral foot some years later.
CN occurs in a properly perfused, insensate foot. Generally, a patient’s gift with warmness, swollen foot, and opposite to a number of earlier texts, can be accompanied by pain or as a minimum pain within the affected limb. The affected individual tends to be slightly extra younger than is every day for the affected person furnished with a diabetic foot ulcer and normally gives with a heat swollen foot which may additionally or won't be painful. even though a history of trauma may be a gift, the trauma is rarely of enough severity to account for the abnormalities positioned on clinical exam (determine 44.7). even though CN is characterized by increased close-by bone resorption, the correct mobile mechanisms contributing to this case stay unresolved. lately, receptor activators of the nuclear factor κB ligand (RANKL) have been recognized as an important mediator for osteoclasts formation and activation. It has been hypothesized that the RANKL/osteoprotegerin (OPG) pathway also plays a vital role in the development of acute CN [89]. It has been shown that peripheral blood monocytes removed from sufferers with CN and cultured inside the presence of macrophages, a colony-stimulating factor, added approximately an improved osteoclasts formation when compared to healthy and diabetic-controlled monocytes [90]. The observations of one study suggested that RANKL-mediated osteoclastic resorption occurs in acute CN.
As a result, the RANKL-primarily based pathway is essential for the pathogenesis of acute CN, suggesting that inhibition of RANKL might be useful as a control in the future.
Treatment of the foot in CN is based on the level at which the ailment is identified. In the acute section, there is evidence that offloading the affected foot by way of the use of plaster and solid is the most effective approach to reducing disorder pastime and local inflammation. The use of the cast needs to hold until the swelling and hyperemia have resolved and the skin temperature differential is 1 °C or much less, at which point the generation of custom-molded footwear with suitable insoles is indicated [91]. Bisphosphonates are strong inhibitors of osteoclasts activation and intravenous pamidronate has been tested to be useful in decreasing disease hobby in acute CN [92]. Large randomized controlled trials are required to confirm these initial observations. The management of advanced CN with bone deformity requiring reconstructive surgery is beyond the scope of this chapter and the reader is said to modern-day evaluations [93].
16 Research Method:
To investigate foot problems in patients with diabetes, a commonplace study approach could be a move-sectional examination involving a sample of diabetic patients. Taking a look at this might involve gathering facts on the prevalence and forms of foot troubles experienced by these patients.
17 Result:
The precise outcomes of the examination might depend on the sample length, the characteristics of the individuals, and the methods used. However, studies on foot problems in patients with diabetes have shown a high prevalence of foot-associated headaches. These headaches can range from minor problems, such as dry skin and calluses, to severe problems, including foot ulcers and infections.
18 Discussion:
The discussion of research outcomes might involve interpreting the findings and discussing their implications. Some key points that may arise during the discussion are as follows.
Incidence and risk factors: The discussion might also highlight the excessive prevalence of foot problems in patients with diabetes and identify the factors that contribute to their extended threat. Hazard elements may also encompass negative glycemic manipulation, duration of diabetes, peripheral neuropathy (nerve damage), peripheral vascular ailments (circulatory issues), foot deformities, and insufficient foot care.
Impact on exceptional o existence: Foot problems in diabetic patients can considerably impact their pleasant lifestyles. The discussion may additionally focus on the physical soreness, aches, and barriers in mobility that foot headaches can cause, leading to a discounted capability to perform daily activities and an elevated chance of incapacity.
Development of headaches: Foot issues, if left untreated or poorly managed, can progress to serious complications, including foot ulcers, infections, and amputations. The discussion emphasizes the significance of early detection, normal foot examinations, and proper foot care practices to prevent the progression of problems.
Preventive measures: The dialogue may additionally address techniques for preventing foot problems in diabetic patients. This will include patient education on foot care, ordinary foot inspections, proper footwear choice, controlling blood sugar levels, and promoting a wholesome way of life to reduce the risk factors associated with foot headaches.
Multidisciplinary approach: Handling foot issues in diabetic patients frequently requires a multidisciplinary method involving healthcare professionals consisting of physicians, podiatrists, diabetes educators, and wound care experts. The discussion may additionally underscore the significance of collaboration among healthcare carriers in optimizing foot care and enhancing affected-person effects.
Future study directions: The dialogue may additionally spotlight regions for future studies, together with exploring novel interventions, developing powerful instructional programs, or investigating the effect of unique risk factors on foot problems in patients with diabetes. This can help in additional studies and interventions to improve foot care in this population. Ordinarily, the discussion might aim to offer comprehensive knowledge of foot issues in patients with diabetes, their implications, and potential techniques to prevent and control these problems efficiently.
Conclusions
There can be no doubt that despite our efforts in early identification, prevention, and aggressive treatment of diabetic foot problems, the incidence of diabetic foot disease is likely to increase in the next few decades, with a global explosion in the prevalence of type 2 diabetes reviewed elsewhere in this book. It is also clear that diabetic foot disease carries not only a significantly higher risk but also mortality. [94]. pointed out that the outlook for patients with diabetic foot disease is worse than that for patients with many malignant diseases. There is increasing recognition of the multifactorial nature of complications, which led Young et al. [95] .to review the survival of patients with diabetic foot lesions over the past 13 years. They reported that survival has improved
This has been accompanied by the adoption of an aggressive cardiovascular risk management policy that should be encouraged in all patients with diabetic foot disease. The ultimate prognosis for the limb with a diabetic foot lesion depends upon the presence or absence of an ischemic component, it has been shown that patients with higher Wagner or UT grading and severity are more likely to result in minor or major amputations. Thus, neuropathic foot lesions generally carry a good prognosis, whereas those with significant ischaemic components are more likely to require the input of the vascular surgeon.
The team approach
It should be clear that the spectrum of diabetic foot problems requires the involvement of individuals from many specialties. The diabetic foot cannot be regarded as the sole responsibility of the Diabetologist, and several reports over the last decade have promoted the benefits of a multidisciplinary approach to diabetic foot care [96]. This started in the early 1990s when the concept of the " annual review " was adopted by most national diabetes societies. This requires that all patients with diabetes be screened on an annual basis for evidence of long-term complications [97]. There is increasing evidence from several long-term studies that the adoption of this approach not only in hospitals but in community care, has been associated with a reduced incidence of foot problems [98 – 101]. The improved management of diabetic foot care in the district of Leverkusen, Germany ultimately resulted in a 37% reduction in non-traumatic amputations in patients with diabetes; however, this took more than 10 years after the establishment of specialist foot care [98] .Two studies from the UK [99,100] have reported reductions of up to 60% in diabetic amputations and both of these followed either the introduction of multidisciplinary teamwork in the community or the improved organization of general diabetes care. Finally, a sustained reduction in major amputations has been reported in Sweden over the last 20 years suggesting that a substantial decrease in diabetes-related amputations can not only be achieved but maintained over a long period [101]. The team approach involves Diabetologist working together with surgeons (orthopedic and vascular), specialist nurses, podiatrists, orthotics, and often many other health care professionals is therefore strongly recommended in the management of complex lesions of the diabetic foot. It should be remembered; however, it is the patient at risk of, or with foot ulceration, who must be regarded as the most important in this team. Without the patient's willing participation, there is little that the other team members can achieve to improve the overall outlook for the diabetic foot in the 21st century.
Acknowledgment
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project We would also like to thank My Mentor [. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project Declaration of Interest I at this moment declare that:
I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript
References
- Singh N, Armstrong DG, Lipsky BA. (2005). preventing foot ulcers in patients with diabetes. JAMA, 293: 217-228.
View at Publisher | View at Google Scholar - Boulton AJM, Vileikyte L, Ragnarson - Tennvall G, Apelqvist J. (2005). The global burden of diabetic foot ailment. Lancet, 366 1719-1724.
View at Publisher | View at Google Scholar - Boulton AJM. (2004). The diabetic foot: from artwork to technological know-how: the 18th Camillo Golgi lecture. Diabetologia, 47:1343-1353.
View at Publisher | View at Google Scholar - Ragnarson - Tennvall G, Apelqvist J. (2001). Prevention of diabetes-related foot ulcers and amputations: a value – software evaluation primarily based on Markov version simulations. Diabetologia, 44:2077-2087.
View at Publisher | View at Google Scholar - Connor H. (2008). Some ancient elements of diabetic foot ailment. Diabet Metab Res Rev, 24:7-13.
View at Publisher | View at Google Scholar - McKeown KC. (1995). The records of the diabetic foot. Diabet Med ,12: 19-23.
View at Publisher | View at Google Scholar - Boulton AJM, Cavanagh PR, Rayman G. (2006). The Foot in Diabetes I, 4th edn. Chichester: John Wiley & Sons Ltd.
View at Publisher | View at Google Scholar - Bowker JH, Pfeifer MA. (2008). Levin & O ' Neal's The Diabetic Foot, 7th edn. Philadelphia: Mosby – Elsevier.
View at Publisher | View at Google Scholar - S ä maan A, Tajiyeva O, Müller N, Tschauner T, Hoyer H, Wolf G, et al. (2008). Incidence of Diabetic foot syndrome on the number one care stage in Germany: a cross-sectional observation. Diabet Med, 25: 557-563.
View at Publisher | View at Google Scholar - Al - Mahroos F, Al - Roomi K. (2007). Diabetic neuropathy foot ulceration, peripheral vascular sickness and capability chance elements amongst sufferers with diabetes in Bahrain: a nationwide primary care diabetes sanatorium - primarily based on observation. Ann Saudi Med, 27: 25-31.
View at Publisher | View at Google Scholar - Abbott CA, Carrington AL, Ashe H, bathtub S, every LC, Griffiths J, et al. (2002). The Northwest Diabetes Foot Care take a look at the occurrence of, and hazard factors for brand new diabetic foot ulceration in a community-based patient cohort. Diabet Med, 19:377- 384.
View at Publisher | View at Google Scholar - Manes C, Papazoglou N, Sassidou E, Tzounas. (2002). okay, incidence of diabetic neuropathy and foot ulceration: a population-based study. Wounds,14: 11-15.
View at Publisher | View at Google Scholar - M ü ller IS, de Grauw WJ, van Gerwen WH, Bartelink ML, van Den Hoogen HJ, Rutten GE. (2002). Foot ulceration and decrease limb amputation in kind 2 diabetic sufferers in Dutch primary fitness care. Diabetes Care, 25:570-576.
View at Publisher | View at Google Scholar - Ramsay SD, Newton K, Blough D, McCulloch DK, Sandhu N, Reiber GE, et al. (1999). Prevalence, results, and expenses of foot ulcers in patients with diabetes. Diabetes Care, 22: 382-387.
View at Publisher | View at Google Scholar - Vozar J, Adamka J, Holeczy P. (1997). Diabetics with foot lesions and amputations in the location of sexy Zitmy Ostrov 1993 – 1995. Diabetologia, 40:46.
View at Publisher | View at Google Scholar - Kumar S, Ashe HA, Parnell LN, Fernando DJ, younger RJ, Tsigos C, et al. (1994). The prevalence of foot ulceration and its correlates in type 2 diabetic patients: a populace-based take a look at. Diabet Med, 11:480-484.
View at Publisher | View at Google Scholar - Moss S, Klein R, Klein B. (1992). The superiority and occurrence of lower extremity amputation in a diabetic population. Arch Intern Med ,152: 510 -616.
View at Publisher | View at Google Scholar - Boulton AJM, Vileikyte L. (2008). Diabetic foot problems and their management around the sector. In: Bowker JH, Pfeifer MA, eds. Levin & O ' Neal's The Diabetic Foot, 7th edn. Philadelphia: Mosby - Elsevier,487-496.
View at Publisher | View at Google Scholar - Van Houtun WH. (2008). Amputations and ulceration: pitfalls in assessing occurrence. Diabet Metab Res Rev ,24 14-18.
View at Publisher | View at Google Scholar - Deerochanawong C, domestic PD, Alberti KG. (1992). A survey of decreased - limb amputations in diabetic sufferers. Diabet Med ,9: 942 -946.
View at Publisher | View at Google Scholar - Shearer A, Scuffham P, Gordois A, Oglesby A. (2003). Predicted prices and effects from reduced vibration detection in human beings with diabetes within the US. Diabetes Care, 26: 2305-2310.
View at Publisher | View at Google Scholar - Gordois A, Scuffham P, Shearer A, Oglesby A, Tobian JA. (2003). The fitness care costs of diabetic peripheral neuropathy in the US. Diabetes Care ,26: 1790 -1795.
View at Publisher | View at Google Scholar - Gordois A, Scuffham P, Shearer A, Oglesby A. (2003). The healthcare fees of diabetic peripheral neuropathy inside the United Kingdom. Diabetic Foot ,6: 62-73.
View at Publisher | View at Google Scholar - Rogers LC, Lavery l. a, Armstrong DG. (2008). The proper to endure legs. J Am Podiat Med Assoc, 98: 166-168.
View at Publisher | View at Google Scholar - Pecoraro RE, Reiber GE, Burgess EM. (1990). Pathways to diabetic limb amputation: basis for prevention. Diabetes Care, 13:510-521.
View at Publisher | View at Google Scholar - Siitonen OI, Niskanen LK, Laakso M, Siitonen JT, Py ö r ä l ä okay. (1993). lower extremity amputation in diabetic and non-diabetic sufferers: a populace - based have a look at from Japanese Finland. Diabetes Care, 16: 16 -20.
View at Publisher | View at Google Scholar - Boulton AJM, Malik RA, Arezzo JL, Sosenko JM. (2004). Diabetic somatic neuropathy: a technical comparison. Diabetes Care, 27: 1458-1486.
View at Publisher | View at Google Scholar - Boulton AJM. (1990). Diabetic foot ulcers: association with leprosy. Practice Diabetes Digest, 3:35-37.
View at Publisher | View at Google Scholar - Boulton AJM. (2008). Diabetic foot: a big review. Diabetes Metab Res Rev, 24:3- 6.
View at Publisher | View at Google Scholar - Game FL, Chip Chase SY, Hubbard R, Burden RP, Jeffcoate WJ. (2006). Temporal affiliation between the advantages of leg ulceration and initiation of dialysis in diabetes mellitus. Transplantation of Nephrol numbers, 21: 3207-3210.
View at Publisher | View at Google Scholar - Murray HJ, Young MJ, Boulton AJM. (1996). The relationship between callus formation, disproportionate pressure on the feet, and neuropathy in diabetics leg ulceration. Diabetes Med, 13: 979-982.
View at Publisher | View at Google Scholar - Boulton AJM, Kirsner RS, Vileikyte L. (2004). Neuropathic diabetic foot ulcers. N Engl J Med, 351:48-55.
View at Publisher | View at Google Scholar - Abbott CA, Garrow AP, Carrington AL, Morris J, Van Ross ER, Boulton AJM. (2005). The likelihood of leg ulcers is lower in South Asia and Africa Caribbean compared to European diabetics in the UK:Check out North-West Diabetes Foot Care. Diabetes Care,28:1869-1875.
View at Publisher | View at Google Scholar - Lavery LA, Armstrong DG, Wunderlich RP, Tredwell J, Boulton AJM. (2003). Diabetic foot syndrome: an assessment of the prevalence and incidence of foot pathology in Mexicans and non-Hispanicsdiabetes whites manipulate cohort. Diabetes care, 26: 1435-1438.
View at Publisher | View at Google Scholar - Solano MP, Prieto LM, Varon JC, Moreno M, Boulton AJM. (2008). Ethnic variation of plantar pressures in diabetic patients with peripheral neuropathy. Diabetes Med, 25:505-507
View at Publisher | View at Google Scholar - Reiber GE, Vileikyte L, Boyko EJ, del Aguila M, Smith DG, Lavery los angeles et al. (1999). Causal pathways for the improvement of lower limb ulcers in diabetic sufferers from two settings. Diabetes Care, 22:157-162.
View at Publisher | View at Google Scholar - Boulton AJM, Armstrong DG, Albert SF, Frykberg RG, Hellman R, Kirkman MS, et al. (2008). A comprehensive exam of the toes and dangers evaluation. Diabetes Care,31:1679-1685.
View at Publisher | View at Google Scholar - Abbott CA, Vileikyte L, Williamson S, Carrington AL, Boulton AJ. (1998). A multicenter takes a look at the occurrence and predictive factors in diabetics 'leg ulceration. Diabetes Care, 21: 1071-1075.
View at Publisher | View at Google Scholar - Frykberg RG, Lavery la, Pham H, Harvey C, Harkless L, Veves A. (1998). The function of neuropathy and high leg stress in diabetic foot ulceration. Diabetes Care, 21: 1714-1719.
View at Publisher | View at Google Scholar - Mason J, O'Keeffe C, McIntosh A, Hutchinson A, sales space A, younger RJ. (1999). A systematic assessment of the prevention of leg ulcers in patients with kind 2 diabetes. 1: Prevention. Diabetes Med ,16:801-812.
View at Publisher | View at Google Scholar - Vileikyte L, Rubin RR, Leventhal H. (2004). Psychological aspects of the diabetic neuropathic headaches of the foot: an overview. Diabetes Metab Res Rev, 20: 13-18.
View at Publisher | View at Google Scholar - Vileikyte L. (2008). Psychosocial and behavioral components of the diabetic foot lesions. Curr Diab Rep, 8:119-125.
View at Publisher | View at Google Scholar - Lincoln NB, Radford KA, game FL, Jeffcoate WJ. (2008). training for secondary prevention of foot ulcers in human beings with diabetes: a randomized controlled trial. Diabetology, 51: 1954-1961
View at Publisher | View at Google Scholar - Tentolouris N, Achtsidis V, Marinou okay, Katsilambros N. (2008). Evaluation. self-administered indicator plaster neuro pad for analysis of neuropathy in diabetes. Diabetes Care, 31: 236-237.
View at Publisher | View at Google Scholar - van Schie CH, Abbott CA, Vileikyte L, Shaw JE, Hollis S, Boulton AJM. (1999). Comparative commentary of the Podotrack, a simple semi-quantitative plantar strain dimension device, and the optical pedobarograph inside the assessment of pressures below the diabetic foot.Diabetes Med ,16: 144-159.
View at Publisher | View at Google Scholar - Uccioli L, Faglia E, Montocine G, Favales F, Durola L, Aldeghi A, et al. (1995). Artificial shoes in the prevention of diabetic foot ulcers.Diabetes Care, 18: 1376-1378.
View at Publisher | View at Google Scholar - Veves A, Masson EA, Fernando DJ, Boulton AJM. (1989). Use of experimental padded hosiery to lessen unusual foot pressures in diabetics neuropathy. Diabetes Care, 12: 653-655.
View at Publisher | View at Google Scholar - Garrow AP, van Schie CH, Boulton AJM. (2005). The effectiveness of the multi-layer hosiery in lowering the burden on the ft in high-risk footwear laid low with diabetes. Diabetes Care, 28: 2001-2006.
View at Publisher | View at Google Scholar - Lavery l.A, Higgins KR, Lanctot DR, Constantinides GP, Zamorano RG, Athanasiou KA, et al. (2007). Stopping the recurrence of a diabetic foot ulcer in excessive-risk patients: use of temperature tracking as a self-assessment device. Diabetes Care, 30:14-20.
View at Publisher | View at Google Scholar - Armstrong DG, Holtz-Neiderer ok, Wendel C, Mohler MJ, Kimbriel HR, Lavery la. (2007). pores and pores and skin temperature tracking reduce the threat of diabetic foot ulceration in sufferers with excess possibility. Am J Med, 100 and 20: 1042-1046.
View at Publisher | View at Google Scholar - van Schie CHM, Whalley A, Vileikyte L, Wignall T, Hollis S, Boulton AJ. (2000). Efficacy of injected liquid silicone inside the diabetic foot to reduce randomized elements for ulceration: a randomized double-blind placebo-managed trial. Diabetes Care, 23: 634-638.
View at Publisher | View at Google Scholar - van Schie CH, Whalley A, Armstrong DG, Vileikyte L, Boulton AJM. (2002). effect of silicone injections within the diabetic foot on plantar top strain and thickness of plantar tissue: and a pair of years by - up. Arch Phys Med Rehabil, 83: 919-923.
View at Publisher | View at Google Scholar - Jeffcoate WJ, sports activities FL. (2006). Description and type of diabetics leg lesions: systems for scientific care, examination, and audit. In: BoultonAJM, Cavanagh PR, Rayman G, eds. The Foot in Diabetes, 4th edn. Chichester: John Wiley & Sons Ltd, 92-107.
View at Publisher | View at Google Scholar - Armstrong DG, Lavery l. a., Harkless LB. (1998). Validation of a diabetic wound-type gadget. Diabet Med, 21: 855-859.
View at Publisher | View at Google Scholar - Oyibo S, Jude EB, Tarawneh I, Nguyen HC, Harkless LB, Boulton AJ. (2001). A comparison of diabetic foot ulcer class structures. Diabetes Care, 24: 84-88.
View at Publisher | View at Google Scholar - Sibbald RG, Woo KY. (2008). The biology of continual foot ulcers in men and women with diabetes. Diabet Metab Res Rev,24:25- 30.
View at Publisher | View at Google Scholar - Blakytny R, Jude EB, Gibson M, Boulton AJM, Ferguson MW. (2000). Lack of insulin-like boom element 1 (IGF1) in the basal keratinocyte layer of diabetic pores and skin and diabetic foot ulcers. J Pathol ,190: 589-594.
View at Publisher | View at Google Scholar - Jude EB, Blakytny R, Bulmer J, Boulton AJM, Ferguson MW. (2002). reworking growth trouble - beta 1,2,3 and receptor international type 1 and a of interventions nation for t diabetic foot ulcers. Diabet Med, 19: 440- 447.
View at Publisher | View at Google Scholar - M ü ller M, Trocme C, Lardy B, Morel F, Halimi S, Benhamou PY. (2008). Matrix metalloproteinases and diabetic foot ulcers: the ratio of MMP - 1 to TIMP - 1 is a predictor of wound restoration. Diabet Med, 25:419 -426.
View at Publisher | View at Google Scholar - Armstrong DG, Nguyen HC, Lavery la, van Schie CH, Boulton AJM, Harkless LB. (2001). Offloading the diabetic foot wound: a randomized medical trial. Diabetes Care, 24:1019-1022.
View at Publisher | View at Google Scholar - Armstrong DG, Lavery la, Kimbriel HR, Nixon BP, Boulton AJM. (2003). Interested kinds of sufferers with diabetic foot ulceration: patients with energetic ulcers may not adhere to a desired pressure offloading ordinary. Diabetes Care, 26: 2595- 2597.
View at Publisher | View at Google Scholar - Katz IA, Harlan A, Miranda - Palma B, Preto L, Armstrong DG, Bowker JH, et al. (2005). A randomized trial of two irremovable offloading gadgets in the control of plantar neuropathic diabetic foot ulcers. Diabetes Care, 28: 555-559.
View at Publisher | View at Google Scholar - Piaggesi A, Viacava P, Rizzo L, Naccarato G, Baccetti F, Romanelli M, et al. (2003). Semi-quantitative evaluation of the histopathological features of the neuropathic foot ulcers: results of stress relief. Diabetes Care, 26: 3123-3128.
View at Publisher | View at Google Scholar - Vileikyte L. (2007). strain and wound restoration. Clin Dermatol, 25: 49-55.
View at Publisher | View at Google Scholar - Nabuurs - Franssen MH, Sleegers R, Huijberts MS, Wijnen W, Sanders AP, Walenkamp G, et al. (2005). Overall contact casting of the diabetic foot in each day practice: a potential observe - up look at. Diabetes Care, 28: 243- 247.
View at Publisher | View at Google Scholar - Mason J, ' O'Keeffe CO, Hutchinson A, McIntosh A, younger R, sales space A. (1999). A scientific overview of foot ulcers in patients with kind 2 diabetes. II: remedy. Diabet Med, 16: 889-909.
View at Publisher | View at Google Scholar - Knowles EA. (2006). Dressings: is there an evidence base? In: Boulton AJM, Cavanagh PR, Rayman G, eds. The Foot in Diabetes, 4th edn. Chichester: John Wiley & Sons Ltd, 186-197.
View at Publisher | View at Google Scholar - Lipsky BA. (2008). New traits in diagnosing and treating diabetic foot infections. Diabet Metab Res Rev,24: 66-71.
View at Publisher | View at Google Scholar - Chantelau EA, Tanudjaja T, Altenh ö fer F, Ersanli Z, Lacigova S, Metzger C. (1996). Antibiotic remedy for simple neuropathic forefoot ulcers in diabetes: a controlled trial. Diabet Med, 26: 267-276.
View at Publisher | View at Google Scholar - Lipsky BA. (2004). A report from the global consensus on diagnosing and treating the infected diabetic foot. Diabetes Metab Res Rev, 20: 68-77.
View at Publisher | View at Google Scholar - Lipsky BA, Berendt AR, Deery HG, Embil JM, Joseph WS, Karchmer AW, et al. (2004). Infectious diseases Society of our pointers: diagnosis and treatment of diabetic foot infections. Clin Infect Dis, 39: 885- 910.
View at Publisher | View at Google Scholar - Nelson EA, O'Meara S, Golder S, Dalton J, Craig D, Iglesias C. (2006). DASIDU consulting organization. Systematic evaluation of antimicrobial agents Treatment for diabetic foot ulcers. Diabetes Medicine, 23:348-359
View at Publisher | View at Google Scholar - Sotto A, Richard J-L, Jordan N, Convecure C, Bougie N,Lavigne J-P. (2007). Small oligonucleotide arrays:latest devices Distinguishing Between Staphylococcal Colonization and Contamination Staphylococcus aureus in diabetic foot ulcers. Diabetes Care,30:2819 -2828.
View at Publisher | View at Google Scholar - Bowling FL, Sarugami EV, Boulton AJM. (2007). Larvae treatment: A unique means of eradicating methicillin-resistant Staphylococcus aureus Diabetic foot ulcer. Diabetes Care, 30:370-371.
View at Publisher | View at Google Scholar - Rozzanigo U, Tagliani A, Vittorini E, Pacchioni R, Brivio LR, Kaudana R. (2009). Function of Magnetic Resonance Imaging in Evaluation Diabetic foot with suspected osteomyelitis. Radiorumed, 114:121-132.
View at Publisher | View at Google Scholar - Butalia S, Paruda VA, Sargent RJ, Detsky AS, Murad O. (2008). Do Diabetics Have Lower Extremity Osteomyelitis?JAMA , 299:806-813.
View at Publisher | View at Google Scholar - Fleischer AE, Didik AA, Woods JB, Burns SE, Lobel JS, ArmstrongDG. (2009). Combining scientific and clinical tests improves the diagnosis Accuracy of osteomyelitis in the diabetic foot. J foot and ankle surgery, 40-8:39-46.
View at Publisher | View at Google Scholar - Training FL, Jeff Court WJ. (2008). Through extensive non-surgical treatment, Foot osteomyelitis in diabetes. Diabetes, 51:962-967.
View at Publisher | View at Google Scholar - Berent AR, Peters EJ, Bakker OK, Envil JM, Eneros M, Hinchliffe RJ, et al. (2008). Diabetic poliomyelitis:Improvement file for evaluation and scientific evaluation of treatments. Diabetes Meta Tab Resolution Revised,24:100 :40:151-161.
View at Publisher | View at Google Scholar - Jeffcoate WJ, Lipsky BA, Berendt AR, Cavanagh PR, Bass SA, Peters EJ et al. (2008). An unsolved problem in the treatment of foot ulcers with diabetes. Diabetes Medicine, 25:1380-1389.
View at Publisher | View at Google Scholar - Wieman TJ, Smiell JM, Yachin S. (2006). Efficacy and safety of topical gels.Components of the Recombinant Human Platelet Boom Problem -BB (becapermine) in patients with persistent neuropathic diabetic foot Ulcer. Diabetes Care 1998; 21:822-827. 82 Berent AR. Counterpoint: Hyperbaric oxygen for diabetic feet does not affect wounds. Clin Infect Dis, 193-198.
View at Publisher | View at Google Scholar - Avidia A, Laden G, Kuhan G, Johnson BF, Wilkinson AR. (2003). Renwick Characteristics of hyperbaric oxygen therapy for ischemic diabetic ulcers of the lower extremities: Double-blind, randomized controlled court proceedings. Eur J Vasc Endovasc Surg ,25:513-518.
View at Publisher | View at Google Scholar - Hinchliffe RJ, Valk GD, Apelqvist J, Armstrong DG. (2008). Bakker accuracy, activity Florida, etc. Systematic assessment of the effectiveness of interventions Promotes healing of persistent diabetic foot ulcers. Diabetes Metab Res Rev, 24:119-144.
View at Publisher | View at Google Scholar - Armstrong DG, Boulton AJM. (2006). Wound healing against severe strain (VAC). of: Boulton AJM, Cavanagh PR, Rayman G ed, The Foot Diabetes, 4th Edition, Chichester: John Wiley & Sons, Inc,360-364.
View at Publisher | View at Google Scholar - Armstrong DG, Ravelry l. A. (2005). Diabetic Foot Examination Consortium.Treatment of severe stress wounds after a partial leg amputation due to diabetes: Multicenter, randomized, controlled trial. Lancet,366:1704.
View at Publisher | View at Google Scholar - Blume PA, Walters J, Payne W, Ayala J, Lantis J. (2008). A comparison vacuums wound remedy using vacuum closure with superior wet wound therapy inside the remedy for diabetic’s leg ulcers: a multicenter randomized controlled trial. Diabetes care, 31: 631-636.
View at Publisher | View at Google Scholar - Blozíokay E, Scherer M. (2008). Pores and skin substitute treatment for the diabetic foot ulcers: a scientific review and meta-evaluation. Diabetes Care, 31: 693-694.
View at Publisher | View at Google Scholar - Jeffcoate WJ. (2008). Charcot neuroarthropathy. Diabetes Metab Res Rev, 24: 62-65.
View at Publisher | View at Google Scholar - Mabilleau G, Petrova NL, Edmonds ME, Sabokhar A. (2008). Improved osteoclastic activity in acute Charcot osteoarthropathy: function receptor activator of nuclear thing - kappa B ligand. Diabetology, 51:1035-1040.
View at Publisher | View at Google Scholar - Rathur H, Boulton AJM. (2007). Neuropathic diabetic foot. Natl Clin Pract Endocrinol Metab,3: 14- 25.
View at Publisher | View at Google Scholar - Jude EB, Selby PL, Burgess J, Lilleystone P, Mawer EB, page SR, et al. (2001). Bisphosphonates in the treatment of Charcot neuroarthropathy thy: a double-blind randomized managed trial. Diabetology, 44:2032-2037.
View at Publisher | View at Google Scholar - Robinson AH, Pasapula C, Brodsky JW. (2009). Surgical elements diabetic foot. J Bone Joint Surg Br, 91:1-7.
View at Publisher | View at Google Scholar - Armstrong DG, Wrobel J, Robbins JM. (2007). visitor editor: you've got diabetes-related wounds and amputations worse than most cancers? inner wound J; 4: 286-287.
View at Publisher | View at Google Scholar - young MJ, McCardle JE, Randall LE, Barclay JI. (2008). advanced survival of diabetic foot ulcer patients 1995–2008: possible impact aggressive cardiovascular threat management. Diabetes Care, 31: 2143-2147.
View at Publisher | View at Google Scholar - Boulton AJM. (1995). Why bother instructing the multidisciplinary crew and the affected person: the instance of prevention of decreased extremity amputation in diabetes. affected person EducCoun,26: 183-188.
View at Publisher | View at Google Scholar - Boulton AJM. (1992). The yearly assessment: right here to live. Diabet Med, 9: 887.
View at Publisher | View at Google Scholar - Trautner C, Haastert B, Mauckner P Gatcke LM, Giani G. (2007). Decreased incidence of lower-limb amputations in the diabetic population of a German city, 1990–2005: outcomes of the Leverkusen Amputation Discount Study (LARS). Diabetes Care, 30: 2633-2637.
View at Publisher | View at Google Scholar - Krishnan S, Nash F, Baker N, Fowler D, Rayman (2008). discount in diabetic amputations over 11 years in a defi ned UK population: benefits of multidisciplinary group paintings and non-stop prospective audits. Diabetes Care, 31(8):99-101.
View at Publisher | View at Google Scholar - Canavan RJ, Unwin ND, Kelly WF, and Connolly VM. (2008). Diabetes and non-diabetes-associated lower extremity amputation incidence earlier than and after the introduction of more organized diabetes foot care: continuous longitudinal monitoring using a trendy approach. Diabetes Care, 459-463.
View at Publisher | View at Google Scholar - Larsson J, Eneroth M, Apelqvist J, Stenstöm A. (2008). Sustained reduction in principal amputations in diabetic sufferers: 628 amputations in 461 patients in a defined populace over 20 years. Acta Orthop, 79: 665-673.
View at Publisher | View at Google Scholar
