

Case report | DOI: https://doi.org/10.31579/2834-8508/014
Fascinating Five Cases of foreign Body in throat in Fifteen Flicks: from Denture to Denomination to Demineralised Bone.
- Sphoorthi Basavannaiah *
Associate Professor, Department of ENT, Subbaiah Institute of Medical Sciences, NH-13, Purle, Holebenavalli Post, Shimoga-577222, Karnataka, India
*Corresponding Author: Sphoorthi Basavannaiah, Associate Professor, Department of ENT, Subbaiah Institute of Medical Sciences, NH- 13, Purle, Holebenavalli Post, Shimoga-577222, Karnataka, India.
Citation: Sphoorthi Basavannaiah (2023), Fascinating Five Cases of foreign Body in throat in Fifteen Flicks: from Denture to Denomination to Demineralised Bone. Archives of Clinical and Experimental Pathology. 2(2); Doi:10.31579/2834-8508/014
Copyright: © 2023 Sphoorthi Basavannaiah, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 March 2023 | Accepted: 17 March 2023 | Published: 03 April 2023
Keywords: foreign body; oral cavity; oropharynx; throat; oesophagus; ingestion; impacted
Abstract
Foreign body (FB) ingestion is an everyday existence and a common emergency exhibition. Many ingested FBs become impacted, often in and around the oral cavity, oropharynx and oesophagus. They have potential chances to cause serious impediments, apart from substantial agony to the patient and family.
Introduction
Foreign body (FB) ingestion and impaction in and around the oral cavity, oropharynx and oesophagus constitute an important cause of morbidity and mortality worldwide. One-third of foreign bodies retained in the gastrointestinal tract are present in the oesophagus. It is mostly seen in children which require endoscopic removal with rigid oesophagoscopy [1,3]. This can happen as an everyday existence and present as a common emergency. They have potential chances to cause solemn obstacles, apart from ample anguish to the patient and family members. Here, are 5 interesting cases of foreign body throat ingested and impacted with diverse & discrete case scenarios.
Case report/ Series
Case 1- Rough, Rutted jammed bone.
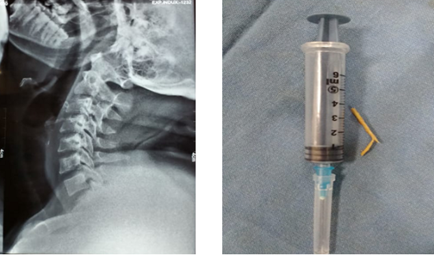
Figure 1 & 2: 1- X-Ray neck (Lateral view) showing inverted L shaped radiopaque foreign body impacted in the oesophageal wall below the hyoid bone and almost at the level of thyroid cartilage. 2 – piece of mutton bone measuring nearly 4 cm3 after removal.
Here, is a middle aged adult male comes to ENT OPD with h/o choking while having food. On history, it was known that patient had taken mutton biryani about an hour back. He had excessive throat pain, unable to swallow even saliva and unable to converse even. Patient had tried to remove the foreign body by forceful vomiting, but unable to do so but rather had blood-tinged vomitus. There was no symptoms of breathing difficulty or signs of sridor. But Videolaryngoscopic examination was unable to perform as he was not cooperative and there was excessive pooling and dribbling of saliva. Then a radiograph was done as shown in Figure 1. This wedged foreign body was removed with help of Rigid Oesophagoscopy under general anaesthesia as shown in Figure 2. Patient was discharged after about 3 hours of keeping under observation. The patient was fine with vitals stable at the time of discharge.
Case 2 – Sleek, Shrill wedged bone.

Figure 3 & 4: 3- X-Ray neck (Lateral view) showing thin, sleek, radiopaque foreign body impinged in the oesophageal wall. 4 – gross picture of chicken bone measuring nearly 2cm after removal.
Here, a young adult male comes to ENT OPD with h/o foreign body sensation in the throat immediately after lunch. On history, it was known that patient had taken chicken biryani about an hour back. He had excessive throat pain, unable to swallow even saliva and unable to converse even. Patient had even tried forceful vomiting to get relieved from this symptom, but was unable to do so but rather had blood-tinged vomitus. There were no symptoms of breathing difficulty or signs of stridor. Videolaryngoscopic examination was unable to perform as the patient was not cooperative plus there was excessive nausea, pooling and dribbling of saliva. Radiograph was done as shown in Figure 3. This lodged foreign body was removed with help of Rigid Oesophagoscopy under general anaesthesia, as shown in Figure 4. Patient was discharged after about 3 hours of keeping under observation. The patient was fine with vitals stable at the time of discharge.
Case 3 (a, b & c): Slick, Shiny squeezed bone.
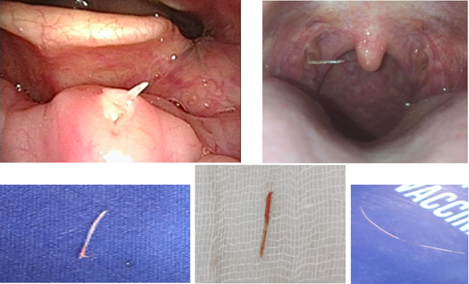
Figure 5, 6, 7, 8, 9: 3- X-Ray neck (Lateral view) showing thin, sleek, radiopaque foreign body impinged in the oesophageal wall. 4 – gross picture of chicken bone measuring nearly 2cm after removal.
Here are 2 cases with foreign body fish bone in the oropharynx who visited the ENT OPD with dysphagia, odynophagia, pain and pricking sensation in the throat. On history, very typical of ingestion of fish during lunch and dinner was present. Patients had even tried forceful vomiting to get rid of their symptoms, but was unable to do so. There were no symptoms of breathing difficulty or signs of stridor. On clinical examination of oral cavity oropharynx and videolaryngoscopic examination of larynx, fish bone were noted as described in Figure 5 & 6. In these cases, fish bone was removed in the OPD under local anaesthesia as shown in Figure 7, 8 & 9. Patient was discharged immediately post removal of the foreign body. The patient was fine with vitals stable at the time of discharge.
Case 4: Spherical, Stout squeezed coin.
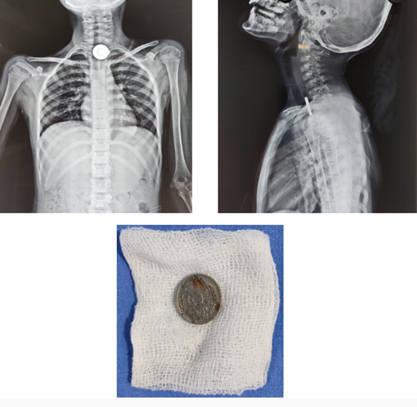
Figure 10, 11 & 12: Figure 10 & 11- X-Ray neck with thorax (AP (9) &Lateral (10) views) showing circular, round radiopaque foreign body lodged in the oesophagus while in lateral view it looks like a slit which appears like a coin. 12- gross picture of 5 rupee coin after removal.
Here is a case of 7 year old boy who accidentally swallowed a foreign body while playing. His parents brought him to the ENT OPD immediately. Patient was appearing okay but his parents were anxious. The boy was not cooperative for any sort of clinical examination. Hence, radiograph was done as shown in Figure 10 & 11. The child was posted for Oesophagoscopy under general anaesthesia for foreign body removal as shown in Figure 12. The patient was kept for observation for 1 day and discharged the next day.
Case 5: Dangerous, Dangled denture.

Figure 13, 14 & 15: Figure 13- X-Ray neck lateral view showing irregular radiopaque foreign body in the oesophagus. Figure 14- MRI Neck with contrast showing huge irregular radiodensity in the oesophagus with pockets of air shadow unable to exactly identify the nature of foreign body. 15- gross picture of this huge denture after 4 days of ingestion which was removed under Rigid Oesophagoscopy under general anaesthesia without any complications on and post removal.
Here is a case of 70 year old male who accidentally swallowed his denture while lying down ideally. He was brought to ENT OPD the next morning. Patient was very anxious and stressed. He had not taken orally since the episode. Clinically, patient was not co-operative for videolaryngoscopic examination as he had excessive pooling of saliva. There were no signs suggestive of oesophageal perforation or any signs of stridor by then. Hence, radiograph was done as shown in Figure 13, which was barely conclusive. Further, for confirmation an MRI neck was done as depicted in Figure 14. The old man was then posted for Foreign body removal under emergency basis and removed with Rigid Oesophagoscopy under general anaesthesia as shown in Figure 15. As per history, as the nature of body was suggested as Denture, any untoward complication with relation to oesophagus was anticipated. But, the case got over clean without any hustles. The patient was kept for observation for 2 days and discharged. The patient was fine with vitals stable at the time of discharge.
Discussion
There is enough of literature (1-5) regarding foreign body throat removal, Hence, I just wanted to bring upon certain highlights that has to be kept in mind when situation like this arises. So, here is the gist of things chosen from the literature mentioned below that is accounted and considered in this study. Every surgeon has his/ her own take and experiences encountered by far for foreign body removal which has been dealt with at various time in their professional life. The things mentioned below could be a repetition for most of us but still at times these crucial points are often masked in our thoughts during dealing with the present case scenario.
The highlights for foreign body throat (1-5):
- It is an emergency and airway has to be kept secure which is a priority.
- Proper history from the patient is utmost important (especially time of intake of last meal).
- Videolaryngoscopy is a helpful tool at times to visualise the foreign body in oral cavity, oropharynx and throat (provided he is comfortable and at ease) and at times has even aid in its removal.
- Plain radiography and computer tomography are both highly sensitive and specific to locate the foreign and also to know the nature of the foreign body itself.
- The foreign body can be anything regardless of its shape and size( sharp or not sharp) if it can easily accommodate in the mouth- pebbles, coin, bone( fish/ chicken/ mutton), safety pins, dentures, parts of toys and which can be easily swallowed.
- McGill’s forceps at times comes handy for foreign body removal (must have in the tray).
- Removal if planned in outpatient department, local anaesthetic spray or local anaesthetic viscous must be made available.
- Proper instrumentation must be available for removal of foreign body if visualised under local anesthesia.
- First attempt is the best attempt after visualisation of foreign body and avoid repeated manipulation for its removal.
- After removal the foreign body must be handed over to the patient (if possible shown to the patient on videolaryngoscopic examination as well prior to removal).
- Do not forcefully try to remove the foreign body (own attempts by forceful vomiting, coughing etc).
- Do not panic (as patient is already anxious state).
- Do not eat on lying down position.
- Do not talk or laugh while having food (to avoid choking).
- Both patient and the surgeon have to be patientful throughout during this entire process from the word “go”.
Conclusion
Foreign body in throat will continue to be a common emergency. Even though better community education and parent teaching programs might be of some value, it is unlikely that there will be a substantial drop in the occurrence of the most common reason for emergency endoscopy. The best approach towards this problem lies in evolving standard strategies for dealing with this situation, a hope that can only turn into reality through further evidence- based medicine along these lines and universal persuasive.
References
- Patel NR, Sharma P. (2021). Foreign Bodies in Esophagus: An Experience with Rigid Esophagoscope in ENT Practice. International Journal of Head and Neck Surgery. January–March; 12 (1): 1-5.
View at Publisher | View at Google Scholar - Chuanyao Lin, Dingding Liu, Han Zhoul, et al. (2020). Clinical diagnosis and treatment of throat foreign bodies under video laryngoscopy: A retrospective clinical research report. Journal of International Medical Research. 48(7): 1-8.
View at Publisher | View at Google Scholar - Wei-Shuyi Ruan, Yu-Ning Li, Meng-Xiao Feng et al. (2020). Retrospective observational analysis of esophageal foreign bodies: a novel characterization based on shape. Scientific Reports. 10:4273
View at Publisher | View at Google Scholar - Opoku-Buabeng J, Abdulai Re. (2012). Unsual foreign body in the throat: a report on 3 cases. Case Reports & Case Series. Journal of the West African College of Surgeons. July-Sept. 1(3): 88-95.
View at Publisher | View at Google Scholar - Ashraf O. (2006). Foreign body in the esophagus: a review. Sao Paulo Med J. 124(6): 346-9.
View at Publisher | View at Google Scholar
