

Case Report | DOI: https://doi.org/10.31579/2835-2882/039
Facial Eccrine Angiomatous Hamartoma in a Fifty-two-Year-Old Lady: Case Report
1 Department of dermatology, New Ahmadi Hospital, Ahmadi, Kuwait.
2 Histopathology unit, Jaber Al Ahmad Hospital, Kuwait.
*Corresponding Author: Shaymaa M Ahmad. Consultant Dermatologist, New Ahmadi Hospital, Kuwait.
Citation: Shaymaa M. Ahmad, Mohammad T., Ahmad M. L. Elsebaey, (2023), Facial Eccrine Angiomatous Hamartoma in a Fifty-two-Year-Old Lady: Case Report., Clinical Research and Studies, 2(6); DOI: 10.31579/2835-2882/039
Copyright: © 2023, Shaymaa M. Ahmad. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 November 2023 | Accepted: 17 November 2023 | Published: 27 November 2023
Keywords: eccrine; hamartoma; hyperhidrosis; facial
Abstract
Eccrine angiomatous hamartoma (EAH) is a rare benign condition, Patients typically present with a solitary, sometimes enlarging nodule of the extremities usually appearing at birth or arising during childhood. Eccrine angiomatous hamartoma is usually sporadic, but one familial case of the multifocal variant has been reported. It is recognized histologically by increased numbers of eccrine elements, as well as numerous vascular channels and proliferation of other dermal elements, such as adipose tissue, hair and epidermis. When symptomatic, EAH may be associated with hyperhidrosis or pain. We report a case of 52 years old lady with EAH on the face. We also share our experience with botulinum toxins in the treatment of this condition.
Introduction
Eccrine angiomatous hamartoma is a rare benign malformation that is usually congenital or prepubertal and there is no preference related to patient’s sex. It presents as a solitary flesh colored lesion, either asymptomatic or may cause mild pain and hyperhidrosis on extremities. Enlargement typically occurs commensurate with growth of the patient's limb. Histologically it is characterized by increased number of sweat glands (eccrine) and numerous capillaries. The condition is usually benign and required no intervention unless the patient is bothered with the shape and hyperhidrosis. At this point surgical intervention is established. Many cases in the literature were successfully treated with botulinum toxins.
Case Report:

Figure 1

Figure 2

Figure 3
Hyperhidrosis could be confirmed with the iodine starch test. Figure [4]

Figure 4
5 mm punch biopsy was done from the lesion and the histopathology examination revealed nodular clusters of dilated vessels intimately associated with an increased number of mature eccrine glands while the epidermis is unremarkable as shown in figure [5] [6] [7]
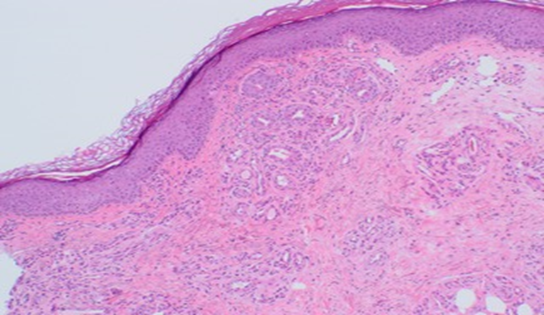
Figure 5
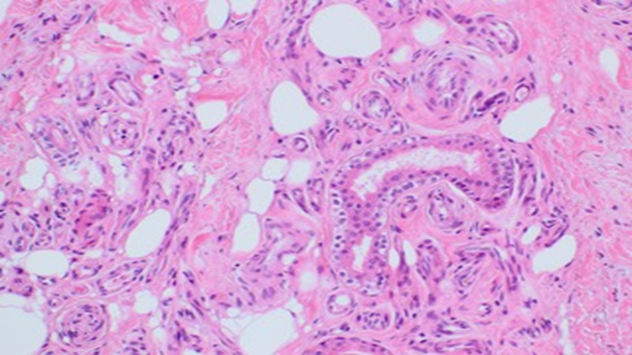
Figure 6
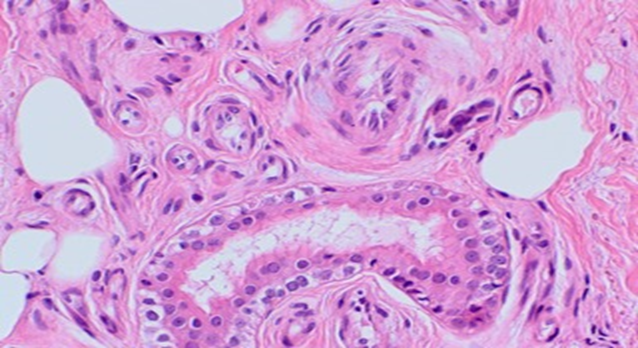
Figure 7
The constellation of clinical and pathological features consistent with the diagnosis of eccrine angiomatous hamartoma EAH.
The lesion was injected with 30 U botulinum toxin diluted in 2.5 ml normal saline in superficial dermis with moderate improvement in pain and hyperhidrosis.
Discussion:
EAH is a rare benign condition that is usually congenital or arise during prepubertal years [1]. It has also been reported to occur in older age group. [2] Our case is a 52 years old lady presenting with EAH. The unusual location of EAH in our case and the paucity of its mention in the literature prompted us to report this case. The infiltrated plaque presented on the face particularly the chin.
EAH was first described by Lotzbeck in 1859 as an angiomatous- appearing lesion on the cheek of a child [3]. True incidence is yet unknown. It is a rare benign tumor characterized by proliferation of eccrine and vascular components. It usually presents as a solitary lesion but multiple lesions have been reported. [4] Generally, they enlarge very gradually; more rapid growth and pain have been described during pregnancy and adolescence and this suggests hormonal influence [5]. Other authors have suggested that lesional pain may be caused by the fluid retention associated with menstruation and pregnancy. [5] Eighty percent of the cases are reported over the extremities, [2] with a predilection for palms and soles. The exact pathogenesis is not known but various theories like abnormal induction of heterotypic dependency with resultant malformation of adnexal as well as mesenchymal elements have been proposed. [6]
The hamartoma usually a symptomatic but some patients experience pain due to infiltration of the small nerves. The vascularity in the lesions may raise the temperature [7] and induce hyperhidrosis as in our case. Since hyperhidrosis is a relatively common finding associated with this condition, various other terms have been used to describe this entity, including sudoriparous angioma [8] and functioning sudoriparous angiomatous hamartoma [9]. Lesional hypertrichosis and the association of EAH with Cowden’s syndrome, [10] neurofibromatosis [11] have all been reported.
Radiographic modalities such as magnetic resonance imaging and ultrasound may help to confirm clinical suspicion of an angioma but accurate diagnosis of EAH remain with histology. [7]
The histopathologic hallmarks of EAH include the presence of an increased number of eccrine glands in the mid- and lower dermis along with ectatic or collapsed vessels that are seen in close approximation to the hyperplastic eccrine units. The overlying epidermis may be normal or may show acanthosis or papillomatosis. [1][12]
Physician should consider other differential diagnosis when dealing with EAH such as eccrine nevus, blue rubber bleb nevus syndrome, tufted angioma, glomus tumor, and smooth muscle cell hamartoma, nevus flammeus and angioma serpiginosum. [13] [14] [15] Although aggressive treatment is generally unwarranted, simple excision is usually curative. Recently botulinum toxin [16] and intralesional sclerosants [17] have been successfully used in the treatment of this condition.
Acknowledgment
We dedicate this article to our dear patient who cooperated with us to the maximum and allowed us to publish the case, thanking her for her kind cooperation and wishing her recovery
Conflict of interest
there is no conflict of interest
Financial support and sponsorship
Nil
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patients understand that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
References
- Sulica, R. Lucien; Kao, Grace F.; Sulica, Virginia I.; Penneys, Neal S. (1994). Eccrine angiomatous hamartoma (nevus): Immunohistochemical findings and review of the literature. Journal of Cutaneous Pathology. 21 (1): 71–75.
View at Publisher | View at Google Scholar - Morrell DS, Ghali FE, Stahr BJ, McCauliffe DP. (2001). Eccrine angiomatous hamartoma: A report of symmetric and painful lesions of the wrists. Pediatr Dermatol. 18:117-119.
View at Publisher | View at Google Scholar - Lotzbeck., (1859). Ein Fall von Schweissdrüsengeschwulst an der Wange. Archiv für Pathologische Anatomie und Physiologie und für Klinische Medicin. 16 (1–2): 160–165.
View at Publisher | View at Google Scholar - Jorge-Finnigan, Conrado; Conejero, Claudia; Hernández-Martín, Angela; Sánchez-Gómez, Julian; Noguera-Morel, Lucero, (2015). Congenital Erythematous Plaques and Papules on the Right Arm. Pediatric Dermatology. 32 (2): 285–286.
View at Publisher | View at Google Scholar - Gabrielsen TO, Elgjo K, Sommerschild H. (1991). Eccrine angiomatous hamartoma of the finger leading to amputation. Clin Exp Dermatol. 16:44–45.
View at Publisher | View at Google Scholar - Zeller DJ, Goldman RL. (1971). Eccrine-pilar angiomatous hamartoma: A report of a unique case. Dermatologica. 143:100–104.
View at Publisher | View at Google Scholar - Laeng RH, Heilbrunner J, Itin PH. (2001). Late-onset eccrine angiomatous hamartoma: Clinical, histological and imaging findings. Dermatology. 203:70–74.
View at Publisher | View at Google Scholar - Domonkos AN, Suarez LS. (1967). Sudoriparous angioma. Arch Dermatol. 96:552-553.
View at Publisher | View at Google Scholar - Issa O. (1964). Hamartoma angiomatoso sudoriparo funcionante. Actas Dermo Sifiliogr. 55:361-365.
View at Publisher | View at Google Scholar - Oh JG, Yoon CH Lee CW. (2007). Case of Cowden syndrome associated with eccrine angiomatous hamartoma. J Dermatol. 34:135-137.
View at Publisher | View at Google Scholar - Castilla EA, Schwimer CJ, Bergfeld WF, Skacel M, Ormsby A. (2002). Eccrine angiomatous hamartoma in neurofibromatosistype-1 patient. Pathology. 34:378-380.
View at Publisher | View at Google Scholar - Tempark, T.; Shwayder, T. (2012). Mucinous eccrine naevus: case report and review of the literature. Clinical and Experimental Dermatology. 38 (1): 1–6.
View at Publisher | View at Google Scholar - Aloi F, Tomasini C, Pippione M. (1992). eccrine angiomatous hamartoma; a multiple variant. Dermatology. 184: 219-222.
View at Publisher | View at Google Scholar - Pelle MT, Pride HB, Tyler WB. (2002). Eccrine angiomatous hamartoma. J Am Acad Dermatol. 47:429-435
View at Publisher | View at Google Scholar - Diaz-Landeata L, Kerdel FA. (1993). Hyperhidrotic, painful lesion. Arch Dermatol. 129:105-110.
View at Publisher | View at Google Scholar - Barco D, Baselga E, Alegre M, Curell R, Alomar A. (2009). Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 145:241–243.
View at Publisher | View at Google Scholar - Kaliyadan F, Sundeep V, Hiran KR. (2007). Late onset eccrine angiomatous hamartoma treated with intralesional sclerosant: A case report. Ind J Dermatolo. 52:99–101.
View at Publisher | View at Google Scholar
