

Case report | DOI: https://doi.org/10.31579/2834-796X/033
Extreme Severe Tricuspid Regurgitation in Patient with the First Clinical Manifestation of Right Ventricular Failure: a Case Report
1 Hospital “Dr Aleksa Savić” Prokuplje.
2 Doctor’s office, InterKardia 027 Prokuplje.
*Corresponding Author: Mirjana Isailović-Keković, Miloša Mamića 5, 18400 Prokuplje, Srbija.
Citation: Citation: Mirjana Isailović-Keković, Predrag Keković (2023), Extreme Severe Tricuspid Regurgitation in Patient with the First Clinical Manifestation of Right Ventricular Failure: a Case Report, International Journal of Cardiovascular Medicine, 2(4); DOI:10.31579/2834-796X/033
Copyright: © 2023, Mirjana Isailović-Keković. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 July 2023 | Accepted: 17 July 2023 | Published: 20 July 2023
Keywords: tricuspid regurgitation; right ventricular failure; mitral regurgitation; atrial fibrillation
Abstract
The aim of this study is to demonstrate unrecognized tricuspid regurgitation leading to heart failure. I would like to point out the importance of the ultrasound examination of the heart in detecting severe tricuspid regurgitation
Introduction
The aim of this study is to demonstrate unrecognized tricuspid regurgitation leading to heart failure. I would like to point out the importance of the ultrasound examination of the heart in detecting severe tricuspid regurgitation.
Case report: 81-years-old patient was admitted to the hospital because of the firstclinical manifestation of right ventricular failure. He had acute myocardial infarction in 2009. He hasn't seen a doctor in 14 years. On admission, he had dyspnea and bradyarrhythmia and massive pretibial edema. NT-proBNP was over 12000 pg/ml. The therapy includes a diuretic, bronchodilator, ACE inhibitor and other necessary drugs. He already has atrial fibrillation, and he is already at oral anticoagulant therapy. 12-lead ECG: dextrogram, atrial fibrillation with ventricular response around 60/beats per minute, right bundle branch block. Echocardiography: aorta normal, left atrium enlarged (Figure 1), diastolic dysfunction, mitral regurgitation 3-4+ (EROA 0.3 cm2 and RVol 56ml) (Figure 2); left ventricular ejection fraction 45%, inferior wall akinesis; right atrium and right ventricle are extremely enlarged with spontaneous echo contrast (Figure 3); tricuspid leaflets impaired coaptation; severe TR 4+ in two jets with SPDK=80mmHg (Figure 4); inferior vena cava greatly expanded (about 40mm); vena contracta 15mm.Roentgenogram of lungs and heart: bilateral pleural effusion. Abdominal ultrasound: signs of liver congestion, VCI diameter 42 mm; ascites fluid perihepatic and perisplenic. Therapy at hospital discharge: furosemide, spironolactone, direct oral anticoagulant therapy, ACE inhibitor with mandatory prophylaxis of bacterial endocarditis.
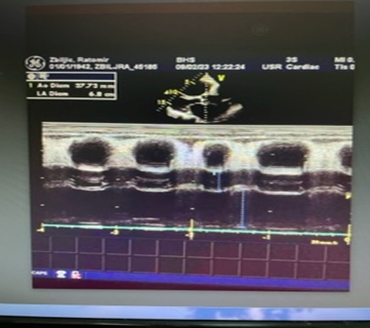
Figure 1: Enlarged left atrium
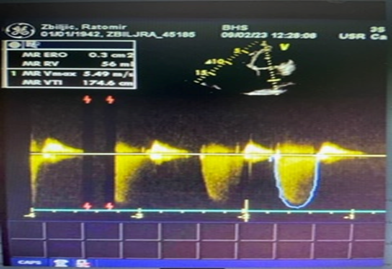
Figure 2: Severe mitral regurgitation
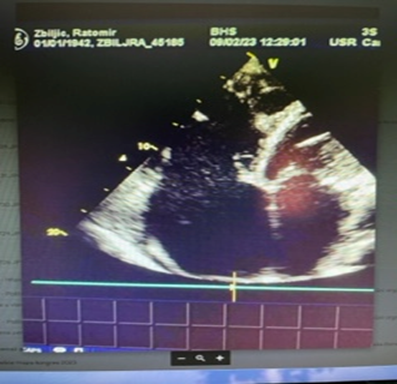
Figure 3: Enlarged right atrium and right ventricle with spontaneous echo contrast
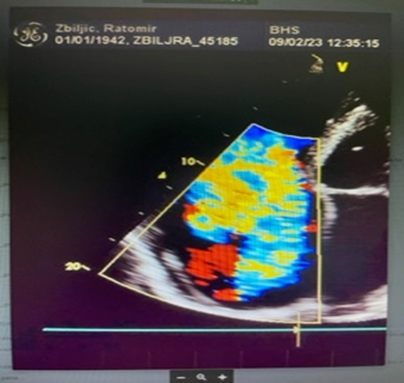
Figure 4: Severe tricuspidal regurgitation
Conclusion
This case report indicates the importance of regular visits to the cardiologist, as well as the importance of timely diagnosis in order to prevent unwanted cardiac events.
References
- Arsalan M, Walther T, Smith RL 2nd, Grayburn PA. Tricuspid regurgitation diagnosis and treatment. Eur Heart J. 2017 Mar 1;38(9):634-638. https://doi.org/10.1093/eurheartj/ehv487
View at Publisher | View at Google Scholar - Buja LM, Butany J, editors. Cardiovascular Pathology, Fifth Edition. Academic Press,2022.
View at Publisher | View at Google Scholar - Mushlin SB, Greene HL. Decision Making in Medicine. Mosby, 3rd Edition, 2010.
View at Publisher | View at Google Scholar - Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017 Sep 21;38(36):2739-2791. https://doi.org/10.1093/eurheartj/ehx391
View at Publisher | View at Google Scholar
