

Case Report | DOI: https://doi.org/10.31579/2835-835X/066
Exclusively percutaneous retrieval of a lost vena cava stent from the right atrium – a case report
- Ruxandra I Sava 1,2
- Truc Mai Nguyen 5
- Emmanuel Cassar 1
- Antoine Marie 3
- Nathanaël F Bayard 4
- Lionel Mangin 1
- Loïc Belle 1*
1Cardiology Department, CH Annecy-Genevois, France
2Cardiology Department, Emergency Hospital Elias,Bucharest, Romania
3Radiology Department, CH Annecy-Genevois, France
4Cardiac Surgery Department, CH Annecy-Genevois, France
5Medicine Department, Department of Medicine,Service of Geriatric Medicine & Geriatric Rehabilitation, University of LausanneHospital (CHUV), Lausanne, Switzerland.
*Corresponding Author: Loic Belle, GCS de cardiologie interventionnelle, 1 Av. de l'Hôpital, 74370 Epagny Metz-Tessy, France
Citation: Ruxandra I Sava, Truc M. Nguyen, Emmanuel Cassar, Antoine Marie, Nathanaël F Bayard, et al, (2024), Exclusively percutaneous retrieval of a lost vena cava stent from the right atrium – a case report, Clinical Trials and Case Studies, 3(5); DOI:10.31579/2835-835X/066
Copyright: © 2024, Loic Belle. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 April 2024 | Accepted: 30 May 2024 | Published: 07 June 2024
Keywords: percutaneous retrieval; vena cava stent; right atrium; case report
Abstract
Background: Vena cava stenting has become the treatment of choice for patients presenting with superior vena cava syndrome. Stent migration into the right heart is a rare, but potentially severe complication, usually requiring cardiac or vascular surgery.
Case Description: An 84-year-old patient with a history of lymphoma was hospitalized for superior vena cava syndrome caused by stenosis and thrombosis of an implantable chemotherapy port. The patient was in complete remission after chemotherapy of diffuse large B cell lymphoma. After an initial course of anticoagulation therapy, the patient was scheduled for percutaneous stenting of the superior vena cava. Unfortunately, this procedure was complicated by stent migration into the right atrium (Fig. B). Multiple attempts to snare the lost stent failed. As the attending cardiac surgeon considered the patient high-risk, the interventional cardiology attending was consulted for percutaneous intracardiac stent removal. The stent retrieval procedure was conducted via femoral access using a 12 French deflectable sheath and a 0.035” hydrophilic guidewire. Using orthogonal projections, the central part of the stent was encircled by the hydrophilic guidewire, followed by snaring of the free end of the guidewire using an endovascular snare. The snared end was subsequently exteriorized. By pulling on both guidewire ends, the vena cava stent was folded onto itself and retracted into the sheath and outside the exit port of the deflectable sheath. Finally, the superior vena cava was successfully stented during a separate intervention, with excellent results. The patient was asymptomatic at 6-month follow-up.
Conclusions: The use of a steerable, large diameter sheath can facilitate the safe retrieval of a lost vena cava stent from the right atrium by an exclusively percutaneous approach, obviating the need for cardiac or vascular surgery.
Introduction
Superior vena cava (SVC) stenting has become the treatment of choice for patients affected by superior vena cava syndrome [1-2]. In a review of thirty-two studies encompassing 884 patients, SVC stenting was fatal in 2% of cases, out of which 41% of cases were due to a cardiovascular cause: arrhythmia, myocardial infarction or tamponade[2]. In this study, the rate of major adverse events was 4% (38 patients), out of which 18 cases were assigned to either stent migration or stent malposition [2]. Although rare, stent migration into the right heart chambers is a significant complication, as it can lead to tricuspid regurgitation[3-4], arrythmia [2,5,6] or cardiac perforation [2,7]. Most case reports describe surgical or hybrid (interventional and vascular surgery) [4,8-12] approaches to retrieve vena cava stents migrated to the right heart chambers. As SVC syndrome is often diagnosed in the context of malignancy, surgical procedures and the need for general anaesthesia are particularly challenging. In such circumstances, the cardiologist may be called upon to attempt percutaneous retrieval of a venous stent that migrated into the right heart chambers. In this case report we illustrate a step-by-step, fully illustrated description of a simple percutaneous means to retrieve a vena cava stent from the right atrium (RA) using a large diameter, steerable catheter that is routinely utilized for position of ablation catheters at the level of the RA. To the best of our knowledge, this technique has not been previously described. We present the following case in accordance with the CARE reporting checklist.
Case Description
An 84-year-old patient with a history of diffuse large B cell lymphoma and an implantable chemotherapy port presented with persistent facial oedema, suggestive of SVC syndrome. Doppler vascular ultrasound suggested obstruction of the right axilar-subclavian axis and the right internal jugular vein. A contrast-enhanced computed tomography scan showed thrombosis of the SVC (around the chemotherapy port) extended to both brachiocephalic veins and to the right internal jugular vein (Figure 1). From a haematological perspective, the patient had been in complete remission for the past 5 years, and cancer recurrence was excluded at the current hospitalisation. However, she was under-weight and fragile. Therapeutic anticoagulation with apixaban 5 mg b.i.d. was initiated, and the patient was scheduled for planned superior vena cava stenting in the following month.
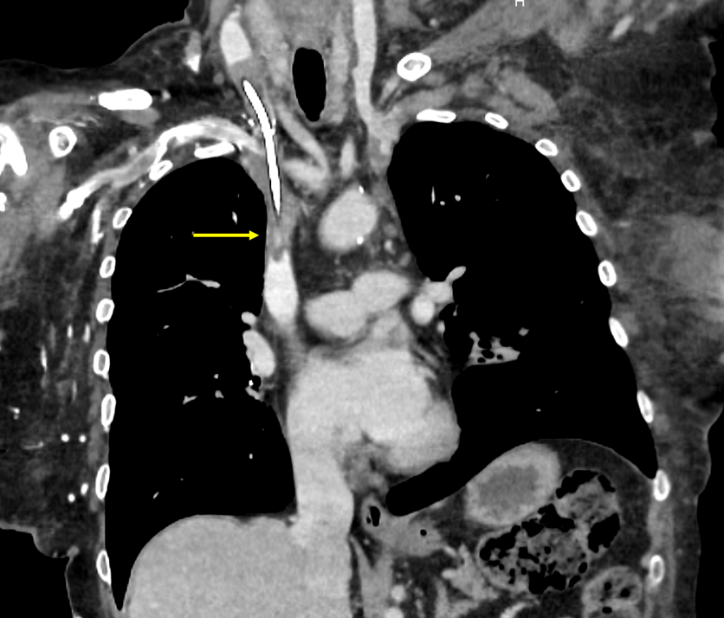
Figure 1: Thoracic computed tomography scan showing superior vena cava thrombosis (yellow arrow).
Stenting of the SVC was attempted by the interventional radiology attendant using right femoral vein access. Venous puncture was guided by vascular ultrasound. The SVC stenosis was crossed using a 0.035” hydrophilic wire (Terumo, Radifocus) via a 5F multipurpose catheter. Following pre-dilation with a 6 mm 0.035” balloon dilation catheter (Boston Scientific, Charger), a 16 mm x 60 mm self-expanding venous stent (Optimed) was implanted. The stent was post-dilated using a 10 mm 0.035” balloon dilation catheter (Boston Scientific, Charger). Upon deflation of the post-dilation balloon, the stent was unfortunately completely dislodged, followed by migration into the RA (Figure 2). Multiple snaring attempts using a right internal jugular, left internal jugular and a left common femoral approach were pursued, with no success.
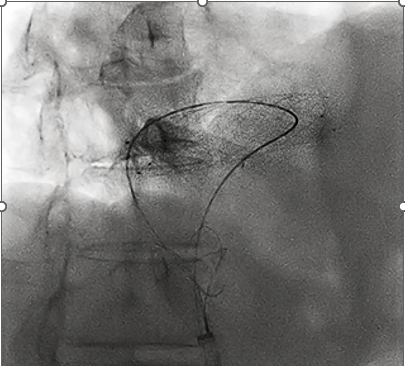
Figure 2: Vena cava stent lost in the right atrium (16 x 60 mm venous stent, OptiMede), encircled by 0,035” hydrophilic guidewire. The guidewire free-end was snared and then retracted down the 12 French deflectable sheath (Medtronic, FlexCath), followed by exteriorization.
The cardiac surgeon attending reviewed the case, assessed the patient to be at high surgical risk, and suggested the interventional cardiology team attempt to retrieve the lost stent percutaneously.
The second stent retrieval procedure was conducted via femoral access using a 12 French deflectable sheath (FlexCath Advance Steerable Sheath, Medtronic). This long sheath, designed for ablation catheter positioning in the RA, allowed us to easily manoeuvre the tip of the sheath in the RA, in close proximity to the lost SVC stent. We first attempted to encircle the stent using a 0.014’’ guidewire (BMW, Abbott), which proved ineffective as this slender guidewire broke. We then attempted to encircle the stent using a stronger, yet highly flexible 0.035” hydrophilic guidewire (Radifocus, Terumo). Using orthogonal projections, we checked for complete encirclement around the central part of the stent (Video 1). We then snared the distal end of the guidewire (Lasso Ensnare, Merit) (Figure 2, 4), gently retracted the end all the way down to the sheath exit port, and then proceeded to pull on both ends of the 0.035” guidewire in order to fold the vena cava stent onto itself and safely retract it into the sheath and outside of the patient (Figure 3, 4; Video 2). The stent was fully retracted at the level of the RA. Finally, the superior vena cava was successfully stented during a separate intervention, with excellent results (Figure. 5). The patient had an uncomplicated hospital stay and was asymptomatic upon discharge, as well as at a 6-month follow-up call.

Figure 3: Stent retraction into the FlexCath by pulling down on both guidewire ends.
Video 1: Terumo Radifocus 0.035” hydrophilic guidewire encircling vena cava stent using orthogonal projections.
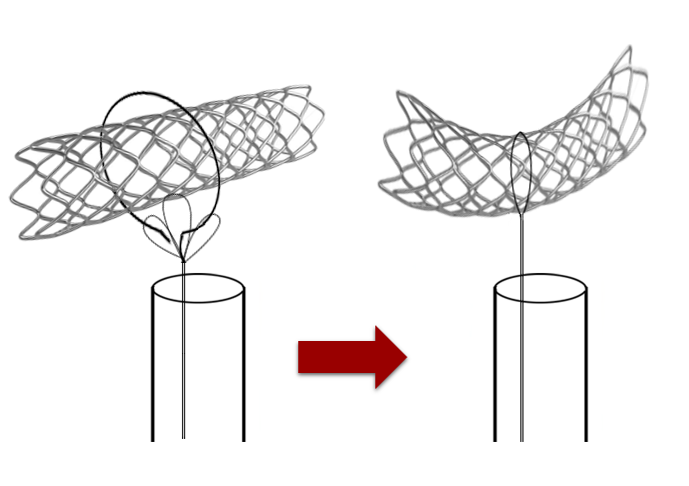
Figure 4: Graphic representation of the procedure.
Video 2: Vena cava stent capturing and retraction into the 12 French deflectable, steerable FlexCath.
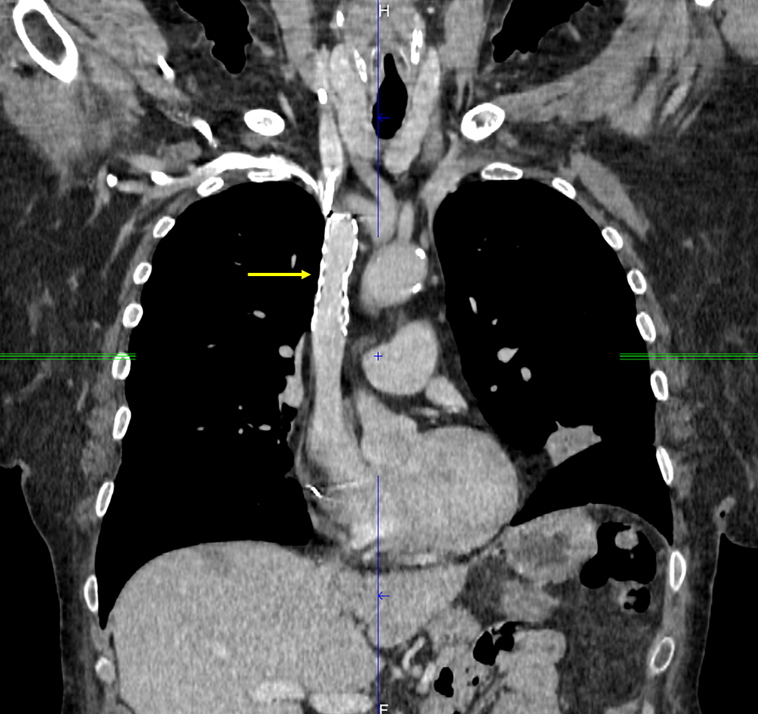
Figure 5: Final thoracic computed tomography scan showing optimal vena cava stent expansion.
Discussion
This case report describes a fully percutaneous approach to vena cava stent retrieval from the right atrium, using a large diameter, steerable catheter that is routinely utilized for ablation catheter positioning. This catheter possesses multiple advantages. Firstly, it is designed to be placed into the RA; this obviates the need for a potentially traumatic retraction of the stent through the venous system down to the femoral vein, as was employed by most case reports citing a hybrid approach at SVC stent retrieval [4,8,11]. Secondly, the catheter is steerable, which allows positioning of the tip of the catheter in close proximity to the migrated stent. Finally, its diameter is large enough to allow for the passage of a stent folded on itself. To the best of our knowledge, this technique has not been reported previously.
Bagu et al used a hybrid, interventional and vascular surgical approach that shares similarities with our method [11]. Initial attempts to directly sna6re the stent failed. The authors then passed a sidewinder catheter (Cordis Europa N.V) over an angled Terumo wire (Terumo Corp, Japan) through a 10 Fr flexible, long venous sheath (Teleflex, 10 Fr Super Arrow-flex sheath, 45 cm in length). They passed the Terumo wire through the entire length of the stent, followed by snaring of the free wire end and shortening of the stent along its long axis. The shortened stent was then retracted into the left femoral vein, from where it was removed by vascular surgeons via venotomy. By comparison, our encirclement of the stent around its middle portion allowed the stent to be folded on itself, while the 12 French deflectable sheath placed into the RA allowed complete retraction of the stent at the level of the RA. Srinathan et al[4] described a method similar to ours, using a Terumo wire to encircle the center part of the SVCS, followed by wire snaring and retraction of the stent into the right common femoral vein, from where it was similarly removed by venotomy. While others have employed large snares or other combinations of snares and guidewires to directly snare the lost stent into the femoral veins, the stent had to be recovered surgically in most of these procedures [4,8,11]. Only two case reports have successfully retracted the lost stent through a short femoral vein sheath: Taylor et al utilized a large snare/wire combination[13], while Ghanem et al grabbed the lost VCS stent from the right ventricle by using an intravascular biopsy forceps, followed by retraction into a 14-F venous sheath[14]. Another case report has described stent recovery from across the tricuspid valve via a 14F sheath placed within the right internal jugular vein, by means of combined balloon and lasso trapping[15]. However, these methods include the inconvenience of dragging the stent through the veinous system, which carries the theoretical risk of causing vascular injury. Treatment should be individualized to each patient and discussed in a heart team consisting of at least an interventional cardiologist and a cardiothoracic or vascular surgeon. The choice in favor of a percutaneous versus a surgical retrieval technique should take into consideration the patient’s surgical risk and the location of the migrated stent, as well as the local expertise, as percutaneous retrieval can require specific material competencies to ensure optimal results and procedural safety.
3.2 Strengths and limitations
We present a fully percutaneous approach to retrieving a SVC stent migrated into the right atrium. Its strengths include lack of stent dragging down the veinous system, as well as no requirement for surgical intervention. The procedure requires good hydrophilic guidewires and endovascular snares, which are routinely found in most catheterization laboratories. However, the large diameter deflectable sheath we employed is a tool dedicated for atrial fibrillation ablation catheter positioning. We had access to such a catheter as we share the catheterization laboratory with the electrophysiology team, and we acknowledge that it may not be available in every institution.
Conclusion
Superior vena cava stenting is the treatment of choice for SVC syndrome. Stent migration from the SVC to the RA is an infrequent, but potentially serious complication. Fully percutaneous retrieval of a lost SVC stent can be achieved by using a hydrophilic 0.035” guidewire, a snare system and a steerable, large diameter sheath destined for right atrial ablation catheter positioning. This avoids the need for cardiac or vascular surgery in patients at high surgical risk.
Acknowledgements
Report the funding source or any other acknowledgements here.
Footnote
Reporting Checklist: The authors have completed the CARE reporting checklist.
Conflict of Interest: The authors have no conflicts of interest to disclose.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. We did not we did not obtain ethical approval for our submission as all procedures were clinically indicated and thus not investigational. We did not include any patient identifiers in our case presentation, nor any identifiable patient characteristics. The patient signed an informed consent form before every procedure and agreed to publication of this case report.
Key findings
- A steerable, large diameter sheath and a hydrophilic 0.035” guidewire can be used to facilitate safe extraction of a vena cava stent migrated into the right atrium, without the need for a surgical approach.
What is known and what is new?
- Stent migration into the right heart is a potential severe complication of vena cava stenting, frequently requiring a surgical approach.
- Our case illustrates a fully percutaneous extraction technique which is particularly valuable in fragile or highly comorbid patients at high surgical risk.
- What is the implication, and what should change now?
- Considering an ageing patient population, interventional cardiologists may increasingly be called upon to assist interventional radiologists in case of cardiac embolization of various devices.
References
- Nguyen NP, Borok TL, Welsh J, Vinh-Hung V (2009). Safety and effectiveness of vascular endoprosthesis for malignant superior vena cava syndrome. Thorax; 2009;64(2):174–8.
View at Publisher | View at Google Scholar - Quencer KB (2022). Superior Vena Cava Syndrome: Etiologies, Manifestations, and Treatments. Semin Intervent Radiol;39(3):292–303.
View at Publisher | View at Google Scholar - Schefold JC, Krackhardt F (2008). Dislocation of a metal stent to the right ventricle: an unusual finding in the heart. J Cardiovasc Med (Hagerstown);9(7):742–3.
View at Publisher | View at Google Scholar - Srinathan S, McCafferty I, Wilson I (2005). Radiological management of superior vena caval stent migration and infection.Cardiovasc Intervent Radiol;28(1):127–30.
View at Publisher | View at Google Scholar - Michael Tempelhof MJCMLIMM (2014). Sinus Arrest Following Angioplasty and Stenting for Superior Vena Cava Syndrome. Journal of Invasive Cardiology;26(2).
View at Publisher | View at Google Scholar - Zannad N, Michy B, Brisse A, et al (2022). Atrial flutter caused by migration of a superior vena cava stent into the right atrium. Ann Cardiol Angeiol (Paris);2022;71(5):331–4
View at Publisher | View at Google Scholar - Prahlow JA, O’Bryant TJ, Barnard JJ (1997). Cardiac perforation due to Wallstent embolization: a fatal complication of the transjugular intrahepatic portosystemic shunt procedure.Radiology; 1997;205(1):170–2.
View at Publisher | View at Google Scholar - Rejjal L, Al-Taweel O, Alwash H, et,.al(2019).Stent migration during endovascular stenting in superior vena cava syndrome in a patient with recent heart transplantation. J Am Coll Cardiol. 2019;73(9).
View at Publisher | View at Google Scholar - Toyoda N, Torregrossa G, Itagaki S, et al (2014). Intracardiac migration of vena caval stent: Decision-making and treatment considerations. J Card Surg;29(3).
View at Publisher | View at Google Scholar - Kang W, Kim I-S, Kim J-U, et al (2011). Surgical Removal of Endovascular Stent after Migration to the Right Ventricle Following Right Subclavian Vein Deployment for Treatment of Central Venous Stenosis. J Cardiovasc Ultrasound. 19(4).
View at Publisher | View at Google Scholar - Bagul NB, Moth P, Menon NJ, et al (2008). Migration of superior vena cava stent. J Cardiothorac Surg. J Cardiothorac Surg;3(1).
View at Publisher | View at Google Scholar - Khazi FM, Alhashimi SBE, Majthoob MY, et al (2021). Multiple Migrated Superior Vena Cava Stents With Cardiac Injury - A Stepwise Open Cardiotomy Strategy to Mitigate Potential Fatality. J Saudi Heart Assoc. J Saudi Heart Assoc; 2021;33(4):317–20.
View at Publisher | View at Google Scholar - of SVC stent migration into the right atrium. Cardiovasc Intervent Taylor JD, Lehmann ED, Belli AM, et al. Strategies for the management Radiol; 2007;30(5):1003–9.
View at Publisher | View at Google Scholar - Ghanem A, Tiemann K, Nickenig G (2009). Gone with the flow: percutanous retrieval of a migrated wallstent trapped in the right ventricle. Eur Heart J. Eur Heart J;30(6):717.
View at Publisher | View at Google Scholar - P. G. Haddad, A. Mohamed, and E. K. Peden (2021). ‘Novel technique of stent retrieval after migration to the right heart’, J Vasc Surg Cases Innov Tech, vol. 7, no. 4, pp. 781–784.
View at Publisher | View at Google Scholar
